
Effectiveness of Maternal Inactivated COVID-19 Vaccination against Omicron Infection in Infants during the First 12 Months of Life: A Test-Negative Case-Control Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
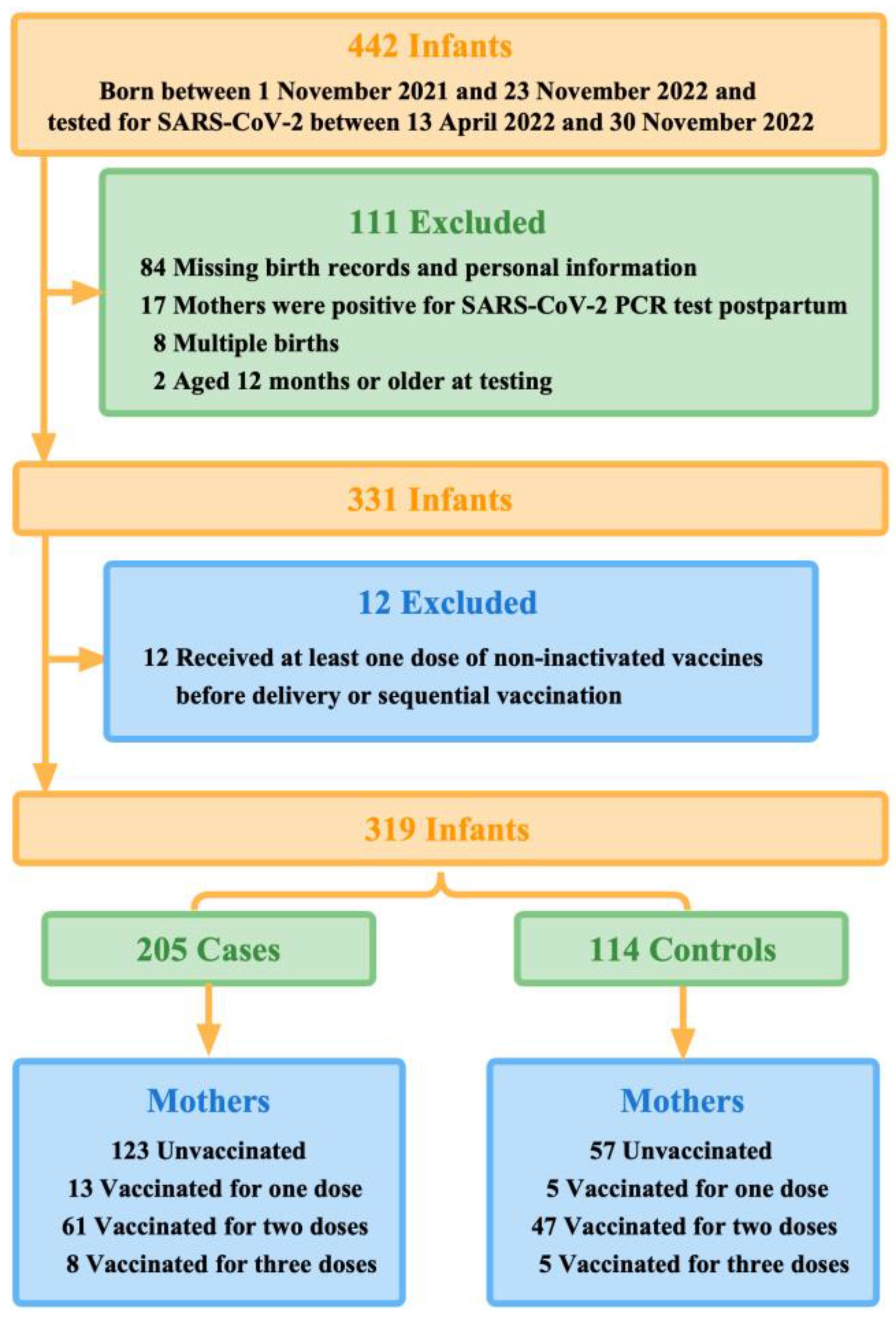
2.1. Study Design and Participants
2.2. Data Sources and Collection
2.3. Outcomes and Covariates
2.4. Power Analysis and Sample Size Calculation
2.5. Statistical Analysis
3. Results
3.1. Study Population
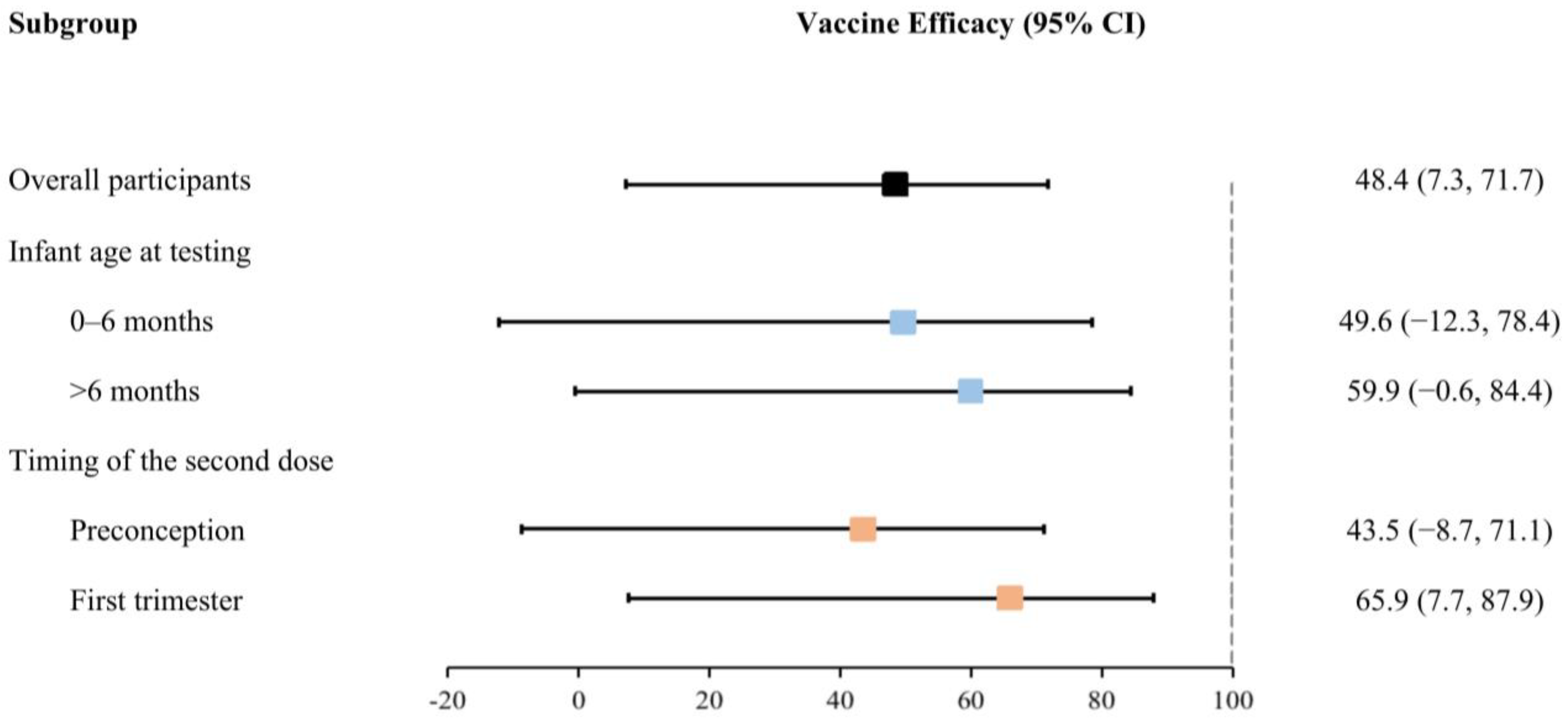
3.2. Vaccine Effectiveness for Maternal Full Vaccination
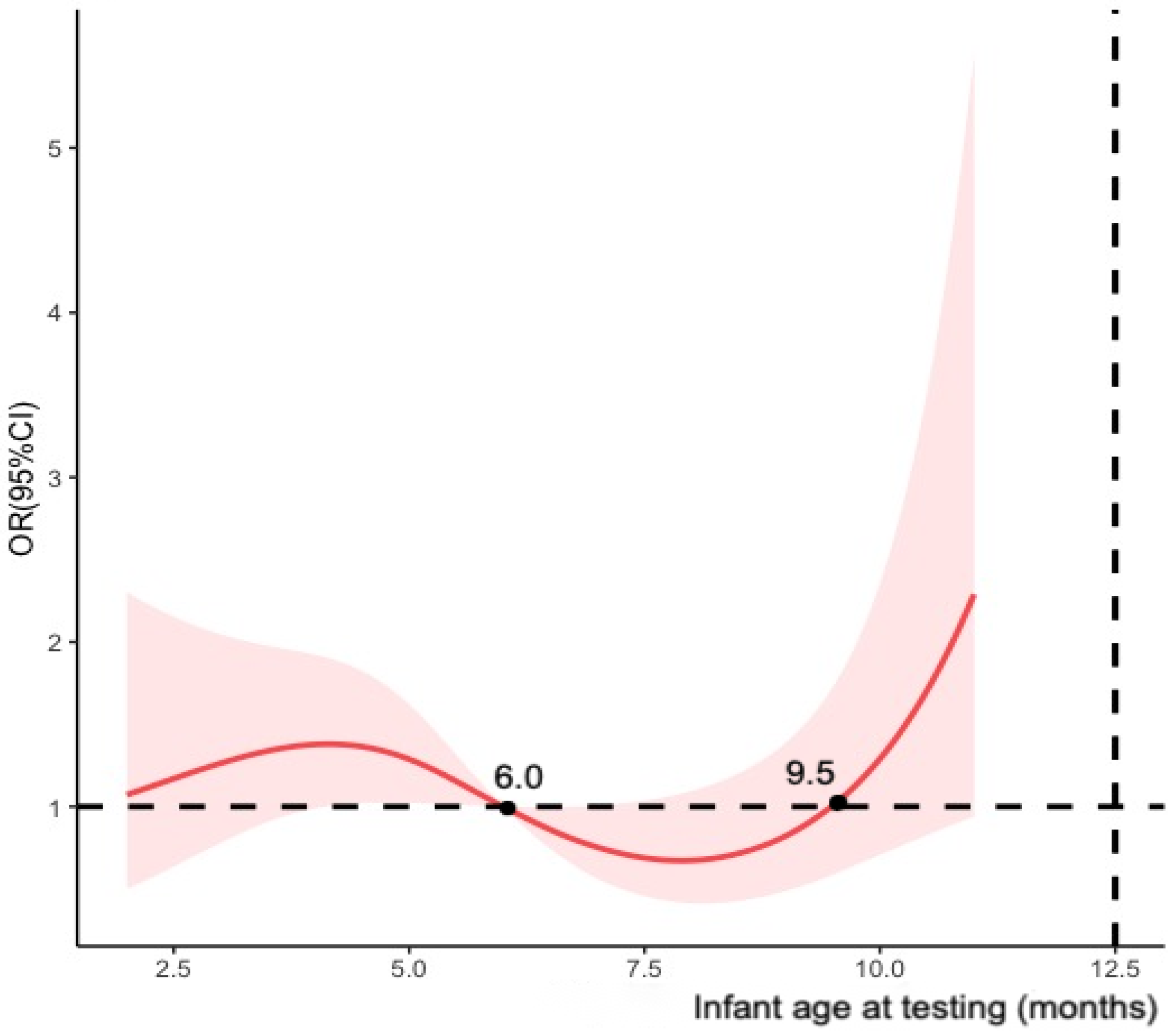
3.3. Additional Analysis and Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2020, 93, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.M.; Prata-Barbosa, A.; da Cunha, A.J.L.A. Update on SARS-CoV-2 infection in children. Paediatr. Int. Child Health 2021, 41, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Torjesen, I. COVID-19: Omicron variant is linked to steep rise in hospital admissions of very young children. BMJ 2022, 376, o110. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, S.C.J.; Hernandez, A.; Fell, D.B.; Austin, P.C.; D’souza, R.; Guttmann, A.; A Brown, K.; A Buchan, S.; Gubbay, J.B.; Nasreen, S.; et al. Maternal mRNA COVID-19 vaccination during pregnancy and delta or omicron infection or hospital admission in infants: Test negative design study. BMJ 2023, 380, e074035. [Google Scholar] [CrossRef]
- Liu, S.; Zhong, J.; Zhang, D. Transplacental Transfer of Maternal Antibody against SARS-CoV-2 and Its Influencing Factors: A Review. Vaccines 2022, 10, 1083. [Google Scholar] [CrossRef]
- Halasa, N.B.; Olson, S.M.; Staat, M.A.; Newhams, M.M.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Cameron, M.A.; Pannaraj, P.S.; Bline, K.E.; et al. Effectiveness of Maternal Vaccination with mRNA COVID-19 Vaccine During Pregnancy Against COVID-19-Associated Hospitalization in Infants Aged <6 Months—17 States, July 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 264–270. [Google Scholar]
- Male, V. SARS-CoV-2 infection and COVID-19 vaccination in pregnancy. Nat. Rev. Immunol. 2022, 22, 277–282. [Google Scholar] [CrossRef]
- Englund, J.; Glezen, W.P.; Piedra, P.A. Maternal immunization against viral disease. Vaccine 1998, 16, 1456–1463. [Google Scholar] [CrossRef]
- Benowitz, I.; Esposito, D.B.; Gracey, K.D.; Shapiro, E.D.; Vázquez, M. Influenza Vaccine Given to Pregnant Women Reduces Hospitalization Due to Influenza in Their Infants. Clin. Infect. Dis. 2010, 51, 1355–1361. [Google Scholar] [CrossRef]
- Madhi, S.A.; Polack, F.P.; Piedra, P.A.; Munoz, F.M.; Trenholme, A.A.; Simões, E.A.F.; Swamy, G.K.; Agrawal, S.; Ahmed, K.; August, A.; et al. Respiratory Syncytial Virus Vaccination during Pregnancy and Effects in Infants. N. Engl. J. Med. 2020, 383, 426–439. [Google Scholar] [CrossRef]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-neonatal transfer of SARS-CoV-2 immunoglobulin G antibodies among parturient women treated with BNT162b2 messenger RNA vaccine during pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100492. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg-Friedman, M.; Kigel, A.; Bahar, Y.; Werbner, M.; Alter, J.; Yogev, Y.; Dror, Y.; Lubetzky, R.; Dessau, M.; Gal-Tanamy, M.; et al. BNT162b2 mRNA vaccine elicited antibody response in blood and milk of breastfeeding women. Nat. Commun. 2021, 12, 6222. [Google Scholar] [CrossRef] [PubMed]
- Soysal, A.; Bilazer, C.; Gönüllü, E.; Barin, E.; Çivilibal, M. Cord blood antibody following maternal SARS-CoV-2 inactive vaccine (CoronaVac) administration during the pregnancy. Hum. Vaccin. Immunother. 2021, 17, 3484–3486. [Google Scholar] [CrossRef] [PubMed]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef]
- Shook, L.L.; Atyeo, C.G.; Yonker, L.M.; Fasano, A.; Gray, K.J.; Alter, G.; Edlow, A.G. Durability of Anti-Spike Antibodies in Infants After Maternal COVID-19 Vaccination or Natural Infection. JAMA 2022, 327, 1087–1089. [Google Scholar] [CrossRef]
- Kugelman, N.; Nahshon, C.; Shaked-Mishan, P.; Cohen, N.; Sher, M.L.; Gruber, M.; Marom, I.; Zolotarevsky, A.; Lavie, O.; Damti, A.; et al. Maternal and Neonatal SARS-CoV-2 Immunoglobulin G Antibody Levels at Delivery After Receipt of the BNT162b2 Messenger RNA COVID-19 Vaccine During the Second Trimester of Pregnancy. JAMA Pediatr. 2022, 176, 290–295. [Google Scholar] [CrossRef]
- Kashani-Ligumsky, L.; Lopian, M.; Cohen, R.; Senderovich, H.; Czeiger, S.; Halperin, A.; Chaim, A.B.; Kremer, I.; Lessing, J.B.; Somekh, E.; et al. Titers of SARS CoV-2 antibodies in cord blood of neonates whose mothers contracted SARS CoV-2 (COVID-19) during pregnancy and in those whose mothers were vaccinated with mRNA to SARS CoV-2 during pregnancy. J. Perinatol. 2021, 41, 2621–2624. [Google Scholar] [CrossRef]
- Fell, D.B.; Dimitris, M.C.; Hutcheon, J.A.; Ortiz, J.R.; Platt, R.W.; Regan, A.K.; Savitz, D.A. Guidance for design and analysis of observational studies of fetal and newborn outcomes following COVID-19 vaccination during pregnancy. Vaccine 2021, 39, 1882–1886. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association Between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 326, 728–735. [Google Scholar] [CrossRef]
- Tormen, M.; Taliento, C.; Salvioli, S.; Piccolotti, I.; Scutiero, G.; Cappadona, R.; Greco, P. Effectiveness and safety of COVID-19 vaccine in pregnant women: A systematic review with meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2022, 130, 348–357. [Google Scholar] [CrossRef]
- Fell, D.B.; Dimanlig-Cruz, S.; Regan, A.K.; Håberg, S.E.; Gravel, C.A.; Oakley, L.; Alton, G.D.; Török, E.; Dhinsa, T.; Shah, P.S.; et al. Risk of preterm birth, small for gestational age at birth, and stillbirth after COVID-19 vaccination during pregnancy: Population based retrospective cohort study. BMJ 2022, 378, e071416. [Google Scholar] [CrossRef] [PubMed]
- Fell, D.B.; Dhinsa, T.; Alton, G.D.; Török, E.; Dimanlig-Cruz, S.; Regan, A.K.; Sprague, A.E.; Buchan, S.A.; Kwong, J.C.; Wilson, S.E.; et al. Association of COVID-19 Vaccination in Pregnancy with Adverse Peripartum Outcomes. JAMA 2022, 327, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, E.O.; Haapala, J.; DeSilva, M.; Vazquez-Benitez, G.; Vesco, K.K.; Naleway, A.L.; Lipkind, H.S. Spontaneous Abortion Following COVID-19 Vaccination During Pregnancy. JAMA 2021, 326, 1629–1631. [Google Scholar] [CrossRef] [PubMed]
- Kugelman, N.; Nahshon, C.; Shaked-Mishan, P.; Cohen, N.; Lahav Sher, M.; Barsha, H.; Shalabna, E.; Zolotarevsky, A.; Lavie, O.; Kedar, R.; et al. Third trimester messenger RNA COVID-19 booster vaccination upsurge maternal and neonatal SARS-CoV-2 immunoglobulin G antibody levels at birth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 274, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Zdanowski, W.; Waśniewski, T. Evaluation of SARS-CoV-2 Spike Protein Antibody Titers in Cord Blood after COVID-19 Vaccination during Pregnancy in Polish Healthcare Workers: Preliminary Results. Vaccines 2021, 9, 675. [Google Scholar] [CrossRef]
- Zerbo, O.; Ray, G.T.; Fireman, B.; Layefsky, E.; Goddard, K.; Lewis, E.; Ross, P.; Omer, S.; Greenberg, M.; Klein, N.P. Maternal SARS-CoV-2 vaccination and infant protection against SARS-CoV-2 during the first six months of life. Nat. Commun. 2023, 14, 894. [Google Scholar] [CrossRef]
- Carlsen, E.Ø.; Magnus, M.C.; Oakley, L.; Fell, D.B.; Greve-Isdahl, M.; Kinge, J.M.; Håberg, S.E. Association of COVID-19 Vaccination During Pregnancy with Incidence of SARS-CoV-2 Infection in Infants. JAMA Intern. Med. 2022, 182, 825–831. [Google Scholar] [CrossRef]
- Halasa, N.B.; Olson, S.M.; Staat, M.A.; Newhams, M.M.; Price, A.M.; Pannaraj, P.S.; Boom, J.A.; Sahni, L.C.; Chiotos, K.; Cameron, M.A.; et al. Maternal Vaccination and Risk of Hospitalization for COVID-19 among Infants. N. Engl. J. Med. 2022, 387, 109–119. [Google Scholar] [CrossRef]
- Danino, D.; Ashkenazi-Hoffnung, L.; Diaz, A.; Erps, A.D.; Eliakim-Raz, N.; Avni, Y.S.; Greenberg, D.; Givon-Lavi, N.; Youngster, I. Effectiveness of BNT162b2 Vaccination During Pregnancy in Preventing Hospitalization for Severe Acute Respiratory Syndrome Coronavirus 2 in Infants. J. Pediatr. 2023, 254, 48–53.e1. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Infants Tested for SARS-CoV-2 | Maternal COVID-19 Vaccination Status | ||||||
|---|---|---|---|---|---|---|---|---|
| Case (n = 205) (%) | Control (n = 114) (%) | p-Value (Effect Size) | Unvaccinated 1 (n = 180) (%) | Partially 2 (n = 18) (%) | Fully 3 (n = 108) (%) | Booster 4 (n = 13) (%) | p-Value (Effect Size) | |
| Infant sex, female | 91 (44.4) | 59 (51.8) | 0.252 (0.18) | 93 (51.7) | 4 (22.2) | 48 (44.4) | 5 (38.5) | 0.083 (0.23) |
| Infant age at testing (months), median (interquartile range) | 6.00 (4.00, 10.00) | 7.00 (4.00, 9.00) | 0.764 (0.38) | 9.00 (5.75, 10.00) | 7.50 (5.25, 9.00) | 4.00 (3.00, 6.00) | 1.00 (1.00, 2.00) | <0.001 a (0.27) |
| Infant’s age category (months) | 0.428 (0.18) | <0.001 (0.21) | ||||||
| 0–6 | 108 (52.7) | 54 (47.4) | 57 (31.7) | 7 (38.9) | 85 (78.7) | 13 (1.0) | ||
| >6 | 97 (47.3) | 60 (52.6) | 123 (68.3) | 11 (61.1) | 23 (21.3) | 0 (0.0) | ||
| Symptoms of confirmed cases | - | 0.825 b (0.37) | ||||||
| Fever | 84 (41.0) | - | 41 (22.8) | 8 (44.4) | 33 (30.6) | 2 (15.4) | ||
| Cough | 22 (10.7) | - | 13 (7.2) | 1 (5.6) | 8 (7.4) | 0 (0.0) | ||
| Classification of cases | - | 0.007 b (0.26) | ||||||
| Mild | 112 (54.6) | - | 56 (31.1) | 9(50.0) | 43 (39.8) | 4 (30.8) | ||
| Asymptomatic | 93 (45.4) | - | 67 (37.2) | 4 (22.2) | 18 (16.7) | 4 (30.8) | ||
| Admission to hospital related to COVID-19 | 14 (6.8) | - | - | 3 (1.7) | 3 (16.7) | 7 (6.5) | 1 (7.7) | - |
| Mother’s age at birth (years), mean (standard deviations) | 31.20 (5.04) | 32.86 (4.83) | 0.004 (0.33) | 31.54 (5.16) | 30.72 (4.89) | 32.19 (4.68) | 33.54 (5.90) | 0.320 (0.21) |
| Mother’s age category (years) | 0.017 (0.20) | 0.283 b (0.23) | ||||||
| ≤24 | 13 (6.3) | 4 (3.5) | 14 (7.8) | 1 (5.6) | 2 (1.9) | 0 (0.0) | ||
| 25–34 | 143 (69.8) | 66 (57.9) | 115 (63.9) | 13 (72.2) | 74 (68.5) | 7 (53.8) | ||
| 35–46 | 49 (23.9) | 44 (38.6) | 51 (28.3) | 4 (22.2) | 32 (29.6) | 6 (46.2) | ||
| Timing of full vaccination received before delivery | 0.247 b (0.34) | - | ||||||
| Two doses all received before pregnancy | 52 (25.4) | 36 (31.6) | 0 (0.0) | 0 (0.0) | 88 (81.5) | 0 (0.0) | ||
| One dose before pregnancy and one dose during pregnancy | 6 (2.9) | 4 (3.5) | 0 (0.0) | 0 (0.0) | 10 (9.3) | 0 (0.0) | ||
| Two doses all received during pregnancy | 3 (1.5) | 7 (6.1) | 0 (0.0) | 0 (0.0) | 10 (9.3) | 0 (0.0) | ||
| Manufacturers of maternal vaccination dose 1 and 2 | 0.568 (0.32) | - | ||||||
| CNBG-CNBG 5 | 18 (8.8) | 10 (8.8) | 0 (0.0) | 0 (0.0) | 26 (24.1) | 2 (15.4) | ||
| Sinovac R&D-Sinovac R&D 5 | 31 (15.1) | 23 (20.2) | 0 (0.0) | 0 (0.0) | 47 (43.5) | 7 (53.8) | ||
| Heterologous 6 | 20 (9.8) | 19 (16.7) | 0 (0.0) | 0 (0.0) | 35 (32.4) | 4 (30.8) | ||
| Timing of maternal vaccination | ||||||||
| First dose | 0.237 b (0.30) | - | ||||||
| Preconception | 71 (34.6) | 45 (39.5) | 0 (0.0) | 5 (27.8) | 98 (90.7) | 13 (100.0) | ||
| First trimester | 10 (4.9) | 12 (10.5) | 0 (0.0) | 13 (72.2) | 9 (8.3) | 0 (0.0) | ||
| Second trimester | 1 (0.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.9) | 0 (0.0) | ||
| Second dose | 0.207 b (0.32) | - | ||||||
| Preconception | 60 (29.3) | 41 (36.0) | 0 (0.0) | 0 (0.0) | 88 (81.5) | 13 (100.0) | ||
| First trimester | 8 (3.9) | 11 (9.6) | 0 (0.0) | 0 (0.0) | 19 (17.6) | 0 (0.0) | ||
| Second trimester | 1 (0.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.9) | 0 (0.0) | ||
| Third dose | 0.005 b (0.90) | - | ||||||
| Preconception | 7 (3.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 7 (53.8) | ||
| First trimester | 1 (0.5) | 5 (4.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 6 (46.2) | ||
| Interval between doses 1 and 2 | 0.261 b (0.32) | - | ||||||
| 21–34 days | 51 (24.9) | 35 (30.7) | 0 (0.0) | 0 (0.0) | 76 (70.4) | 10 (76.9) | ||
| 35–55 days | 17 (8.3) | 13 (11.4) | 0 (0.0) | 0 (0.0) | 27 (25.0) | 3 (23.1) | ||
| ≥56 days | 1 (0.5) | 4 (3.5) | 0 (0.0) | 0 (0.0) | 5 (4.6) | 0 (0.0) | ||
| Interval between doses 2 and 3 | 0.103 b (0.90) | - | ||||||
| 180–193 days | 6 (2.9) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 7 (53.8) | ||
| ≥194 days | 2 (1.0) | 4 (3.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 6 (46.2) | ||
| Infants in Case Group (n = 205) (%) | Infants in Control Group (n = 114) (%) | p-Value | Adjusted Odds Ratio (OR) 1 and 95% Confidence Interval (95% CI) | Adjusted Effectiveness of Full Vaccination 1 (95% CI) | |
|---|---|---|---|---|---|
| Overall participants | 0.028 | ||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Received full vaccination 3 | 61 (29.8) | 47 (41.2) | 0.516 (0.283, 0.927) | 48.4 (7.3, 71.7) | |
| Infant age at testing | |||||
| 0–6 months | 0.101 | ||||
| Unvaccinated 2 | 43 (21.0) | 14 (12.3) | Reference | Reference | |
| Received full vaccination 3 | 51 (24.9) | 34 (29.8) | 0.504 (0.216, 1.123) | 49.6 (−12.3, 78.4) | |
| >6 months | 0.053 | ||||
| Unvaccinated 2 | 80 (39.0) | 43 (37.7) | Reference | Reference | |
| Received full vaccination 3 | 10 (4.9) | 13 (11.4) | 0.401 (0.156, 1.006) | 59.9 (−0.6, 84.4) | |
| Timing of the second dose | |||||
| Preconception | 0.090 | ||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Received full vaccination 3 | 52 (25.4) | 36 (31.6) | 0.565 (0.289, 1.087) | 43.5 (−8.7, 71.1) | |
| First trimester | 0.035 | ||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Received full vaccination 3 | 8 (3.9) | 11 (9.6) | 0.341 (0.121, 0.923) | 65.9 (7.7, 87.9) | |
| Second trimester | - | ||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Received full vaccination 3 | 1 (0.5) | 0 (0.0) | - | - |
| Infants in Case Group (n = 205) (%) | Infants in Control Group (n = 114) (%) | p-Value | Adjusted Odds Ratio (OR) 1 and 95% Confidence Interval (95% CI) | Adjusted Effectiveness of Maternal Vaccination 1 (95% CI) | |
|---|---|---|---|---|---|
| Overall participants | |||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Received partial vaccination 3 | 13 (6.3) | 5 (4.4) | 0.955 | 0.969 (0.329, 3.247) | 3.1 (−224.7, 67.1) |
| Received booster vaccination 4 | 8 (3.9) | 5 (4.4) | 0.683 | 0.753 (0.195, 3.089) | 24.7 (−208.9, 80.5) |
| Timing of full vaccination 5 received before delivery | |||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Two doses all received before pregnancy | 52 (25.4) | 36 (31.6) | 0.090 | 0.565 (0.289, 1.087) | 43.5 (−8.7, 71.1) |
| One dose before pregnancy and one dose during pregnancy | 6 (2.9) | 4 (3.5) | 0.644 | 0.726 (0.190, 3.070) | 27.4 (−207.0, 81.0) |
| Two doses all received during pregnancy | 3 (1.5) | 7 (6.1) | 0.042 | 0.229 (0.047, 0.889) | 77.1 (11.1, 95.3) |
| Timing of booster vaccination 4 received before delivery | |||||
| Unvaccinated 2 | 123 (60.0) | 57 (50.0) | Reference | Reference | |
| Three doses all received before pregnancy | 7 (3.4) | 0 (0.0) | - | - | - |
| Two doses before pregnancy and only booster dose during pregnancy | 1 (0.5) | 5 (4.4) | 0.031 | 0.082 (0.004, 0.589) | 91.8 (41.1, 99.6) |
| Case Infants | Control Infants | Adjusted OR 1 | Effectiveness of Full Vaccination 1 | |
|---|---|---|---|---|
| No. Vaccinated Mothers/Total No. (%) | (95% Confidence Interval) | % (95% Confidence Interval) | ||
| Model 1 2 | 70/222 (31.5) | 47/114 (41.2) | 0.561 (0.311, 1.000) | 43.9 (0.0, 68.9) |
| Model 2 3 | 61/188 (32.4) | 47/87 (54.0) | 0.350 (0.181, 0.660) | 65.0 (34.0, 81.9) |
| Model 3 4 | 54/191 (28.3) | 47/114 (41.2) | 0.475 (0.259, 0.858) | 52.5 (14.2, 74.1) |
| Model 4 5 | 54/191 (28.3) | 42/102 (41.2) | 0.481 (0.253, 0.897) | 51.9 (10.3, 74.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, J.; Wang, W.; Liu, S.; Chen, Y.; Xiong, H.; Meng, X.; Zhang, D.; Ma, Y. Effectiveness of Maternal Inactivated COVID-19 Vaccination against Omicron Infection in Infants during the First 12 Months of Life: A Test-Negative Case-Control Study. Vaccines 2023, 11, 1402. https://doi.org/10.3390/vaccines11091402
Zhong J, Wang W, Liu S, Chen Y, Xiong H, Meng X, Zhang D, Ma Y. Effectiveness of Maternal Inactivated COVID-19 Vaccination against Omicron Infection in Infants during the First 12 Months of Life: A Test-Negative Case-Control Study. Vaccines. 2023; 11(9):1402. https://doi.org/10.3390/vaccines11091402
Chicago/Turabian StyleZhong, Jiayi, Wen Wang, Shuang Liu, Yifei Chen, Husheng Xiong, Xiang Meng, Dingmei Zhang, and Yu Ma. 2023. "Effectiveness of Maternal Inactivated COVID-19 Vaccination against Omicron Infection in Infants during the First 12 Months of Life: A Test-Negative Case-Control Study" Vaccines 11, no. 9: 1402. https://doi.org/10.3390/vaccines11091402
APA StyleZhong, J., Wang, W., Liu, S., Chen, Y., Xiong, H., Meng, X., Zhang, D., & Ma, Y. (2023). Effectiveness of Maternal Inactivated COVID-19 Vaccination against Omicron Infection in Infants during the First 12 Months of Life: A Test-Negative Case-Control Study. Vaccines, 11(9), 1402. https://doi.org/10.3390/vaccines11091402