
Local Lidocaine–Prilocaine for Immunisation in Infants

 , ,
, , 
Abstract
1. Introduction
1.1. Vaccination in Infants
1.2. Pain in Infants
1.3. Pain Perception in Infants
1.4. Factors Influencing Pain Response
1.5. Assessment of Pain in Infants
1.6. Pain-Reducing Methods
2. Materials and Methods
- Population (P): paediatric patients aged 0–12 months requiring intramuscular vaccination.
- Intervention (I): application of lidocaine–prilocaine cream to the thigh prior to vaccination.
- Comparison (C): effectiveness of the anaesthetic cream versus other interventions (placebo or no intervention).
- Outcomes (O): evaluation of whether lidocaine–prilocaine cream could effectively reduce vaccination pain, using pain scales (e.g., FLACC, NIPS), behavioural distress indicators, and physiological measures (e.g., heart rate).
- Types of studies (T): included randomised clinical trials, observational cohort studies, and relevant guidelines.
2.1. Data Sources and Search Strategies
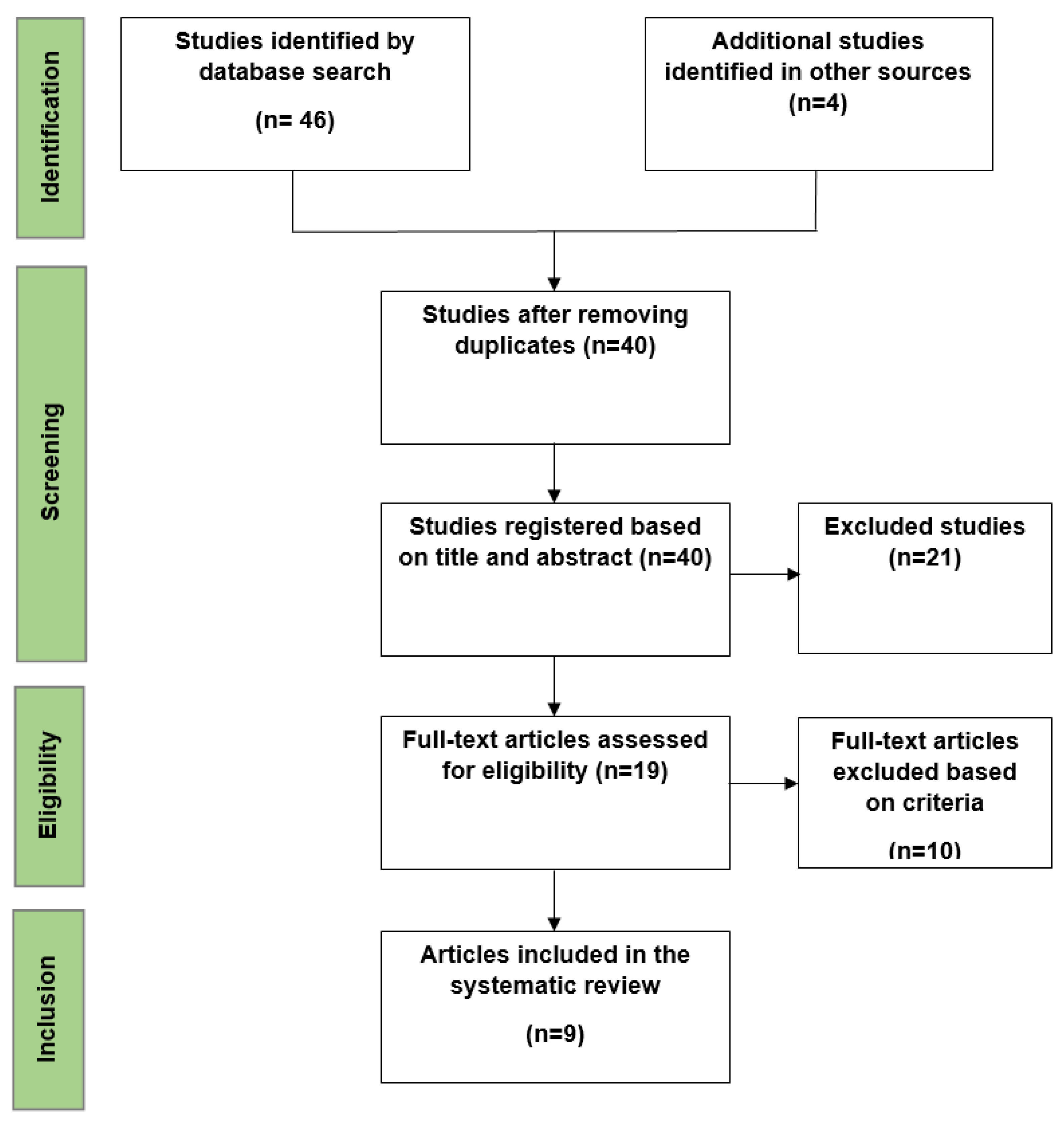
2.2. Study Selection
- Participants aged 0–12 months requiring intramuscular vaccination.
- Studies must involve lidocaine–prilocaine cream.
- Randomised controlled trials or comparative studies.
- Full-text articles published from 2000 to 2023.
2.3. Data Extraction
2.4. Data Analysis
3. Results
- Selected Studies
- Study Population
- Outcomes
4. Discussion
4.1. Applicability of Evidence
4.2. Concordances and Discordances
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kassab, M.; Hamadneh, S.; Nuseir, K.; ALmomani, B.; Hamadneh, J. Factors Associated With Infant Pain Severity Undergoing Immunization Injections. J. Pediatr. Nurs. 2018, 42, e85–e90. [Google Scholar] [CrossRef] [PubMed]
- Azoicai, D.; Barbacariu, C.L.; Barbacariu, I.C.; Branza, I.L.; Chitan, L.E.; Cioc, S.M. Indreptar de Vaccinare in Cabinetul Medicului de Familie, 2023rd ed.; Amaltea: Bucharest, Romania, 2023. [Google Scholar]
- Herdea, V.; Ghionaru, R.; Lungu, C.N.; Leibovitz, E.; Diaconescu, S. Vaccine Coverage in Children Younger Than 1 Year of Age during Periods of High Epidemiological Risk: Are We Preparing for New Outbreaks? Children 2022, 9, 1334. [Google Scholar] [CrossRef] [PubMed]
- Pop, T.L.; Burlea, M.; Falup-Pecurariu, O.; Borzan, C.; Gabor-Harosa, F.; Herdea, V.; Pop, C.F.; Rajka, D.; Ognean, M.L.; Căinap, S.S. Overview of the Pediatric Healthcare System in Romania. Turk. Pediatri. Arsivi. 2020, 55, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Pop, C.F.; Coblisan, P.; Capalna, L.; Panța, P.C.; Buzoianu, A.D.; Bocsan, I.C. Safety of Vaccination within First Year of Life-The Experience of One General Medicine Center. Children 2023, 10, 104. [Google Scholar] [CrossRef]
- Min, H.J.; Kim, Y.J. Analysis of Gluteal Subcutaneous and Muscle Thickness in Infants and Children for Application to Intramuscular Injection, Autologous Fat Grafting, and Gluteal Artery Perforator Flaps. Arch. Plast. Surg. 2018, 45, 550–556. [Google Scholar] [CrossRef]
- Polania Gutierrez, J.J.; Munakomi, S. Intramuscular Injection. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Mabbott, A.P.; Bedford, H. Pain Management in Infant Immunisation: A Cross-Sectional Survey of UK Primary Care Nurses. Prim. Health Care Res. Dev. 2023, 24, e71. [Google Scholar] [CrossRef]
- Taddio, A.; McMurtry, C.M.; Logeman, C.; Gudzak, V.; de Boer, A.; Constantin, K.; Lee, S.; Moline, R.; Uleryk, E.; Chera, T.; et al. Prevalence of Pain and Fear as Barriers to Vaccination in Children—Systematic Review and Meta-Analysis. Vaccine 2022, 40, 7526–7537. [Google Scholar] [CrossRef]
- Fahriani, M.; Anwar, S.; Yufika, A.; Bakhtiar, B.; Wardani, E.; Winardi, W.; Akel, K.B.; Wagner, A.L.; Harapan, H. Disruption of Childhood Vaccination during the COVID-19 Pandemic in Indonesia. Narra. J. 2021, 1, e7. [Google Scholar] [CrossRef]
- Taddio, A.; Shah, V.; Bucci, L.; MacDonald, N.E.; Wong, H.; Stephens, D. Effectiveness of a Hospital-Based Postnatal Parent Education Intervention about Pain Management during Infant Vaccination: A Randomized Controlled Trial. CMAJ Can. Med. Assoc. J. 2018, 190, E1245–E1252. [Google Scholar] [CrossRef]
- Eissler, A.B.; Stoffel, L.; Nelle, M.; Hahn, S.; Zwakhalen, S. Pain Responses in Preterm Infants and Parental Stress over Repeated Painful Procedures: A Randomized Pilot Trial. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2023, 36, 2183753. [Google Scholar] [CrossRef]
- The Long Life of Early Pain|Harvard Medical School. Available online: https://hms.harvard.edu/news/long-life-early-pain (accessed on 29 September 2024).
- Hatfield, L.A. Neonatal Pain: What’s Age Got to Do with It? Surg. Neurol. Int. 2014, 5, S479–S489. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Smith, E.M. Procedural Pain Management in Neonates, Infants and Children. Rev. Pain 2011, 5, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Nader, R. Age Related Differences in Infant Pain Expression and Parental Judgements of Pain Throughout the First Year of Life. Ph.D. Thesis, University of British Columbia, Vancouver, BC, Canada, 2005. [Google Scholar]
- Ullsten, A.; Campbell-Yeo, M.; Eriksson, M. Parent-Led Neonatal Pain Management-a Narrative Review and Update of Research and Practices. Front. Pain Res. 2024, 5, 1375868. [Google Scholar] [CrossRef] [PubMed]
- Piira, T.; Champion, G.D.; Bustos, T.; Donnelly, N.; Lui, K. Factors Associated with Infant Pain Response Following an Immunization Injection. Early Hum. Dev. 2007, 83, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Kagan, J. Temperament and the Reactions to Unfamiliarity. Child Dev. 1997, 68, 139–143. [Google Scholar] [CrossRef]
- Kagan, J. Temperamental and Theoretical Contributions to Clinical Psychology. Annu. Rev. Clin. Psychol. 2022, 18, 1–18. [Google Scholar] [CrossRef]
- McNair, C.; Fung, M.; Taddio, A.; Ipp, M.; Moss, S.; Baker, S.; Tolkin, J.; Dave, M.; Feerasta, S.; Govan, P.; et al. Parent-Led Interventions in Reducing Infant Vaccination Pain after Participation in a Longitudinal Randomized Control Trial. Paediatr. Child Health 2017, 22, 217–219. [Google Scholar] [CrossRef]
- Crellin, D.J.; Harrison, D.; Santamaria, N.; Huque, H.; Babl, F.E. The Psychometric Properties of the FLACC Scale Used to Assess Procedural Pain. J. Pain 2018, 19, 862–872. [Google Scholar] [CrossRef]
- Kucukoglu, S.; Celebioglu, A.; Caner, I.; Ok, G.; Maden, R. The Effects of Instrumental Touching on Infant Pain Perception and the Effects of Eutectic Mixture of Local Anesthetics (EMLA) on the Reduction of Pain. Iran. J. Pediatr. 2015, 25, e532. [Google Scholar] [CrossRef]
- Gupta, N.K.; Upadhyay, A.; Dwivedi, A.K.; Agarwal, A.; Jaiswal, V.; Singh, A. Randomized Controlled Trial of Topical EMLA and Vapocoolant Spray for Reducing Pain during wDPT Vaccination. World J. Pediatr. WJP 2017, 13, 236–241. [Google Scholar] [CrossRef]
- Crellin, D.J.; Harrison, D.; Hutchinson, A.; Schuster, T.; Santamaria, N.; Babl, F.E. Procedural Pain Scale Evaluation (PROPoSE) Study: Protocol for an Evaluation of the Psychometric Properties of Behavioural Pain Scales for the Assessment of Procedural Pain in Infants and Children Aged 6-42 Months. BMJ Open 2017, 7, e016225. [Google Scholar] [CrossRef] [PubMed]
- Altay, G.; Küçükoğlu, S. Effects of the Facilitated Tucking Position in Early Period on Physiological Parameters, Comfort and Breastfeeding Performance in Late Preterm Infants: A Randomized Controlled Trial. Midwifery 2022, 115, 103492. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.; Engle, S.; Jorgensen, J.; Kralik, A.; Whitman, K. Effects of Facilitated Tucking during Routine Care of Infants Born Preterm. Pediatr. Phys. Ther. Off. Publ. Sect. Pediatr. Am. Phys. Ther. Assoc. 2005, 17, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Vu-Ngoc, H.; Uyen, N.C.M.; Thinh, O.P.; Don, L.D.; Danh, N.V.T.; Truc, N.T.T.; Vi, V.T.; Vuong, N.L.; Huy, N.T.; Duong, P.D.T. Analgesic Effect of Non-Nutritive Sucking in Term Neonates: A Randomized Controlled Trial. Pediatr. Neonatol. 2020, 61, 106–113. [Google Scholar] [CrossRef]
- Shah, P.S.; Herbozo, C.; Aliwalas, L.L.; Shah, V.S. Breastfeeding or Breast Milk for Procedural Pain in Neonates. Cochrane Database Syst. Rev. 2012, 12, CD004950. [Google Scholar] [CrossRef]
- Sridharan, K.; Sivaramakrishnan, G. Pharmacological Interventions for Reducing Pain Related to Immunization or Intramuscular Injection in Children: A Mixed Treatment Comparison Network Meta-Analysis of Randomized Controlled Clinical Trials. J. Child Health Care Prof. Work. Child. Hosp. Community 2018, 22, 393–405. [Google Scholar] [CrossRef]
- Foster, J.P.; Taylor, C.; Spence, K. Topical Anaesthesia for Needle-Related Pain in Newborn Infants. Cochrane Database Syst. Rev. 2017, 2, CD010331. [Google Scholar] [CrossRef]
- Harrison, D.; Beggs, S.; Stevens, B. Sucrose for Procedural Pain Management in Infants. Pediatrics 2012, 130, 918–925. [Google Scholar] [CrossRef]
- Schweitzer-Chaput, A.; Callot, D.; Bouazza, N.; Lesage, F.; Oualha, M.; Paret, N.; Boyer-Gervoise, M.; Treluyer, J.-M.; Chouchana, L. Local Anesthetics Systemic Toxicity in Children: Analysis of the French Pharmacovigilance Database. BMC Pediatr. 2023, 23, 321. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Taddio, A.; Nulman, I.; Reid, E.; Shaw, J.; Koren, G. Effect of Lidocaine-Prilocaine Cream (EMLA®) on Pain of Intramuscular Fluzone® Injection. Can. J. Hosp. Pharm. 1992, 45. [Google Scholar] [CrossRef]
- Abuelkheir, M.; Alsourani, D.; Al-Eyadhy, A.; Temsah, M.-H.; Meo, S.A.; Alzamil, F. EMLA(R) Cream: A Pain-Relieving Strategy for Childhood Vaccination. J. Int. Med. Res. 2014, 42, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Halperin, B.A.; Halperin, S.A.; McGrath, P.; Smith, B.; Houston, T. Use of Lidocaine-Prilocaine Patch to Decrease Intramuscular Injection Pain Does Not Adversely Affect the Antibody Response to Diphtheria-Tetanus-Acellular Pertussis-Inactivated Poliovirus-Haemophilus Influenzae Type b Conjugate and Hepatitis B Vaccines in Infants from Birth to Six Months of Age. Pediatr. Infect. Dis. J. 2002, 21, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Lindh, V.; Wiklund, U.; Blomquist, H.K.; Håkansson, S. EMLA Cream and Oral Glucose for Immunization Pain in 3-Month-Old Infants. Pain 2003, 104, 381–388. [Google Scholar] [CrossRef]
- Dilli, D.; Küçük, I.G.; Dallar, Y. Interventions to Reduce Pain during Vaccination in Infancy. J. Pediatr. 2009, 154, 385–390. [Google Scholar] [CrossRef]
- Gupta, N.K.; Upadhyay, A.; Agarwal, A.; Goswami, G.; Kumar, J.; Sreenivas, V. Randomized Controlled Trial of Topical EMLA and Breastfeeding for Reducing Pain during wDPT Vaccination. Eur. J. Pediatr. 2013, 172, 1527–1533. [Google Scholar] [CrossRef]
- Basiri-Moghadam, M.; Kianmehr, M.; Pasban-Noghabi, S.; Basiri-Moghadam, K. Comparison of EMLA Cream with Rattles on Reducing Immunization Pain in Four Months Infants. JPMA J. Pak. Med. Assoc. 2014, 64, 874–878. [Google Scholar]
- Kumar, M.; Venkateshwar, V. A Study of Effect of Topical Anaesthetics on Injection Pain during Immunization in Infants. Int. J. Contemp. Pediatr. 2020, 7, 1463–1468. [Google Scholar] [CrossRef]
- Olsson Duse, B.; Sporrong, Y.; Bartocci, M.; Skoglund, K. Efficacy of Topical Lidocaine-prilocaine (EMLA®) for Management of Infant Pain during Pneumococcal Vaccination: A Randomized Controlled Trial. Paediatr. Neonatal Pain 2021, 4, 53–60. [Google Scholar] [CrossRef]
- Chapter 8: Assessing Risk of Bias in a Randomized Trial. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 30 October 2024).

{kind=link}
{kind=link}
| Type of Vaccine | Recommended Age |
|---|---|
| Hepatitis B vaccine (HB) | the first 24 h after birth |
| Diphtheria, Tetanus, Pertussis (acellular, component), Hepatitis B (rDNA), Poliomyelitis (inactivated) and Haemophilus Influenzae type B conjugate vaccine (adsorbed) (DTaP-IPV-HB-Hib) | 2, 4, 11 months |
| Pneumococcal polysaccharide 13-valent conjugate vaccine | 2, 4, 11 months |
| Measles, Mumps, and Rubella vaccine (MMR) | 12 months |
| Author, Year, Country | Population | Intervention | Comparator | Vaccine | Scale Used | Behavioural Indicators | Conclusions |
|---|---|---|---|---|---|---|---|
| Halperin BA. et al., 2002, Canada [37] | 153 infants aged between 0 and 6 months | EMLA cream patch (1 g 60–180 min before vaccination) | Patch with placebo cream | DTaP-IPV-Hib, Hepatitis B | MBPS | - | The highest statistically significant difference between pain scores was observed in infants aged 6 months. The group of patients aged 2–4 months was too small and no statistically significant differences between pain scores were identified. No difference was seen in 2-month-old infants. |
| Lindh V. et al., 2003, Sweden [38]. | 90 patients aged under 3 months | EMLA cream patch (1 g 60 min before vaccination) and glucose solution | Patch with placebo cream and water | DTaP | MBPS; VAS. | Presence of crying, latency to first cry, and total duration of crying. | Patients in the EMLA + glucose group had a significant reduction in pain scores, with less crying than in the placebo group, and crying started later and lasted less. |
| Dilli D. et al., 2008, Turkey [39]. | 14 patients aged between 6 and 12 months | Lidocaine–prilocaine cream (1 g 60 min before vaccination) | No intervention | Hepatitis B; MMR. | NIPS | Total duration of crying | The use of anaesthetic cream was much more effective than vaccination without any pre-applied intervention. |
| Gupta NK. et al., 2013, India [40]. | 60 patients aged under 3 months | EMLA cream patch (1 g 60 min before vaccination) and distilled water. | Placebo cream (Vaseline) and distilled water | DTaP | MFCS (modified NFCS scale) | Latency to first cry and total duration of crying. | The use of EMLA cream significantly reduced the pain score and total duration of crying in the group treated with it in combination with distilled water. The EMLA + breastfeeding group was not considered. |
| Basiri-Moghadam M. et al., 2014, Iran [41]. | 32 patients aged 4 months | EMLA cream (2 g 60 min before vaccination) | Rattle toy | Unspecified | Own scale, modified. | - | In the toy group, the pain was more severe than in the EMLA group. There was also a group that did not receive any intervention, and the pain score was significantly increased compared to the intervention groups. |
| Kucukoglu S. et al., 2015, Turkey [23]. | 75 patients aged 4 months | EMLA cream (0.5 g 30 min before vaccination) | Instrumental touch (placebo) | Hepatitis B | PIPP | - | The pain score in the EMLA group was lower than in the instrumental touch group. |
| Gupta NK. et al., 2017, India [24]. | 60 infants aged 3 months | EMLA cream (1 g 60 min before vaccination) and breastfeeding | Cooling spray with breastfeeding | DTaP | MFCS; NIPS. | Latency to first cry and total duration of crying. | The use of EMLA cream or cooling spray with breastfeeding reduced the pain score, but did not reduce the duration of crying. |
| Kumar M. et al., 2020, India [42]. | 150 patients aged between 6 weeks and 6 months | Lidocaine–prilocaine cream (no data regarding the dose, 60 min before vaccination) | Without intervention | Combined vaccine DTaP–HiB–Hepatitis B | MBPS | “The group that received the lidocaine–prilocaine cream had the lowest pain scores, followed by the groups that received other types of interventions, which were not included in our study”. | |
| Duse BO. et al., 2021, Sweden [43]. | 70 patients aged 3 months | EMLA cream (1 g 60 min before vaccination) | Placebo cream | Pneumococcal | FLACC; VAS. | Latency to first cry and total duration of crying. | “The use of EMLA cream significantly reduced pain during vaccination, increasing the latency to the first cry; however, no significant reduction in the total duration of crying was observed”. |
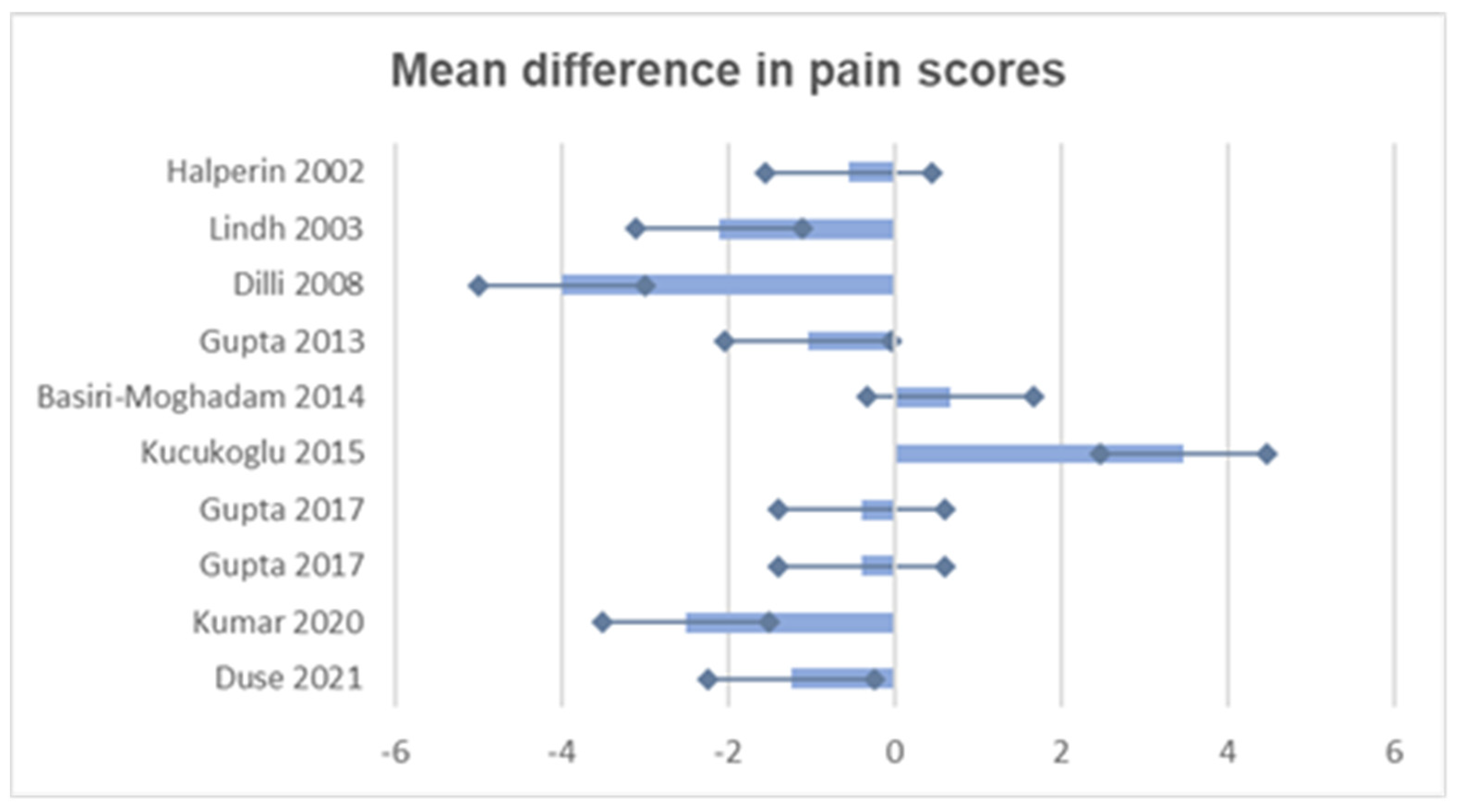
| Study | Mean Intervention (SD) | Mean Comparator (SD) | Mean Difference | Confidence Interval 95% | p Value |
|---|---|---|---|---|---|
| Halperin, 2002 [37] | 2.77 (0.335) | 3.33 (0.76) | −0.56 | (−0.88, −0.24) | 0.0029 |
| Lindh, 2003 [38] | 3.7 (1.8) | 5.8 (1.8) | −2.1 | (−3.5, −0.7) | 0.004 |
| Dilli, 2008 [39] | 2.0 (1.02) | 6.0 (0.51) | −4.0 | (−5.2, −2.8) | 0.001 |
| Gupta, 2013 [40] | 4.23 (2.66) | 5.26 (1.83) | −1.03 | (−2.08, 0.02) | 0.05 |
| Basiri-Moghadam, 2014 [41] | 4.87 (1.31) | 4.19 (1.94) | 0.68 | (−0.60, 1.96) | 0.27 |
| Kucukoglu, 2015 [23] | 9.6 (5.12) | 6.13 (5.97) | 3.47 | (1.54, 5.40) | 0.001 |
| Gupta, 2017 [24] | 1.4 (2.4) | 1.8 (2.5) | −0.4 | (−1.59, 0.79) | 0.05 |
| 1.9 (3.1) | 2.3 (3.0) | −0.4 | (−1.98, 1.18) | 0.05 | |
| Kumar, 2020 [42] | 4.1 (1.1) | 6.6 (0.9) | −2.5 | (−3.1, −1.9) | 0.0024 |
| Duse, 2021 [43] | 6.37 (2.22) | 7.62 (1.48) | −1.25 | (−2.11, −0.39) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, C.-F.; Coblișan, P.; Sas, V.; Drugă, C.; Cherecheș-Panța, P. Local Lidocaine–Prilocaine for Immunisation in Infants. Vaccines 2024, 12, 1329. https://doi.org/10.3390/vaccines12121329
Pop C-F, Coblișan P, Sas V, Drugă C, Cherecheș-Panța P. Local Lidocaine–Prilocaine for Immunisation in Infants. Vaccines. 2024; 12(12):1329. https://doi.org/10.3390/vaccines12121329
Chicago/Turabian StylePop, Claudia-Felicia, Petronela Coblișan, Valentina Sas, Cătălina Drugă, and Paraschiva Cherecheș-Panța. 2024. "Local Lidocaine–Prilocaine for Immunisation in Infants" Vaccines 12, no. 12: 1329. https://doi.org/10.3390/vaccines12121329
APA StylePop, C.-F., Coblișan, P., Sas, V., Drugă, C., & Cherecheș-Panța, P. (2024). Local Lidocaine–Prilocaine for Immunisation in Infants. Vaccines, 12(12), 1329. https://doi.org/10.3390/vaccines12121329