
Validation of a Novel Fluorescent Lateral Flow Assay for Rapid Qualitative and Quantitative Assessment of Total Anti-SARS-CoV-2 S-RBD Binding Antibody Units (BAU) from Plasma or Fingerstick Whole-Blood of COVID-19 Vaccinees

 , ,
, ,  , , , , ,
, , , , ,  ,
,  and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Samples Collection and Ethical Approval
2.2. FinecareTM Anti-SARS-CoV-2 S-RBD Total Abs Test
2.2.1. Fingerstick Samples
2.2.2. Plasma Samples
2.3. Commercially Available Serological Assays
2.4. cPass GenScript sVNT
2.5. Statistical Method
3. Results
3.1. FinecareTM Is a Very Specific and Sensitive Assay
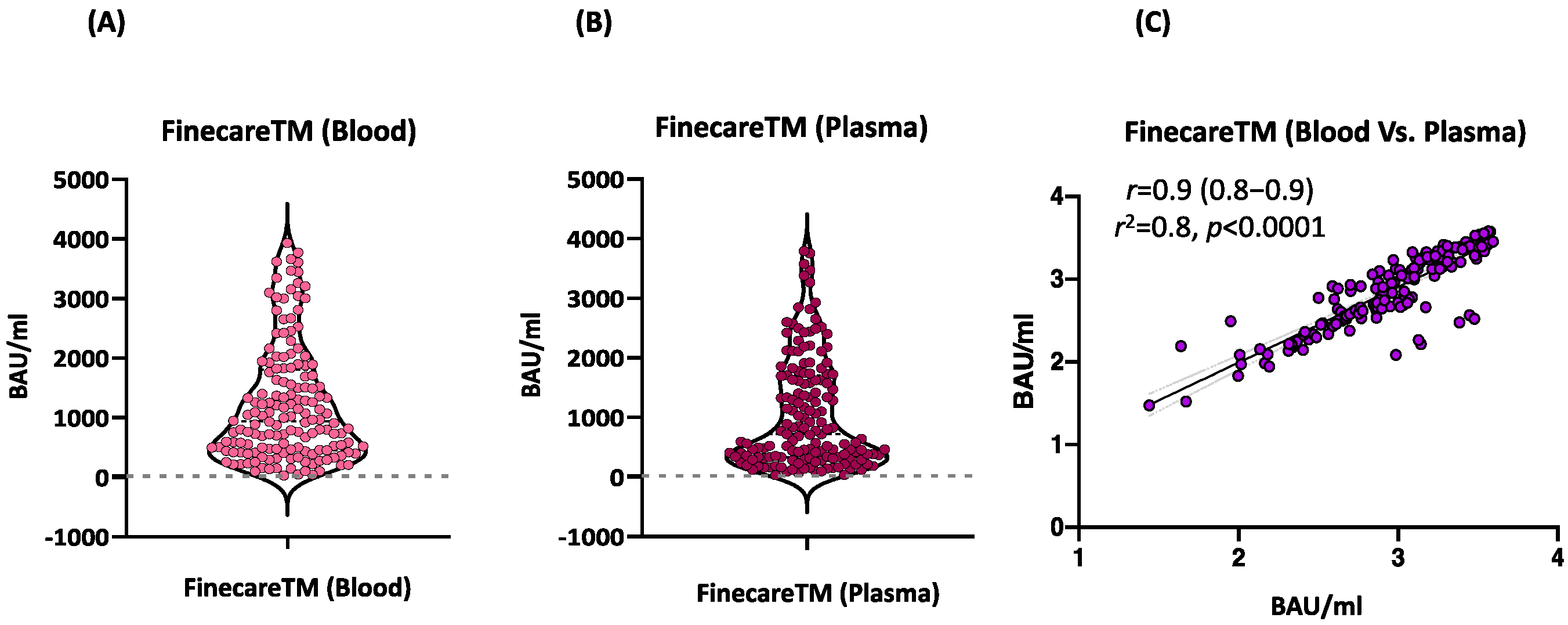
3.2. FinecareTM Fingerstick and Plasma Results Are Comparable
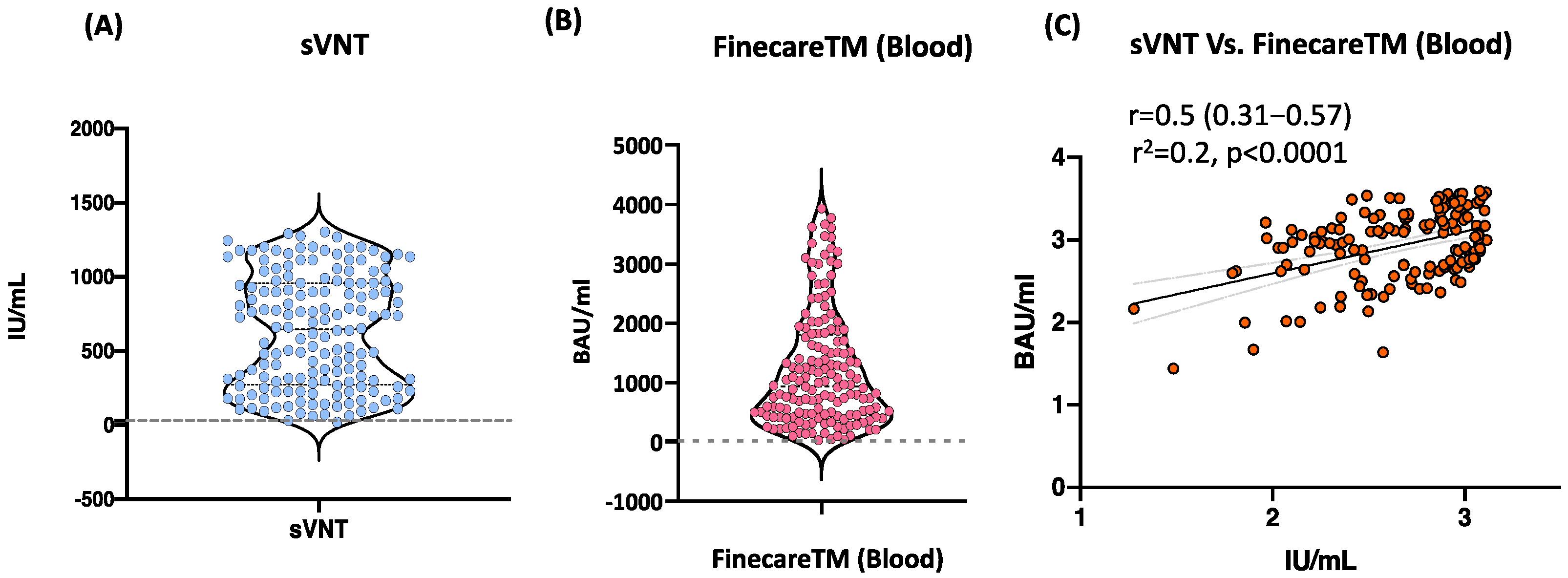
3.3. Moderate Correlation between FinecareTM and sVNT Using Fingerstick Whole Blood Samples
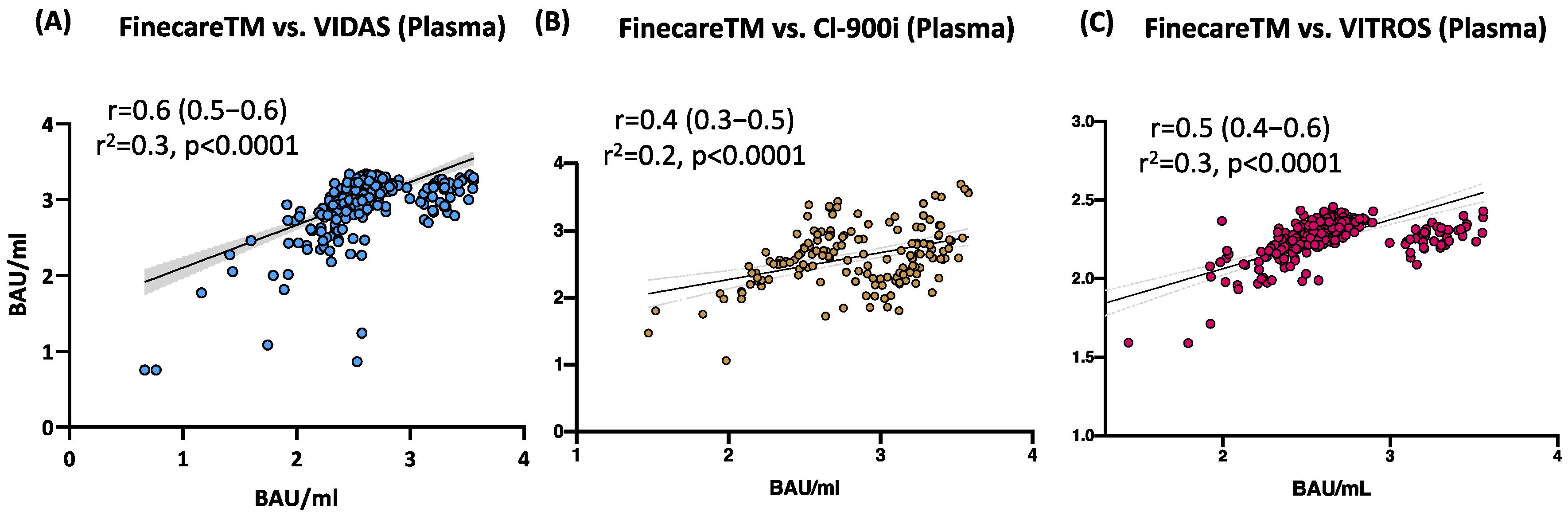
3.4. Moderate to Strong Correlation between FinecareTM and Three Commercially Available Automated Anti-SARS-CoV-2 Immunoassays Using Plasma Samples
3.5. Excellent Agreement between FinecareTM and the Three Automated Anti-SARS-CoV-2 Immunoassays
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bond, K.; Nicholson, S.; Lim, S.M.; Karapanagiotidis, T.; Williams, E.; Johnson, D.; Hoang, T.; Sia, C.; Purcell, D.; Mordant, F.; et al. Evaluation of Serological Tests for SARS-CoV-2: Implications for Serology Testing in a Low-Prevalence Setting. J. Infect. Dis. 2020, 222, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 1862. [Google Scholar] [CrossRef] [PubMed]
- McAndrews, K.M.; Dowlatshahi, D.P.; Dai, J.; Becker, L.M.; Hensel, J.; Snowden, L.M.; Leveille, J.M.; Brunner, M.R.; Holden, K.W.; Hopkins, N.S.; et al. Heterogeneous antibodies against SARS-CoV-2 spike receptor binding domain and nucleocapsid with implications for COVID-19 immunity. JCI Insight 2020, 5, 272. [Google Scholar] [CrossRef]
- Dispinseri, S.; Secchi, M.; Pirillo, M.F.; Tolazzi, M.; Borghi, M.; Brigatti, C.; De Agelis, M.L. Neutralizing antibody responses to SARS-CoV-2 in symptomatic COVID-19 is persistent and critical for survival. Nat. Commun. 2021, 12, 2670. [Google Scholar] [CrossRef]
- Premkumar, L.; Segovia-Chumbez, B.; Jadi, R.; Martinez, D.R.; Raut, R.; Markmann, A.; Pieri, M.; Grelli, S. The receptor binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. Sci. Immunol. 2020, 5, 2992. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Chia, W.N.; Qin, X. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Traugott, M.; Aberle, S.W.; Aberle, J.H.; Griebler, H.; Karolyi, M.; Pawelka, E.; Puchhammer-Stöckl, E.; Zoufaly, A.; Weseslindtner, L. Performance of Severe Acute Respiratory Syndrome Coronavirus 2 Antibody Assays in Different Stages of Infection: Comparison of Commercial Enzyme-Linked Immunosorbent Assays and Rapid Tests. J. Infect. Dis. 2020, 222, 362–366. [Google Scholar] [CrossRef]
- Okba, N.M.A.; Müller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Lamers, M.M.; Sikkema, R.S.; De Bruin, E.; Chandler, F.D. Severe Acute Respiratory Syndrome Coronavirus 2-Specific Antibody Responses in Coronavirus Disease Patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Khoury, D.S.; Wheatley, A.K.; Ramuta, M.D.; Reynaldi, A.; Cromer, D.; Subbarao, K.; O’Connor, D.H.; Kent, S.J.; Davenport, M.P. Measuring immunity to SARS-CoV-2 infection: Comparing assays and animal models. Nat. Rev. Immunol. 2020, 20, 727–738. [Google Scholar] [CrossRef]
- Zhu, F.; Althaus, T.; Tan, C.W.; Costantini, A.; Chia, W.N.; Van Vinh Chau, N.; Pieri, M.; Grelli, S. WHO international standard for SARS-CoV-2 antibodies to determine markers of protection. Lancet Microbe 2020, 29, 2881. [Google Scholar] [CrossRef]
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for evaluation of the antibody response to COVID-19 vaccines: Call for urgent action by the scientific community. Lancet Microbe 2009, 9, 292. [Google Scholar] [CrossRef]
- Wondfo. Finecare 2019-nCoV RBD Antibody Test. 2021. Available online: https://www.finecare.it/wp-content/uploads/2021/04/W290_RBD_Antibody_Binder.pdf (accessed on 20 June 2022).
- Younes, S.; Al-Jighefee, H.; Shurrab, F.; Al-Sadeq, D.W.; Younes, N.; Dargham, S.R.; Liu, P. Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-CoV-2 Individuals. Microorganisms 2021, 9, 2771. [Google Scholar] [CrossRef]
- Ismail, A.; Shurrab, F.M.; Al-Jighefee, H.T.; Al-Sadeq, D.W.; Qotba, H.; Al-Shaar, I.A.; Ramuta, M.D.; Reynaldi, A. Can commercial automated immunoassays be utilized to predict neutralizing antibodies after SARS-CoV-2 infection? A comparative study between three different assays. Front. Biosci. 2021, 26, 198–206. [Google Scholar]
- Nuccetelli, M.; Pieri, M.; Grelli, S.; Ciotti, M.; Miano, R.; Andreoni, M.; Bernardini, S. SARS-CoV-2 infection serology: A useful tool to overcome lockdown? Cell Death Discov. 2020, 6, 38. [Google Scholar] [CrossRef]
- IgG(CLIA) ICM-C-MS-C-2020. Available online: https://www.mindray.com/en/product/CL-900i.html (accessed on 14 January 2022).
- BIOMÉRIEUX. VIDAS® SARS-CoV-2. 2020. Available online: https://www.biomerieux-diagnostics.com/vidas-sars-cov-2 (accessed on 14 January 2022).
- VIPA-S-C-TRP-If U. VITROS Immunodiagnostic Products Anti-SARS-CoV-2 Total Reagent Pack—Instructions for Use. 2021. Available online: https://www.fda.gov/media/136967/download (accessed on 14 January 2022).
- Miot, H.A. Correlation analysis in clinical and experimental studies. J. Vasc Bras. 2018, 17, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Kirch, W. Kappa coefficient. In Encyclopedia of Public Health; Springer: Dordrecht, The Netherlands, 2008; pp. 821–822. [Google Scholar]
- Fulford, T.S.; Van, H.; Gherardin, N.A.; Zheng, S.; Ciula, M.; Drummer, H.E.; Lim, S.M. A point-of-care lateral flow assay for neutralising antibodies against SARS-CoV-2. EBioMedicine 2021, 74, 103729. [Google Scholar] [CrossRef]
- Lu, L.; Mok, B.W.; Chen, L.L.; Chan, J.M.; Tsang, O.T.; Lam, B.H.; Tang, M.S.; Case, J.B. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. Clin. Infect. Dis. 2021, 2, 181. [Google Scholar]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.C.; Tiu, C.; Hu, Z.; Wei Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2–spike protein–protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Valcourt, E.J.; Manguiat, K.; Robinson, A.; Chen, J.C.; Dimitrova, K.; Philipson, C.; Anderson, N.W.; Henderson, J.P. Evaluation of a commercially-available surrogate virus neutralization test for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). Diagn. Microbiol. Infect. Dis. 2021, 99, 115294. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.S.; Case, J.B.; Franks, C.E.; Chen, R.E.; Anderson, N.W.; Henderson, J.P.; Diamond, M.S.; Gronowski, A.M.; Farnsworth, C.W. Association between SARS-CoV-2 Neutralizing Antibodies and Commercial Serological Assays. Clin. Chem. 2020, 66, 1538–1547. [Google Scholar] [CrossRef] [PubMed]
- Hörber, S.; Soldo, J.; Relker, L.; Jürgens, S.; Guther, J.; Peter, S.; Lehmann, R.; Peter, A. Evaluation of three fully-automated SARS-CoV-2 antibody assays. Clin. Chem. Lab. Med. 2020, 58, 2113–2120. [Google Scholar] [CrossRef] [PubMed]
- Seydoux, E.; Homad, L.J.; MacCamy, A.J.; Parks, K.R.; Hurlburt, N.K.; Jennewein, M.F.; Al-Sadeq, D.W.; Qotba, H. Characterization of neutralizing antibodies from a SARS-CoV-2 infected individual. bioRxiv 2020. bioRxiv:2020.05.12.091298. [Google Scholar]
- Rump, A.; Risti, R.; Kristal, M.-L.; Reut, J.; Syritski, V.; Lookene, A.; Relker, L.; Jürgens, S. Dual ELISA using SARS-CoV-2 nucleocapsid protein produced in E. coli and CHO cells reveals epitope masking by N-glycosylation. Biochem. Biophys. Res. Commun. 2021, 534, 457–460. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Manufacturer | Automated Analyzer | Detection Method | Targeted Antigen | Sample Volume | Result Interpretation | Reported Sensitivity | Reported Specificity | WHO Conversion Factor | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Mindray Bio-Medical Electronics Co., Ltd (Shenzhen, China) | Mindray CL-900i® SARS-CoV-2 S-RBD IgG | CLIA * | S-RBD | 10 μL (this volume does not include the dead volume) | <10 AU/mL: Negative ≥10 AU/mL: Positive | 100% (≥15 days) | 94.9% | 1.15 | [15,16] |
| BioMérieux Diagnostics (Marcy-l’Étoile, France) | VIDAS®3 SARS-CoV-2 IgG | ELFA * | S-RBD | 100 μL (including the dead volume) | <1 AU/mL: Negative ≥1 AU/mL: Positive | 100% (≥15 days) | 98.5% | 20.3 | [17] |
| Ortho Clinical Diagnostics (New Jersey, USA) | Ortho VITROS® anti-SARS-CoV-2 Total Ab | CLIA | S (S1 subunit) | 20 μL (this volume does not include the dead volume) | <1.0 S/C: Negative ≥1.0 S/C: Positive | NR | 100% | 17.8 | [18] |
| Test | Compared to | Overall Percent Agreement (OPA) | Positive Percent Agreement (PPA) | Negative Percent Agreement (NPA) | Accuracy/Efficiency | Cohen’s Kappa Statistic |
|---|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | % (95% CI) | k (95% CI) | ||
| FinecareTM | VIDAS®3 | 100 (98.90–100) | 100 (98.90–100) | 100 (2.5–100.00) | 100 (98.90–100.00) | 1.00 (00.40–0.86) |
| CL-900i® | 100 (99.25–100.00) | 100 (99.25–100.00) | 100 (15.81–100) | 100 (99.25–100.00) | 1.00 (0.52 to 0.96) | |
| VITROS® | 100 (98.85–100) | 100 (98.84–100) | 100 (2.5–100.00) | 100 (98.85–100.00) | 1.00 (00.46–0.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Younes, N.; Al-Sadeq, D.W.; Shurrab, F.M.; Zedan, H.T.; Abou-Saleh, H.; Abo-Halawa, B.Y.; AlHamaydeh, F.M.; Elsharafi, A.E.; Daas, H.I.; Thomas, S.; et al. Validation of a Novel Fluorescent Lateral Flow Assay for Rapid Qualitative and Quantitative Assessment of Total Anti-SARS-CoV-2 S-RBD Binding Antibody Units (BAU) from Plasma or Fingerstick Whole-Blood of COVID-19 Vaccinees. Vaccines 2022, 10, 1318. https://doi.org/10.3390/vaccines10081318
Younes N, Al-Sadeq DW, Shurrab FM, Zedan HT, Abou-Saleh H, Abo-Halawa BY, AlHamaydeh FM, Elsharafi AE, Daas HI, Thomas S, et al. Validation of a Novel Fluorescent Lateral Flow Assay for Rapid Qualitative and Quantitative Assessment of Total Anti-SARS-CoV-2 S-RBD Binding Antibody Units (BAU) from Plasma or Fingerstick Whole-Blood of COVID-19 Vaccinees. Vaccines. 2022; 10(8):1318. https://doi.org/10.3390/vaccines10081318
Chicago/Turabian StyleYounes, Nadin, Duaa W. Al-Sadeq, Farah M. Shurrab, Hadeel T. Zedan, Haissam Abou-Saleh, Bushra Y. Abo-Halawa, Fatima M. AlHamaydeh, Amira E. Elsharafi, Hanin I. Daas, Swapna Thomas, and et al. 2022. "Validation of a Novel Fluorescent Lateral Flow Assay for Rapid Qualitative and Quantitative Assessment of Total Anti-SARS-CoV-2 S-RBD Binding Antibody Units (BAU) from Plasma or Fingerstick Whole-Blood of COVID-19 Vaccinees" Vaccines 10, no. 8: 1318. https://doi.org/10.3390/vaccines10081318
APA StyleYounes, N., Al-Sadeq, D. W., Shurrab, F. M., Zedan, H. T., Abou-Saleh, H., Abo-Halawa, B. Y., AlHamaydeh, F. M., Elsharafi, A. E., Daas, H. I., Thomas, S., Aboalmaaly, S., Al Farsi, A., Al-Buainain, R., Ataelmannan, S., Paul, J., Al Saadi, A. S., Yassine, H. M., Majdalawieh, A. F., Ismail, A., ... Nasrallah, G. K. (2022). Validation of a Novel Fluorescent Lateral Flow Assay for Rapid Qualitative and Quantitative Assessment of Total Anti-SARS-CoV-2 S-RBD Binding Antibody Units (BAU) from Plasma or Fingerstick Whole-Blood of COVID-19 Vaccinees. Vaccines, 10(8), 1318. https://doi.org/10.3390/vaccines10081318