




Sociodemographic Factors Associated with COVID-19 Vaccination among People in Guatemalan Municipalities

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Data
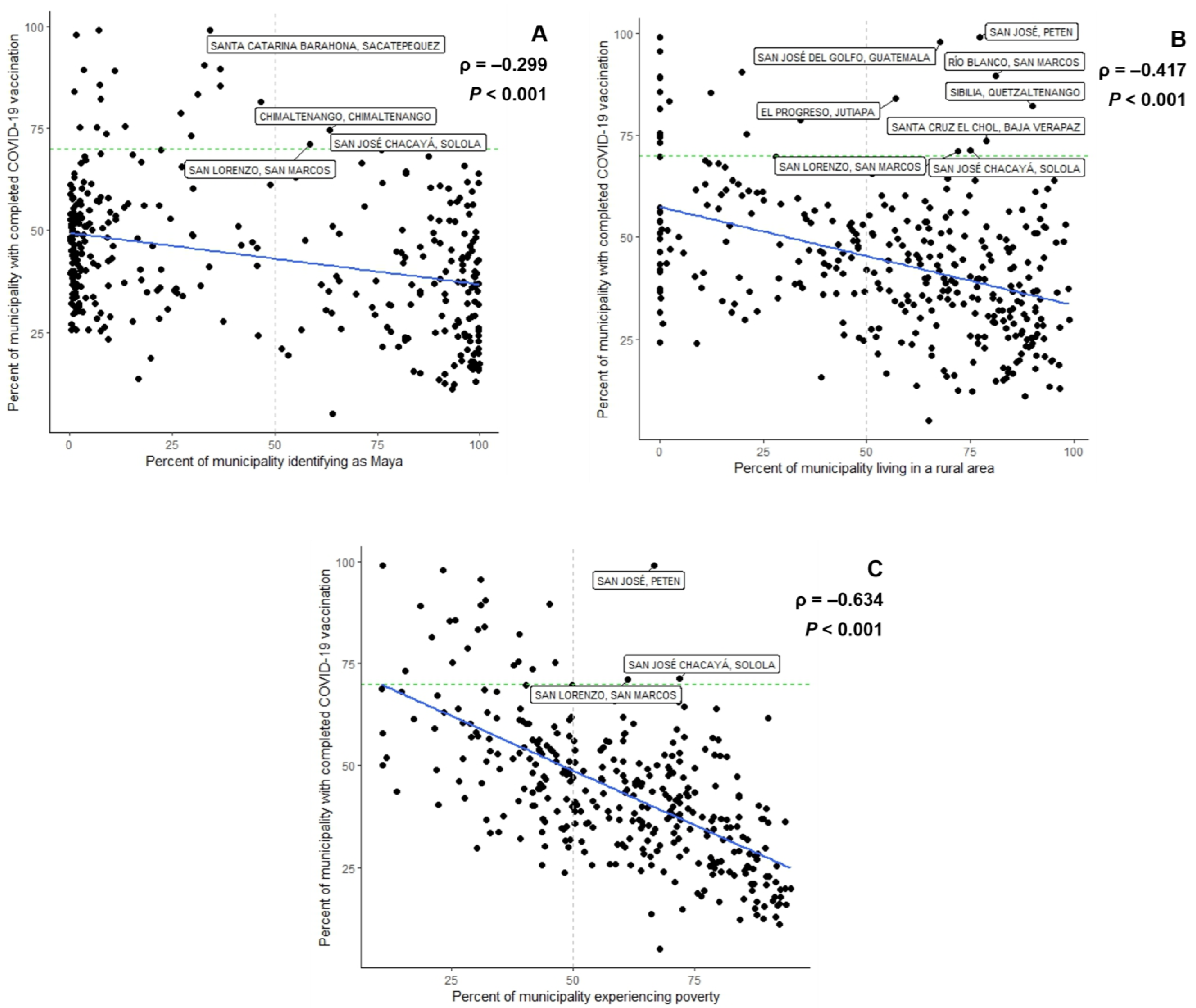
3.2. Factors Associated with COVID-19 Vaccination
3.3. Factors Associated with COVID-19 Vaccination among People Aged 60 Years or Older
3.4. Factors Associated with COVID-19 Vaccination up to 1 October 2021
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The World Bank. The World Bank in Guatemala. 2022. Available online: https://www.worldbank.org/en/country/guatemala/overview (accessed on 11 January 2023).
- Pan American Health Organization. Health in the Americas 2012 Edition; Pan American Health Organization: Guatemala City, Guatemala, 2012. [Google Scholar]
- United States Agency for International Development. Prosperity in Guatemala. Available online: https://www.usaid.gov/guatemala/prosperity (accessed on 6 February 2023).
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 6 December 2022).
- Taylor, L. Guatemala’s COVID vaccine roll-out failed: Here’s what researchers know. Nature 2022. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Health Emergency Dashboard. Available online: https://covid19.who.int/region/amro/country/gt (accessed on 4 December 2022).
- Johns Hopkins University. Coronavirus Resource Center. 2022. Available online: https://coronavirus.jhu.edu/region/guatemala (accessed on 4 December 2022).
- Republic of Guatemala Ministry of Health Public and Social Assistance (MSPAS). National Vaccination Plan against COVID-19. 2021. Available online: https://oiss.org/wp-content/uploads/2021/02/Plan-Nacional-de-Vacunacion-contra-la-COVID-19.pdf (accessed on 4 December 2022).
- COVID-19 Observatory in Latin America and the Caribbean. Economic and Social Impact. 2022. Available online: https://statistics.cepal.org/forms/covid-countrysheet/index.html?country=GTM (accessed on 4 December 2022).
- COVID-19 Vaccine Tracker. 4 Vaccines Approved for Use in Guatemala. 2022. Available online: https://covid19.trackvaccines.org/country/guatemala/ (accessed on 4 December 2022).
- Gobierno de Guatemala Ministerio de Salud Publica y Asistencia Social. COVID-19 Situation in Guatemala. 2022. Available online: https://tablerocovid.mspas.gob.gt/tablerocovid/ (accessed on 5 December 2022).
- Gobierno de Guatemala Ministerio de Salud Publica y Asistencia Social. COVID-19 Vaccination in Guatemala (Tablero). 2022. Available online: https://gtmvigilanciacovid.shinyapps.io/Coberturas_Tablero/ (accessed on 5 December 2022).
- Sobral, M.F.F.; Bezerra de Oliveira, B.R.; Gomes da Penha Sobral, A.I.; Monteiro Marinho, M.L.; Duarte, G.B.; de Souza Melo, A. SARS-CoV-2 Vaccines: What Indicators are Associated with the Worldwide Distribution of the First Doses. Inquiry 2021, 58, 469580211060184. [Google Scholar] [CrossRef] [PubMed]
- Etienne, C.F. COVID-19 has revealed a pandemic of inequality. Nat. Med. 2022, 28, 17. [Google Scholar] [CrossRef] [PubMed]
- Gozzi, N.; Chinazzi, M.; Dean, N.E.; Longini, I.M.; Halloran, M.E.; Perra, N.; Vespignani, A. Estimating the impact of COVID-19 vaccine allocation inequities: A modeling study. medRxiv 2022. [Google Scholar] [CrossRef]
- Baack, B.N.; Abad, N.; Yankey, D.; Kahn, K.E.; Razzaghi, H.; Brookmeyer, K.; Kolis, J.; Wilhelm, E.; Nguyen, K.H.; Singleton, J.A. COVID-19 Vaccination Coverage and Intent among Adults Aged 18–39 Years—United States, March–May 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Murthy, B.P.; Sterrett, N.; Weller, D.; Zell, E.; Reynolds, L.; Toblin, R.L.; Murthy, N.; Kriss, J.; Rose, C.; Cadwell, B.; et al. Disparities in COVID-19 Vaccination Coverage between Urban and Rural Counties—United States, December 14, 2020–April 10, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 759–764. [Google Scholar] [CrossRef]
- Hughes, M.M.; Wang, A.; Grossman, M.K.; Pun, E.; Whiteman, A.; Deng, L.; Hallisey, E.; Sharpe, J.D.; Ussery, E.N.; Stokley, S.; et al. County-Level COVID-19 Vaccination Coverage and Social Vulnerability—United States, December 14, 2020–March 1, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 431–436. [Google Scholar] [CrossRef]
- Avila, C.; Bright, R.; Gutierrez, J.; Hoadley, K.; Manuel, C.; Romero, N.; Rodriguez, M.P. Guatemala Health System Assessment, August 2015; Health Finance & Governance Project, Abt Associates Inc.: Bethesda, MD, USA, 2015. [Google Scholar]
- Lou-Meda, R.; Méndez, S.; Calgua, E.; Orozco, M.; Hall, B.J.; Fahsen, N.; Taicher, B.M.; Doty, J.P.; Colindres, J.G.; Menegazzo, C.S.; et al. Developing a national patient safety plan in Guatemala. Rev. Panam. Salud Pública 2019, 43, e64. [Google Scholar] [CrossRef]
- Laboratorio de Datos GT. COVID-19 Vaccination and Vulnerable Populations: Inequality and Institutional Barriers (MSPAS) of Access to Vaccination; Laboratorio de Datos GT: Guatemala City, Guatemala, 2022. [Google Scholar]
- National Institute of Statistics (Guatemala); United Nations Population Fund (UNFPA). Guatemala Population and Housing Census 2018. 2018. Available online: https://www.censopoblacion.gt/ (accessed on 5 December 2022).
- Cifuentes, M.P.; Rodriguez-Villamizar, L.A.; Rojas-Botero, M.L.; Alvarez-Moreno, C.A.; Fernández-Niño, J.A. Socioeconomic inequalities associated with mortality for COVID-19 in Colombia: A cohort nationwide study. J. Epidemiol. Community Health 2021, 75, 610–615. [Google Scholar] [CrossRef]
- United Nations Educational, Scientific and Cultural Organization (UNESCO). COVID-19 and Vaccination in Latin America and the Caribbean; United Nations Educational, Scientific and Cultural Organization (UNESCO): Paris, France, 2021. [Google Scholar]
- Pires, C. Global Predictors of COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 1349. [Google Scholar] [CrossRef]
- Morales-García, W.C.; Huancahuire-Vega, S.; Saintila, J.; Morales-García, M.; Fernández-Molocho, L.; Ruiz Mamani, P.G. Predictors of Intention to Vaccinate against COVID-19 in a Peruvian Sample. J. Prim. Care Community Health 2022, 13, 21501319221092254. [Google Scholar] [CrossRef] [PubMed]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.; Rodriguez-Morales, A.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef] [PubMed]
- Health Policy Plus. Guatemala’s Tailored, Rural Vaccination Plan Strengthens COVID-19 Vaccine Coverage. 2021. Available online: http://www.healthpolicyplus.com/GuateRuralVacc.cfm (accessed on 26 January 2023).
- Ministerio de Salud Pública y Asistencia Social—MSPAS/Guatemala; Instituto Nacional de Estadística—INE/Guatemala; Secretaría de Planificación y Programación del la Presidencia—Segeplán/Guatemala; ICF International. Encuesta Nacional de salud Materno Infantil 2014–2015: Informe Final; Ministerio de Salud Pública y Asistencia Social (MSPAS): Guatemala City, Guatemala; Instituto Nacional de Estadística (INE): Guatemala City, Guatemala; Secretaría de Planificación y Programación de la Presidencia (Segeplán): Guatemala City, Guatemala; ICF International: Rockville, MD, USA, 2017.
- Caycho-Rodríguez, T.; Tomás, J.M.; Carbajal-León, C.; Vilca, L.W.; Reyes-Bossio, M.; Intimayta-Escalante, C.; Vivanco-Vidal, A.; Saroli-Araníbar, D.; Esteban, R.F.C.; White, M. Sociodemographic and Psychological Predictors of Intention to Receive a COVID-19 Vaccine in Elderly Peruvians. Trends Psychol. 2022, 30, 206–223. [Google Scholar] [CrossRef]
- Caycho-Rodríguez, T.; Valencia, P.D.; Vilca, L.W.; Carbajal-León, C.; Vivanco-Vidal, A.; Saroli-Araníbar, D.; Reyes-Bossio, M.; White, M.; Rojas-Jara, C.; Polanco-Carrasco, R.; et al. Prevalence and Predictors of Intention to be Vaccinated against COVID-19 in Thirteen Latin American and Caribbean Countries. Trends Psychol. 2022, 1–25. [Google Scholar] [CrossRef]
- Huang, J.; Chan, S.C.; Ko, S.; Wang, H.H.X.; Yuan, J.; Xu, W.; Zheng, Z.J.; Xue, H.; Zhang, L.; Jiang, J.Y.; et al. Factors Associated with Vaccination Intention against the COVID-19 Pandemic: A Global Population-Based Study. Vaccines 2022, 10, 1539. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, R. (Centers for Disease Control and Prevention, Atlanta, GA, USA); Marsicovetere, P. (University of the Valley of Guatemala, Guatemala City, Guatemala). Personal communication, 2022.
- Instituto Nacional de Estadística—INE/Guatemala. Encuesta Nacional de Condiciones de Vida 2014; Instituto Nacional de Estadística (INE): Guatemala City, Guatemala, 2016.
- Figueroa Chávez, W.; Peñate, M.; Marsicovetere, P. Estimación de Pobreza a Nivel Municipal en Guatemala Mediante la Utilización de Machine Learning. 2020. Available online: https://www.researchgate.net/publication/343678849_Estimacion_de_pobreza_a_nivel_municipal_en_Guatemala_mediante_la_utilizacion_de_machine_learning (accessed on 5 December 2022).
- World Health Organization. Achieving 70% COVID-19 Immunization Coverage by Mid-2022. 2021. Available online: https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022#:~:text=%5B4%5D%20These%20targets%20were%20then,population%20coverage%20by%20mid%2D2022 (accessed on 6 February 2023).
- R Core Team. R: A Language and Environment for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 18 December 2022).
- Infobae. Guatemala Starts Vaccination against COVID-19 for Children Aged 6 to 11. 2022. Available online: https://www.infobae.com/en/2022/03/14/guatemala-starts-vaccination-against-covid-19-for-children-aged-6-to-11/ (accessed on 23 January 2023).
- Gobierno de Guatemala Ministerio de Salud Publica y Asistencia Social. MSPAS Habilita Pruebas COVID-19 en dos Puestos de Vacunación. 2022. Available online: https://prensa.gob.gt/comunicado/mspas-habilita-pruebas-covid-19-en-dos-puestos-de-vacunacion (accessed on 6 February 2023).
- Lima, E.E.C.; Vilela, E.A.; Peralta, A.; Rocha, M.; Queiroz, B.L.; Gonzaga, M.R.; Piscoya-Díaz, M.; Martinez-Folgar, K.; García-Guerrero, V.M.; Freire, F.H.M.A. Investigating regional excess mortality during 2020 COVID-19 pandemic in selected Latin American countries. Genus 2021, 77, 30. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Folgar, K.; Alburez-Gutierrez, D.; Paniagua-Avila, A.; Ramirez-Zea, M.; Bilal, U. Excess Mortality during the COVID-19 Pandemic in Guatemala. Am. J. Public Health 2021, 111, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Akanbi, O.A. Structural and Institutional Determinants of Poverty in Sub-Saharan African Countries. J. Hum. Dev. Capab. 2015, 16, 122–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Source |
|---|---|
| Total municipality population | 2018 Guatemala Population and Housing Census |
| Female sex population in the municipality | 2018 Guatemala Population and Housing Census |
| Population aged 0–17 years in municipality | 2018 Guatemala Population and Housing Census |
| Population aged 18–59 years in municipality | 2018 Guatemala Population and Housing Census |
| Population aged 60 years or older in municipality | 2018 Guatemala Population and Housing Census |
| Ethnicity identification in the municipality | 2018 Guatemala Population and Housing Census |
| Population in a municipality having received at least primary school education | 2018 Guatemala Population and Housing Census |
| Population in municipality with household in a rural location | 2018 Guatemala Population and Housing Census |
| Population in municipality experiencing poverty | Figueroa Chavez et al., 2020 [30] |
| Department-level childhood mortality rate (deaths per 1000 livebirths) among children aged under five years | 2014–2015 Demographic and Health Survey |
| Percentage of women aged 15–49 years in department who reported having problems accessing health services when ill due to distance to a health establishment | 2014–2015 Demographic and Health Survey |
| Percent of children aged 12–23 months in the department who have received the third Pentavalent vaccine dose | 2014–2015 Demographic and Health Survey |
| Department Gini coefficient (%) | 2014–2015 Demographic and Health Survey |
| SARS-CoV-2 vaccination status among the municipality population aged six years or older (incomplete, complete, one booster dose, two booster doses) | Ministry of Public Health and Social Assistance (MSPAS) of Guatemala, 2021–2022 |
| Municipality population aged 60 years or older with completed SARS-CoV-2 primary vaccination course | Ministry of Public Health and Social Assistance (MSPAS) of Guatemala, 2021–2022 |
| SARS-CoV-2 tests reported per municipal population. | Ministry of Public Health and Social Assistance (MSPAS) of Guatemala, 2020–2022 |
| Deaths due to COVID-19 among the municipality population | Ministry of Public Health and Social Assistance (MSPAS) of Guatemala, 2020–2022 |
| Municipality Characteristic | N Median (IQR) | % a Median (IQR) |
|---|---|---|
| Population | 28,156.5 (15,730.8–51,426.0) | - |
| Female sex | 14,580.0 (8067.3–27,052.3) | 51.3 (50.6–52.2) |
| Age group (years) | ||
| 0–17 | 11,599.5 (6227.3–21,980.8) | 40.8 (37.4–45.3) |
| 18–59 | 14,131.0 (7891.3–25,263.5) | 51.1 (48.0–53.4) |
| ≥60 | 2226.0 (1321.0–3797.8) | 7.8 (6.9–9.3) |
| Ethnicity | ||
| Maya | 7129.0 (1008.8–25,847.5) | 30.0 (2.9–91.4) |
| Garifuna | 25.0 (13.0–50.8) | 0.1 (0.1–0.1) |
| Xinka | 4.0 (1.0–16.0) | 0.0 (0.0–0.1) |
| Latino(a) | 11,362.5 (2463.0–26,008.5) | 63.7 (8.2–93.5) |
| Educational level primary school and above | 18,065.0 (10,058.5–32,712.8) | 74.4 (68.5–78.9) |
| Household rural location | 13,458.5 (6260.5–28,052.5) | 64.8 (37.1–82.7) |
| People experiencing poverty | 16,086.0 (7909.0–30,343.5) | 60.8 (43.8–75.8) |
| SARS-CoV-2 vaccination status | ||
| Vaccine eligible population (≥6 years) | 27,156.0 (15,180.3–50,978.5) | - |
| Incomplete | 13,853.5 (7890.8–23,373.3) | 53.0 (43.0–66.6) |
| Complete | 10,633.5 (6286.3–18,466.8) | 42.3 (31.8–53.8) |
| One booster dose | 4813.0 (2887.5–8097.5) | 18.8 (13.1–27.0) |
| Two booster doses | 385.5 (183.8–952.0) | 1.7 (0.9–3.0) |
| MSPAS b SARS-CoV-2 indicators | ||
| Confirmed cases | 917.5 (442.0–1899.8) | 3.0 (1.7–5.4) |
| Tests reported | 5248.5 (2798.0–10,824.5) | 19.4 (10.7–28.6) |
| Deaths due to COVID-19 | 20.0 (10.0–38.0) | 0.07 (0.0–0.1) |
| People aged 60 or more years with complete vaccination | 1173.5 (733.8–2071.0) | 53.0 (41.5–66.9) |
| Measures as of 1 October 2021 | ||
| Complete vaccination | 3160.5 (1918.0–5897.8) | 13.1 (8.5–19.6) |
| Tests reported | 2129.0 (966.5–4492.8) | 7.9 (4.5–12.4) |
| Deaths due to COVID-19 | 16.5 (8.0–30.8) | 5.6 (3.2–9.5) |
| Departmental Characteristic | % Median (IQR) | |
| Under-5 childhood mortality rate (deaths per 1000 live births) | 37.0 (31.0–42.5) | |
| Difficult access to healthcare facilities due to distance | 38.6 (33.8–46.9) | |
| 12–23 months old children receiving third Pentavalent vaccine | 86.9 (82.0–90.4) | |
| Gini coefficient | 30.0 (30.0–40.0) |
| Bivariate Model | Full Multivariable Model | Simplified Multivariable Model | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | ||||
| Null multi-level model | 43.766 | 39.645 | 47.949 | 0.000 | 0.239 | ||||||||||
| Municipal level variables | 0.523 | 0.581 | 0.496 | 0.594 | |||||||||||
| % Mayan | −0.151 | −0.206 | −0.095 | 0.120 | 0.342 | 0.048 | −0.008 | 0.105 | - | - | - | ||||
| % Rural residence | −0.188 | −0.251 | −0.127 | 0.111 | 0.246 | 0.005 | −0.061 | 0.068 | - | - | - | ||||
| % Educational level primary school or above | 1.400 | 1.184 | 1.616 | 0.400 | 0.451 | 0.894 | 0.534 | 1.259 | 0.736 | 0.383 | 1.075 | ||||
| % Experiencing poverty | −0.542 | −0.625 | −0.460 | 0.405 | 0.462 | −0.216 | −0.409 | −0.026 | −0.249 | −0.433 | −0.070 | ||||
| % Female sex | 2.527 | 1.022 | 4.026 | 0.036 | 0.281 | 1.239 | −0.210 | 2.662 | - | - | - | ||||
| % in 0–17 age group | −1.813 | −2.158 | −1.470 | 0.296 | 0.388 | 0.999 | 0.296 | 1.714 | 1.065 | 0.355 | 1.767 | ||||
| % in 60 or older age group | 4.538 | 3.566 | 5.485 | 0.218 | 0.412 | 2.552 | 1.299 | 3.862 | 2.935 | 1.700 | 4.121 | ||||
| % tested for SARS-CoV-2 | 0.521 | 0.431 | 0.613 | 0.314 | 0.460 | 0.215 | 0.085 | 0.344 | 0.246 | 0.137 | 0.355 | ||||
| % died due to COVID-19 | 1.171 | 0.939 | 1.406 | 0.249 | 0.406 | 0.162 | -0.148 | 0.463 | - | - | - | ||||
| Departmental level variables | |||||||||||||||
| Under-5 childhood mortality rate | −0.087 | −0.461 | 0.268 | 0.003 | 0.249 | 0.199 | −0.035 | 0.424 | - | - | - | ||||
| % reporting difficulty accessing healthcare facilities due to distance | −0.822 | −1.121 | −0.532 | 0.176 | 0.249 | −0.053 | −0.447 | 0.338 | - | - | - | ||||
| % 12–23 month olds receiving third Pentavalent vaccine | 0.653 | 0.201 | 1.106 | 0.073 | 0.244 | 0.111 | −0.273 | 0.496 | - | - | - | ||||
| Gini coefficient | −0.619 | −1.195 | −0.084 | 0.052 | 0.245 | −0.145 | −0.594 | 0.298 | - | - | - | ||||
| Bivariate Model | Full Multivariable Model | Simplified Multivariable Model | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | ||||
| Null multi-level model | 55.119 | 50.395 | 59.914 | 0.000 | 0.246 | ||||||||||
| Municipal level variables | 0.477 | 0.615 | 0.487 | 0.600 | |||||||||||
| % Mayan | −0.205 | −0.268 | −0.143 | 0.162 | 0.415 | −0.016 | −0.080 | 0.050 | - | - | - | ||||
| % Rural residence | −0.181 | −0.253 | −0.112 | 0.079 | 0.241 | 0.097 | 0.027 | 0.165 | 0.094 | 0.027 | 0.159 | ||||
| % Educational level primary school or above | 1.649 | 1.394 | 1.903 | 0.409 | 0.513 | 0.965 | 0.558 | 1.377 | 0.978 | 0.566 | 1.372 | ||||
| % Experiencing poverty | −0.638 | −0.736 | −0.542 | 0.411 | 0.526 | −0.206 | −0.392 | −0.025 | −0.201 | −0.379 | −0.028 | ||||
| % Female sex | 2.370 | 0.662 | 4.073 | 0.025 | 0.269 | 1.887 | 0.250 | 3.504 | 2.057 | 0.639 | 3.451 | ||||
| % tested for SARS-CoV-2 | 0.595 | 0.492 | 0.699 | 0.310 | 0.484 | 0.301 | 0.151 | 0.451 | 0.314 | 0.190 | 0.437 | ||||
| % died due to COVID-19 | 1.271 | 1.003 | 1.543 | 0.213 | 0.441 | 0.037 | −0.318 | 0.385 | - | - | - | ||||
| Departmental level variables | |||||||||||||||
| Under-5 childhood mortality rate | −0.141 | −0.568 | 0.263 | 0.006 | 0.256 | 0.241 | −0.129 | 0.597 | - | - | - | ||||
| % reporting difficulty accessing healthcare facilities due to distance | −0.824 | −1.215 | −0.445 | 0.138 | 0.251 | 0.265 | −0.355 | 0.881 | - | - | - | ||||
| % 12–23 month olds receiving third Pentavalent vaccine | 0.641 | 0.099 | 1.181 | 0.055 | 0.252 | 0.147 | −0.449 | 0.743 | - | - | - | ||||
| Gini coefficient | −0.817 | −1.447 | −0.232 | 0.070 | 0.247 | −0.475 | −1.174 | 0.209 | - | - | - | ||||
| Bivariate Model | Full Multivariable Model | Simplified Multivariable Model | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | Coefficient | 95% Confidence Interval | Marginal R2 | Conditional R2 | ||||
| Null multi-level model | 15.205 | 13.290 | 17.150 | 0.000 | 0.183 | ||||||||||
| Municipal level variables | 0.550 | 0.615 | 0.546 | 0.615 | |||||||||||
| % Mayan | −0.091 | −0.118 | −0.063 | 0.166 | 0.307 | 0.023 | −0.005 | 0.051 | - | - | - | ||||
| % Rural residence | −0.106 | −0.138 | −0.074 | 0.130 | 0.223 | 0.001 | −0.032 | 0.032 | - | - | - | ||||
| % Educational level primary school or above | 0.715 | 0.601 | 0.829 | 0.384 | 0.438 | 0.230 | 0.049 | 0.413 | 0.161 | −0.012 | 0.328 | ||||
| % Experiencing poverty | −0.308 | −0.350 | −0.266 | 0.467 | 0.521 | −0.174 | −0.271 | −0.079 | −0.113 | −0.190 | −0.039 | ||||
| % Female sex | 1.039 | 0.246 | 1.829 | 0.023 | 0.225 | −0.022 | −0.752 | 0.695 | - | - | - | ||||
| % in 0–17 age group | −1.094 | −1.259 | −0.931 | 0.395 | 0.441 | 0.332 | −0.020 | 0.691 | - | - | - | ||||
| % in 60 or older age group | 2.832 | 2.351 | 3.301 | 0.315 | 0.450 | 1.679 | 1.053 | 2.335 | 1.393 | 0.893 | 1.873 | ||||
| % tested for SARS-CoV-2 | 0.621 | 0.521 | 0.722 | 0.358 | 0.455 | 0.203 | 0.063 | 0.341 | 0.262 | 0.146 | 0.380 | ||||
| % died due to COVID-19 | 0.784 | 0.646 | 0.923 | 0.304 | 0.397 | 0.140 | -0.048 | 0.323 | - | - | - | ||||
| Departmental level variables | |||||||||||||||
| Under-5 childhood mortality rate | −0.056 | −0.230 | 0.108 | 0.005 | 0.193 | 0.073 | −0.051 | 0.192 | - | - | - | ||||
| % reporting difficulty accessing healthcare facilities due to distance | −0.376 | −0.518 | −0.239 | 0.140 | 0.194 | −0.011 | −0.220 | 0.197 | - | - | - | ||||
| % 12–23 month olds receiving third Pentavalent vaccine | 0.290 | 0.080 | 0.501 | 0.056 | 0.180 | −0.015 | −0.218 | 0.188 | - | - | - | ||||
| Gini coefficient | −0.137 | −0.427 | 0.132 | 0.010 | 0.190 | 0.106 | −0.132 | 0.339 | - | - | - | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choudhary, R.; Carter, E.; Monzon, J.; Stewart, A.; Slotnick, J.; Samayoa Jerez, L.L.; Rodriguez Araujo, D.S.; Zielinski-Gutierrez, E.; Suchdev, P.S. Sociodemographic Factors Associated with COVID-19 Vaccination among People in Guatemalan Municipalities. Vaccines 2023, 11, 745. https://doi.org/10.3390/vaccines11040745
Choudhary R, Carter E, Monzon J, Stewart A, Slotnick J, Samayoa Jerez LL, Rodriguez Araujo DS, Zielinski-Gutierrez E, Suchdev PS. Sociodemographic Factors Associated with COVID-19 Vaccination among People in Guatemalan Municipalities. Vaccines. 2023; 11(4):745. https://doi.org/10.3390/vaccines11040745
Chicago/Turabian StyleChoudhary, Rewa, Emily Carter, Jose Monzon, Allison Stewart, Jennifer Slotnick, Leslie L. Samayoa Jerez, David S. Rodriguez Araujo, Emily Zielinski-Gutierrez, and Parminder S. Suchdev. 2023. "Sociodemographic Factors Associated with COVID-19 Vaccination among People in Guatemalan Municipalities" Vaccines 11, no. 4: 745. https://doi.org/10.3390/vaccines11040745
APA StyleChoudhary, R., Carter, E., Monzon, J., Stewart, A., Slotnick, J., Samayoa Jerez, L. L., Rodriguez Araujo, D. S., Zielinski-Gutierrez, E., & Suchdev, P. S. (2023). Sociodemographic Factors Associated with COVID-19 Vaccination among People in Guatemalan Municipalities. Vaccines, 11(4), 745. https://doi.org/10.3390/vaccines11040745