
Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis

 ,
,  , ,
, ,  ,
,  , , , , , ,
, , , , , ,  , , ,
, , ,  and
and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search Strategy and Data Extraction
2.4. Assessment of the Methodological Quality
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Selection of Studies
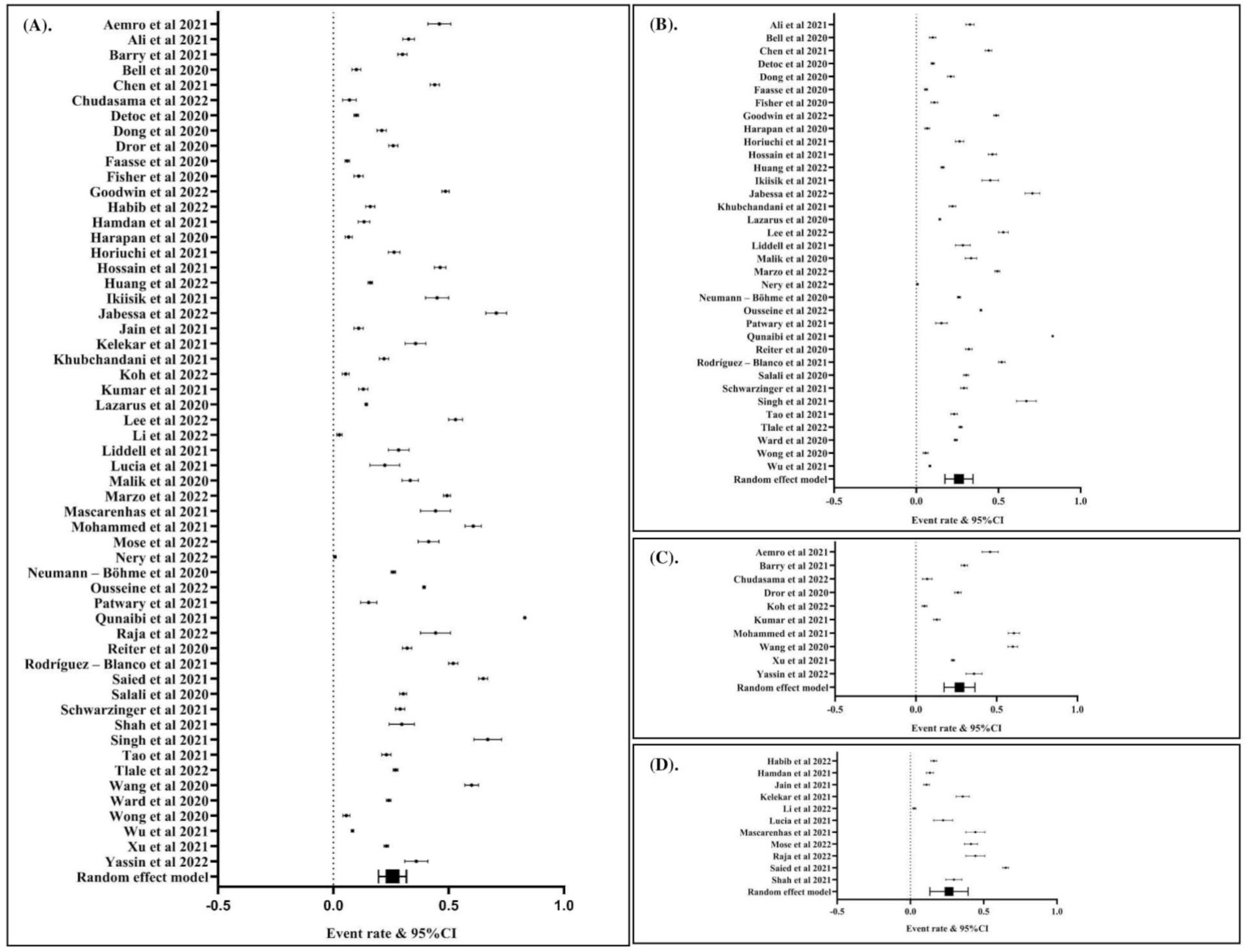
3.2. Global Prevalence of COVID-19 Vaccination Hesitancy
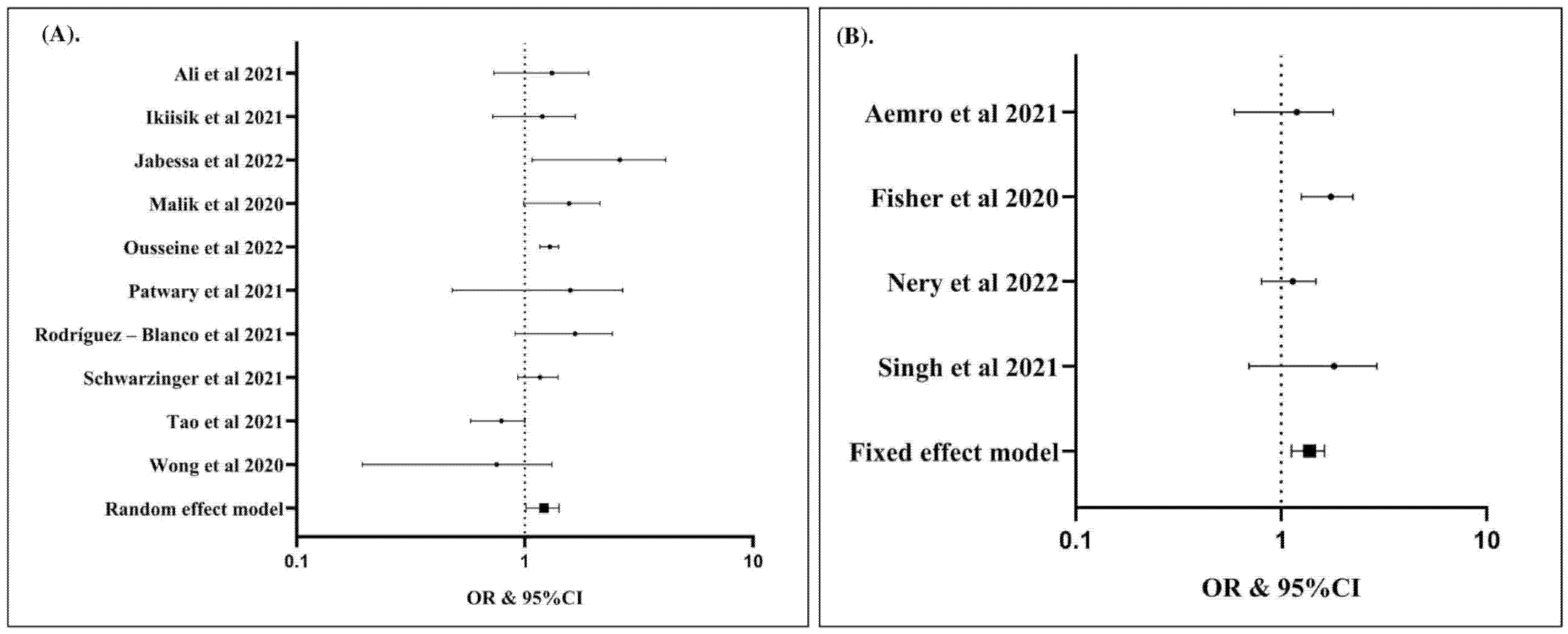
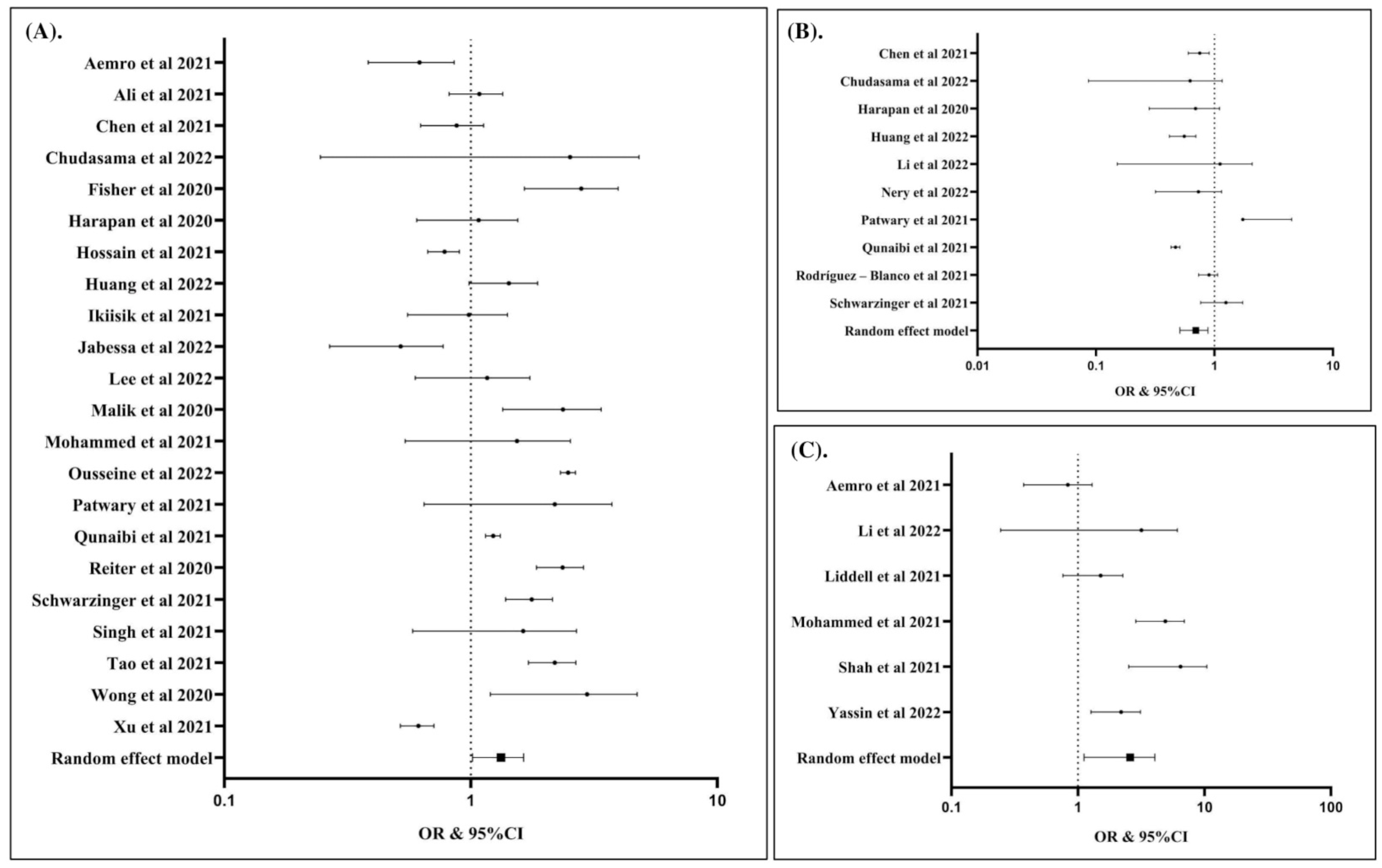
3.3. Potential Factors Associated with COVID-19 Vaccination Hesitancy
3.4. Source of Heterogeneity and Potential Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kashte, S.; Gulbake, A.; El-Amin, S.F., III; Gupta, A. COVID-19 vaccines: Rapid development, implications, challenges and future prospects. Hum. Cell 2021, 34, 711–733. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. Lond B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef]
- Salo, H.; Kilpi, T. National vaccination program—A success story of public health and economy. Duodecim 2017, 133, 977–983. [Google Scholar] [PubMed]
- Anderson, E.L. Recommended solutions to the barriers to immunization in children and adults. Mo. Med. 2014, 111, 344–348. [Google Scholar] [PubMed]
- Shen, S.C.; Dubey, V. Addressing vaccine hesitancy: Clinical guidance for primary care physicians working with parents. Can. Fam. Physician 2019, 65, 175–181. [Google Scholar]
- Pugliese-Garcia, M.; Heyerdahl, L.W.; Mwamba, C.; Nkwemu, S.; Chilengi, R.; Demolis, R.; Guillermet, E.; Sharma, A. Factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, Zambia. Vaccine 2018, 36, 5617–5624. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Aide, P.; Bassat, Q.; Alonso, P.L. Towards an effective malaria vaccine. Arch. Dis. Child. 2007, 92, 476–479. [Google Scholar] [CrossRef]
- Fatima, K.; Syed, N.I. Dengvaxia controversy: Impact on vaccine hesitancy. J. Glob. Health 2018, 8, 010312. [Google Scholar] [CrossRef] [PubMed]
- Mesch, G.S.; Schwirian, K.P. Vaccination hesitancy: Fear, trust, and exposure expectancy of an Ebola outbreak. Heliyon 2019, 5, e02016. [Google Scholar] [CrossRef] [PubMed]
- Voo, J.Y.H.; Lean, Q.Y.; Ming, L.C.; Md Hanafiah, N.H.; Al-Worafi, Y.M.; Ibrahim, B. Vaccine Knowledge, Awareness and Hesitancy: A Cross Sectional Survey among Parents Residing at Sandakan District, Sabah. Vaccines 2021, 9, 1348. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Beste, L.A.; Chen, A.; Geyer, J.; Wilson, M.; Schuttner, L.; Wheat, C.; Rojas, J.; Nelson, K.; Reddy, A. Best Practices for an Equitable Covid-19 Vaccination Program. NEJM Catal. Innov. Care Deliv. 2021, 2. [Google Scholar] [CrossRef]
- Norhayati, M.N.; Che Yusof, R.; Azman, Y.M. Systematic Review and Meta-Analysis of COVID-19 Vaccination Acceptance. Front. Med. 2022, 8, 783982. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18, 2407. [Google Scholar] [CrossRef]
- Rosiello, D.F.; Anwar, S.; Yufika, A.; Adam, R.Y.; Ismaeil, M.I.H.; Ismail, A.Y.; Dahman, N.B.H.; Hafsi, M.; Ferjani, M.; Sami, F.S.; et al. Acceptance of COVID-19 vaccination at different hypothetical efficacy and safety levels in ten countries in Asia, Africa, and South America. Narra J. 2021, 1, e55. [Google Scholar] [CrossRef]
- Sallam, M.; Anwar, S.; Yufika, A.; Fahriani, M.; Husnah, M.; Kusuma, H.I.; Raad, R.; Khiri, N.M.E.; Abdalla, R.Y.A.; Adam, R.Y.; et al. Willingness-to-pay for COVID-19 vaccine in ten low-middle-income countries in Asia, Africa and South America: A cross-sectional study. Narra J. 2022, 2, e74. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 Vaccine Acceptance among the Adult Population of Bangladesh Using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.A.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef]
- Montalti, M.; Di Valerio, Z.; Rallo, F.; Squillace, L.; Costantino, C.; Tomasello, F.; Mauro, G.L.; Stillo, M.; Perrone, P.; Resi, D.; et al. Attitudes toward the SARS-CoV-2 and Influenza Vaccination in the Metropolitan Cities of Bologna and Palermo, Italy. Vaccines 2021, 9, 1200. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Fajar, J.K. Supplementary files: Global prevalence and potential influencing factors of COVID-19 vaccination hesitancy: A meta-analysis. Figshare 2022, 1, 1. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Aemro, A.; Amare, N.S.; Shetie, B.; Chekol, B.; Wassie, M. Determinants of COVID-19 vaccine hesitancy among health care workers in Amhara region referral hospitals, Northwest Ethiopia: A cross-sectional study. Epidemiol. Infect. 2021, 149, e225. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Hossain, A. What is the extent of COVID-19 vaccine hesitancy in Bangladesh? A cross-sectional rapid national survey. BMJ Open 2021, 11, e050303. [Google Scholar] [CrossRef]
- Barry, M.; Temsah, M.H.; Alhuzaimi, A.; Alamro, N.; Al-Eyadhy, A.; Aljamaan, F.; Saddik, B.; Alhaboob, A.; Alsohime, F.; Alhasan, K.; et al. COVID-19 vaccine confidence and hesitancy among health care workers: A cross-sectional survey from a MERS-CoV experienced nation. PLoS ONE 2021, 16, e0244415. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef]
- Chudasama, R.V.; Khunti, K.; Ekezie, W.C.; Pareek, M.; Zaccardi, F.; Gillies, C.L.; Seidu, S.; Davies, M.J.; Chudasama, Y.V. COVID-19 vaccine uptake and hesitancy opinions from frontline health care and social care workers: Survey data from 37 countries. Diabetes Metab. Syndr. 2022, 16, 102361. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.T.; Feng, D.; Feng, Z.; Yeoh, E.K.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Faasse, K.; Newby, J. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Goodwin, R.; Ben-Ezra, M.; Takahashi, M.; Luu, L.N.; Borsfay, K.; Kovacs, M.; Hou, W.K.; Hamama-Raz, Y.; Levin, Y. Psychological factors underpinning vaccine willingness in Israel, Japan and Hungary. Sci. Rep. 2022, 12, 439. [Google Scholar] [CrossRef]
- Habib, S.S.; Alamri, M.S.; Alkhedr, M.M.; Alkhorijah, M.A.; Jabaan, R.D.; Alanzi, M.K. Knowledge and Attitudes of Medical Students toward COVID-19 Vaccine in Saudi Arabia. Vaccines 2022, 10, 541. [Google Scholar] [CrossRef]
- Hamdan, M.B.; Singh, S.; Polavarapu, M.; Jordan, T.R.; Melhem, N.M. COVID-19 vaccine hesitancy among university students in Lebanon. Epidemiol. Infect. 2021, 149, e242. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R.; et al. Factors of parental COVID-19 vaccine hesitancy: A cross sectional study in Japan. PLoS ONE 2021, 16, e0261121. [Google Scholar] [CrossRef]
- Hossain, M.B.; Alam, M.Z.; Islam, M.S.; Sultan, S.; Faysal, M.M.; Rima, S.; Hossain, M.A.; Mamun, A.A. COVID-19 vaccine hesitancy among the adult population in Bangladesh: A nationwide cross-sectional survey. PLoS ONE 2021, 16, e0260821. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Su, X.; Xiao, W.; Wang, H.; Si, M.; Wang, W.; Gu, X.; Ma, L.; Li, L.; Zhang, S.; et al. COVID-19 vaccine hesitancy among different population groups in China: A national multicenter online survey. BMC Infect. Dis. 2022, 22, 153. [Google Scholar] [CrossRef] [PubMed]
- Ikiisik, H.; Sezerol, M.A.; Tasci, Y.; Maral, I. COVID-19 vaccine hesitancy: A community-based research in Turkey. Int. J. Clin. Pract. 2021, 75, e14336. [Google Scholar] [CrossRef]
- Jabessa, D.; Bekele, F. Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study. Patient Prefer. Adherence 2022, 16, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, e132. [Google Scholar] [CrossRef]
- Kelekar, A.K.; Lucia, V.C.; Afonso, N.M.; Mascarenhas, A.K. COVID-19 vaccine acceptance and hesitancy among dental and medical students. J. Am. Dent. Assoc. 2021, 152, 596–603. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Koh, S.W.C.; Liow, Y.; Loh, V.W.K.; Liew, S.J.; Chan, Y.H.; Young, D. COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore. BMC Prim. Care 2022, 23, 81. [Google Scholar] [CrossRef]
- Kumar, R.; Alabdulla, M.; Elhassan, N.M.; Reagu, S.M. Qatar Healthcare Workers’ COVID-19 Vaccine Hesitancy and Attitudes: A National Cross-Sectional Survey. Front. Public Health 2021, 9, 727748. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Lee, M.; You, M. Direct and Indirect Associations of Media Use With COVID-19 Vaccine Hesitancy in South Korea: Cross-sectional Web-Based Survey. J. Med. Internet Res. 2022, 24, e32329. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Gao, Z.; Zhong, M.; Yu, Z.; Li, J.; Bi, H. Chinese University Students’ Awareness and Acceptance of the COVID-19 Vaccine: A Cross-Sectional Study. Risk Manag. Healthc. Policy 2022, 15, 845–864. [Google Scholar] [CrossRef] [PubMed]
- Liddell, B.J.; Murphy, S.; Mau, V.; Bryant, R.; O’Donnell, M.; McMahon, T.; Nickerson, A. Factors associated with COVID-19 vaccine hesitancy amongst refugees in Australia. Eur. J. Psychotraumatol. 2021, 12, 1997173. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Marzo, R.R.; Sami, W.; Alam, M.Z.; Acharya, S.; Jermsittiparsert, K.; Songwathana, K.; Pham, N.T.; Respati, T.; Faller, E.M.; Baldonado, A.M.; et al. Hesitancy in COVID-19 vaccine uptake and its associated factors among the general adult population: A cross-sectional study in six Southeast Asian countries. Trop. Med. Health 2022, 50, 4. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, A.K.; Lucia, V.C.; Kelekar, A.; Afonso, N.M. Dental students’ attitudes and hesitancy toward COVID-19 vaccine. J. Dent. Educ. 2021, 85, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef]
- Mose, A.; Haile, K.; Timerga, A. COVID-19 vaccine hesitancy among medical and health science students attending Wolkite University in Ethiopia. PLoS ONE 2022, 17, e0263081. [Google Scholar] [CrossRef]
- Nery, N., Jr.; Ticona, J.P.A.; Cardoso, C.W.; Prates, A.; Vieira, H.C.A.; de Almeida, A.S.; Souza, M.; dos Reis, O.B.; Pellizzaro, M.; Portilho, M.M.; et al. COVID-19 vaccine hesitancy and associated factors according to sex: A population-based survey in Salvador, Brazil. PLoS ONE 2022, 17, e0262649. [Google Scholar] [CrossRef]
- Neumann-Bohme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyogg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Ousseine, Y.M.; Vaux, S.; Vandentorren, S.; Bonmarin, I.; Champenois, K.; Lydie, N.; Velter, A. Predictors of Uncertainty and Unwillingness to Receive the COVID-19 Vaccine in Men Who Have Sex with Men in France. Int. J. Environ. Res. Public Health 2022, 19, 5372. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. Elife 2021, 10, e68038. [Google Scholar] [CrossRef]
- Raja, S.M.; Osman, M.E.; Musa, A.O.; Hussien, A.A.; Yusuf, K. COVID-19 vaccine acceptance, hesitancy, and associated factors among medical students in Sudan. PLoS ONE 2022, 17, e0266670. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, N.; Montero-Navarro, S.; Botella-Rico, J.M.; Felipe-Gomez, A.J.; Sanchez-Mas, J.; Tuells, J. Willingness to Be Vaccinated against COVID-19 in Spain before the Start of Vaccination: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5272. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1, 1–3. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Shah, A.K.; Daniel, R.A.; Kusuma, Y.S. Knowledge and Willingness to Accept Vaccine Against SARS-CoV-2 Among Undergraduate Medical Students in Delhi, India. Curr. Health Sci. J. 2021, 47, 479–484. [Google Scholar] [CrossRef]
- Singh, A.; Lai, A.H.Y.; Wang, J.; Asim, S.; Chan, P.S.; Wang, Z.; Yeoh, E.K. Multilevel Determinants of COVID-19 Vaccine Uptake Among South Asian Ethnic Minorities in Hong Kong: Cross-sectional Web-Based Survey. JMIR Public Health Surveill. 2021, 7, e31707. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: A multi-center cross-sectional study based on health belief model. Hum. Vaccin Immunother. 2021, 17, 2378–2388. [Google Scholar] [CrossRef] [PubMed]
- Tlale, L.B.; Gabaitiri, L.; Totolo, L.K.; Smith, G.; Puswane-Katse, O.; Ramonna, E.; Mothowaeng, B.; Tlhakanelo, J.; Masupe, T.; Rankgoane-Pono, G.; et al. Acceptance rate and risk perception towards the COVID-19 vaccine in Botswana. PLoS ONE 2022, 17, e0263375. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.K.; Alleaume, C.; Peretti-Watel, P.; Group, C. The French public’s attitudes to a future COVID-19 vaccine: The politicization of a public health issue. Soc. Sci. Med. 2020, 265, 113414. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Wu, J.; Li, Q.; Silver Tarimo, C.; Wang, M.; Gu, J.; Wei, W.; Ma, M.; Zhao, L.; Mu, Z.; Miao, Y. COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study. Front. Immunol. 2021, 12, 781161. [Google Scholar] [CrossRef]
- Xu, B.; Zhang, Y.; Chen, L.; Yu, L.; Li, L.; Wang, Q. The influence of social network on COVID-19 vaccine hesitancy among healthcare workers: A cross-sectional survey in Chongqing, China. Hum. Vaccine Immunother. 2021, 17, 5048–5062. [Google Scholar] [CrossRef]
- Yassin, E.O.M.; Faroug, H.A.A.; Ishaq, Z.B.Y.; Mustafa, M.M.A.; Idris, M.M.A.; Widatallah, S.E.K.; Abd El-Raheem, G.O.H.; Suliman, M.Y. COVID-19 Vaccination Acceptance among Healthcare Staff in Sudan, 2021. J. Immunol. Res. 2022, 2022, 3392667. [Google Scholar] [CrossRef]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 Vaccine Acceptance among Low- and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Ulbrichtova, R.; Svihrova, V.; Svihra, J. Prevalence of COVID-19 Vaccination among Medical Students: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4072. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Roy, D.N.; Biswas, M.; Islam, E.; Azam, M.S. Potential factors influencing COVID-19 vaccine acceptance and hesitancy: A systematic review. PLoS ONE 2022, 17, e0265496. [Google Scholar] [CrossRef]
- Yazdani, A.; Mirmosayyeb, O.; Ghaffary, E.M.; Hashemi, M.S.; Ghajarzadeh, M. COVID-19 vaccines and patients with multiple sclerosis: Willingness, unwillingness and hesitancy: A systematic review and meta-analysis. Neurol. Sci. 2022, 43, 4085–4094. [Google Scholar] [CrossRef]
- Veronese, N.; Saccaro, C.; Demurtas, J.; Smith, L.; Dominguez, L.J.; Maggi, S.; Barbagallo, M. Prevalence of unwillingness and uncertainty to vaccinate against COVID-19 in older people: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 72, 101489. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Haque, M.Z.; Sultana, R.; Alam, M.A.; Browning, M. COVID-19 Vaccine Acceptance Rate and Its Factors among Healthcare Students: A Systematic Review with Meta-Analysis. Vaccines 2022, 10, 806. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. First COVID-19 Booster Dose in the General Population: A Systematic Review and Meta-Analysis of Willingness and Its Predictors. Vaccines 2022, 10, 1097. [Google Scholar] [CrossRef]
- Hussain, B.; Latif, A.; Timmons, S.; Nkhoma, K.; Nellums, L.B. Overcoming COVID-19 vaccine hesitancy among ethnic minorities: A systematic review of UK studies. Vaccine 2022, 40, 3413–3432. [Google Scholar] [CrossRef]
- Mudatsir, M.; Fajar, J.K.; Wulandari, L.; Soegiarto, G.; Ilmawan, M.; Purnamasari, Y.; Mahdi, B.A.; Jayanto, G.D.; Suhendra, S.; Setianingsih, Y.A.; et al. Predictors of COVID-19 severity: A systematic review and meta-analysis. F1000Research 2020, 9, 1107. [Google Scholar] [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef]
- Rattay, P.; von der Lippe, E. Association between Living with Children and the Health and Health Behavior of Women and Men. Are There Differences by Age? Results of the “German Health Update” (GEDA) Study. Int. J. Environ. Res. Public Health 2020, 17, 3180. [Google Scholar] [CrossRef] [PubMed]
- García, L.M.R.; Navarrro, J.M.R. The Impact of Quality of Life on the Health of Older People from a Multidimensional Perspective. J. Aging Res. 2018, 2018, 4086294. [Google Scholar] [CrossRef]
- Robards, J.; Evandrou, M.; Falkingham, J.; Vlachantoni, A. Marital status, health and mortality. Maturitas 2012, 73, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.A.; Solehan, H.M.; Rani, M.D.M.; Ithnin, M.; Che Isahak, C.I. Knowledge, acceptance and perception on COVID-19 vaccine among Malaysians: A web-based survey. PLoS ONE 2021, 16, e0256110. [Google Scholar] [CrossRef]
- Bari, M.S.; Hossain, M.J.; Ahmmed, F.; Sarker, M.M.R.; Khandokar, L.; Chaithy, A.P.; Aziz, F.; Mitra, S.; Emran, T.B.; Islam, M.S.; et al. Knowledge, Perception, and Willingness towards Immunization among Bangladeshi Population during COVID-19 Vaccine Rolling Period. Vaccines 2021, 9, 1449. [Google Scholar] [CrossRef]
- Theodorea, C.F.; Widyarman, A.S.; Dewanto, I.; Astoeti, T.E. COVID-19 Vaccines in Indonesia: Knowledge, Attitudes, and Acceptance Among Dental Professionals. Front. Med. 2021, 8, 784002. [Google Scholar] [CrossRef]
- Harapan, H.; Fajar, J.K.; Sasmono, R.T.; Kuch, U. Dengue vaccine acceptance and willingness to pay. Hum. Vaccines Immunother. 2017, 13, 786–790. [Google Scholar] [CrossRef][Green Version]
- Harapan, H.; Anwar, S.; Bustaman, A.; Radiansyah, A.; Angraini, P.; Fasli, R.; Salwiyadi, S.; Bastian, R.A.; Oktiviyari, A.; Akmal, I.; et al. Community Willingness to Participate in a Dengue Study in Aceh Province, Indonesia. PLoS ONE 2016, 11, e0159139. [Google Scholar] [CrossRef]
- Mudatsir, M.; Anwar, S.; Fajar, J.K.; Yufika, A.; Ferdian, M.N.; Salwiyadi, S.; Imanda, A.S.; Azhars, R.; Ilham, D.; Timur, A.U.; et al. Willingness-to-pay for a hypothetical Ebola vaccine in Indonesia: A cross-sectional study in Aceh. F1000Research 2019, 8, 1441. [Google Scholar] [CrossRef]
- Fajar, J.K.; Harapan, H. Socioeconomic and attitudinal variables associated with acceptance and willingness to pay towards dengue vaccine: A systematic review. Arch. Clin. Infect. Dis. 2017, 12, e13914. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Setiawan, A.M.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; et al. Acceptance and willingness to pay for a hypothetical vaccine against monkeypox viral infection among frontline physicians: A cross-sectional study in Indonesia. Vaccine 2020, 38, 6800–6806. [Google Scholar] [CrossRef]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu Rev. Sociol 2010, 36, 349–370. [Google Scholar] [CrossRef]
- Ratzan, S.C. “Vaccine Communication in a Pandemic: Improving Vaccine Literacy to Reduce Hesitancy, Restore Trust and Immunize Communities”: Editor’s Introduction. J. Health Commun. 2020, 25, 745–746. [Google Scholar] [CrossRef]
- Gendler, Y.; Ofri, L. Investigating the Influence of Vaccine Literacy, Vaccine Perception and Vaccine Hesitancy on Israeli Parents’ Acceptance of the COVID-19 Vaccine for Their Children: A Cross-Sectional Study. Vaccines 2021, 9, 1391. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Country | Sample Size | Study Period | Population | Funding | NOS 1 |
|---|---|---|---|---|---|---|
| Aemro et al., 2021 [25] | Ethiopia | 418 | May–June 2021 | Healthcare workers | No funding | 5 |
| Ali et al., 2021 [26] | Bangladesh | 1134 | January 2021 | General population | No funding | 6 |
| Barry et al., 2021 [27] | Saudi Arabia | 1512 | November 2020 | Healthcare workers | No funding | 6 |
| Bell et al., 2020 [28] | England | 1252 | April–May 2020 | General population | London School of Hygiene and Tropical Medicine | 6 |
| Chen et al., 2021 [29] | China | 2531 | January 2021 | General population | NA | 7 |
| Chudasama et al., 2022 [30] | Multinational | 275 | April–July 2021 | Healthcare workers | NA | 6 |
| Detoc et al., 2020 [31] | France | 3259 | March–April 2020 | General population | NA | 5 |
| Dong et al., 2020 [32] | China | 1236 | June–July 2020 | General population | Chinese University of Hong Kong | 6 |
| Dror et al., 2020 [33] | Israel | 1661 | 2020–2022 | Healthcare workers | NA | 5 |
| Faasse et al., 2020 [34] | Australia | 2232 | March 2020 | General population | UNSW Science Goldstar (2020) | 5 |
| Fisher et al., 2020 [35] | US | 991 | April 2020 | General population | Agency for Healthcare Research and Quality | 7 |
| Goodwin et al., 2022 [36] | Multinational | 3059 | December 2020–January 2021 | General population | Ariel University, JSPS KAKENSHI, Hungaria National Excellence Program | 6 |
| Habib et al., 2022 [37] | Saudi Arabia | 1445 | August–October 2021 | Students | King Saud University | 7 |
| Bou Hamdan et al., 2021 [38] | Lebanon | 758 | May–June 2021 | Students | No funding | 7 |
| Harapan et al., 2020 [39] | Indonesia | 1359 | March–April 2020 | General population | No funding | 6 |
| Horiuchi et al., 2021 [40] | Japan | 1200 | May–June 2021 | General population | No funding | 7 |
| Hossain et al., 2021 [41] | Bangladesh | 1497 | February 2021 | General population | No funding | 6 |
| Huang et al., 2022 [42] | China | 4227 | January–March 2021 | General population | National Health Commission of the People’s Republic of China | 7 |
| Ikiisik et al., 2021 [43] | Turkey | 384 | December 2020 | General population | NA | 7 |
| Jabessa et al., 2022 [44] | Ethiopia | 350 | August–September 2021 | General population | No funding | 6 |
| Jain et al., 2021 [45] | India | 1068 | February–March 2021 | Students | No funding | 6 |
| Kelekar et al., 2021 [46] | US | 408 | September–December 2020 | Students | NA | 6 |
| Khubchandani et al., 2021 [47] | US | 1878 | June 2020 | General population | No funding | 8 |
| Koh et al., 2022 [48] | Singapore | 528 | May–June 2021 | Healthcare workers | No funding | 6 |
| Kumar et al., 2021 [49] | Qatar | 1414 | October–November 2020 | Healthcare workers | Qatar National Library | 5 |
| Lazarus et al., 2020 [50] | Multinational | 13,426 | June 2020 | General population | City University of New York | 6 |
| Lee et al., 2022 [51] | South Korea | 1016 | January 2021 | General population | No funding | 6 |
| Li et al., 2022 [52] | China | 721 | June 2021 | Students | Xuzhou Medical University | 7 |
| Liddell et al., 2021 [53] | Australia | 437 | June 2021 | General population | UNSW Sydney/Australian Red Cross | 6 |
| Lucia et al., 2021 [54] | US | 167 | NA | Students | No funding | 5 |
| Malik et al., 2020 [55] | US | 672 | May 2020 | General population | Yale Institute for Global Health | 8 |
| Marzo et al., 2022 [56] | Multinational | 5260 | February–May 2021 | General population | No funding | 7 |
| Mascarenhas et al., 2021 [57] | US | 245 | 2020 | Students | No funding | 6 |
| Mohammed et al., 2021 [58] | Ethiopia | 614 | March–July 2021 | Healthcare workers | No funding | 7 |
| Mose et al., 2022 [59] | Ethiopia | 420 | March 2021 | Students | No funding | 6 |
| Nery et al., 2022 [60] | Brazil | 2537 | November 2020–January 2021 | General population | Brazilian Ministry of Health | 8 |
| Neumann-Böhme et al., 2020 [61] | Multinational | 7664 | April 2020 | General population | European Union’s Horizon 2020 research and innovation programme | 6 |
| Ousseine et al., 2022 [62] | France | 15,427 | February–April 2021 | General population | National Agency for Research on AIDS and Viral Hepatitis (ANRS) | 6 |
| Patwary et al., 2021 [19] | Bangladesh | 543 | July–August 2021 | General population | No funding | 6 |
| Qunaibi et al., 2021 [63] | Multinational | 36,220 | January 2021 | General population | No funding | 7 |
| Raja et al., 2022 [64] | Sudan | 217 | June–July 2021 | Students | No funding | 5 |
| Reiter et al., 2020 [65] | US | 2006 | May 2020 | General population | National Center for Advancing Translational Sciences | 7 |
| Rodríguez-Blanco et al., 2021 [66] | Spain | 2494 | November–December 2020 | General population | No funding | 6 |
| Saied et al., 2021 [67] | Egypt | 2133 | January 2021 | Students | NA | 7 |
| Salali et al., 2020 [68] | Multinational | 5024 | May 2020 | General population | No funding | 6 |
| Schwarzinger et al., 2021 [69] | France | 1942 | July 2020 | General population | French Public Health Agency | 7 |
| Shah et al., 2021 [70] | India | 274 | February 2021 | Students | NA | 7 |
| Singh et al., 2021 [71] | Hong Kong | 245 | May 2021 | General population | Tung Foundation | 7 |
| Tao et al., 2021 [72] | China | 1392 | November 2020 | General population | National Key Research and Development Project of China | 7 |
| Tlale et al., 2022 [73] | Botswana | 4952 | February 2021 | General population | No funding | 6 |
| Wang et al., 2020 [74] | Hong Kong | 806 | February–March 2020 | Healthcare workers | No funding | 6 |
| Ward et al., 2020 [75] | France | 5018 | April 2020 | General population | Agence Nationale de la Recheche and the CNRS | 8 |
| Wong et al., 2020 [76] | Malaysia | 1159 | April 2020 | General population | Ministry of Education Malaysia | 8 |
| Wu et al., 2021 [77] | China | 29,925 | August 2021 | General population | National Social Science Fund of China | 7 |
| Xu et al., 2021 [78] | China | 5247 | January 2021 | Healthcare workers | Health Commission of Chongqing municipal, China | 6 |
| Yassin et al., 2022 [79] | Sudan | 365 | April 2021 | Healthcare workers | NA | 6 |
| Covariates | Hesitancy/Total (n [%]) | NS | p Egger | p Het | OR | 95% CI | p |
|---|---|---|---|---|---|---|---|
| Age group (years) | |||||||
| ≤30 | 6568/14,356 [45.8] | 16 | 0.2320 | <0.0001 | 1.14 | 0.98–1.32 | 0.0870 |
| 31–40 | 5097/11,335 [45.0] | 16 | 0.2360 | <0.0001 | 1.09 | 0.94–1.26 | 0.2630 |
| 41–50 | 3034/6536 [46.4] | 15 | 0.2730 | <0.0001 | 0.88 | 0.74–1.06 | 0.1760 |
| >50 | 2034/4677 [43.5] | 13 | 0.2980 | <0.0001 | 0.79 | 0.64–0.98 | 0.0290 |
| Sex | |||||||
| Male | 8934/22,362 [40.0] | 31 | 0.2840 | <0.0001 | 0.76 | 0.67–0.85 | <0.0001 |
| Female | 11,170/28,707 [38.9] | 31 | 0.2840 | <0.0001 | 1.32 | 1.17–1.49 | <0.0001 |
| Marital status | |||||||
| Married | 6888/20,496 [33.6] | 17 | 0.1950 | <0.0001 | 0.84 | 0.75–0.95 | 0.0040 |
| Single | 7173/18,764 [38.2] | 17 | 0.1950 | <0.0001 | 1.19 | 1.06–1.34 | 0.0040 |
| Educational attainment | |||||||
| <BSC | 12,130/22,950 [52.9] | 22 | 0.5260 | <0.0001 | 1.30 | 1.03–1.65 | 0.0300 |
| ≥BSC | 17,532/41,182 [42.6] | 22 | 0.5260 | <0.0001 | 0.77 | 0.61–0.97 | 0.0300 |
| Religion | |||||||
| Christian | 1053/2124 [49.6] | 5 | <0.0001 | 0.4380 | 1.17 | 1.01–1.35 | 0.0340 |
| Muslim | 1265/3961 [31.9] | 6 | 0.5110 | <0.0001 | 1.39 | 0.85–2.26 | 0.1860 |
| Hindu | 16/129 [12.4] | 2 | 1.5700 | 0.0710 | 0.28 | 0.02–3.40 | 0.3150 |
| Employment | |||||||
| Not working | 1704/4455 [38.2] | 10 | 0.1790 | 0.0090 | 1.20 | 1.02–1.42 | 0.0300 |
| Working | 5883/16,413 [35.8] | 10 | 0.1790 | 0.0090 | 0.83 | 0.71–0.98 | 0.0300 |
| Healthcare-related job | 2886/8313 [34.7] | 10 | 0.3340 | <0.0001 | 0.68 | 0.52–0.89 | 0.0040 |
| Socioeconomic status | |||||||
| Low income | 1320/2939 [44.9] | 7 | 0.4840 | <0.0001 | 1.31 | 0.88–1.94 | 0.1790 |
| Middle income | 1217/3220 [37.8] | 7 | 1.2050 | <0.0001 | 0.61 | 0.25–1.52 | 0.2900 |
| High income | 1427/2515 [56.7] | 7 | 1.2860 | <0.0001 | 1.28 | 0.49–3.38 | 0.6140 |
| Urbanicity | |||||||
| Urban | 9192/28,583 [32.2] | 15 | 0.4500 | <0.0001 | 0.92 | 0.72–1.18 | 0.5070 |
| Rural | 3128/8338 [37.5] | 15 | 0.4500 | <0.0001 | 1.09 | 0.85–1.39 | 0.5070 |
| Children at home | 1207/4595 [26.3] | 8 | 1.4040 | <0.0001 | 0.37 | 0.14–0.99 | 0.0490 |
| Aged people at home | 456/1542 [29.6] | 5 | 0.2760 | 0.0140 | 1.07 | 0.78–1.45 | 0.6920 |
| Household number (n) | |||||||
| ≤2 | 930/3192 [29.1] | 5 | 0.3900 | <0.0001 | 0.94 | 0.64–1.36 | 0.7270 |
| 3–4 | 564/2067 [27.3] | 5 | 0.2290 | 0.0110 | 0.89 | 0.69–1.14 | 0.3510 |
| ≥5 | 278/712 [39.0] | 4 | 0.1680 | 0.1620 | 1.36 | 1.13–1.63 | 0.0010 |
| Family members with medical backgrounds | 464/1382 [33.6] | 2 | 0.0410 | 0.3170 | 0.92 | 0.78–1.07 | 0.2770 |
| Wearing masks all the time | 1523/6606 [23.1] | 6 | 0.5570 | <0.0001 | 0.61 | 0.36–1.05 | 0.0720 |
| Constantly washing hands | 1209/4974 [24.3] | 4 | 0.8900 | <0.0001 | 0.45 | 0.18–1.16 | 0.0980 |
| Keep physical distancing | 213/745 [28.6] | 3 | 0.8370 | 0.0010 | 0.23 | 0.08–0.65 | 0.0050 |
| Smoker | 665/2236 [29.7] | 5 | 0.0590 | 0.3360 | 1.13 | 0.99–1.29 | 0.0610 |
| History of chronic disease(s) | 3828/8197 [46.7] | 17 | 0.1840 | <0.0001 | 0.91 | 0.80–1.03 | 0.1420 |
| Ever tested for COVID-19 | 670/4430 [15.1] | 6 | 0.4340 | <0.0001 | 0.46 | 0.31–0.68 | <0.0001 |
| Personal history of COVID-19 diagnosis | 4114/7733 [53.2] | 15 | 0.6090 | <0.0001 | 0.94 | 0.66–1.33 | 0.7150 |
| Family member/friend ever diagnosed with COVID-19 | 1192/3759 [31.7] | 7 | 0.2960 | <0.0001 | 0.83 | 0.63–1.09 | 0.1730 |
| Hospitalization due to COVID-19 among people in the same social circle | 69/621 [11.1] | 2 | <0.0001 | 0.9770 | 0.57 | 0.37–0.88 | 0.0110 |
| Death due to COVID-19 among people in the same social circle | 63/537 [11.7] | 3 | <0.0001 | 0.9450 | 0.73 | 0.49–1.08 | 0.1160 |
| COVID-19 vaccines are not safe | 628/1595 [39.4] | 6 | 0.7000 | <0.0001 | 2.24 | 1.21–4.14 | 0.0100 |
| Influenza vaccination in the past few years | 3481/10,687 [32.6] | 11 | 0.3460 | <0.0001 | 0.46 | 0.36–0.58 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fajar, J.K.; Sallam, M.; Soegiarto, G.; Sugiri, Y.J.; Anshory, M.; Wulandari, L.; Kosasih, S.A.P.; Ilmawan, M.; Kusnaeni, K.; Fikri, M.; et al. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines 2022, 10, 1356. https://doi.org/10.3390/vaccines10081356
Fajar JK, Sallam M, Soegiarto G, Sugiri YJ, Anshory M, Wulandari L, Kosasih SAP, Ilmawan M, Kusnaeni K, Fikri M, et al. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines. 2022; 10(8):1356. https://doi.org/10.3390/vaccines10081356
Chicago/Turabian StyleFajar, Jonny Karunia, Malik Sallam, Gatot Soegiarto, Yani Jane Sugiri, Muhammad Anshory, Laksmi Wulandari, Stephanie Astrid Puspitasari Kosasih, Muhammad Ilmawan, Kusnaeni Kusnaeni, Muhammad Fikri, and et al. 2022. "Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis" Vaccines 10, no. 8: 1356. https://doi.org/10.3390/vaccines10081356
APA StyleFajar, J. K., Sallam, M., Soegiarto, G., Sugiri, Y. J., Anshory, M., Wulandari, L., Kosasih, S. A. P., Ilmawan, M., Kusnaeni, K., Fikri, M., Putri, F., Hamdi, B., Pranatasari, I. D., Aina, L., Maghfiroh, L., Ikhriandanti, F. S., Endiaverni, W. O., Nugraha, K. W., Wiranudirja, O., ... Harapan, H. (2022). Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines, 10(8), 1356. https://doi.org/10.3390/vaccines10081356