
Effectiveness and Protection Duration of Anti-COVID-19 Vaccinations among Healthcare Personnel in Cluj-Napoca, Romania

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
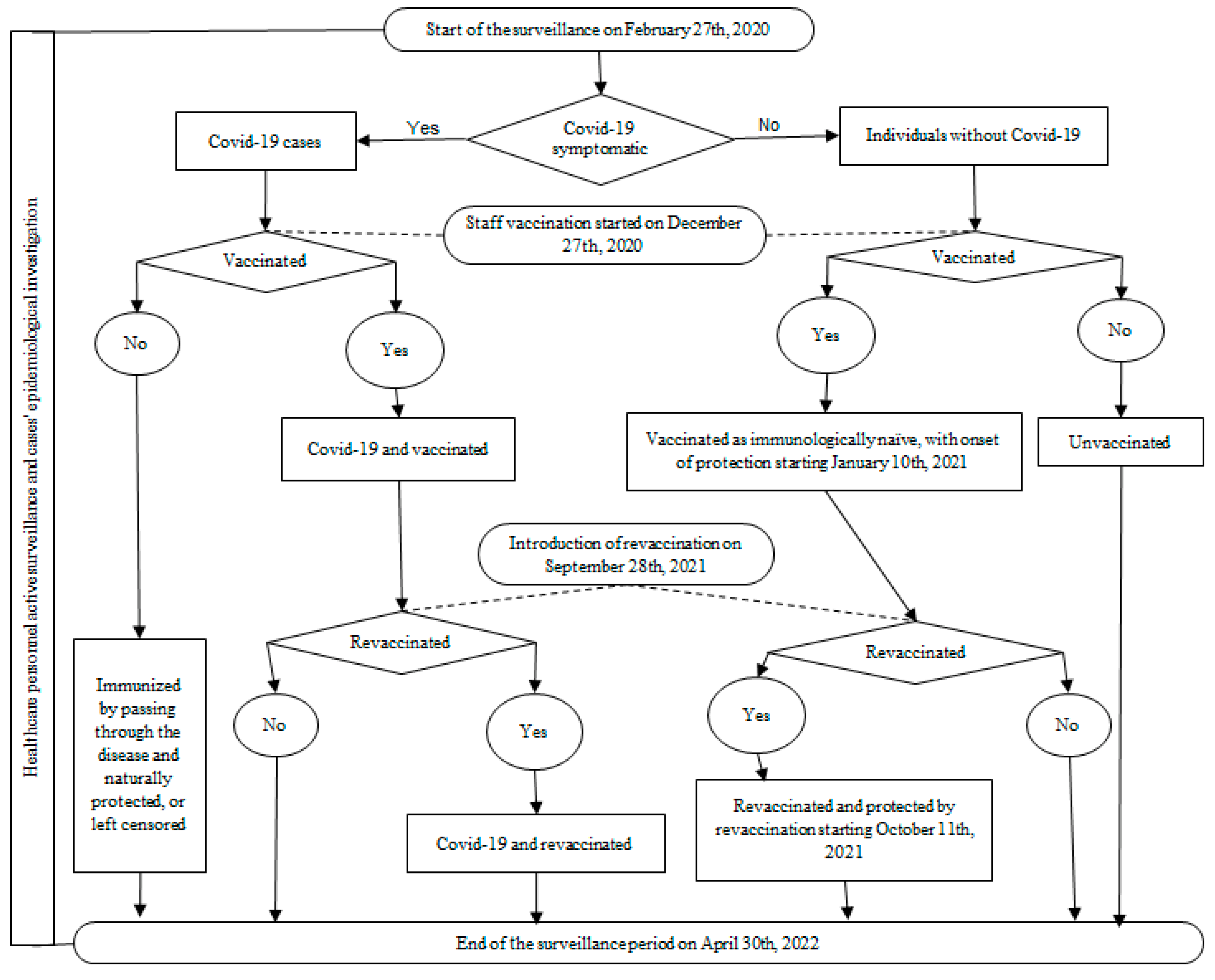
2.1. Study Design
2.2. Participants
2.3. Data Sources and Variables
2.4. Statistical Methods
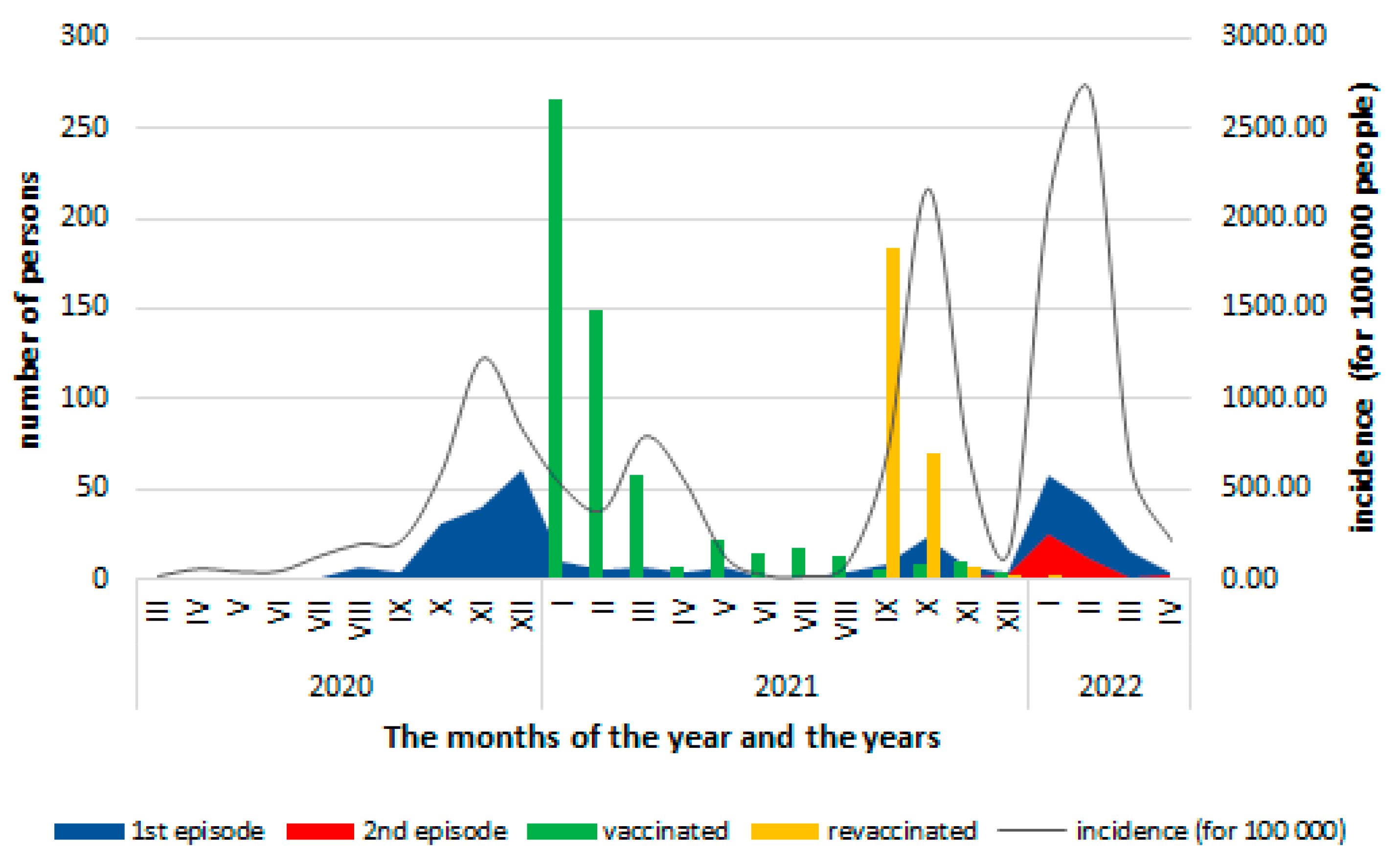
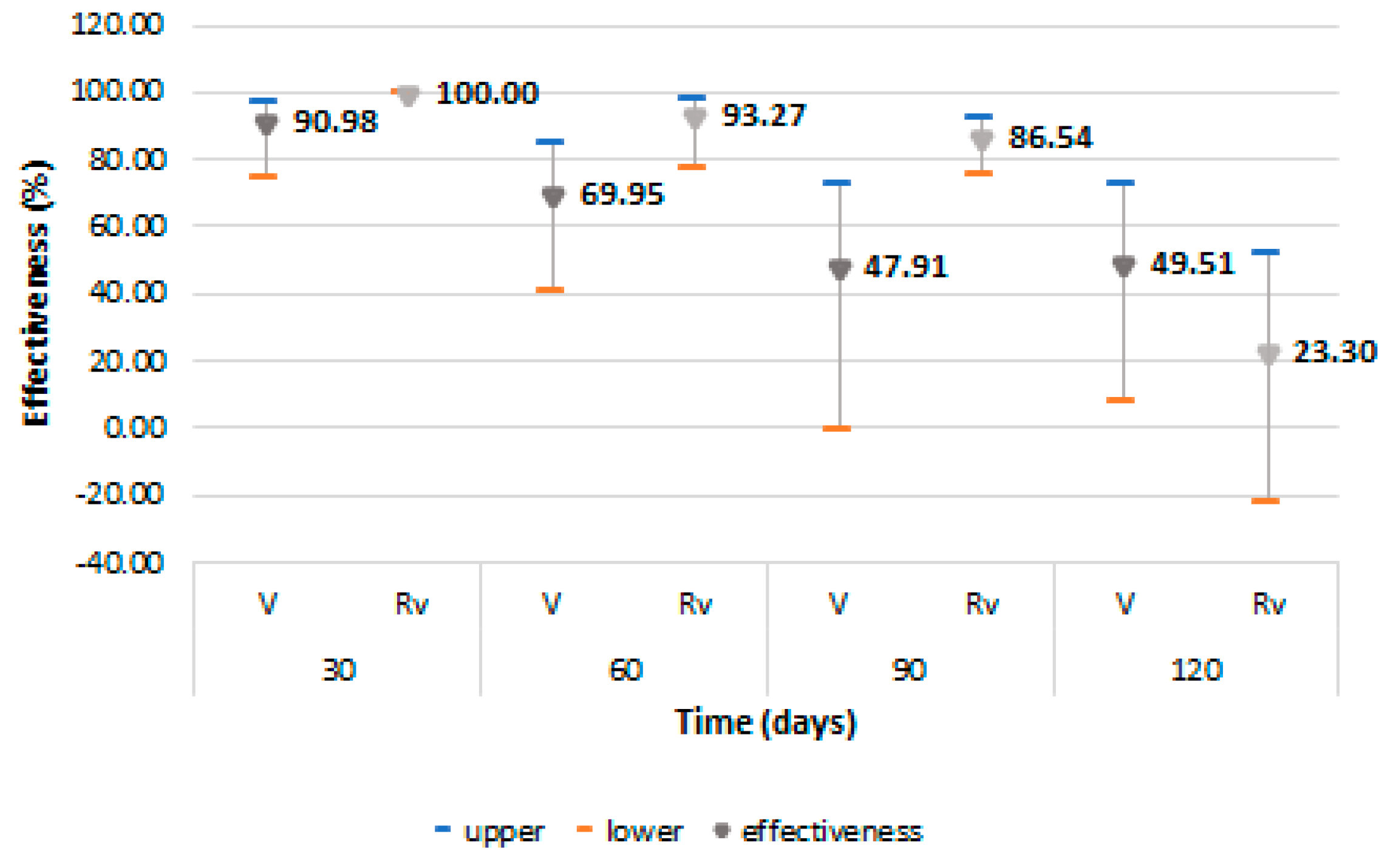
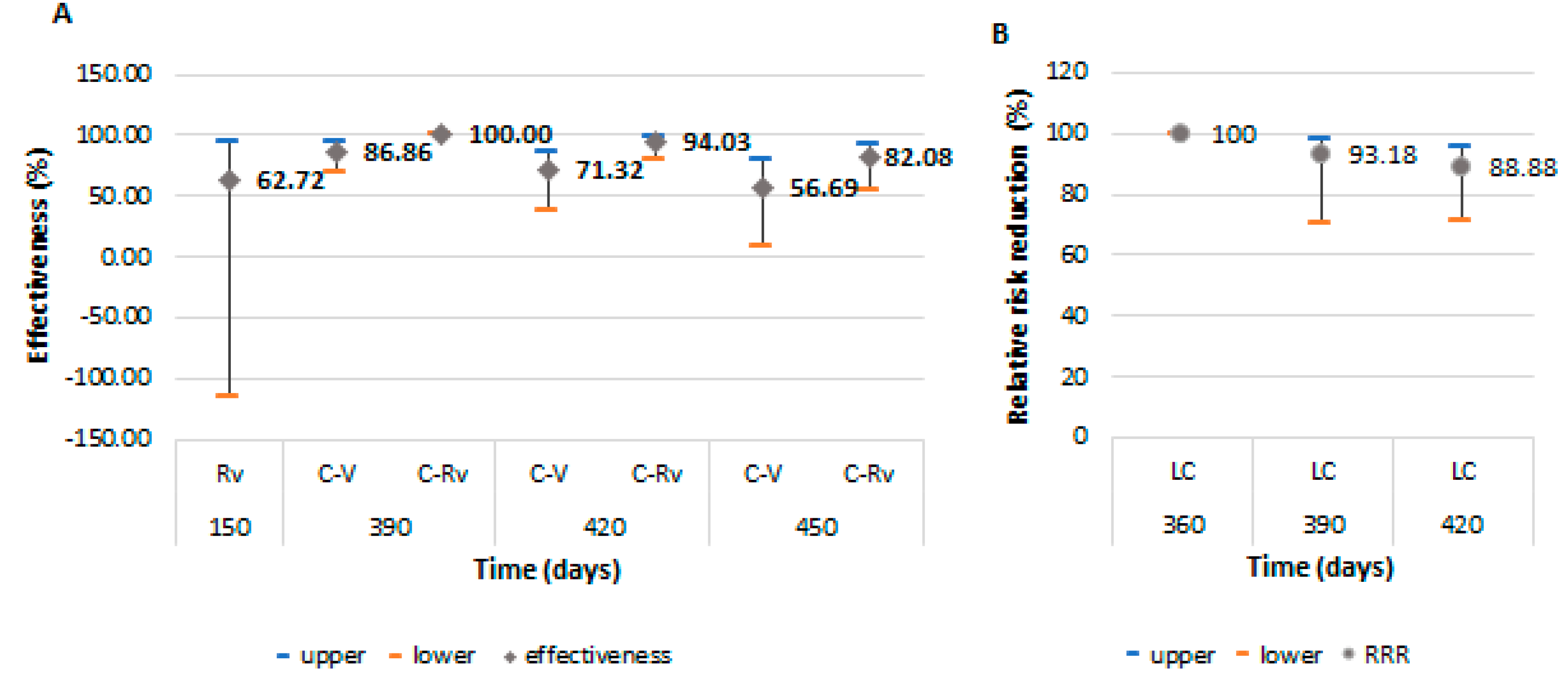
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Director-General’s opening remarks at the media briefing on COVID-19–11 March 2020. World Health Organization. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 25 September 2022).
- 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan. World Health Organization (WHO). Creative Commons Attribution Non-Commercial Share Alike 3.0 IGO licence CC BY NC SA 3.0 IGO. Geneva, Switzerland. 4 February 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/strategies-and-plans (accessed on 24 September 2022).
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. COVID-19 Situation Update—Download COVID-19 Data Sets: Download Historical Data (to 14 December 2020) on the Daily Number of New Reported COVID-19 Cases and Deaths Worldwide. Available online: https://www.ecdc.europa.eu/en/covid-19/data (accessed on 21 August 2022).
- Funk, C.D.; Laferrière, C.; Ardakani, A. Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective. Viruses 2021, 13, 418. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. COVID-19 Vaccines: Authorised. Vaccines Authorised in the European Union (EU) to Prevent COVID-19, Following Evaluation by the European Medicines Agency (EMA). Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/vaccines-covid-19/covid-19-vaccines-authorised#originally-authorised-covid-19-vaccines-section (accessed on 24 September 2022).
- European Centre for Diseases Prevention and Control. Efficacy, Effectiveness and Safety of EU/EEA-Authorised Vaccines against COVID-19: Living Systematic Review. Update 23 February 2022. Available online: https://www.ecdc.europa.eu/en/covid-19-efficacy-effectiveness-and-safety-vaccines (accessed on 21 August 2022).
- Orenstein, W.A.; Bernier, R.H.; Dondero, T.J.; Hinman, A.R.; Marks, J.S.; Bart, K.J.; Sirotkin, B. Field evaluation of vaccine efficacy. Bull. World Health Organ. 1985, 63, 1055–1068. [Google Scholar] [PubMed]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.K.; Bergeri, I.; Bresee, J.S.; Cowling, B.J.; Crowcroft, N.S.; Fahmy, K.; Hirve, S.; Kang, G.; Katz, M.A.; Lanata, C.F.; et al. Evaluation of post-introduction COVID-19 vaccine effectiveness: Summary of interim guidance of the World Health Organization. Vaccines 2021, 39, 4013–4024. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Evaluation of COVID-19 Vaccine Effectiveness: Interim Guidance, 17 March 2021. License: CC BY-NC-SA 3.0 IGO. World Health Organization. 2021. Available online: https://apps.who.int/iris/handle/10665/340301 (accessed on 30 August 2022).
- Cohort Study to Measure COVID-19 Vaccine Effectiveness among Health Workers in WHO European Region: Guidance Document. Copenhagen: WHO Regional Office for Europe; Licence: CC BY-NC-SA 3.0 IGO. 2021. Available online: https://apps.who.int/iris/handle/10665/340217 (accessed on 21 August 2022).
- Clinical Management of COVID-19: Living Guideline, 23 June 2022. (WHO/2019-nCoV/Clinical/2022.1). License: CC BY-NC-SA 3.0 IGO. World Health Organization: Geneva, Switzerland, 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2022-1 (accessed on 30 August 2022).
- Hackshaw, A. Statistical formulae for calculating some 95% confidence intervals. In A Concise Guide to Clinical Trials; Wiley-Blackwell: Hoboken, NJ, USA, 2009; pp. 205–207. [Google Scholar]
- European Centre for Disease Prevention and Control. Generic Protocol for COVID-19 Vaccine Effectiveness Studies during Outbreaks in Semi-Closed Settings in the EU/EEA–Version 1.0. ECDC: Stockholm, Sweden, 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-vaccine-effectiveness-outbreaks-semi-closed-settings (accessed on 21 August 2022).
- Zhu, Z.; Xu, L.; Chen, G. Is there a difference in the efficacy of COVID-19 vaccine in males and females?—A systematic review and meta-analysis. Hum. Vaccin. Immunother. 2021, 17, 4741–4746. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Euro Surveill. 2021, 26, 2100420. [Google Scholar] [CrossRef]
- Pilishvili, T.; Gierke, R.; Fleming-Dutra, K.E.; Farrar, J.L.; Mohr, N.M.; Talan, D.A.; Krishnadasan, A.; Harland, K.K.; Smithline, H.A.; Hou, P.C.; et al. Vaccine Effectiveness among Healthcare Personnel Study Team. Effectiveness of mRNA COVID-19 Vaccine among U.S. Health Care Personnel. N. Engl. J. Med. 2021, 385, e90. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Ayoub, H.H.; Al Mukdad, S. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat. Commun. 2022, 13, 3082. [Google Scholar] [CrossRef] [PubMed]
- Heftdal, L.D.; Schultz, M.; Lange, T.; Knudsen, A.D.; Fogh, K.; Hasselbalch, R.B.; Linander, C.B.; Kallemose, T.; Bundgaard, H.; Grønbæk, K.; et al. Incidence of Positive Severe Acute Respiratory Syndrome Coronavirus Polymerase Chain Reaction after Coronavirus Disease 2019 Vaccination with up to 8 Months of Follow-up: Real-life Data from the Capital Region of Denmark. Clin. Infect Dis. 2022, 75, e675–e682. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Public Health; National Center for Surveillance and Control of Communicable Diseases. Information on Confirmed Cases of COVID-19 with Variants of SARS-CoV-2, Causing Concern (VOC). Cumulative Data—Including Week 34 (22/08/2022–28/08/2022). Available online: https://www.cnscbt.ro/index.php/analiza-cazuri-confirmate-covid19/3307-s-34-informare-cazuri-cu-variante-care-determina-ingrijorare-voc-1/file (accessed on 30 August 2022).
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Hasan, M.R.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Al-Kanaani, Z.; Al-Kuwari, E.; et al. Protective Effect of Previous SARS-CoV-2 Infection against Omicron BA.4 and BA.5 Subvariants. N. Engl. J. Med. 2022, 387, 1620–1622. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Bertollini, R.; National Study Group for COVID-19 Epidemiology. Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections. N. Engl. J. Med. 2021, 385, 2487–2489. [Google Scholar] [CrossRef] [PubMed]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Herzel, E.; Alapi, H.; Cohen, D.; Muhsen, K.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Naturally Acquired Immunity versus Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: A Retrospective Cohort Study. Clin. Infect Dis. 2022, 75, e545–e551. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; Al Kanaani, Z.; et al. Association of Prior SARS-CoV-2 Infection with Risk of Breakthrough Infection Following mRNA Vaccination in Qatar. JAMA 2021, 326, 1930–1939. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Sample (n = 783) | First COVID-19 Episode (n = 335) | Second COVID-19 Episode (n = 40) | Without COVID-19 (n = 448) | p a | ||||
|---|---|---|---|---|---|---|---|---|---|
| Age (Years) | Value | Range | Value | Range | Value | Range | Value | Range | |
| Mean | 45.06 | 19.65–68.76 | 44.17 | 19.99–68.54 | 41.85 | 25.98–59.72 | 45.72 | 19.65–68.76 | 0.054 |
| Gender | no | % | no | % | no | % | no | % | |
| Female | 641 | 81.86 | 277 | 82.69 | 32 | 80.00 | 364 | 81.25 | 0.691 |
| Male | 142 | 18.14 | 58 | 17.31 | 8 | 20.00 | 84 | 18.75 | 0.691 |
| Occupation | |||||||||
| Administrative | 116 | 14.81 | 50 | 14.92 | 10 | 25.00 | 66 | 14.73 | 0.628 |
| Care staff | 193 | 24.65 | 64 | 19.10 | 4 | 10.00 | 129 | 28.80 | 0.009 |
| Nurse | 291 | 37.16 | 145 | 43.28 | 22 | 55.00 | 146 | 32.59 | 0.010 |
| Pharmacist | 7 | 0.89 | 4 | 1.20 | 0 | 0 | 3 | 0.67 | 0.707 b |
| Physician | 176 | 22.48 | 72 | 21.49 | 4 | 10.00 | 104 | 23.21 | 0.311 |
| Clinical unit category | |||||||||
| Administration | 115 | 14.68 | 52 | 15.52 | 10 | 25.00 | 63 | 14.10 | 0.331 |
| Ambulatory | 180 | 22.98 | 87 | 25.97 | 8 | 20.00 | 93 | 20.76 | 0.133 |
| Clinical unit | 377 | 48.15 | 148 | 44.18 | 14 | 35.00 | 229 | 51.12 | 0.025 |
| Pharmacy | 8 | 1.02 | 5 | 1.49 | 0 | 0 | 3 | 0.67 | 0.480 b |
| Laboratory | 72 | 9.20 | 32 | 9.55 | 5 | 12.50 | 40 | 8.93 | 0.719 |
| Radiology | 31 | 3.96 | 11 | 3.28 | 3 | 7.50 | 20 | 4.46 | 0.726 |
| Vaccination | |||||||||
| Fully vaccinated -before first episode -after first episode | 570 463 107 | 72.80 59.13 13.67 | 245 138 107 | 73.13 41.19 31.94 | 23 3 20 | 57.50 7.50 50.00 | 325 - - | 72.54 - - | 0.033 0.004 0.041 |
| Booster -before first episode -after first episode | 262 222 40 | 33.46 28.35 5.11 | 101 58 43 | 30.15 17.31 12.83 | 7 1 6 | 17.50 2.50 15.00 | 161 - - | 35.94 - - | 0.031 0.011 0.609 |
| Non-vaccinated | 213 c | 27.20 | 90 d | 26.87 | 17 | 42.50 | 123 e | 27.46 | 0.046 |
| Vaccine type | |||||||||
| Comirnaty | 534 c | 68.20 | 225 d | 67.16 | 20 | 50.00 | 309 e | 68.97 | 0.251 |
| Janssen | 33 | 4.22 | 18 | 5.37 | 2 | 5.00 | 15 | 3.35 | 0.330 |
| Vaxzevria | 5 | 0.64 | 2 | 0.60 | 1 | 2.50 | 3 | 0.67 | 0.197 |
| Spikevax | 1 | 0.13 | 1 | 0.30 | 0 | 0 | 0 | 0 | 0.377 b |
| Parameter | First COVID-19 Episode (n = 335) | Second COVID-19 Episode (n = 40) | p-Value | ||
|---|---|---|---|---|---|
| No. | % | No. | % | - | |
| Clinical forms | |||||
| Critical disease | 1 | 0.29 | 0 | 0 | 0.976 a |
| Severe disease | 2 | 0.60 | 0 | 0 | 0.994 a |
| Moderate disease | 58 | 17.32 | 3 | 7.50 | <0.0001 |
| Mild disease | 274 | 81.79 | 37 | 92.50 | <0.0001 |
| Hospitalization | |||||
| Intensive care | 1 | 0.30 | 0 | 0 | 0.996 a |
| Hospital stay/hospitalization | 51 | 15.22 | 0 | 0 | 0.003 a |
| Outpatient evaluation | 193 | 57.61 | 11 | 27.50 | <0.001 |
| Without evaluation | 90 | 26.87 | 29 | 72.50 | <0.0001 |
| Associated diseases | |||||
| Present concomitant diseases | 145 | 43.28 | 18 | 45.00 | 0.527 |
| Cardiovascular diseases | 66 | 19.70 | 10 | 25.00 | 0.549 |
| Obesity | 47 | 14.03 | 7 | 17.50 | 0.644 |
| Endocrine and metabolic diseases | 40 | 11.94 | 3 | 7.50 | 0.607 |
| Allergic diseases | 33 | 9.85 | 6 | 15.00 | 0.491 |
| Digestive diseases | 18 | 5.37 | 1 | 2.50 | 0.709 |
| Respiratory diseases | 17 | 4.78 | 3 | 7.50 | 0.475 |
| Neoplasia | 5 | 1.49 | 1 | 2.50 | 0.506 |
| Other diseases | 48 | 14.33 | 3 | 7.50 | 0.341 |
| Source of contamination | |||||
| unknown | 180 | 53.73 | 20 | 50.00 | 0.738 |
| community | 113 | 33.73 | 16 | 40.00 | 0.482 |
| patients | 25 | 7.46 | 1 | 2.50 | 0.338 |
| colleague | 9 | 2.69 | 0 | 0 | 0.606 a |
| office | 8 | 2.39 | 3 | 7.50 | 0.101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brumboiu, M.I.; Iuga, E.; Ivanciuc, A.; Mutaffof, S.; Tudosa, A.S.; Gherasimovici, C.; Iaru, I. Effectiveness and Protection Duration of Anti-COVID-19 Vaccinations among Healthcare Personnel in Cluj-Napoca, Romania. Vaccines 2023, 11, 521. https://doi.org/10.3390/vaccines11030521
Brumboiu MI, Iuga E, Ivanciuc A, Mutaffof S, Tudosa AS, Gherasimovici C, Iaru I. Effectiveness and Protection Duration of Anti-COVID-19 Vaccinations among Healthcare Personnel in Cluj-Napoca, Romania. Vaccines. 2023; 11(3):521. https://doi.org/10.3390/vaccines11030521
Chicago/Turabian StyleBrumboiu, Maria I., Edina Iuga, Andreea Ivanciuc, Sergiu Mutaffof, Alice S. Tudosa, Cristina Gherasimovici, and Irina Iaru. 2023. "Effectiveness and Protection Duration of Anti-COVID-19 Vaccinations among Healthcare Personnel in Cluj-Napoca, Romania" Vaccines 11, no. 3: 521. https://doi.org/10.3390/vaccines11030521
APA StyleBrumboiu, M. I., Iuga, E., Ivanciuc, A., Mutaffof, S., Tudosa, A. S., Gherasimovici, C., & Iaru, I. (2023). Effectiveness and Protection Duration of Anti-COVID-19 Vaccinations among Healthcare Personnel in Cluj-Napoca, Romania. Vaccines, 11(3), 521. https://doi.org/10.3390/vaccines11030521