
Anaphylatoxin Complement 5a in Pfizer BNT162b2-Induced Immediate-Type Vaccine Hypersensitivity Reactions

 ,
,
Abstract
1. Introduction
2. Materials and Methods
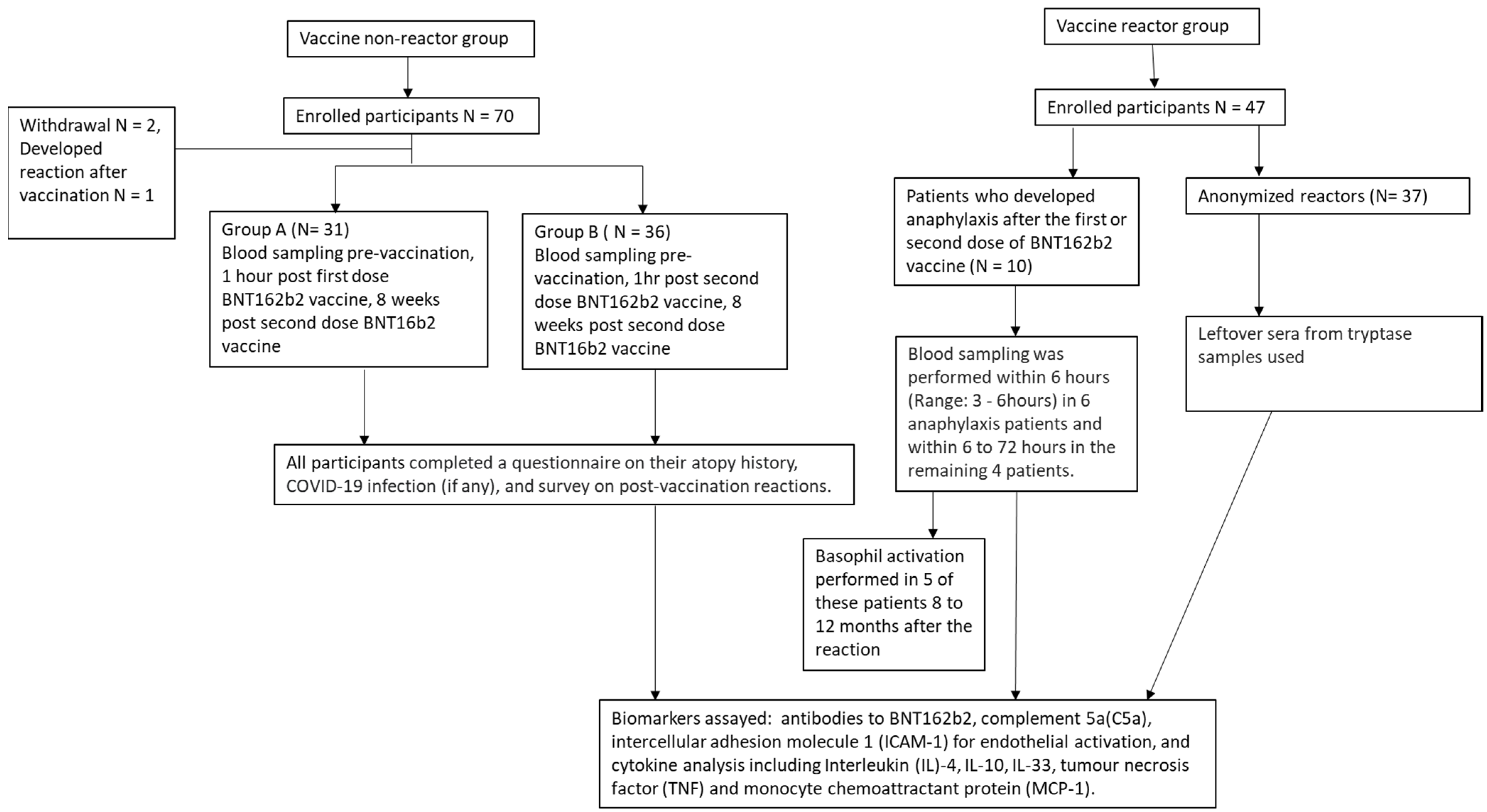
2.1. Participant Selection
2.2. Sample Collection
- (a)
- Group A: Blood sampling pre-vaccination, 1 h post first dose BNT162b2 vaccine, 8 weeks post second dose BNT16b2 vaccine;
- (b)
- Group B: Blood sampling pre-vaccination, 1 h post second dose BNT162b2 vaccine, 8 weeks post second dose BNT16b2 vaccine.
2.3. Immunological Methods
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization [Internet]. Geneva: World Health Organization; c2022. Weekly Epidemiological Update on COVID-19-17 August 2022; [about 1 Screen]. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---17-august-2022 (accessed on 20 August 2022).
- World Health Organization [Internet]. Geneva: World Health Organization; c2022. COVID-19 in Singapore Situation Report 61; [about 1 Screen]. Available online: https://www.who.int/singapore/internal-publications-detail/covid-19-in-singapore-situation-report-61 (accessed on 20 August 2022).
- CDC COVID-19 Response Team; Food and Drug Administration. Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine-United States, December 14–23, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M.; Weintraub, E.S.; Duffy, J.; Sukumaran, L.; Jacobsen, S.J.; Klein, N.P.; Hambidge, S.J.; Lee, G.M.; Jackson, L.A.; Irving, S.A.; et al. Risk of anaphylaxis after vaccination in children and adults. J. Allergy Clin. Immunol. 2016, 137, 868–878. [Google Scholar] [CrossRef]
- Health Sciences Authority [Internet]. Singapore: Health Sciences Authority; c2020. Interim Authorisation of Pfizer-BioNTech COVID-19 Vaccine (BNT162b2) for Active Immunisation to Prevent COVID-19 Disease in Singapore; [about 1 Screen]. Available online: https://www.hsa.gov.sg/announcements/dear-healthcare-professional-letter/interim-authorisation-of-pfizer-biontech-covid-19-vaccine-(bnt162b2)-for-active-immunisation-to-prevent-covid-19-disease-in-singapore (accessed on 20 August 2022).
- Health Sciences Authority [Internet]. Singapore: Health Sciences Authority; c2021. HSA Grants Interim Authorisation for Moderna COVID-19 Vaccine in Singapore; [about 1 Screen]. Available online: https://www.hsa.gov.sg/announcements/press-release/hsa-grants-interim-authorisation-for-moderna-covid-19-vaccine-in-singapore (accessed on 20 August 2022).
- Health Sciences Authority [Internet]. Singapore: Health Sciences Authority; c2021. HSA’s Safety Update #1 Pfizer-BioNTech and Moderna COVID-19 Vaccines (30 December 2020–18 April 2021); [about 1 Screen]. Available online: https://www-hsa-gov-sg-admin.cwp.sg/docs/default-source/hprg-vcb/safety-update-on-covid19-vaccines/safety-update-no-1-on-covid-19-vaccines-(18-apr-2021) (accessed on 20 August 2022).
- Health Sciences Authority [Internet]. Singapore: Health Sciences Authority; c2022. HSA’s COVID-19 Vaccine Safety Update #11 (30 December 2020–28 February 2022); [about 1 Screen]. Available online: https://www.hsa.gov.sg/docs/default-source/hprg-vcb/safety-update-on-covid19-vaccines/hsa-safety-update-no-11-on-covid-19-vaccines-(28-february-2022).pdf (accessed on 20 August 2022).
- Barbaud, A.; Garvey, L.H.; Arcolaci, A.; Brockow, K.; Mori, F.; Mayorga, C.; Bonadonna, P.; Atanaskovic-Markovic, M.; Moral, L.; Zanoni, G.; et al. Allergies and COVID-19 vaccines: An ENDA/EAACI Position paper. Allergy 2022, 77, 2292–2312. [Google Scholar] [CrossRef] [PubMed]
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A.; Edwards, K.M.; Hummell, D.S.; Little, F.F.; Norton, A.E.; Stallings, A.; Wood, R.A.; Milner, J.D. Potential mechanisms of anaphylaxis to COVID-19 mRNA vaccines. J. Allergy Clin. Immunol. 2021, 147, 2075–2082.e2. [Google Scholar] [CrossRef] [PubMed]
- Klimek, L.; Novak, N.; Cabanillas, B.; Jutel, M.; Bousquet, J.; Akdis, C.A. Allergenic components of the mRNA-1273 vaccine for COVID-19: Possible involvement of polyethylene glycol and IgG-mediated complement activation. Allergy 2021, 76, 3307–3313. [Google Scholar] [CrossRef]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef] [PubMed]
- Castells, M.C.; Phillips, E.J. Maintaining Safety with SARS-CoV-2 Vaccines. N. Engl. J. Med. 2021, 384, 643–649. [Google Scholar] [CrossRef]
- Lim, X.R.; Tan, J.W.L.; Chan, G.Y.L.; Hou, J.; Xie, L.; Goh, V.H.L.; Boon, J.; Lee, S.S.M.; Teo, C.M.L.; Tan, S.C.; et al. Evaluation of Patients with Vaccine Allergies Prior to mRNA-Based COVID-19 Vaccination. Vaccines 2022, 10, 1025. [Google Scholar] [CrossRef]
- Ruggeberg, J.U.; Gold, M.S.; Bayas, J.M.; Blum, M.D.; Bonhoeffer, J.; Friedlander, S.; de Souza Brito, G.; Heininger, U.; Imoukhuede, B.; Khamesipour, A.; et al. Brighton Collaboration Anaphylaxis Working Group. Anaphylaxis: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2007, 25, 5675–5684. [Google Scholar] [CrossRef]
- Lim, X.R.; Leung, B.P.; Ng, C.Y.L.; Tan, J.W.L.; Chan, G.Y.L.; Loh, C.M.; Tan, G.L.X.; Goh, V.H.H.; Wong, L.T.; Chua, C.R.; et al. Pseudo-Anaphylactic Reactions to Pfizer BNT162b2 Vaccine: Report of 3 Cases of Anaphylaxis Post Pfizer BNT162b2 Vaccination. Vaccines 2021, 9, 974. [Google Scholar] [CrossRef]
- Warren, C.M.; Snow, T.T.; Lee, A.S.; Shah, M.M.; Heider, A.; Blomkalns, A.; Betts, B.; Buzzanco, A.S.; Gonzalez, J.; Chinthrajah, R.S.; et al. Assessment of Allergic and Anaphylactic Reactions to mRNA COVID-19 Vaccines With Confirmatory Testing in a US Regional Health System. JAMA Netw. Open 2021, 4, e2125524. [Google Scholar] [CrossRef]
- Troelnikov, A.; Perkins, G.; Yuson, C.; Ahamdie, A.; Balouch, S.; Hurtado, P.R.; Hissaria, P. Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in patients with PEG allergy. J. Allergy Clin. Immunol. 2021, 148, 91–95. [Google Scholar] [CrossRef]
- Saxena, A.; Khosraviani, S.; Noel, S.; Mohan, D.; Donner, T.; Hamad, A.R.A. Interleukin-10 paradox: A potent immunoregulatory cytokine that has been difficult to harness for immunotherapy. Cytokine 2015, 74, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Stone, S.F.; Cotterell, C.; Isbister, G.K.; Holdgate, A.; Brown, S.G. Elevated serum cytokines during human anaphylaxis: Identification of potential mediators of acute allergic reactions. J. Allergy Clin. Immunol. 2009, 124, 786–792.e4. [Google Scholar] [CrossRef]
- Pushparaj, P.N.; Tay, H.K.; H’ng, S.C.; Pitman, N.; Xu, D.; McKenzie, A.; Liew, F.Y.; Melendez, A.J. The cytokine interleukin-33 mediates anaphylactic shock. Proc. Natl. Acad. Sci. USA 2009, 106, 9773–9778, retracted in Proc. Natl. Acad. Sci. USA 2012, 109, 13877. [Google Scholar] [CrossRef]
- Jiang, S.Y.; Smith, E.M.; Vo, V.; Akdis, C.; Nadeau, K.C. Non-immunoglobulin E-mediated allergy associated with Pfizer-BioNTech coronavirus disease 2019 vaccine excipient polyethylene glycol. Ann. Allergy Asthma. Immunol. 2021, 127, 694–696. [Google Scholar] [CrossRef]
- Krantz, M.S.; Bruusgaard-Mouritsen, M.A.; Koo, G.; Phillips, E.J.; Stone, C.A., Jr.; Garvey, L.H. Anaphylaxis to the first dose of mRNA SARS-CoV-2 vaccines: Don’t give up on the second dose! Allergy 2021, 76, 2916–2920. [Google Scholar] [CrossRef]
- Puxkandl, V.; Bangerl, T.; Hanfstingl, K.; Guenova, E.; Hoetzenecker, W.; Altrichter, S. Second-dose COVID-19 vaccines are well tolerated in patients with allergic reactions to the first dose—A single center experience. World. Allergy Organ. J. 2022, 15, 100654. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.R.; Robinson, L.B.; Li, L.; McMahon, A.E.; Cogan, A.S.; Fu, X.; Wickner, P.; Samarakoon, U.; Saff, R.R.; Blumenthal, K.G. First-Dose mRNA COVID-19 Vaccine Allergic Reactions: Limited Role for Excipient Skin Testing. J. Allergy Clin. Immunol. Pract. 2021, 9, 3308–3320.e3. [Google Scholar] [CrossRef] [PubMed]
- Kennard, L.; Rutkowski, K.; Mirakian, R.; Wagner, A. Polyethylene glycol: Not just a harmless excipient. J. Allergy Clin. Immunol. Pract. 2018, 6, 2173. [Google Scholar] [CrossRef]
- Yang, Q.; Jacobs, T.M.; McCallen, J.D.; Moore, D.T.; Huckaby, J.T.; Edelstein, J.N.; Lai, S.K. Analysis of Pre-existing IgG and IgM Antibodies against Polyethylene Glycol (PEG) in the General Population. Anal Chem. 2016, 88, 11804–11812. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.L.; Jacob, S.; Hymes, J.; Usvyat, L.A.; Maddux, F.W. Anaphylaxis and hypotension after administration of peginesatide. N. Engl. J. Med. 2014, 370, 2055–2056. [Google Scholar] [CrossRef]
- Lee, S.H.; Cha, J.M.; Lee, J.I.; Joo, K.R.; Shin, H.P.; Baek, I.H.; Jeon, J.W.; Lim, J.U.; Lee, J.L.; Lee, H.M.; et al. Anaphylactic shock caused by ingestion of polyethylene glycol. Intest. Res. 2015, 13, 90–94. [Google Scholar] [CrossRef]
- Somiya, M.; Mine, S.; Yasukawa, K.; Ikeda, S. Sex differences in the incidence of anaphylaxis to LNP-mRNA COVID-19 vaccines. Vaccine 2021, 39, 3313–3314. [Google Scholar] [CrossRef]
- Szebeni, J.; Fontana, J.L.; Wassef, N.M.; Mongan, P.D.; Morse, D.S.; Dobbins, D.E.; Stahl, G.L.; Bunger, R.; Alving, C.R. Hemodynamic changes induced by liposomes and liposome-encapsulated hemoglobin in pigs: A model for pseudoallergic cardiopulmonary reactions to liposomes. Role of complement and inhibition by soluble CR1 and anti-C5a antibody. Circulation 1999, 99, 2302–2309. [Google Scholar] [CrossRef] [PubMed]
- Rabinovici, R.; Rudolph, A.S.; Feuerstein, G. Characterization of hemodynamic, hematologic and biochemical responses to administration of liposome-encapsulated hemoglobin in the conscious, freely moving rat. Circ. Shock 1989, 29, 115–132. [Google Scholar] [PubMed]
- Hongo, T.; Nozaki, S.; Tsuchiya, M.; Inaba, M.; Takahashi, K.; Fujiwara, T. Contrast medium-induced transient severe leukopenia. Acute Med. Surg. 2017, 5, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Ju, Y.; Lee, W.S.; Pilkington, E.H.; Kelly, H.G.; Li, S.; Selva, K.J.; Wragg, K.M.; Subbarao, K.; Nguyen, T.H.; Rowntree, L.C.; et al. Anti-PEG Antibodies Boosted in Humans by SARS-CoV-2 Lipid Nanoparticle mRNA Vaccine. ACS Nano 2022, 16, 11769–11780. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.; Gioria, S.; Sauer, A.V.; Lucchesi, S.; Montagnani, F.; Pastore, G.; Ciabattini, A.; Medaglini, D. Monitoring Anti-PEG Antibodies Level upon Repeated Lipid Nanoparticle-Based COVID-19 Vaccine Administration. Int. J. Mol. Sci. 2022, 23, 8838. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics | Vaccine Non-Reactors N = 67 | Anaphylaxis Patients N = 10 |
|---|---|---|
| Age, mean (SD) | 35 (17.5) | 43.4 (14.5) |
| Sex (female, %) | 75(77.3%) | 8 (80%) |
| Race (%) | ||
| Chinese | 71 (73.2%) | 8 (80%) |
| Malay | 14 (14.4%) | 0 (0%) |
| Indian | 4 (4.12%) | 2 (20%) |
| Others | 8 (8.25%) | 0 (0%) |
| Allergic and atopic conditions | ||
| Allergic rhinitis | 15 (15.5%) | 6 (60%) |
| Asthma | 10 (10.3%) | 5 (50%) |
| Chronic spontaneous urticaria | 10 (10.3%) | 2 (20%) |
| Food allergy | 28 (28.9%) | 3 (30%) |
| Eczema | 12 (12.4%) | 1 (10%) |
| Drug allergy/hypersensitivity | 13 (23.4%) | 4 (40%) |
| Vaccine reactions | ||
| Cutaneous | N.A. | 9 (90%) |
| Upper airway | N.A. | 8 (80%) |
| Lower airway | N.A. | 10 (100%) |
| Cardiovascular | N.A. | 2 (20%) |
| Gastrointestinal | N.A. | 3(30%) |
| Brighton Level 1 | N.A. | 6 (60%) |
| Brighton Level 2 | N.A. | 4 (40%) |
| S/N | Age | Gender | Ethnicity | Reaction Onset | Vaccine Dose | Atopy History | Signs and Symptoms | Brighton Level | Treatment |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 45 | M | Indian | 30 min | Second | Asthma, urticaria to etoricoxib | Flushing, periorbital edema, globus sensation, wheezing * Developed periorbital edema after first dose | 1 | IM Adrenaline x two doses, IV hydrocortisone, IV diphenhydramine, nebulised salbutamol |
| 2 | 39 | F | Chinese | 30 min | First | Asthma, allergic rhinitis | Flushing, erythema, breathlessness, globus sensation, wheezing * Had triphasic reaction with symptoms recurring 8 and 27 h post vaccination | 1 | IM adrenaline, IV hydrocortisone, IV diphenhydramine, IV cimetidine, nebulised salbutamol and ipratropium |
| 3 | 42 | F | Chinese | 20 min | Second | Chronic rhinosinusitis | Generalised urticaria, periorbital edema, globus sensation, breathlessness | 2 | IM adrenaline, IV hydrocortisone and diphenhydramine |
| 4 | 80 | F | Chinese | 30 min | First | Nil | Flushing, erythema, globus sensation, breathlessness, vomiting | 2 | IV hydrocortisone and diphenhydramine |
| 5 | 26 | F | Chinese | 45 min | First | Allergic rhinitis, shellfish allergy | Urticaria, angioedema, breathlessness, giddiness, vomiting | 2 | IM adrenaline, IV hydrocortisone, PO chlorphenamine |
| 6 | 52 | F | Chinese | 25 min | First | NSAID hypersensitivity, asthma, allergic rhinitis, peanut allergy | Periorbital edema, globus sensation, wheezing, hypotension | 1 | IM adrenaline x two doses, promethazine, Nebulised salbutamol |
| 7 | 35 | F | Indian | 20 min | First | NSAID hypersensitivity, allergic rhinitis, episodic contact urticaria | Urticaria, globus sensation, breathlessness, hypotension | 1 | IV hydrocortisone, cimetidine, diphenhydramine, fluids |
| 8 | 39 | F | Chinese | 10 min | First | Allergic rhinitis, chronic spontaneous urticaria, eczema, shellfish allergy | Epiglottic swelling, globus sensation, breathlessness, abdominal discomfort and diarrhoea | 2 | IM adrenaline x two doses, IV dexamethasone, diphenhydramine |
| 9 | 38 | F | Chinese | 30 min | First | Asthma, allergic rhinitis, NSAID hypersensitivity | Urticaria, globus sensation, shortness of breath | 1 | Unknown (received initial treatment outside the institution) |
| 10 | 38 | M | Chinese | 6 min | Second | Asthma | Urticaria, breathlessness, wheezing * Had mild breathlessness and wheezing after dose 1 | 1 | IV diphenhydramine, hydrocortisone, salbutamol |
| (a) | |||||
|---|---|---|---|---|---|
| Vaccine Non-Reactors N = 67 | Vaccine Reactors Combined N = 47 | p Value (Comparing Vaccine Non-Reactors and Vaccine Reactors Combined) | * Vaccine Non-Reactors 1 h after 1st Dose BNT162b2 Vaccine N = 31 | * Vaccine Non-Reactors 1 h after 2nd Dose BNT162b2 Vaccine N = 36 | |
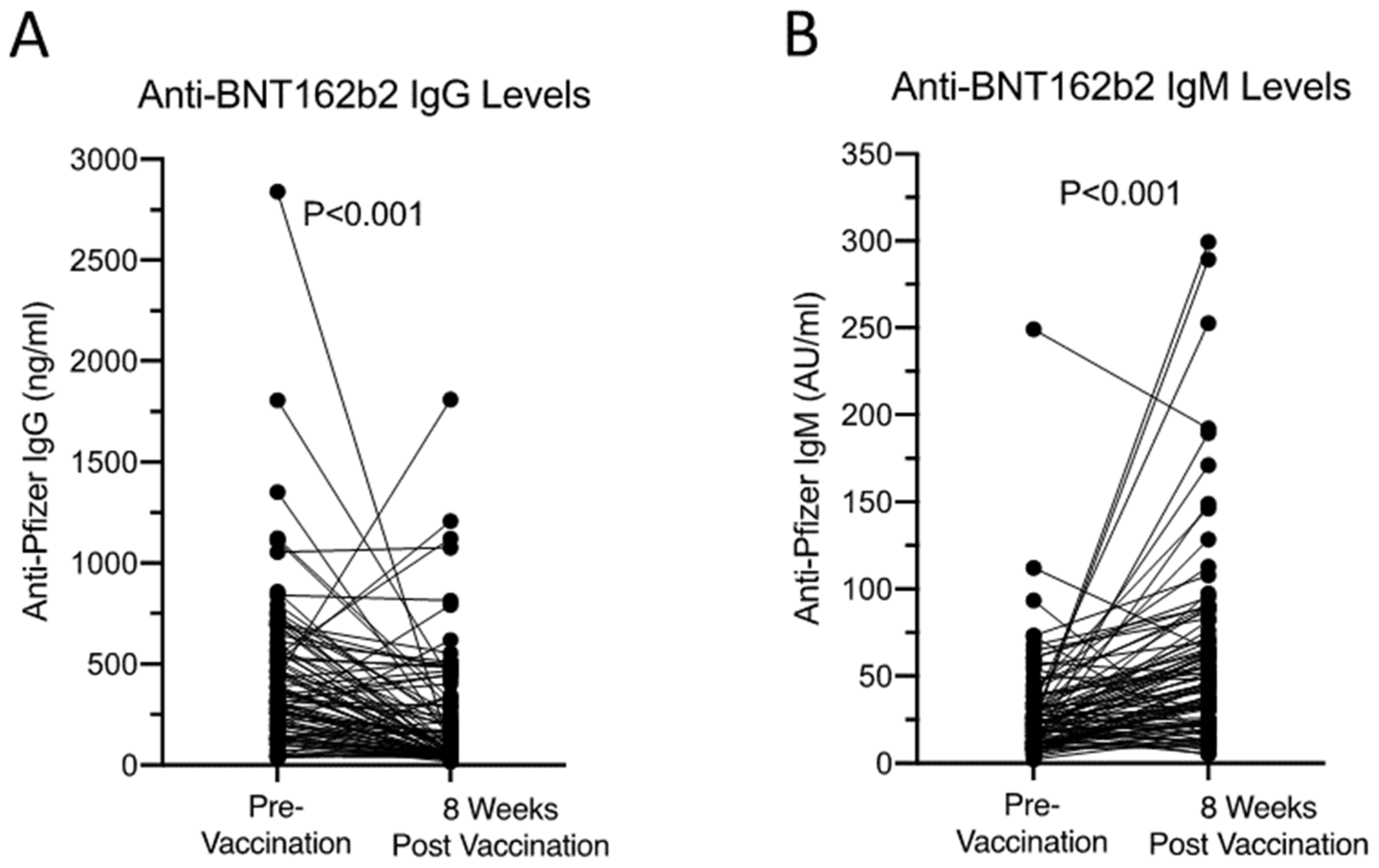
| Anti-BNT162b2 IgG (ng/mL) | 230.6 (77.6–449) | 222.0 (118–360) | 0.897 | 202.9 (75.7–377.5) | 249.7 (95.8–482.7) |
| Anti-BNT162b2 IgM (AU/mL) | 23.9 (13.8–48.9) | 67.2 (36.2–91.6) | <0.001 | 20.9 (14.6–35.6) | 34.8 (15.3–52.7) |
| Anti-BNT162b2 IgE (ng/mL) | N.D. | N.D. | N.A. | N.D. | N.D. |
| C5a (ng/mL) | 39.4 (27.5–50.7) | 160.0 (42.2–728.0) | <0.001 | 36.1 (24.5–45.0) | 43.7 (32.6–52.1) |
| ICAM-1 (ng/mL) | 46.0 (39.5–66.2) | 136.0 (99.9–170.0) | <0.001 | 42.6 (37.1–63.4) | 44.0 (39.5–56.3) |
| (b) | |||||
| Vaccine Non-Reactors N= 67 | Anaphylaxis Patients N= 6 | pValue | |||
| Anti-BNT162b2 IgG (ng/mL) | 230.6 (77.6–449) | 372.6 (298.6–1169.8) | <0.05 | ||
| Anti-BNT162b2 IgM (AU/mL) | 23.9 (13.8–48.9) | 50.0 (30.3–56.9) | <0.05 | ||
| Anti-BNT162b2 IgE (ng/mL) | N.D. | N.D. | N.A. | ||
| C5a (ng/mL) | 39.4 (27.5–50.7) | 571.6 (448.6–625.1) | <0.05 | ||
| ICAM-1 (ng/mL) | 46.0 (39.5–66.2) | 126.0 (89.0–135.0) | <0.05 | ||
| Vaccine Reactors with High C5a (N = 37) | Vaccine Reactors with Low C5a (N = 8) | p Value | |
|---|---|---|---|
| C5a (ng/mL) * | 697 (271–1147) | 37.6 (27.0–49.1) | <0.001 |
| Anti-BNT162b2 IgG (ng/mL) | 302 (200–417) | 292 (148–491) | 0.999 |
| Anti-BNT162b2 IgM (AU/mL) | 62.8 (30.7–80) | 50.3 (28–75.5) | 0.961 |
| Anti-BNT162b2 IgE (ng/mL) | N.D. | N.D. | N.A. |
| ICAM-1 (ng/mL) | 119 (68.6–146) | 105 (68.9–141) | 0.999 |
| IL-4 (pg/mL) | 5.65 (1.21–46.0) | 0.29 (0.15–2.33) | <0.02 |
| IL-10 (pg/mL) | 9.52 (8.97–15.6) | 2.69 (2.41–6.44) | 0.456 |
| IL-33 (pg/mL) | 9.34 (4.4–86.4) | 2.34 (0.52–5.05) | <0.003 |
| TNF (pg/mL) | 0.54 (0.39–1.1) | 7.02 (2.88–19.9) | <0.042 |
| MCP-1 (pg/mL) | 308 (252–412) | 31.6 (16.2–233) | <0.003 |
| Patient No | Experiments | CCR+/CD63+ Basophil (%) | CCR3+/CD 203c+ Basophil (%) |
|---|---|---|---|
| Patient 1 * | Negative control (buffer solution) | 0.5 | 0.9 |
| Anti-IgE positive control | 7.8 * | 20.3 | |
| Pfizer-BNT162b2 1% | 0.1 | 1.4 | |
| Pfizer-BNT162b2 0.1% | 0.7 | 1.7 | |
| Patient 2 | Negative control (buffer solution) | 0.2 | 0.4 |
| Anti-IgE positive control | 81.7 | 56.2 | |
| Pfizer-BNT162b2 1% | 0.5 | 0.9 | |
| Pfizer-BNT162b2 0.1% | 0.2 | 0.8 | |
| Patient 3 | Negative control (buffer solution) | 0.2 | 0.5 |
| Anti-IgE positive control | 84.6 | 49.5 | |
| Pfizer-BNT162b2 1% | 0 | 1.5 | |
| Pfizer-BNT162b2 0.1% | 0.1 | 0.7 | |
| PEG 2000 1% | 0.2 | 0.1 | |
| DMG-PEG 2000 1% | 0.3 | 0.4 | |
| Patient 4 | Negative control (buffer solution) | 0.1 | 0.2 |
| Anti-IgE positive control | 69.2 | 65.2 | |
| Pfizer-BNT162b2 1% | 0.2 | 0.6 | |
| Pfizer-BNT162b2 0.1% | 0.1 | 0.4 | |
| PEG 2000 1% | 0.2 | 0.1 | |
| DMG-PEG 2000 1% | 0.6 | 0.4 | |
| Patient 5 | Negative control (buffer solution) | 0.1 | 1.2 |
| Anti-IgE positive control | 50.4 | 39.9 | |
| Pfizer-BNT162b2 1% | 0.2 | 0.7 | |
| Pfizer-BNT162b2 0.1% | 0.1 | 0.5 | |
| PEG 2000 1% | 0.2 | 0.7 | |
| DMG-PEG 2000 1% | 0.1 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, X.R.; Chan, G.Y.L.; Tan, J.W.L.; Ng, C.Y.L.; Chua, C.G.; Tan, G.B.; Chan, S.S.W.; Ong, K.H.; Tan, Y.Z.; Tan, S.H.Z.; et al. Anaphylatoxin Complement 5a in Pfizer BNT162b2-Induced Immediate-Type Vaccine Hypersensitivity Reactions. Vaccines 2023, 11, 1020. https://doi.org/10.3390/vaccines11061020
Lim XR, Chan GYL, Tan JWL, Ng CYL, Chua CG, Tan GB, Chan SSW, Ong KH, Tan YZ, Tan SHZ, et al. Anaphylatoxin Complement 5a in Pfizer BNT162b2-Induced Immediate-Type Vaccine Hypersensitivity Reactions. Vaccines. 2023; 11(6):1020. https://doi.org/10.3390/vaccines11061020
Chicago/Turabian StyleLim, Xin Rong, Grace Yin Lai Chan, Justina Wei Lynn Tan, Carol Yee Leng Ng, Choon Guan Chua, Guat Bee Tan, Stephrene Seok Wei Chan, Kiat Hoe Ong, Ying Zhi Tan, Sarah Hui Zhen Tan, and et al. 2023. "Anaphylatoxin Complement 5a in Pfizer BNT162b2-Induced Immediate-Type Vaccine Hypersensitivity Reactions" Vaccines 11, no. 6: 1020. https://doi.org/10.3390/vaccines11061020
APA StyleLim, X. R., Chan, G. Y. L., Tan, J. W. L., Ng, C. Y. L., Chua, C. G., Tan, G. B., Chan, S. S. W., Ong, K. H., Tan, Y. Z., Tan, S. H. Z., Teo, C. M. L., Lee, S. S. M., Thong, B. Y. H., & Leung, B. P. L. (2023). Anaphylatoxin Complement 5a in Pfizer BNT162b2-Induced Immediate-Type Vaccine Hypersensitivity Reactions. Vaccines, 11(6), 1020. https://doi.org/10.3390/vaccines11061020