
Latent Class Analysis Identifies Distinct Phenotypes of Systemic Lupus Erythematosus Predictive of Flares after mRNA COVID-19 Vaccination: Results from the Coronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING)

 , ,
, ,  , , , , , ,
, , , , , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analyses
3. Results
3.1. Demographics and Clincal Characteristics of All SLE Patients
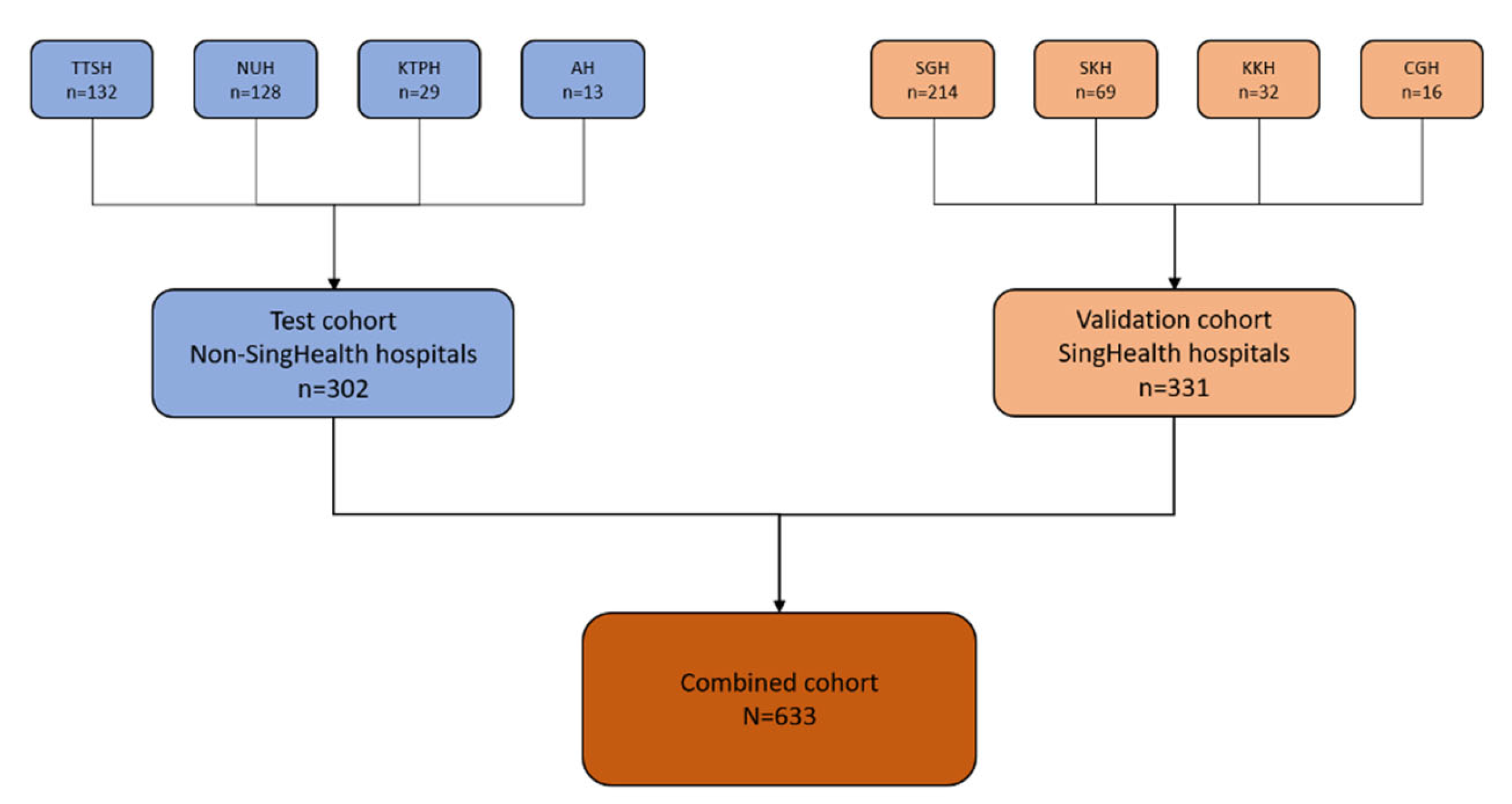
3.2. Test Cohort
3.3. Validation Cohort
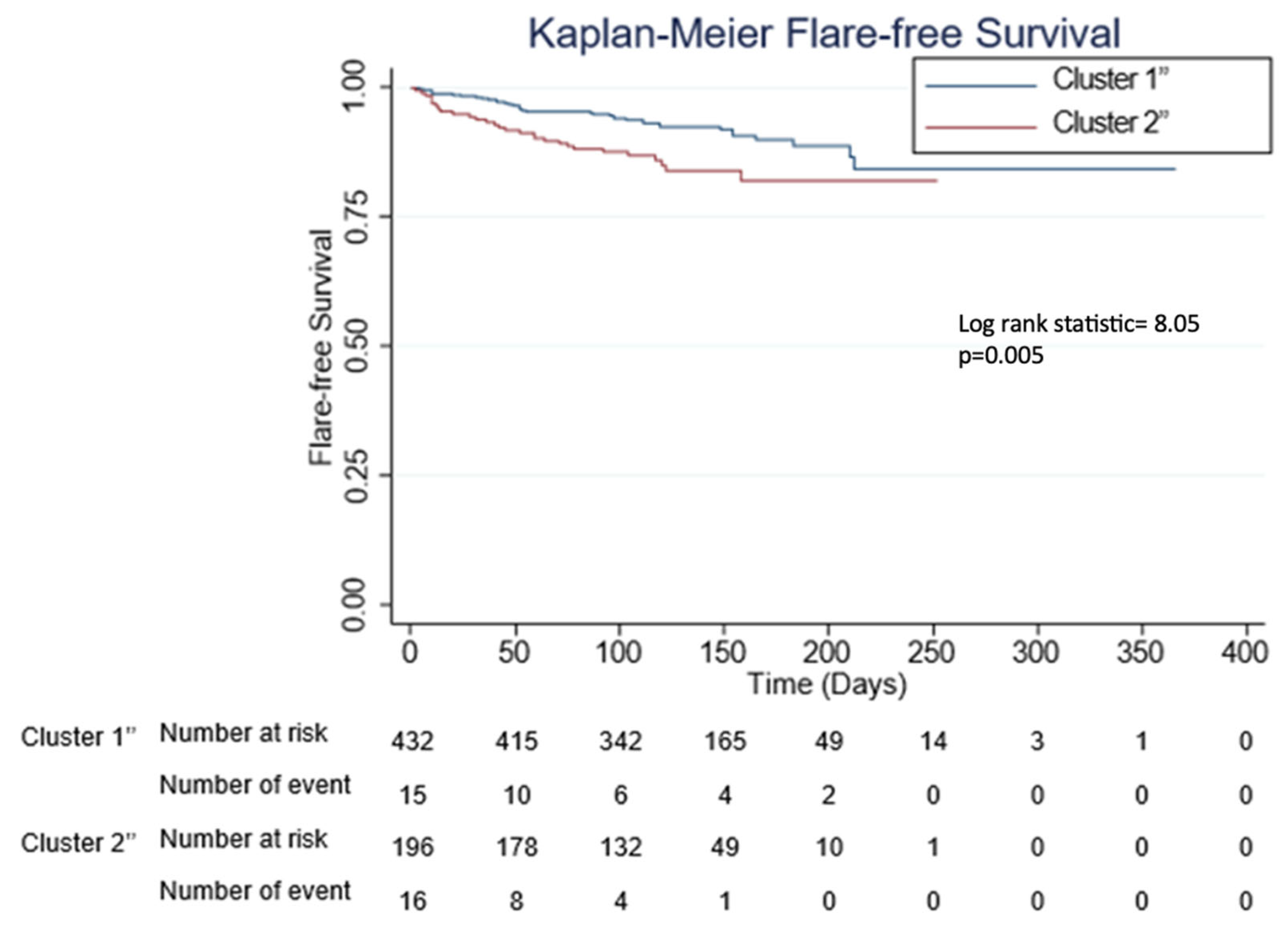
3.4. Cox Regression Analysis of SLE Flare-Free Survival in the Combined Cohort
3.5. Baseline Characteristics of the Major Ethnic Groups in the Combined Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sim, T.M.; Mak, A.; Tay, S.H. Insights into the Role of Neutrophils in Neuropsychiatric Systemic Lupus Erythematosus: Current Understanding and Future Directions. Front. Immunol. 2022, 13, 957303. [Google Scholar] [CrossRef] [PubMed]
- Ameer, M.A.; Chaudhry, H.; Mushtaq, J.; Khan, O.S.; Babar, M.; Hashim, T.; Zeb, S.; Tariq, M.A.; Patlolla, S.R.; Ali, J.; et al. An Overview of Systemic Lupus Erythematosus (Sle) Pathogenesis, Classification, and Management. Cureus 2022, 14, e30330. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Yi, Z.; Cai, R.; Chen, R.; Thong, B.Y.-H.; Mu, R. Clinical Outcomes of COVID-19 in Patients with Rheumatic Diseases: A Systematic Review and Meta-Analysis of Global Data. Autoimmun. Rev. 2021, 20, 102778. [Google Scholar] [CrossRef] [PubMed]
- Antinori, A.; Bausch-Jurken, M. The Burden of COVID-19 in the Immunocompromised Patient: Implications for Vaccination and Needs for the Future. J. Infect. Dis. 2023, 228, S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Shen, G.; Yang, H.; Huang, A.; Chen, X.; Dong, L.; Wu, B.; Zhang, A.; Su, L.; Hou, X. COVID-19 in Patients with Rheumatic Disease in Hubei Province, China: A Multicentre Retrospective Observational Study. Lancet Rheumatol. 2020, 2, e557–e564. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.L.; Qian, Y.; Jin, X.H.; Yu, H.R.; Du, L.; Wu, H.; Chen, H.L.; Shi, Y.Q. COVID-19 in Patients with Systemic Lupus Erythematosus: A Systematic Review. Lupus 2022, 31, 684–696. [Google Scholar] [CrossRef]
- Hou, X.; Zaks, T.; Langer, R.; Dong, Y. Lipid Nanoparticles for mRNA delivery. Nat. Rev. Mater. 2021, 6, 1078–1094. [Google Scholar] [CrossRef]
- Mok, C.C.; Chan, K.L.; Tse, S.M. Hesitancy for SARS-CoV-2 Vaccines and Post-Vaccination Flares in Patients with Systemic Lupus Erythematosus. Vaccine 2022, 40, 5959–5964. [Google Scholar] [CrossRef]
- Pappa, M.; Panagiotopoulos, A.; Thomas, K.; Fanouriakis, A. Systemic Lupus Erythematosus and COVID-19. Curr. Rheumatol. Rep. 2023, 25, 192–203. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-Onset Autoimmune Phenomena Post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef]
- Sim, T.M.; Ong, S.J.; Mak, A.; Tay, S.H. Type I Interferons in Systemic Lupus Erythematosus: A Journey from Bench to Bedside. Int. J. Mol. Sci. 2022, 23, 2505. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Marken, J.; Chen, J.; Tran, V.B.; Li, Q.-Z.; Li, M.; Cerosaletti, K.; Elkon, K.B.; Zeng, X.; Giltiay, N.V. High TLR7 Expression Drives the Expansion of CD19+ CD24hiCD38hi Transitional B Cells and Autoantibody Production in SLE Patients. Front. Immunol. 2019, 10, 1243. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.J.; Cañete, P.F.; Wang, H.; Medhavy, A.; Bones, J.; Roco, J.A.; He, Y.; Qin, Y.; Cappello, J.; Ellyard, J.I.; et al. TLR7 Gain-of-Function Genetic Variation Causes Human Lupus. Nature 2022, 605, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Teijaro, J.R.; Farber, D.L. COVID-19 Vaccines: Modes of Immune Activation and Future Challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lagniton, P.N.; Liu, Y.; Xu, R.-H. mRNA Vaccines for COVID-19: What, Why and How. Int. J. Biol. Sci. 2021, 17, 1446. [Google Scholar] [CrossRef] [PubMed]
- Coit, P.; Ruffalo, L.; Sawalha, A.H. Clinical Subgroup Clustering Analysis in a Systemic Lupus Erythematosus Cohort from Western Pennsylvania. Eur. J. Rheumatol. 2022, 9, 3. [Google Scholar] [CrossRef]
- Ma, M.; Santosa, A.; Fong, W.; Chew, L.-C.; Low, A.H.; Law, A.; Poh, Y.J.; Yeo, S.I.; Leung, Y.Y.; Ng, V.W. Post-mRNA Vaccine Flares in Autoimmune Inflammatory Rheumatic Diseases: Results from the COronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING). J. Autoimmun. 2023, 134, 102959. [Google Scholar] [CrossRef]
- Chessa, E.; Piga, M.; Floris, A.; Devilliers, H.; Cauli, A.; Arnaud, L. Use of Physician Global Assessment in Systemic Lupus Erythematosus: A Systematic Review of Its Psychometric Properties. Rheumatology 2020, 59, 3622–3632. [Google Scholar] [CrossRef]
- Arnaud, L.; Mertz, P.; Amoura, Z.; Voll, R.E.; Schwarting, A.; Maurier, F.; Blaison, G.; Bonnotte, B.; Poindron, V.; Fiehn, C. Patterns of Fatigue and Association with Disease Activity and Clinical Manifestations in Systemic Lupus Erythematosus. Rheumatology 2021, 60, 2672–2677. [Google Scholar] [CrossRef]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent Class Analysis: A Guide to best Practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Nakafero, G.; Grainge, M.J.; Card, T.; Mallen, C.D.; Nguyen Van-Tam, J.S.; Williams, H.C.; Abhishek, A. Is Vaccination against COVID-19 Associated with Autoimmune Rheumatic Disease Flare? A Self-Controlled Case Series Analysis. Rheumatology 2023, 62, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Grainger, R.; Kim, A.H.; Conway, R.; Yazdany, J.; Robinson, P.C. COVID-19 in People with Rheumatic Diseases: Risks, Outcomes, Treatment Considerations. Nat. Rev. Rheumatol. 2022, 18, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Rider, L.G.; Parks, C.G.; Wilkerson, J.; Schiffenbauer, A.I.; Kwok, R.K.; Noroozi Farhadi, P.; Nazir, S.; Ritter, R.; Sirotich, E.; Kennedy, K. Baseline Factors Associated with Self-Reported Disease Flares following COVID-19 Vaccination among Adults with Systemic Rheumatic Disease: Results from the COVID-19 Global Rheumatology Alliance Vaccine Survey. Rheumatology 2022, 61, SI143–SI150. [Google Scholar] [CrossRef]
- Lee, M.H.; Koh, J.W.H.; Ng, C.H.; Lim, S.H.; Cho, J.; Lateef, A.; Mak, A.; Tay, S.H. A Meta-Analysis of Clinical Manifestations in Asian Systemic Lupus Erythematous: The Effects of Ancestry, Ethnicity and Gender. Semin. Arthritis Rheum 2022, 52, 151932. [Google Scholar] [CrossRef] [PubMed]
- Barbhaiya, M.; Levine, J.M.; Siegel, C.H.; Bykerk, V.P.; Jannat-Khah, D.; Mandl, L.A. Adverse Events and Disease Flares after SARS-CoV-2 Vaccination in Patients with Systemic Lupus Erythematosus. Clin. Rheumatol. 2022, 41, 1619–1622. [Google Scholar] [CrossRef] [PubMed]
- Gerosa, M.; Schioppo, T.; Argolini, L.M.; Sciascia, S.; Ramirez, G.A.; Moroni, G.; Sinico, R.A.; Bonelli, G.; Alberici, F.; Mescia, F. The Impact of Anti-SARS-CoV-2 Vaccine in Patients with Systemic Lupus Erythematosus: A Multicentre Cohort Study. Vaccines 2022, 10, 663. [Google Scholar] [CrossRef]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Barbur, I.; Werbel, W.A.; Geetha, D.; Garonzik-Wang, J.M.; Segev, D.L.; Christopher-Stine, L.; Paik, J.J. Disease Flare and Reactogenicity in Patients with Rheumatic and Musculoskeletal Diseases following Two-Dose SARS-CoV-2 Messenger RNA Vaccination. Arthritis Rheumatol. 2022, 74, 28–32. [Google Scholar] [CrossRef]
- Sattui, S.E.; Liew, J.W.; Kennedy, K.; Sirotich, E.; Putman, M.; Moni, T.T.; Akpabio, A.; Alpízar-Rodríguez, D.; Berenbaum, F.; Bulina, I. Early Experience of COVID-19 Vaccination in Adults with Systemic Rheumatic Diseases: Results from the COVID-19 Global Rheumatology Alliance Vaccine Survey. RMD Open 2021, 7, e001814. [Google Scholar] [CrossRef]
- Machado, P.M.; Lawson-Tovey, S.; Strangfeld, A.; Mateus, E.F.; Hyrich, K.L.; Gossec, L.; Carmona, L.; Rodrigues, A.; Raffeiner, B.; Duarte, C. Safety of Vaccination against SARS-CoV-2 in People with Rheumatic and Musculoskeletal Diseases: Results from the EULAR Coronavirus Vaccine (COVAX) Physician-Reported Registry. Ann. Rheum. Dis. 2022, 81, 695–709. [Google Scholar] [CrossRef]
- Khanna, U.; Oprea, Y.; Mir, A.; Halverstam, C. New Diagnosis of Systemic Lupus Erythematosus after COVID-19 Vaccination: A Case Report and Review of Literature. JAAD Case Rep. 2022, 30, 30–34. [Google Scholar] [CrossRef]
- Nelson, M.C.; Rytting, H.; Greenbaum, L.A.; Goldberg, B. Presentation of SLE after COVID Vaccination in a Pediatric Patient. BMC Rheumatol. 2022, 6, 81. [Google Scholar] [CrossRef] [PubMed]
- Census of Population 2020 Statistical Release 1; Singapore Department of Statistics: Singapore, 2020.
- Shaharir, S.S.; Hussein, H.; Rajalingham, S.; Mohamed Said, M.S.; Abdul Gafor, A.H.; Mohd, R.; Mustafar, R. Damage in the Multiethnic Malaysian Systemic Lupus Erythematosus (SLE) Cohort: Comparison with Other Cohorts Worldwide. PLoS ONE 2016, 11, e0166270. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.H.; Tay, S.H.; Cheung, P.P.; Santosa, A.; Chan, Y.H.; Yip, J.W.; Mak, A.; Lahiri, M. Attitudes and Behaviors of Patients with Rheumatic Diseases during the Early Stages of the COVID-19 outbreak. J. Rheumatol. 2021, 48, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Alarcón, G.S. Lessons from LUMINA: A Multiethnic US Cohort; Sage Publications Sage: London, UK, 2008; Volume 17, pp. 971–976. [Google Scholar]
- Hasan, B.; Fike, A.; Hasni, S. Health Disparities in Systemic Lupus Erythematosus—A Narrative Review. Clin. Rheumatol. 2022, 41, 3299–3311. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 304. Cluster analysis. Singap. Med. J. 2005, 46, 153–159; quiz 160. [Google Scholar]
- Sen, P.; Lilleker, J.B.; Agarwal, V.; Kardes, S.; Milchert, M.; Gheita, T.; Salim, B.; Velikova, T.; Gracia-Ramos, A.E.; Parodis, I.; et al. Vaccine Hesitancy in Patients with Autoimmune Diseases: Data from the Coronavirus Disease-2019 Vaccination in Autoimmune Diseases Study. Indian. J. Rheumatol. 2022, 17, 188–191. [Google Scholar]
- Murdaca, G.; Orsi, A.; Spanò, F.; Puppo, F.; Durando, P.; Icardi, G.; Ansaldi, F. Influenza and Pneumococcal Vaccinations of Patients with Systemic Lupus Erythematosus: Current Views Upon Safety and Immunogenicity. Autoimmun. Rev. 2014, 13, 75–84. [Google Scholar] [CrossRef]
- Reşit, Y.; Tatiana, O.; David Alan, I. Approach to Vaccination in Systemic Lupus Erythematosus on Biological Treatment. Ann. Rheum. Dis. 2023, 82, 1123. [Google Scholar] [CrossRef]
- Mathian, A.; Pha, M.; Amoura, Z. Lupus and Vaccinations. Curr. Opin. Rheumatol. 2018, 30, 465–470. [Google Scholar] [CrossRef]
- Tzioufas, A.G.; Bakasis, A.-D.; Goules, A.V.; Bitzogli, K.; Cinoku, I.I.; Chatzis, L.G.; Argyropoulou, O.D.; Venetsanopoulou, A.I.; Mavrommati, M.; Stergiou, I.E. A Prospective Multicenter Study Assessing Humoral Immunogenicity and Safety of the mRNA SARS-CoV-2 Vaccines in Greek Patients with Systemic Autoimmune and Autoinflammatory Rheumatic Diseases. J. Autoimmun. 2021, 125, 102743. [Google Scholar] [CrossRef]
- Schiavoni, I.; Olivetta, E.; Natalucci, F.; Olivieri, G.; Lo Presti, A.; Fedele, G.; Stefanelli, P.; Ceccarelli, F.; Conti, F. Evidence of Immune Response to BNT162b2 COVID-19 Vaccine in Systemic Lupus Erythematosus Patients Treated with Belimumab. Lupus 2023, 32, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Geng, Y.; Wang, Y.; Deng, X.; Li, G.; Zhao, J.; Ji, L.; Zhang, X.; Song, Z.; Zhang, H. Safety and Disease Flare of Autoimmune Inflammatory Rheumatic Diseases: A Large Real-World Survey on Inactivated COVID-19 Vaccines. Ann. Rheum. Dis. 2022, 81, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Syversen, S.W.; Jyssum, I.; Tveter, A.T.; Sexton, J.; Christensen, I.E.; Tran, T.T.; Bjørlykke, K.H.; Mjaaland, S.; Warren, D.J.; Kvien, T.K. Immunogenicity and Safety of a Three-Dose SARS-CoV-2 Vaccination Strategy in Patients with Immune-Mediated Inflammatory Diseases on Immunosuppressive Therapy. RMD Open 2022, 8, e002417. [Google Scholar] [CrossRef] [PubMed]
- Moyon, Q.; Sterlin, D.; Miyara, M.; Anna, F.; Mathian, A.; Lhote, R.; Ghillani-Dalbin, P.; Breillat, P.; Mudumba, S.; de Alba, S. BNT162b2 Vaccine-Induced Humoral and Cellular Responses against SARS-CoV-2 Variants in Systemic Lupus Erythematosus. Ann. Rheum. Dis. 2022, 81, 575–583. [Google Scholar] [CrossRef]
- Barbhaiya, M.; Levine, J.M.; Bykerk, V.P.; Jannat-Khah, D.; Mandl, L.A. Systemic Rheumatic Disease Flares after SARS-CoV-2 Vaccination among Rheumatology Outpatients in New York City. Ann. Rheum. Dis. 2021, 80, 1352–1354. [Google Scholar] [CrossRef]
- Murdaca, G.; Noberasco, G.; Olobardi, D.; Lunardi, C.; Maule, M.; Delfino, L.; Triggiani, M.; Cardamone, C.; Benfaremo, D.; Moroncini, G.; et al. Current Take on Systemic Sclerosis Patients’ Vaccination Recommendations. Vaccines 2021, 9, 1426. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Combined Cohort (n = 633) | Test Cohort (n = 302) | Validation Cohort (n = 331) | ||
|---|---|---|---|---|
| Variables | n (%) or Median (IQR) | n (%) or Median (IQR) | n (%) or Median (IQR) | p-Value |
| Race | 0.424 | |||
| Chinese | 474 (74.9) | 235 (77.8%) | 239 (72.2%) | |
| Malay | 90 (14.2) | 38 (12.6%) | 52 (15.7%) | |
| Indian | 29 (4.6) | 13 (4.3%) | 16 (4.8%) | |
| Others | 40 (6.3) | 16 (5.3%) | 24 (7.3%) | |
| Age (years) | 52 (38–64) | 46 (32–60) | 58 (46–67) | <0.001 |
| Sex | ||||
| Male | 72 (11.4) | 39 (12.9%) | 33 (10.0%) | 0.244 |
| Vaccine type Pfizer/Biontech | 575 (90.8) | 282 (93.4%) | 293 (88.5%) | 0.034 |
| Moderna | 58 (9.2) | |||
| Previous COVID-19 infection | 10 (1.6) | 3 (1.0%) | 7 (2.1%) | 0.345 |
| Treatment interruption | 14 (2.2) | 0 (0.0%) | 14 (4.2%) | <0.001 |
| Disease activity | 0.007 | |||
| Remission | 329 (52.0) | 175 (57.9%) | 154 (46.5%) | |
| Low | 264 (41.7) | 114 (37.7%) | 150 (45.3%) | |
| Moderate | 36 (5.7) | 13 (4.3%) | 23 (6.9%) | |
| High | 4 (0.6) | 0 (0.0%) | 4 (1.2%) | |
| Baseline immunosuppression | ||||
| Prednisolone dose > 7.5 mg/day | 51 (8.1) | 17 (5.6%) | 34 (10.3%) | 0.032 |
| Hydroxychloroquine | 519 (82.0) | 236 (78.1%) | 283 (85.5%) | 0.016 |
| Mycophenolate mofetil | 155 (24.5) | 47 (15.6%) | 108 (32.6%) | <0.001 |
| Azathioprine | 85 (13.4) | 56 (18.5%) | 29 (8.8%) | <0.001 |
| Methotrexate | 35 (5.5) | 19 (6.3%) | 16 (4.8%) | 0.423 |
| Tacrolimus | 15 (2.4) | 6 (2.0%) | 9 (2.7%) | 0.545 |
| Cyclosporin | 13 (2.1) | 11 (3.6%) | 2 (0.6%) | 0.007 |
| Sulfasalazine | 9 (1.4) | 3 (1.0%) | 6 (1.8%) | 0.509 |
| Leflunomide | 2 (0.3) | 2 (0.7%) | 0 (0.0%) | 0.227 |
| Rituximab | 2 (0.3) | 0 (0.0%) | 2 (0.6%) | 0.500 |
| Cyclophosphamide | 1 (0.2) | 0 (0.0%) | 1 (0.3%) | 1.000 |
| Test Cohort (n = 302) | Validation Cohort (n = 331) | Combined Cohort (n = 633) | |||||||
|---|---|---|---|---|---|---|---|---|---|
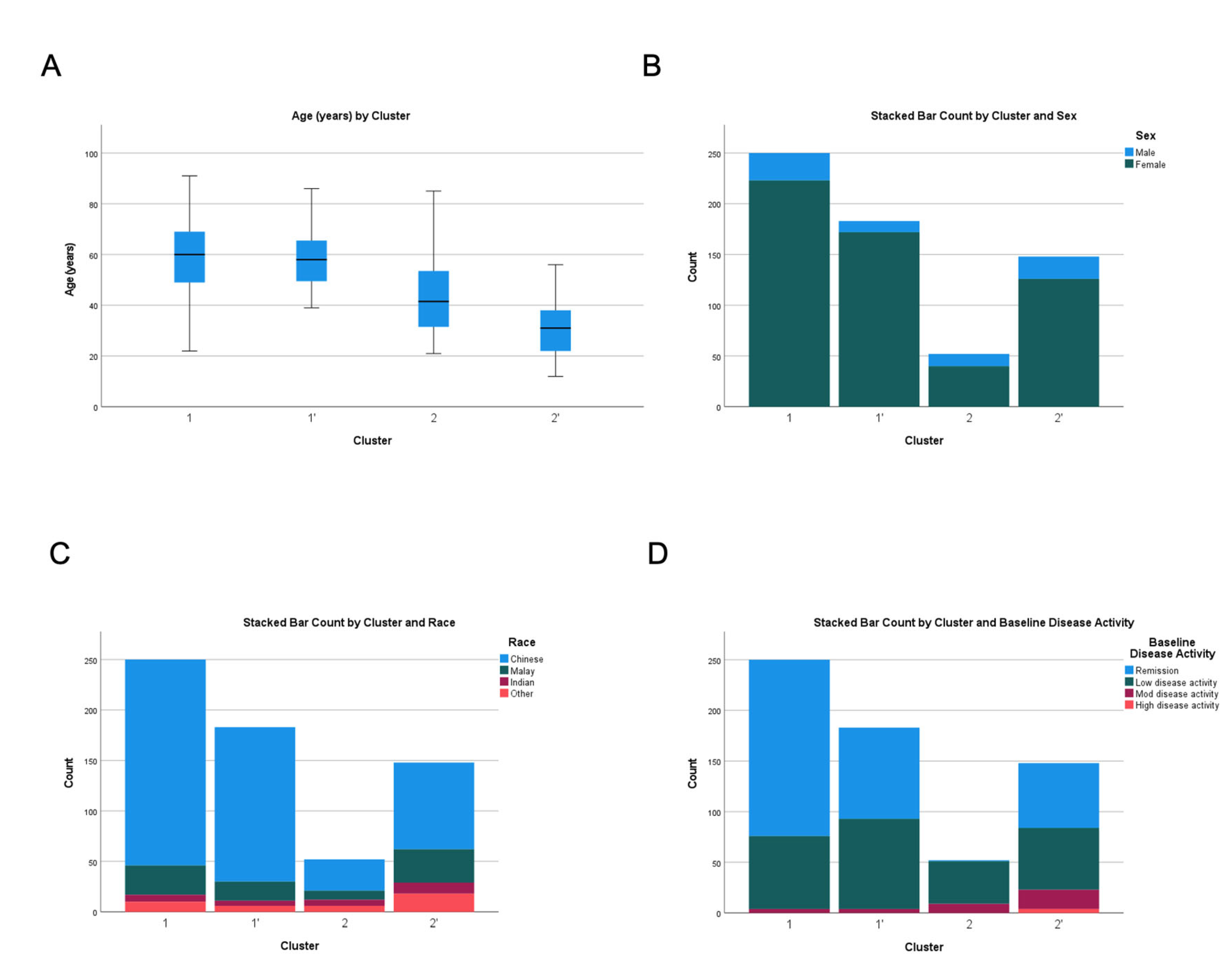
| Cluster | 1 n = 250 | 2 n = 52 | p Value | 1′ n = 183 | 2′ n = 148 | p Value | 1″ n = 435 | 2″ n = 198 | p Value |
| Variables | |||||||||
| Race | <0.001 | <0.001 | <0.001 | ||||||
| Chinese | 204 (81.6) | 31 (59.6) | 153 (83.6) | 86 (58.1) | 363 (83.5) | 111 (56.1) | |||
| Malay | 29 (11.6) | 9 (17.3) | 19 (10.4) | 33 (22.3) | 42 (9.7) | 48 (24.2) | |||
| Indian | 7 (2.8) | 6 (11.5) | 5 (2.7) | 11 (7.4) | 16 (3.7) | 13 (6.6) | |||
| Others | 10 (4.0) | 6 (11.5) | 6 (3.3) | 18 (12.2) | 14 (3.2) | 26 (13.1) | |||
| Age, median (IQR) | 60 | 41.5 | <0.001 | 58 | 31 | <0.001 | 60 | 31 | <0.001 |
| (49–69) | (31.5–53.5) | (49–66) | (22–38) | (51–67) | (24–38) | ||||
| Sex | 0.043 | ||||||||
| Male | 27 (10.8) | 12 (23.1) | 0.023 | 11 (6.0) | 22 (14.9) | 0.009 | 42 (9.7) | 30 (15.2) | |
| Vax type Pfizer/Biontech | 232 (92.8) | 50 (96.2) | 0.376 | 158 (86.3) | 135 (91.2) | 0.166 | 394 (90.6) | 181 (91.4) | 0.734 |
| Previous COVID-19 infection | 3 (1.2) | 0 (0.0) | 0.427 | 5 (2.7) | 2 (1.4) | 0.385 | 8 (1.8) | 2 (1.1) | 0.438 |
| Treatment interruption | 0 (0.0) | 0 (0.0) | - | 1 (0.6) | 13 (8.8) | <0.001 | 1 (0.2) | 13 (6.6) | <0.001 |
| Disease activity | <0.001 | <0.001 | <0.001 | ||||||
| Remission | 174 (69.6) | 1 (1.9) | 90 (49.2) | 64 (43.2) | 244 (56.1) | 85 (42.9) | |||
| Low | 72 (28.8) | 42 (80.8) | 89 (48.6) | 61 (41.2) | 175 (40.2) | 89 (45.0) | |||
| Moderate | 4 (1.6) | 9 (17.3) | 4 (2.2) | 19 (12.8) | 16 (3.7) | 20 (10.1) | |||
| High | 0 (0.0) | 0 (0.0) | 0 (0.0) | 4 (2.7) | 0 (0.0) | 4 (2.0) | |||
| Baseline immunosuppression | |||||||||
| Prednisolone dose > 7.5 mg/day | 4 (1.6) | 13 (25.0) | <0.001 | 2 (1.1) | 32 (21.6) | <0.001 | 12 (2.8) | 39 (19.7) | <0.001 |
| Hydroxychloroquine | 185 (74.0) | 51 (98.1) | <0.001 | 149 (81.4) | 134 (90.5) | 0.027 | 336 (77.2) | 183 (92.4) | <0.001 |
| Mycophenolate mofetil | 37 (14.8) | 10 (19.2) | 0.423 | 41 (22.4) | 67 (19.2) | <0.001 | 77 (17.7) | 78 (39.4) | <0.001 |
| Azathioprine | 47 (18.8) | 9 (17.3) | 0.801 | 14 (7.7) | 15 (45.3) | 0.427 | 59 (13.6) | 26 (13.1) | 0.883 |
| Methotrexate | 9 (3.6) | 10 (19.2) | <0.001 | 12 (6.6) | 4 (2.7) | 0.104 | 28 (6.4) | 7 (3.5) | 0.139 |
| Tacrolimus | 0 (0.0) | 6 (11.5) | <0.001 | 0 (0.0) | 9 (6.1) | 0.001 | 3 (0.7) | 12 (6.1) | <0.001 |
| Cyclosporin | 1 (0.4) | 10 (19.2) | <0.001 | 1 (0.6) | 1 (0.7) | 0.880 | 7 (1.6) | 6 (3.0) | 0.242 |
| Sulfasalazine | 1 (0.4) | 2 (3.8) | 0.078 | 2 (1.1) | 4 (2.7) | 0.275 | 3 (0.7) | 6 (3.0) | 0.030 |
| Leflunomide | 2 (0.8) | 0 (0.0) | 0.518 | 0 (0.0) | 0 (0.0) | - | 2 (0.5) | 0 (0.0) | 0.339 |
| Rituximab | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | 2 (1.4) | 0.115 | 0 (0.0) | 2 (1.1) | 0.098 |
| Cyclophosphamide | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | 1 (0.7) | 0.265 | 0 (0.0) | 1 (0.5) | 0.138 |
| Test Cohort (n = 302) | Validation Cohort (n = 331) | Combined Cohort (n = 633) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Cluster | 1 n = 250 | 2 n = 52 | p Value | 1′ n = 183 | 2′ n = 148 | p Value | 1″ n = 435 | 2″ n = 198 | p Value |
| Variables | |||||||||
| Flare | 19 (7.6) | 9 (17.3) | 0.036 | 17 (9.3) | 24 (16.2) | 0.066 | 39 (9.0) | 30 (15.2) | 0.021 |
| Organ system | |||||||||
| General | 3 (1.2) | 2 (3.8) | 0.206 | 1 (0.5) | 3 (2.0) | 0.328 | 5 (1.1) | 4 (2.0) | 0.471 |
| Haematological | 2 (0.8) | 3 (5.8) | 0.037 | 7 (3.8) | 8 (5.4) | 0.492 | 9 (2.1) | 11 (5.6) | 0.020 |
| Musculoskeletal | 11 (4.4) | 5 (9.6) | 0165 | 4 (2.2) | 8 (5.4) | 0.119 | 17 (3.9) | 11 (5.6) | 0.350 |
| Mucocutaneous | 3 (1.2) | 1 (1.9) | 0.532 | 3 (1.6) | 6 (4.1) | 0.308 | 7 (1.6) | 6 (3.0) | 0.242 |
| Cardiorespiratory | 1 (0.4) | 1 (1.9) | 0.315 | 1 (0.5) | 1 (0.7) | 1.000 | 2 (0.5) | 2 (1.0) | 0.593 |
| Renal | 1 (0.4) | 1 (1.9) | 0.315 | 7 (3.8) | 5 (3.4) | 0.829 | 8 (1.8) | 6 (3.0) | 0.385 |
| Gastrointestinal | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | 1 (0.7) | 0.447 | 0 (0.0) | 1 (0.5) | 0.313 |
| Vasculitis | 2 (0.8) | 0 (0.0) | 1.000 | 1 (0.5) | 1 (0.7) | 1.000 | 4 (0.9) | 0 (0.0) | 0.315 |
| Others | 1 (0.4) | 0 (0.0) | 1.000 | 1 (0.5) | 0 (0.0) | 1.000 | 2 (0.5) | 0 (0.0) | 1.000 |
| Flare severity | 0.034 | 0.020 | 0.022 | ||||||
| No flare | 231 (92.4) | 43 (82.7) | 165 (90.7) | 124 (83.8) | 395 (90.8) | 168 (84.5) | |||
| Mild/self-limiting | 7 (2.8) | 1 (1.9) | 2 (1.1) | 3 (2.0) | 10 (2.3) | 3 (1.5) | |||
| Mild/moderate | 10 (4.0) | 7 (13.5) | 14 (7.7) | 12 (8.1) | 24 (5.5) | 19 (9.6) | |||
| Severe | 2 (0.8) | 1 (1.9) | 1 (0.5%) | 9 (6.1) | 5 (1.2) | 8 (4.0) | |||
| Time to flare | 0.065 | 0.122 | 0.012 | ||||||
| Within 90 days after first dose | 10 (4.0) | 6 (11.8) | 11 (6.1) | 18 (12.2) | 22 (5.1) | 23 (11.7) | |||
| Beyond 90 days | 9 (3.6) | 2 (3.9) | 5 (2.8) | 5 (3.4) | 15 (3.5) | 6 (3.0) | |||
| No flare | 231 (92.4) | 43 (84.3) | 165 (91.2) | 124 (84.4) | 395 (91.4) | 168 (85.3) | |||
| Median time to flare | 59.0 (34.0–154.0) | 55.5 (21.0–96.8) | 0.449 | 52.5 (32.5–111.0) | 40.0 (12.0–75.0) | 0.217 | 53.0 (35.5–115.0) | 42.0 (12.5–76.5) | 0.072 |
| Incidence of flare per 1000 patient-month, (95% CI) | 5.4 (3.3–8.5) | 12.4 (5.7–23.5) | 0.036 | 6.7 (3.9–10.7) | 11.6 (7.4–17.2) | 0.066 | 6.4 (4.6–8.8) | 10.8 (7.3–15.4) | 0.021 |
| Hospital admission | 2 (0.8) | 1 (1.9) | 0.434 | 2 (1.1) | 7 (4.7) | 0.084 | 5 (1.1) | 7 (3.5) | 0.057 |
| Improved disease activity | 35 (14.0) | 10 (19.2) | 0.335 | 16 (8.7) | 11 (7.4) | 0.692 | 54 (12.4) | 18 (9.1) | 0.222 |
| Variables | Unadjusted | Adjusted * | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Cluster | ||||
| 1″ | 1.0 | 1.0 | ||
| 2″ | 2.0 (1.9–2.1) | <0.001 | 1.4 (1.1–1.9) | 0.014 |
| Chinese n = 474 (74.9%) | Malay n = 90 (14.2%) | Indian n = 29 (4.6%) | Others n = 40 (6.3%) | p Value | |
|---|---|---|---|---|---|
| Cluster distribution | <0.001 | ||||
| Cluster 1″ | 363 (76.6) | 42 (46.7) | 16 (55.2) | 14 (35.0) | |
| Cluster 2″ | 111 (23.4) | 48 (53.3) | 13 (44.8) | 26 (65.0) | |
| Age, median (IQR) | 55.0 (42.0–65.3) | 42.0 (27.8–62.3) | 49.0 (35.5–61.0) | 41.5 (32.3–50.1) | <0.001 |
| Sex Male | 56 (11.8) | 13 (14.4) | 2 (6.9) | 1 (2.5) | 0.200 |
| Vax type Pfizer/Biontech | 433 (91.4) | 82 (91.1) | 26 (89.7) | 34 (85.0) | 0.534 |
| Previous COVID-19 infection | 7 (1.5) | 2 (2.2) | 1 (3.4) | 0 (0.0) | 0.458 |
| Treatment interruption | 8 (1.7) | 5 (5.6) | 0 (0.0) | 1 (2.5) | 0.123 |
| Disease activity | 0.383 | ||||
| Remission | 252 (53.2) | 43 (47.8) | 12 (41.4) | 22 (55.0) | |
| Low | 194 (40.9) | 41 (45.6) | 15 (51.7) | 14 (35.0) | |
| Moderate | 26 (5.5) | 5 (5.6) | 1 (3.4) | 4 (10.0) | |
| High | 2 (0.4) | 1 (1.1) | 1 (3.4) | 0 (0.0) | |
| Baseline immunosuppression | |||||
| Prednisolone dose > 7.5 mg/day | 27 (5.7) | 16 (17.8) | 4 (13.8) | 4 (10.0) | 0.001 |
| Hydroxychloroquine | 388 (81.9) | 73 (81.1) | 25 (86.2) | 33 (82.5) | 0.938 |
| Mycophenolate mofetil | 116 (24.5) | 25 (27.8) | 3 (10.3) | 11 (27.5) | 0.277 |
| Azathioprine | 65 (13.7) | 16 (17.8) | 0 (0.0) | 4 (10.0) | 0.060 |
| Methotrexate | 25 (5.3) | 4 (4.4) | 4 (13.8) | 2 (5.0) | 0.278 |
| Tacrolimus | 8 (1.7) | 3 (3.3) | 0 (0.0) | 4 (10.0) | 0.021 |
| Cyclosporin | 10 (2.1) | 2 (2.2) | 1 (3.4) | 0 (0.0) | 0.713 |
| Sulfasalazine | 5 (1.1) | 1 (1.1) | 2 (6.9) | 1 (2.5) | 0.076 |
| Leflunomide | 2 (0.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Rituximab | 1 (0.2) | 1 (1.1) | 0 (0.0) | 0 (0.0) | 0.440 |
| Cyclophosphamide | 0 (0.0) | 1 (1.1) | 0 (0.0) | 0 (0.0) | 0.251 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, T.M.; Lahiri, M.; Ma, M.; Cheung, P.P.-M.; Mak, A.; Fong, W.; Angkodjojo, S.; Xu, C.; Kong, K.O.; Arkachaisri, T.; et al. Latent Class Analysis Identifies Distinct Phenotypes of Systemic Lupus Erythematosus Predictive of Flares after mRNA COVID-19 Vaccination: Results from the Coronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING). Vaccines 2024, 12, 29. https://doi.org/10.3390/vaccines12010029
Sim TM, Lahiri M, Ma M, Cheung PP-M, Mak A, Fong W, Angkodjojo S, Xu C, Kong KO, Arkachaisri T, et al. Latent Class Analysis Identifies Distinct Phenotypes of Systemic Lupus Erythematosus Predictive of Flares after mRNA COVID-19 Vaccination: Results from the Coronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING). Vaccines. 2024; 12(1):29. https://doi.org/10.3390/vaccines12010029
Chicago/Turabian StyleSim, Tao Ming, Manjari Lahiri, Margaret Ma, Peter Pak-Moon Cheung, Anselm Mak, Warren Fong, Stanley Angkodjojo, Chuanhui Xu, Kok Ooi Kong, Thaschawee Arkachaisri, and et al. 2024. "Latent Class Analysis Identifies Distinct Phenotypes of Systemic Lupus Erythematosus Predictive of Flares after mRNA COVID-19 Vaccination: Results from the Coronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING)" Vaccines 12, no. 1: 29. https://doi.org/10.3390/vaccines12010029
APA StyleSim, T. M., Lahiri, M., Ma, M., Cheung, P. P.-M., Mak, A., Fong, W., Angkodjojo, S., Xu, C., Kong, K. O., Arkachaisri, T., Phang, K. F., Tan, T. C., Yap, Q. V., Chan, Y. H., Sriranganathan, M., Chuah, T. Y., Roslan, N. E., Poh, Y. J., Law, A., ... Tay, S. H. (2024). Latent Class Analysis Identifies Distinct Phenotypes of Systemic Lupus Erythematosus Predictive of Flares after mRNA COVID-19 Vaccination: Results from the Coronavirus National Vaccine Registry for ImmuNe Diseases SINGapore (CONVIN-SING). Vaccines, 12(1), 29. https://doi.org/10.3390/vaccines12010029