
Risks of Cardiac Arrhythmia Associated with COVID-19 Vaccination: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Items and Collection Process
2.5. Risk of Bias and Quality Assessment
2.6. Data Synthesis
3. Results
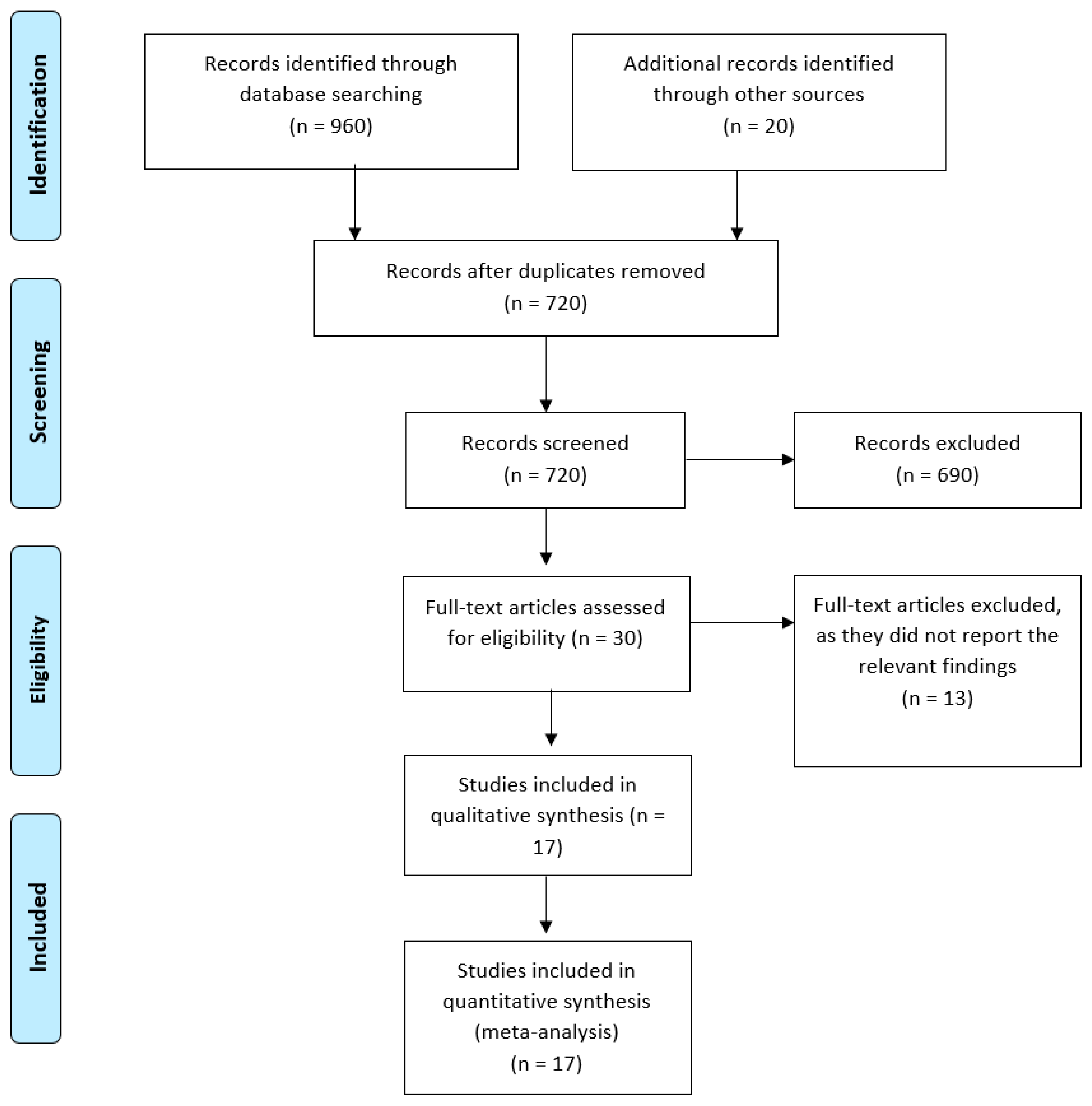
3.1. Study Selection
3.2. Characteristics of Included Studies and Patients
3.3. Quality of the Included Studies
3.4. Meta-Analysis
3.4.1. Incidence of Cardiac Arrhythmia
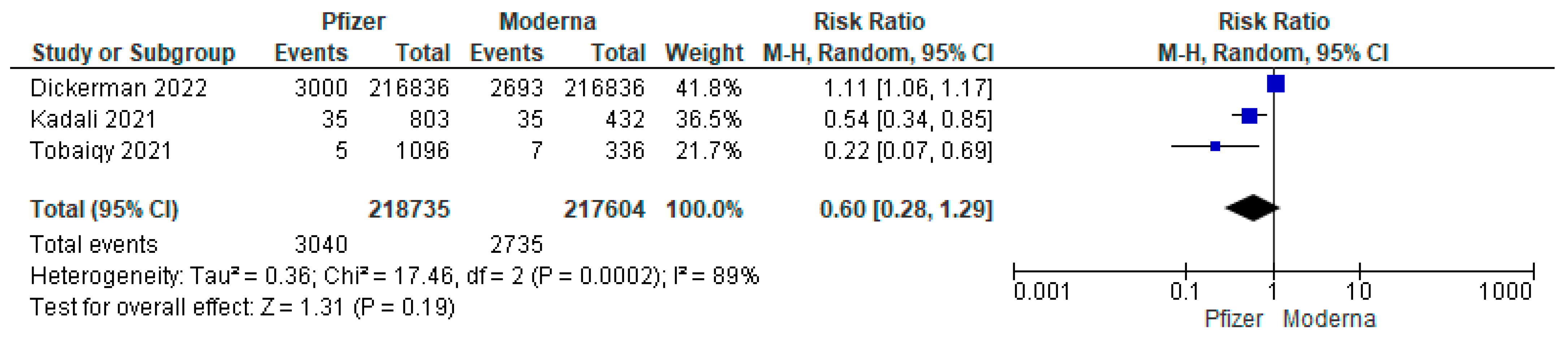
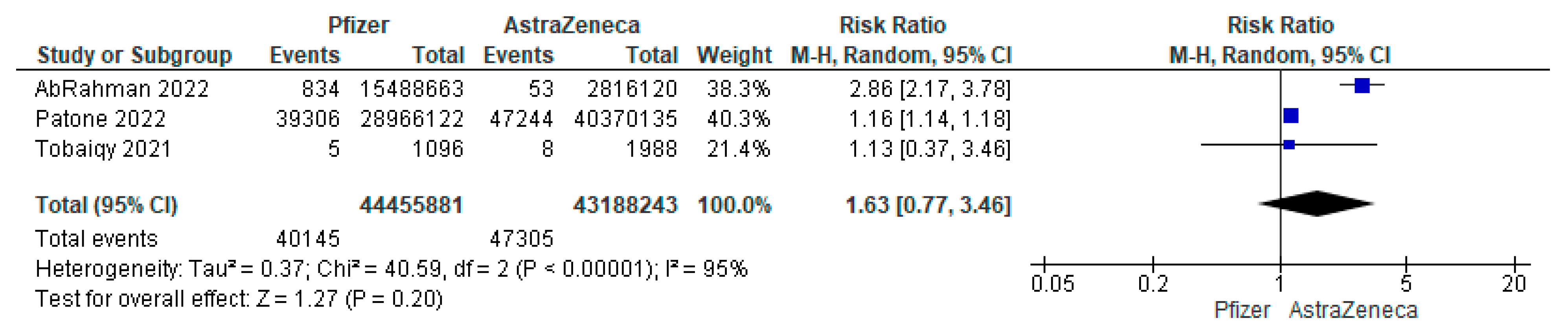
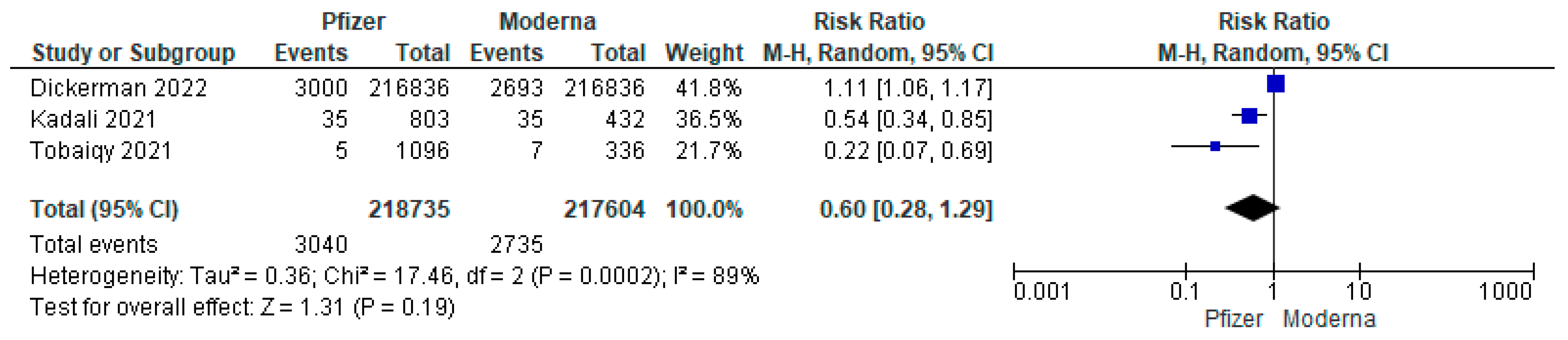
3.4.2. Subgroup Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, F.; Liu, Y.; Mo, M.; Chen, J.; Wang, C.; Yang, Y.; Wu, J. Current Treatment Strategies for COVID-19 (Review). Mol. Med. Rep. 2021, 24, 858. [Google Scholar] [CrossRef] [PubMed]
- Baral, P.K.; Yin, J.; James, M.N.G. Treatment and Prevention Strategies for the COVID 19 Pandemic: A Review of Immunotherapeutic Approaches for Neutralizing SARS-CoV-2. Int. J. Biol. Macromol. 2021, 186, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-Y.; Wang, S.-H.; Tang, Y.; Sheng, W.; Zuo, C.-J.; Wu, D.-W.; Fang, H.; Du, Q.; Li, N. Landscape and Progress of Global COVID-19 Vaccine Development. Hum. Vaccin. Immunother. 2021, 17, 3276–3280. [Google Scholar] [CrossRef] [PubMed]
- Ebada, M.A.; Allah, A.W.; Bahbah, E.; Negida, A. An Updated Review on COVID-19. Infect. Disord. Drug Targets 2021, 21, e160921189190. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 12 August 2022).
- Verbeke, R.; Lentacker, I.; De Smedt, S.C.; Dewitte, H. The Dawn of MRNA Vaccines: The COVID-19 Case. J. Control. Release 2021, 333, 511–520. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Brown, E.S.; Cheeseman, H.M.; Flight, K.E.; Higham, S.L.; Lemm, N.-M.; Pierce, B.F.; Stirling, D.C.; Wang, Z.; Pollock, K.M. Vaccines for COVID-19. Clin. Exp. Immunol. 2020, 202, 162–192. [Google Scholar] [CrossRef]
- Kyriakidis, N.C.; López-Cortés, A.; González, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 Vaccines Strategies: A Comprehensive Review of Phase 3 Candidates. npj Vaccines 2021, 6, 28. [Google Scholar] [CrossRef]
- Heinz, F.X.; Stiasny, K. Distinguishing Features of Current COVID-19 Vaccines: Knowns and Unknowns of Antigen Presentation and Modes of Action. npj Vaccines 2021, 6, 104. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Omran, D.; Al Soda, M.; Bahbah, E.; Esmat, G.; Shousha, H.; Elgebaly, A.; Abdel Ghaffar, M.; Alsheikh, M.; El Sayed, E.; Afify, S.; et al. Predictors of Severity and Development of Critical Illness of Egyptian COVID-19 Patients: A Multicenter Study. PLoS ONE 2021, 16, e0256203. [Google Scholar] [CrossRef]
- AbdelGhaffar, M.M.; Omran, D.; Elgebaly, A.; Bahbah, E.I.; Afify, S.; AlSoda, M.; El-Shiekh, M.; ElSayed, E.S.; Shaaban, S.S.; AbdelHafez, S.; et al. Prediction of Mortality in Hospitalized Egyptian Patients with Coronavirus Disease-2019: A Multicenter Retrospective Study. PLoS ONE 2022, 17, e0262348. [Google Scholar] [CrossRef] [PubMed]
- García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Hernández-Vanegas, L.E.; Núñez, I.; Hernández-Valdivia, N.; Carrillo-García, D.A.; Michel-Chávez, A.; Galnares-Olalde, J.A.; Carbajal-Sandoval, G.; Del Mar Saniger-Alba, M.; et al. Neurologic Adverse Events among 704,003 First-Dose Recipients of the BNT162b2 MRNA COVID-19 Vaccine in Mexico: A Nationwide Descriptive Study. Clin. Immunol. 2021, 229, 108786. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 MRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events After COVID-19 MRNA Vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Abdelgawad, H.A.H.; Sayed, A.; Munir, M.; Elberry, M.H.; Sayed, I.M.; Kamal, M.A.; Negida, A.; Ebada, M.A.; Bahbah, E.I. Clinical Review of COVID-19; Pathogenesis, Diagnosis, and Management. Curr. Pharm. Des. 2021, 27, 4232–4244. [Google Scholar] [CrossRef]
- Matar, R.H.; Mansour, R.; Nakanishi, H.; Smayra, K.; El Haddad, J.; Vankayalapati, D.K.; Daniel, R.S.; Tosovic, D.; Than, C.A.; Yamani, M.H. Clinical Characteristics of Patients with Myocarditis Following COVID-19 MRNA Vaccination: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4521. [Google Scholar] [CrossRef]
- Chou, O.H.I.; Mui, J.; Chung, C.T.; Radford, D.; Ranjithkumar, S.; Evbayekha, E.; Nam, R.; Pay, L.; Satti, D.I.; Garcia-Zamora, S.; et al. COVID-19 Vaccination and Carditis in Children and Adolescents: A Systematic Review and Meta-Analysis. Clin. Res. Cardiol. 2022, 111, 1161–1173. [Google Scholar] [CrossRef]
- Parmar, K.; Subramanyam, S.; Del Rio-Pertuz, G.; Sethi, P.; Argueta-Sosa, E. Cardiac Adverse Events after Vaccination-A Systematic Review. Vaccines 2022, 10, 700. [Google Scholar] [CrossRef]
- Samimisedeh, P.; Jafari Afshar, E.; Shafiabadi Hassani, N.; Rastad, H. Cardiac MRI Findings in COVID-19 Vaccine-Related Myocarditis: A Pooled Analysis of 468 Patients. J. Magn. Reson. Imaging 2022, 56, 971–982. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. Myopericarditis Following COVID-19 Vaccination and Non-COVID-19 Vaccination: A Systematic Review and Meta-Analysis. Lancet. Respir. Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, version 5; Wiley online library: Hoboken, NJ, USA, 2008; ISBN 9780470699515. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Montano, D. Frequency and Associations of Adverse Reactions of COVID-19 Vaccines Reported to Pharmacovigilance Systems in the European Union and the United States. Front. Public Health 2022, 9, 756633. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of Myocarditis, Pericarditis, and Cardiac Arrhythmias Associated with COVID-19 Vaccination or SARS-CoV-2 Infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Balicer, R. Adverse Effects after BNT162b2 Vaccine and SARS-CoV-2 Infection, According to Age and Sex. N. Engl. J. Med. 2021, 27, 2115045. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Madenci, A.L.; Gerlovin, H.; Kurgansky, K.E.; Wise, J.K.; Figueroa Muñiz, M.J.; Ferolito, B.R.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; et al. Comparative Safety of BNT162b2 and MRNA-1273 Vaccines in a Nationwide Cohort of US Veterans. JAMA Intern. Med. 2022, 182, 739. [Google Scholar] [CrossRef] [PubMed]
- El-shitany, N.A.; Bagher, A.M.; Binmahfouz, L.S.; Eid, B.G.; Almukadi, H.; Badr-eldin, S.M.; El-hamamsy, M.; Mohammedsaleh, Z.M.; Saleh, F.M.; Almuhayawi, M.S.; et al. The Adverse Reactions of Pfizer BioNTech COVID-19 Vaccine Booster Dose Are Mild and Similar to the Second Dose Responses: A Retrospective Cross-Sectional Study. Int. J. Gen. Med. 2022, 15, 6821–6836. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side Effects of BNT162b2 MRNA COVID-19 Vaccine: A Randomized, Cross-Sectional Study with Detailed Self-Reported Symptoms from Healthcare Workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Gajula, V.; Madathala, R.R.; Chennaiahgari, N.; Malayala, S.V. Non-life-threatening Adverse Effects with COVID-19 MRNA-1273 Vaccine: A Randomized, Cross-sectional Study on Healthcare Workers with Detailed Self-reported Symptoms. J. Med. Virol. 2021, 93, 4420–4429. [Google Scholar] [CrossRef]
- Kaur, U.; Ojha, B.; Kumar, B.; Singh, A.; Giri, K.R.; Singh, A.; Das, A.; Misra, A.; Kumar, A.; Kansal, S.; et al. EClinicalMedicine A Prospective Observational Safety Study on ChAdOx1 NCoV-19 Corona Virus Vaccine (Recombinant) Use in Healthcare Workers- Fi Rst Results from India. EClinicalMedicine 2021, 38, 101038. [Google Scholar] [CrossRef]
- Kaur, R.; Dutta, S.; Charan, J.; Bhardwaj, P.; Tandon, A.; Yadav, D.; Islam, S.; Haque, M. Cardiovascular Adverse Events Reported from COVID-19 Vaccines: A Study Based on WHO Database. Int. J. Gen. Med. 2021, 14, 3909–3927. [Google Scholar] [CrossRef]
- Tan, J.T.C.; Tan, C.; Teoh, J.; Mt, W.; Zhong, G.; Mbbs, T.; Yew, R.; Chin, Z.; Lee, A.; Mutalib, A.; et al. Adverse Reactions and Safety Profile of the MRNA COVID-19 Vaccines among Asian Military Personnel. Ann. Acad. Med. Singap. 2021, 50, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Tobaiqy, M.; Maclure, K.; Elkout, H. Thrombotic Adverse Events Reported for Moderna, Pfizer and Oxford-AstraZeneca COVID-19 Vaccines: Comparison of Occurrence and Clinical Outcomes in the EudraVigilance Database. Vaccines 2021, 9, 1326. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; Thacker, D.; Elias, M.D.; Li, J.S.; Toro-Salazar, O.H.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis After COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Lau, K.T.K.; Xiong, X.; Au, I.C.H.; Lai, F.T.T.; Wan, E.Y.F.; Chui, C.S.L.; Li, X.; Chan, E.W.Y.; Gao, L.; et al. Adverse Events of Special Interest and Mortality Following Vaccination with MRNA (BNT162b2) and Inactivated (CoronaVac) SARS-CoV-2 Vaccines in Hong Kong: A Retrospective Study. PLOS Med. 2022, 19, e1004018. [Google Scholar] [CrossRef]
- Dizbay, M.; Şenol, E. Evaluation of the Frequency of Side Effects after Coronovirus Inactive Vero Cell Vaccine in Healthcare Workers of Gazi University Hospital. Gazi Med. J. 2021, 32, 651–654. [Google Scholar]
- Ab Rahman, N.; Tsuey, M.; Yee, F.; Chet, S.; Ramli, A. Risk of Serious Adverse Events after the BNT162b2, CoronaVac, and ChAdOx1 Vaccines in Malaysia: A Self-Controlled Case Series Study. Vaccine 2022, 40, 4394–4402. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 MRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Dai, H.; Zhang, Q.; Much, A.A.; Maor, E.; Segev, A.; Beinart, R.; Adawi, S.; Lu, Y.; Bragazzi, N.L.; Wu, J. Global, Regional, and National Prevalence, Incidence, Mortality, and Risk Factors for Atrial Fibrillation, 1990–2017: Results from the Global Burden of Disease Study 2017. Eur. Heart J.—Qual. Care Clin. Outcomes 2021, 7, 574–582. [Google Scholar] [CrossRef]
- Publishing Service. Government of UK COVID-19 MRNA Pfizer- BioNTech Vaccine Analysis Print. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/989996/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print.pdf (accessed on 20 July 2022).
- AstraZeneca COVID-19 Vaccine AstraZeneca Analysis Print; 30 May 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1121352/COVID-19_Vaccine_AstraZeneca_VAP.pdf (accessed on 12 August 2022).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Country | Study Design | Groups | Number of Each Group | Sample Size | Age | Male, n (%) | Any Other Heart Diseases | Hypertension | Coronary Artery Disease | Left Ventricular Dysfunction | MI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AbRahman et al., 2022 [39] | Malaysia | Self-controlled case-series study | BNT162b2 | 15,387,585 | 35,201,509 * | From 12 to 60 years and above | 4,485,174 | 844 (13.83) d | 3061 (50.16) d | NA | NA | NA |
| CoronaVac | 17,030,243 | 4,376,900 | ||||||||||
| ChAdOx1 | 2,744,507 | 1,008,040 | ||||||||||
| Barda et al., 2021 [40] | Israel | Retrospective registry-based analysis | BNT162b2 | 884,828 | 1,769,656 | 39.333 (19.274) a | 461,590 (52) | 31,836 (4) | 94,819 (11) | NA | NA | NA |
| Control | 884,828 | 39.333 (19.274) a | 461,590 (52) | 31,596 (4) | 93,357 (11) | |||||||
| Dagan et al., 2021 [26] | Israel | Subgroup analysis of Barda 2021 study | BNT162b2 | 884,828 | 1,769,656 | 39.333 (19.274) a | 461,590 (52) | 31,836 (4) | 94,819 (11) | NA | NA | NA |
| Control | 884,828 | 39.333 (19.274) a | 461,590 (52) | 31,596 (4) | 93,357 (11) | |||||||
| Dickerman et al., 2022 [27] | US | Cohort Study | BNT162b2 | 216,836 | 433,672 | 67.667 (10.378) a | 200,908 (93) | 59,153 (27) b | 137,265 (63) | NA | NA | NA |
| mRNA-1273 | 216,836 | 67.667 (10.378) a | 200,908 (93) | 59,266 (27) b | 140,774 (65) | |||||||
| El-Shitany et al., 2022 [28] | Saudi Arabia | Cross-Sectional | BNT162b2 | 422 | 422 | Any age groups c | 123 (27.8) | NA | 94 (58.4) | NA | NA | NA |
| Kadali et al., 2021 [29] | US | Cross-Sectional | BNT162b2 | 803 | 803 | From 18 to 90 years (Average 43 years) | 108 (13.45) | NA | NA | NA | NA | NA |
| Kadali et al., 2021a (cross) [30] | US | Cross-Sectional | mRNA-1273 | 432 | 432 | From 18 to 80 years (Average 43.76 years) | 45 (10.42) | 8 (1.85) | 55 (12.73) | NA | NA | NA |
| Kaur et al., 2021 [31] | India | Cohort study | ChAdOx1 | 804 | 804 | 38.44 (11.47) e | 573 (71.27) | NA | 73 (9) | 5 (0.6) | NA | NA |
| Kaur et al., 2021b f [32] | Global | Retrospective registry-based analysis | BNT162b2 | 4201 | 4863 | NA | NA | NA | NA | NA | NA | |
| ChAdOx1 | 262 | |||||||||||
| mRNA-1273 | 400 | |||||||||||
| Montano et al., 2022 [24] | Global | Retrospective registry-based analysis | ChAdOx1 | 34,643,783 | 452,016,608 | From 18 to 65 years and above | 266,008,304 (58.85) | NA | NA | NA | NA | NA |
| Ad26.COV2.S | 32,233,117 | |||||||||||
| mRNA-1273 | 105,518,547 | |||||||||||
| BNT162b2 | 279,620,827 | |||||||||||
| Patone et al., 2022 g [25] | England | Self-controlled case-series | ChAdOx1 (1st) | 20,615,911 | 1st dose at least = 38,615,491 | 55.2 (14.8) e | 7191428 (34.9) | NA | NA | NA | NA | NA |
| ChAdOx1 (2nd) | 19,754,224 | 55.4 (14.7) e | 6900964 (34.9) | |||||||||
| BNt162b2 (1st) | 16,993,389 | 47.8 (21.7) e | 5401842 (31.8) | |||||||||
| BNt162b2 (2nd) | 11,972,733 | Two doses = 32,095,748 | 55.5 (20.4) e | 3,906,666 (32.6) | ||||||||
| mRNA-1273 (1st) | 1,006,191 | 32.3 (9.4) e | 286,893 (28.5) | |||||||||
| mRNA-1273 (2nd) | 368,791 | 39.6 (7.3) e | 97,524 (26.4) | |||||||||
| Tan et al., 2021 g [33] | Singapore | Cohort | BNT162b2 (1st) | 37,367 | 1st dose at least = 64,661 | 27.33 (11.119) a | 33,913 (90.8) | NA | NA | NA | NA | NA |
| BNT162b2 (2nd) | 37,162 | 27 (11.119) a | 33,766 (90.9) | |||||||||
| mRNA-1273 (1st) | 27,294 | Two doses = 62,420 | 21 (2.9653) a | 25,661 (94.0) | ||||||||
| mRNA-1273 (2nd) | 25,258 | 21 (2.9653) a | 23,710 (93.9) | |||||||||
| Tobaiqy et al., 2021 [34] | Global | Retrospective registry-based analysis | mRNA-1273 | 336 | 3420 | From 18 to 85 years and above | 171 (50.9) | NA | NA | NA | NA | NA |
| BNT162b2 | 1096 | 494 (45.1) | ||||||||||
| ChAdOx1 | 1988 | 952 (47.9) | ||||||||||
| Truong et al., 2022 [35] | US and Canada | Retrospective study | BNT162b2 | 131 | 139 | 17.567 (18.728) e | 126 (90.6) | NA | NA | NA | NA | NA |
| mRNA-1273 | 5 | |||||||||||
| Ad26.COV2.S | 1 | |||||||||||
| Unknown | 2 | |||||||||||
| Witberg et al., 2022 [36] | Israel | Retrospective registry-based analysis | BNT162b2 | 2,558,421 | 2,558,421 | 45.667 (24.463) e | 1,248,433 (49) | NA | 7 (13) h | 1 (2) h | 1 (2) h | NA |
| Wong et al., 2022 [37] | China | Retrospective study | BNT162b2 (1st) | 1,308,820 | 1st dose at least = 2,264,679 | 45.7 (16.0) e | 584,158 (44.6) | 657 (0.05) i | 177,913 (13.6) | 253,883 (19.4) | NA | 1662 (0.1) |
| BNT162b2 (2nd) | 1,116,677 | 45.9 (15.7) e | 502,740 (45) | 513 (0.04) i | 148,978 (13.3) | 210,140 (18.8) | NA | 1347 (0.1) | ||||
| CoronaVac (1st) | 955,859 | Two doses = 1,938,237 | 55.3 (14.1) e | 439,928 (46) | 881 (0.09) i | 225,107 (23.6) | 343,413 (35.9) | NA | 2238 (0.2) | |||
| CoronaVac (2nd) | 821,560 | 54.8 (13.9) e | 383,164 (46.6) | 653 (0.07) i | 182,379 (22.2) | 274,353 (33.4) | NA | 1688 (0.2) | ||||
| Dizbay et al., 2021 [38] | Turkey | Retrospective study | CoronaVac | 1102 | 1102 | 37.667 (12.619) a | 352 (31.9) | 13 (1.2) | 48 (4.4) | NA | NA | NA |
| Vaccine | Studies | Pooled Incidence | Lower CI | Upper CI | IR | Heterogeneity (I2) | p-Value |
|---|---|---|---|---|---|---|---|
| Pfizer | 12 | 0.22% | 0.07% | 0.66% | 22 per 10,000 | 99.96% | <0.001 |
| Sinopharm | 2 | 0.03% | 0.00% | 18.48% | 3 per 10,000 | 99.96% | <0.001 |
| Moderna | 4 | 0.76% | 0.04% | 12.08% | 76 per 10,000 | 99.92% | <0.001 |
| CoronaVac | 2 | 0.01% | 0.00% | 0.03% | 1 per 10,000 | 99.59% | <0.001 |
| AstraZeneca | 3 | 0.04% | 0.00% | 0.98% | 4 per 10,000 | 99.78% | <0.001 |
| Subgroup Analysis | Studies | Pooled Incidence | Lower CI | Upper CI | Heterogeneity (I2) | p-Value | |
|---|---|---|---|---|---|---|---|
| Country | Asia | 3 | 0.006% | 0% | 0.009% | 92.8% | <0.001 |
| North America | 3 | 11.95% | 4.92% | 18.98% | 98.6% | <0.001 | |
| Middle East | 4 | 0.022% | 0.001% | 0.046% | 97% | <0.001 | |
| Europe | 1 | 0.136% | 0.134% | 0.137% | - | - | |
| Study Design | Cohort | 2 | 0.692% | 0% | 2.04% | 99.97% | <0.001 |
| Retrospective registry-based | 5 | 0.023% | 0% | 0.053% | 98.9% | <0.001 | |
| Cross-sectional | 2 | 5.25% | 3.42% | 7.07% | 66% | 0.086 | |
| Case-series | 2 | 0.071% | 0% | 0.198% | 100% | <0.001 | |
| Sample Size | >2000 | 6 | 0.238% | 0.183% | 0.294% | 99.99% | <0.001 |
| <2000 | 5 | 8.51% | 3.58% | 13.43% | 98.05% | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abutaleb, M.H.; Makeen, H.A.; Meraya, A.M.; Alqahtani, S.S.; Al-Mass, B.I.; Aljazaeri, R.O.; Alhazmi, B.D.; Kalakattawi, A.M.N.; Alajam, A.A. Risks of Cardiac Arrhythmia Associated with COVID-19 Vaccination: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 112. https://doi.org/10.3390/vaccines11010112
Abutaleb MH, Makeen HA, Meraya AM, Alqahtani SS, Al-Mass BI, Aljazaeri RO, Alhazmi BD, Kalakattawi AMN, Alajam AA. Risks of Cardiac Arrhythmia Associated with COVID-19 Vaccination: A Systematic Review and Meta-Analysis. Vaccines. 2023; 11(1):112. https://doi.org/10.3390/vaccines11010112
Chicago/Turabian StyleAbutaleb, Mohammed H., Hafiz A. Makeen, Abdulkarim M. Meraya, Saad S. Alqahtani, Bayan Ibrahim Al-Mass, Reaam Omar Aljazaeri, Bushra Dhuhayyan Alhazmi, Afnan Mohammed Noor Kalakattawi, and Ahmed Ali Alajam. 2023. "Risks of Cardiac Arrhythmia Associated with COVID-19 Vaccination: A Systematic Review and Meta-Analysis" Vaccines 11, no. 1: 112. https://doi.org/10.3390/vaccines11010112
APA StyleAbutaleb, M. H., Makeen, H. A., Meraya, A. M., Alqahtani, S. S., Al-Mass, B. I., Aljazaeri, R. O., Alhazmi, B. D., Kalakattawi, A. M. N., & Alajam, A. A. (2023). Risks of Cardiac Arrhythmia Associated with COVID-19 Vaccination: A Systematic Review and Meta-Analysis. Vaccines, 11(1), 112. https://doi.org/10.3390/vaccines11010112