
Higher Collective Responsibility, Higher COVID-19 Vaccine Uptake, and Interaction with Vaccine Attitude: Results from Propensity Score Matching



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Measures
2.2.1. COVID-19 Vaccine Uptake (VU)
2.2.2. COVID-19 Vaccine Attitude (VA)
2.2.3. Subjective Norm (SN)
2.2.4. Perceived Behavioral Control (PBC)
2.2.5. Collective Responsibility (CR)
2.2.6. Socio-Demographic Characteristics
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Baseline Covariates after Propensity Score Matching
3.3. The Association of Collective Responsibility and COVID-19 Vaccine Uptake
4. Discussion
4.1. Higher Collective Responsibility Predicts Higher COVID-19 Vaccine Uptake
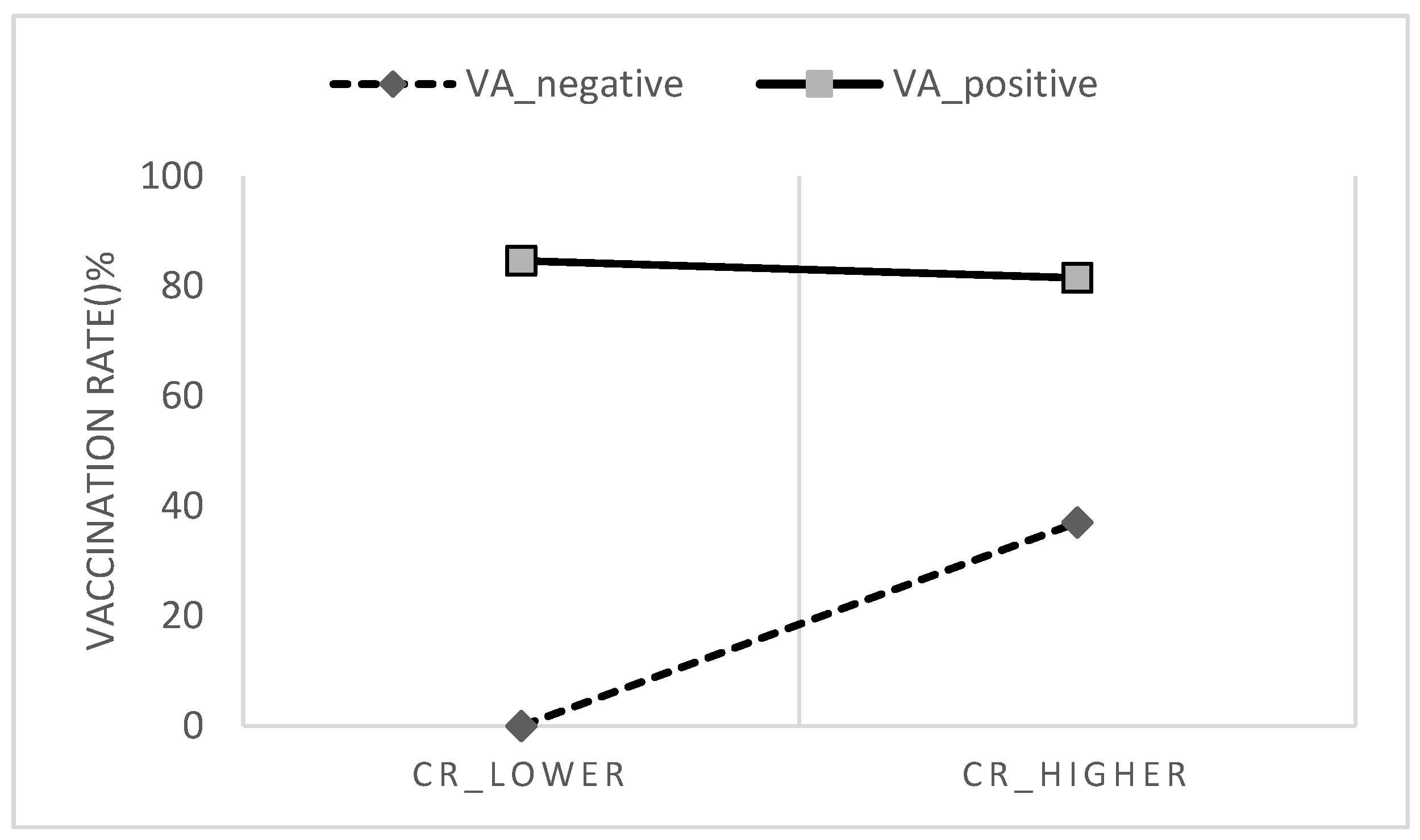
4.2. Collective Responsibility Is More Effective among Individuals Having More Negative COVID-19 Vaccine Attitude
4.3. Implications
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometer. COVID-19 Coronavirus Pandemic. 2022. Available online: https://www.worldometers.info/coronavirus/ (accessed on 8 July 2022).
- León, T.M. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis—California and New York, May–November 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. First COVID-19 Booster Dose in the General Population: A Systematic Review and Meta-Analysis of Willingness and Its Predictors. Vaccines 2022, 10, 1097. [Google Scholar] [CrossRef]
- Friedrich, M. WHO’s top health threats for 2019. JAMA 2019, 321, 1041. [Google Scholar] [CrossRef]
- DiClemente, R.J.; Salazar, L.F.; Crosby, R.A. Health Behavior Theory for Public Health: Principles, Foundations, and Applications; Jones & Bartlett Publishers: Burlington, MA, USA, 2013. [Google Scholar]
- Steptoe, A.; Freedland, K.E.; Jennings, J.R.; Manuck, S.B.; Susman, E.J. Handbook of Behavioral Medicine; Springer: New York, NY, USA, 2010. [Google Scholar]
- Betsch, C.; Böhm, R.; Korn, L. Inviting free-riders or appealing to prosocial behavior? game-theoretical reflections on communicating herd immunity in vaccine advocacy. Health Psychol. 2013, 32, 978–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of influenza vaccination intention and behavior–a systematic review of influenza vaccine hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Volpp, K.G.; Loewenstein, G.; Buttenheim, A.M. Behaviorally informed strategies for a national COVID-19 vaccine promotion program. JAMA 2021, 325, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Rizzo, C.; Rosselli, R.; Battista, T.; Conforto, A.; Cimino, L.; Poscia, A.; Fiacchini, D. Ten Actions to Counteract Vaccine Hesitancy Suggested by the Italian Society of Hygiene, Preventive Medicine, and Public Health. Vaccines 2022, 10, 1030. [Google Scholar] [CrossRef]
- Ajzen, I.; Madden, T.J. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J. Exp. Soc. Psychol. 1986, 22, 453–474. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine 2020, 38, 5131–5138. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Sheeran, P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol. Bull. 2006, 132, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheeran, P.; Webb, T.L. The intention–behavior gap. Soc. Personal. Psychol. Compass 2016, 10, 503–518. [Google Scholar] [CrossRef]
- Marks, G.; Burris, S.; Peterman, T.A. Reducing sexual transmission of HIV from those who know they are infected: The need for personal and collective responsibility. AIDS 1999, 13, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Newton, L.H. Collective responsibility in health care. J. Med. Philos. 1982, 7, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of vaccination readiness. Eur. J. Psychol. Assess. 2021; advance online publication. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Liu, P.L.; Ao, S.H.; Zhao, X.; Zhang, L. Associations between COVID-19 information acquisition and vaccination intention: The roles of anticipated regret and collective responsibility. Health Commun. 2022; Advance online publication. [Google Scholar] [CrossRef]
- Böhm, R.; Betsch, C. Prosocial vaccination. Curr. Opin. Psychol. 2022, 43, 307–311. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2022, 31, 62–86. [Google Scholar] [CrossRef] [PubMed]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing vaccination: Putting psychological science into action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, L.P.; Alias, H.; Danaee, M.; Ahmed, J.; Lachyan, A.; Cai, C.Z.; Lin, Y.; Hu, Z.; Tan, S.Y.; Lu, Y.; et al. COVID-19 vaccination intention and vaccine characteristics influencing vaccination acceptance: A global survey of 17 countries. Infect. Dis. Poverty 2021, 10, 122. [Google Scholar] [CrossRef]
- Navin, M.C.; Oberleitner, L.M.-S.; Lucia, V.C.; Ozdych, M.; Afonso, N.; Kennedy, R.H.; Keil, H.; Wu, L.; Mathew, T.A. COVID-19 Vaccine Hesitancy Among Healthcare Personnel Who Generally Accept Vaccines. J. Community Health 2022, 47, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Government of Macao Special Administrative Region Statistics and Census Service. Macao in Figures. 2021. Available online: https://www.dsec.gov.mo/en-US/Home/Publication/MacaoInFigures (accessed on 8 July 2022).
- Government of Macao Special Administrative Region Statistics and Census Service. Tourism Satellite Account 2019. 2021. Available online: https://www.dsec.gov.mo/getAttachment/57d1dbb0-2a70-4555-8ef5-88b2858e2525/C_TSA_PUB_2019_Y.aspx (accessed on 8 July 2022).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations?country=MAC (accessed on 8 July 2022).
- Macao SAR Government Health Bureau. COVID-19 Vaccine Information Page. Available online: https://www.ssm.gov.mo/apps1/covid19vaccine/ch.aspx#clg18751 (accessed on 8 July 2022).
- Shi, J.; Mo, X.; Sun, Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao. Yi Xue Ban J. Cent. South University. Med. Sci. 2012, 37, 152–155. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. Constructing a Theory of Planned Behavior Questionnaire. 2006. Available online: https://people.umass.edu/aizen/tpb.html (accessed on 8 July 2022).
- Thoemmes, F. Propensity score matching in SPSS. arXiv 2012, arXiv:1201.6385. [Google Scholar]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Nicholls, L.A.B.; Gallant, A.J.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Older adults’ vaccine hesitancy: Psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine 2021, 39, 3520–3527. [Google Scholar] [CrossRef]
- Dorman, C.; Perera, A.; Condon, C.; Chau, C.; Qian, J.; Kalk, K.; DiazDeleon, D. Factors associated with willingness to be vaccinated against COVID-19 in a large convenience sample. J. Community Health 2021, 46, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Böhm, R.; Betsch, C.; Korn, L. Selfish-rational non-vaccination: Experimental evidence from an interactive vaccination game. J. Econ. Behav. Organ. 2016, 131, 183–195. [Google Scholar] [CrossRef]
- Fan, C.-W.; Chen, I.-H.; Ko, N.-Y.; Yen, C.-F.; Lin, C.-Y.; Griffiths, M.D.; Pakpour, A.H. Extended theory of planned behavior in explaining the intention to COVID-19 vaccination uptake among mainland Chinese university students: An online survey study. Hum. Vaccines Immunother. 2021, 17, 3413–3420. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Romanowich, P.; Hantula, D.A. Predicting Intention to Take a COVID-19 Vaccine in the United States: Application and Extension of Theory of Planned Behavior. Am. J. Health Promot. 2022, 36, 710–713. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, Z.; Sultana, R.; Hossain, R.; Browning, M.H.E.M.; Alam, A.; Sallam, M. Determinants of COVID-19 vaccine acceptance among the adult population of Bangladesh using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Willis, D.E.; Selig, J.P.; Andersen, J.A.; Hall, S.; Hallgren, E.; Williams, M.; Bryant-Moore, K.; McElfish, P.A. Hesitant but vaccinated: Assessing COVID-19 vaccine hesitancy among the recently vaccinated. J. Behav. Med. 2022, 1–10, Advance online publication. [Google Scholar] [CrossRef]
- Ieng, S.M.; Cheong, I.H. An overview of epidemiology of COVID-19 in Macau SAR. Front. Public Health 2020, 8, 550057. [Google Scholar] [CrossRef]
- Zhang, M.; Prevention, G.G.P.C.F.D.C.A.; Xiao, J.; Deng, A.; Zhang, Y.; Zhuang, Y.; Hu, T.; Li, J.; Tu, H.; Li, B.; et al. Transmission dynamics of an outbreak of the COVID-19 Delta variant B. 1.617. 2—Guangdong Province, China, May–June 2021. China CDC Wkly. 2021, 3, 584–586. [Google Scholar] [CrossRef]
- Tustin, J.L.; Crowcroft, N.S.; Gesink, D.; Johnson, I.; Keelan, J. Internet exposure associated with Canadian parents’ perception of risk on childhood immunization: Cross-sectional study. JMIR Public Health Surveill. 2018, 4, e8921. [Google Scholar] [CrossRef]
- Ross, M.E.; Kreider, A.R.; Huang, Y.-S.; Matone, M.; Rubin, D.M.; Localio, A.R. Propensity score methods for analyzing observational data like randomized experiments: Challenges and solutions for rare outcomes and exposures. Am. J. Epidemiol. 2015, 181, 989–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McRee, A.-L.; Gower, A.L.; Kiss, D.E.; Reiter, P.L. Has the COVID-19 pandemic affected general vaccination hesitancy? Findings from a national study. J. Behav. Med. 2022; advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Albarracín, D. Concerns for others increase the likelihood of vaccination against influenza and COVID-19 more in sparsely rather than densely populated areas. Proc. Natl. Acad. Sci. USA 2021, 118, e2007538118. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Count | % |
|---|---|---|
| Gender | ||
| Male | 222 | 36.5 |
| Female | 386 | 63.5 |
| Education | ||
| High school or below | 284 | 46.7 |
| Diploma or above | 324 | 53.3 |
| Marital status | ||
| Single | 236 | 38.8 |
| Married | 372 | 61.2 |
| Living with older adults or children | ||
| No | 217 | 35.7 |
| Yes | 391 | 64.3 |
| Monthly income (in local currency MOP) | ||
| ≤10,000 | 98 | 16.1 |
| 10,001∼20,000 | 237 | 39.0 |
| 20,001∼30,000 | 198 | 32.6 |
| 30,001∼30,000 | 49 | 8.1 |
| ≥40,001 | 26 | 4.2 |
| Working industries | ||
| Travel agency | 125 | 20.6 |
| Gaming | 167 | 27.5 |
| Food and beverage | 178 | 29.3 |
| Others | 138 | 22.7 |
| Receiving COVID-19 vaccine | ||
| Not willing to be vaccinated | 38 | 6.3 |
| Undecided whether to vaccinate | 109 | 17.9 |
| Not yet, but planning to vaccinate | 81 | 13.3 |
| 1 dose has been received | 86 | 14.1 |
| 2 doses have been received | 294 | 48.4 |
| Characteristics | Before PSM | After PSM | ||||||
|---|---|---|---|---|---|---|---|---|
| CR-Lower Group | CR-Higher Group | SMD | p-Value | CR-Lower Group | CR-Higher Group | SMD | p-Value | |
| No. of participants | 268 | 340 | 173 | 173 | ||||
| Age, mean ± SD | 36.73 ± 9.53 | 39.46 ± 10.84 | 0.26 | 0.001 | 39.67 ± 9.75 | 39.64 ± 10.90 | <0.01 | 0.974 |
| COVID-19 VA, mean ± SD | −2.25 ± 12.94 | 8.20 ± 13.22 | 0.74 | <0.001 | 2.23 ± 10.93 | 2.82 ± 11.67 | 0.05 | 0.628 |
| SN, mean ± SD | 49.25 ± 22.72 | 67.19 ± 23.93 | 0.71 | <0.001 | 56.45 ± 23.00 | 55.54 ± 21.17 | 0.04 | 0.703 |
| PBC | 0.26 | <0.001 | 0.04 | 0.808 | ||||
| Difficult or very difficult | 22 (8.2%) | 9 (2.6%) | 7 (4.0%) | 9 (5.2%) | ||||
| Moderate | 98 (36.6%) | 62 (18.2%) | 52 (30.1%) | 48 (27.7%) | ||||
| Easy or very easy | 148 (55.2%) | 269 (79.1%) | 114 (65.9%) | 116 (67.1%) | ||||
| Gender | 0.71 | 0.029 | 0.01 | 0.819 | ||||
| Male | 85 (31.7%) | 137 (40.3%) | 58 (33.5%) | 56 (32.4%) | ||||
| Female | 183 (68.3%) | 203 (59.7%) | 115 (66.5%) | 117 (67.6%) | ||||
| Education | 0.03 | 0.532 | 0.04 | 0.452 | ||||
| High school or below | 129 (48.1%) | 155 (45.6%) | 92 (53.2%) | 85 (49.1%) | ||||
| Diploma or above | 139 (51.9%) | 185 (54.4%) | 81 (46.8%) | 88 (50.9%) | ||||
| Marital status | 0.05 | 0.181 | 0.01 | 0.911 | ||||
| Single | 112 (41.8%) | 124 (36.5%) | 62 (35.8%) | 63 (36.4%) | ||||
| Married | 156 (58.2%) | 216 (63.5%) | 111 (64.2%) | 110 (63.6%) | ||||
| Living with older adults or children | 0.01 | 0.818 | 0.03 | 0.568 | ||||
| No | 97 (36.2%) | 120 (35.3%) | 55 (31.8%) | 60 (34.7%) | ||||
| Yes | 171 (63.8%) | 220 (64.7%) | 118 (68.2%) | 113 (65.3%) | ||||
| Monthly income (in local currency MOP) | 0.12 | 0.081 | 0.09 | 0.619 | ||||
| ≤10,000 | 41 (15.3%) | 57 (16.8%) | 33 (19.1%) | 30 (17.3%) | ||||
| 10,001~20,000 | 97 (36.2%) | 140 (41.2%) | 61 (35.3%) | 64 (37.0%) | ||||
| 20,001~30,000 | 103 (38.4%) | 95 (27.9%) | 59 (34.1%) | 55 (31.8%) | ||||
| 30,001~40,000 | 17 (6.3%) | 32 (9.4%) | 11 (6.4%) | 18 (10.4%) | ||||
| ≧40,001 | 10 (3.7%) | 16 (4.7%) | 9 (5.2%) | 6 (3.5%) | ||||
| Working industries | 0.14 | 0.011 | 0.10 | 0.311 | ||||
| Travel agency | 43 (16.0%) | 82 (24.1%) | 37 (21.4%) | 39 (22.5%) | ||||
| Gaming | 84 (31.3%) | 83 (24.4%) | 59 (34.1%) | 55 (31.8%) | ||||
| Food and beverage | 71 (26.5%) | 107 (31.5%) | 52 (30.1%) | 42 (24.3%) | ||||
| Others | 70 (26.1%) | 68 (20.0%) | 25 (14.5%) | 37 (21.4%) | ||||
| COVID-19 vaccine uptake | 0.31 | <0.001 | 0.15 | 0.005 | ||||
| No | 146 (54.5%) | 82 (24.1%) | 87 (50.3%) | 61 (35.3%) | ||||
| Yes | 122 (45.5%) | 258 (75.9%) | 86 (49.7%) | 112 (64.7%) | ||||
| Variables | Coefficient | S.E. | Wald | p-Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| COVID-19 VA | 0.139 | 0.029 | 23.304 | <0.001 | 1.149 | 1.086 | 1.216 |
| SN | 0.012 | 0.007 | 2.868 | 0.090 | 1.012 | 0.998 | 1.027 |
| PBC | 32.892 | <0.001 | |||||
| PBC (moderate = 1) | −0.073 | 0.755 | 0.009 | 0.923 | 0.929 | 0.212 | 4.078 |
| PBC (easy or very easy = 1) | 1.729 | 0.737 | 5.510 | 0.019 | 5.636 | 1.330 | 23.882 |
| CR (higher group = 1) | 0.728 | 0.289 | 6.330 | 0.012 | 2.070 | 1.174 | 3.650 |
| Zscore_COVID-19 VA × CR | −0.081 | 0.035 | 5.478 | 0.019 | 0.922 | 0.861 | 0.987 |
| Working industries | 3.212 | 0.360 | |||||
| Working industries (travel agency = 1) | −0.750 | 0.566 | 1.757 | 0.185 | 0.472 | 0.156 | 1.432 |
| Working industries (gaming = 1) | −0.254 | 0.434 | 0.342 | 0.558 | 0.776 | 0.331 | 1.816 |
| Working industries (food and beverage = 1) | 0.221 | 0.453 | 0.239 | 0.625 | 1.248 | 0.513 | 3.034 |
| Age | 0.004 | 0.018 | 0.039 | 0.844 | 1.004 | 0.968 | 1.041 |
| Education (diploma or above = 1) | 0.430 | 0.341 | 1.590 | 0.207 | 1.537 | 0.788 | 2.999 |
| Monthly income | −0.041 | 0.154 | 0.073 | 0.787 | 0.959 | 0.710 | 1.296 |
| Gender (female = 1) | −0.124 | 0.319 | 0.151 | 0.698 | 0.883 | 0.473 | 1.650 |
| Marital status (married = 1) | 0.475 | 0.334 | 2.027 | 0.155 | 1.609 | 0.836 | 3.095 |
| Living with older adults or children (yes = 1) | −0.008 | 0.322 | 0.001 | 0.981 | 0.992 | 0.528 | 1.865 |
| Constant | −2.459 | 1.325 | 3.443 | 0.064 | 0.085 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.; Chen, C.H.; Wang, H.; Zhang, J. Higher Collective Responsibility, Higher COVID-19 Vaccine Uptake, and Interaction with Vaccine Attitude: Results from Propensity Score Matching. Vaccines 2022, 10, 1295. https://doi.org/10.3390/vaccines10081295
Wu J, Chen CH, Wang H, Zhang J. Higher Collective Responsibility, Higher COVID-19 Vaccine Uptake, and Interaction with Vaccine Attitude: Results from Propensity Score Matching. Vaccines. 2022; 10(8):1295. https://doi.org/10.3390/vaccines10081295
Chicago/Turabian StyleWu, Jianwei, Caleb Huanyong Chen, Hui Wang, and Jinghua Zhang. 2022. "Higher Collective Responsibility, Higher COVID-19 Vaccine Uptake, and Interaction with Vaccine Attitude: Results from Propensity Score Matching" Vaccines 10, no. 8: 1295. https://doi.org/10.3390/vaccines10081295
APA StyleWu, J., Chen, C. H., Wang, H., & Zhang, J. (2022). Higher Collective Responsibility, Higher COVID-19 Vaccine Uptake, and Interaction with Vaccine Attitude: Results from Propensity Score Matching. Vaccines, 10(8), 1295. https://doi.org/10.3390/vaccines10081295