
Behavioural and Cognitive Attitudes of Paediatricians towards Influenza Self-Vaccination—Partial Mediation Model

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Assumptions of Theory of Interpersonal Behaviour
Hypotheses
3. Materials and Methods
3.1. Design and Settings
3.2. Participants and Sample Size
3.3. Data Collection
3.4. Research Instrument
3.5. Statistical Analysis
3.6. Ethical Considerations
4. Results
4.1. Characteristics of Study Participants
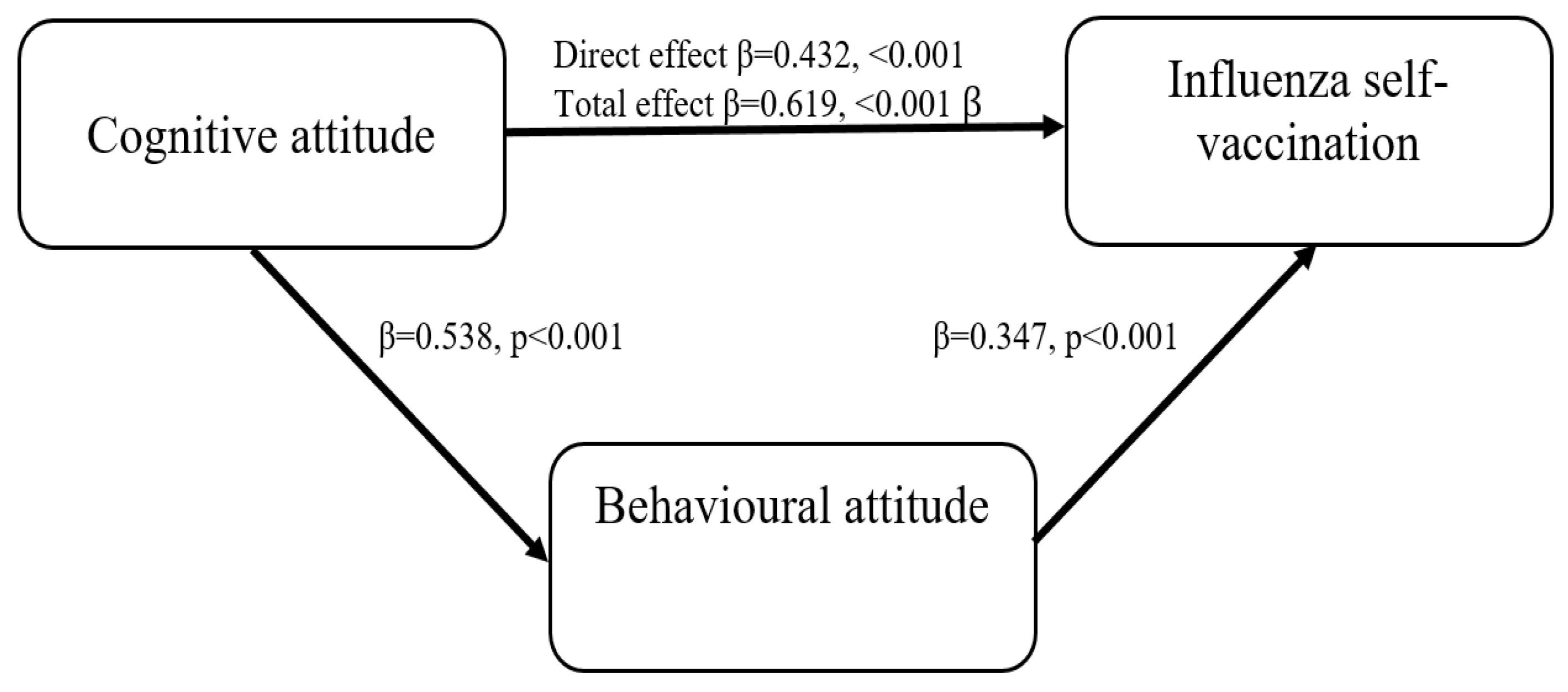
4.2. Cognitive and Behavioural Attitudes and Influenza Self-Vaccination
5. Discussion
Limitations of the Study
6. Conclusions and Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marek, L.; Hobbs, M.; McCarthy, J.; Wiki, J.; Tomintz, M.; Campbell, M.; Kingham, S. Investigating spatial variation and change (2006–2017) in childhood immunisation coverage in New Zealand. Soc. Sci. Med. 2020, 15, 264. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Herbert, N.L.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Rask, K.; Murray, D.; DiClemente, R.J.; Hughes, J.M. Impact of a physician recommendation and parental immunization attitudes on receipt or intention to receive adolescent vaccines. Hum. Vaccines Immunother. 2013, 9, 2627–2633. Available online: https://pubmed.ncbi.nlm.nih.gov/23883781/ (accessed on 22 April 2022). [CrossRef] [PubMed] [Green Version]
- Peretti-Watel, P.; Larson, H.J.; Ward, J.K.; Schulz, W.S.; Verger, P. Vaccine hesitancy: Clarifying a theoretical framework for an ambiguous notion. PLoS ONE 2015, 25, 7. Available online: https://pubmed.ncbi.nlm.nih.gov/25789201/ (accessed on 23 April 2022). [CrossRef] [PubMed]
- Bricout, H.; Torcel-Pagnon, L.; Lecomte, C.; Almas, M.F.; Matthews, I.; Lu, X.; Wheelock, A.; Sevdalis, N. Determinants of shingles vaccine acceptance in the United Kingdom. PLoS ONE 2019, 14, e0220230. [Google Scholar] [CrossRef] [Green Version]
- Arora, G.; Lehman, D.; Charlu, S.; Ross, N.; Ardy, A.; Gordon, B.; Pannaraj, P.S. Vaccine health beliefs and educational influences among pediatric residents. Vaccine 2019, 37, 857–862. [Google Scholar] [CrossRef]
- Smith, P.J.; Kennedy, A.M.; Wooten, K.; Gust, D.A.; Pickering, L.K. Association between health care providers’ influence on parents who have concerns about vaccine safety and vaccination coverage. Pediatrics 2006, 118, 1287–1292. [Google Scholar] [CrossRef]
- Patel, P.R.; Abbey, B.B. Sources of HPV vaccine hesitancy in parents. Hum. Vaccines Immunother. 2013, 9, 2649–2653. Available online: https://pubmed.ncbi.nlm.nih.gov/23982270/ (accessed on 3 March 2022). [CrossRef] [Green Version]
- Tickner, S.; Leman, P.J.; Woodcock, A. Factors underlying suboptimal childhood immunisation. Vaccine 2006, 24, 7030–7036. [Google Scholar] [CrossRef]
- Michalik, A.; Gawlik, K. Attitudes and knowledge of Health care workers in Cieszyn County of the Silesian Province in southern Poland about seasonal flu vaccinations—Preliminary study. Med. Ogólna Nauk. Zdrowiu 2020, 26, 35–41. Available online: http://www.monz.pl/Attitudes-and-knowledge-of-Health-care-workers-in-Cieszyn-County-of-the-Silesian,115121,0,2.html (accessed on 3 March 2022). [CrossRef]
- Kuchar, E.; Ludwikowska, K.; Szenborn, L.; Antczak, A.; Mastalerz-Migas, A.; Nitsch- Osuch, A. Knowledge Regarding Influenza and Influenza Vaccination in General Population: Results of a National Survey in Poland. Adv. Exp. Med. Biol. 2018, 1108, 55–61. [Google Scholar] [CrossRef]
- Stefanoff, P.; Sobierajski, T.; Bulinska-Stangrecka, H.; Augustynowicz, E. Exploring Factors Improving for Support Vaccinations Among Polish Primary Care Physicians. PLoS ONE 2020, 15, e0232722. [Google Scholar] [CrossRef]
- Pellulo, C.P.; Della Polla, G.; Napolitano, F.; Di Giuseppe, G.; Angelillo, I.F. Healthcare Workers’ Knowledge, Attitudes, and Practices about Vaccinations: A Cross-Sectional Study in Italy. Vaccines 2020, 26, 148. [Google Scholar] [CrossRef] [Green Version]
- Schlemper, B.R., Jr.; Beltrame, V.; Hellmann, F. The Ethical Duty of Physicians to Strengthen Their Own Immunization and Childhood Vaccination. In Reflections on Bioethics; Morales-Gonzales, J.A., Aguilar Najera, M.E., Eds.; Intechopen: Rijeka, Croatia, 2018; Available online: https://www.intechopen.com/books/reflections-on-bioethics/the-ethical-duty-of-physicians-to-strengthen-their-own-immunization-and-childhood-vaccination (accessed on 12 December 2021).
- Collange, F.; Verger, P.; Launay, O.; Pulcini, C. Knowledge, attitudes, beliefs and behaviors of general practitioners/family physicians toward their own vaccination: A systematic review. Hum. Vaccines Immunother. 2016, 12, 1282–1292. [Google Scholar] [CrossRef]
- Manca, T. One of the greatest medical success stories: Physicians and nurses’ small stories about vaccine knowledge and anxieties. Soc. Sci. Med. 2018, 196, 182–189. [Google Scholar] [CrossRef]
- Picchio, C.A.; Garcia Carrasco, M.; Sagué-Vilavella, M.; Rius, C. Knowledge, attitudes, and beliefs about vaccination in primary healthcare workers involved in the administration of systematic childhood vaccines, Barcelona, 2016/17. Eurosurveillance 2019, 24, 1800117. Available online: https://pubmed.ncbi.nlm.nih.gov/30755298/ (accessed on 11 April 2022). [CrossRef] [Green Version]
- Triandis, H.C. Attitude and Attitude Change. Foundations of Social Psychology; John Wiley & Sons Inc.: Hoboken, NJ, USA, 1971. [Google Scholar]
- Triandis, H.C. Individualism & Collectivism; Routledge Taylor & Francis Group: New York, NY, USA; London, UK, 1977. [Google Scholar]
- Anonymous. Announcement of the Chief Sanitary Inspectorate of 28 October 2021 notice on the National Vaccination Program. Journal of Laws; Dz. U. 2020, poz. 1845. 2022. Available online: http://dziennikmz.mz.gov.pl/legalact/2020/117/ (accessed on 4 May 2022).
- Al-Rafee, S.; Cronan, T.P. Digital piracy: Factors that influence attitude toward behaviour. J. Bus. Ethics 2006, 63, 237–259. [Google Scholar] [CrossRef]
- Zimmerman, D.W.; Zumbo, B.D.; Williams, R.H. Bias in Estimation and Hypothesis Testing of Correlation. Psicológica 2003, 24, 133–158. [Google Scholar]
- Hayes, A.F. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. Available online: https://pubmed.ncbi.nlm.nih.gov/18697684/ (accessed on 24 November 2021). [CrossRef]
- Lu, P.; Srivastav, A.; Santibanez, T.A.; Stringer, M.C.; Bostwick, M.; Dever, J.A.; Stanley Kurtz, M.; Williams, W.W. Knowledge of influenza vaccination recommendation and early vaccination uptake during the 2015–2016 season among adults aged ≥ 18 years-United States. Vaccine 2017, 35, 4346–4354. [Google Scholar] [CrossRef]
- Bekkat-Berkani, R.; Romano-Mazzotti, L. Understanding the unique characteristics of seasonal influenza illness to improve vaccine uptake in the US. Vaccine 2018, 36, 7276–7285. [Google Scholar] [CrossRef]
- Corace, K.M.; Srigley, J.A.; Hargadon, D.P.; Yu, D.; MacDonald, T.K.; Fabrigar, L.R.; Garber, G.E. Using behavior change frameworks to improve healthcare worker influenza vaccination rates: A systematic review. Vaccine 2016, 34, 3235–3242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulo, S.; Nuvoli, A.; Sobaszek, A.; Salembier-Trichard, A. Knowledge and attitudes towards influenza vaccination of health care workers in emergency services. Vaccine 2017, 35, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Çiftci, F.; Şen, E.; Demir, N.; Çiftci, O.; Erol, S.; Kayacan, O. Beliefs, attitudes, and activities of healthcare personnel about influenza and pneumococcal vaccines. Hum. Vaccines Immunother. 2018, 14, 111–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, L.; Newall, A.; Heywood, A.E. Knowledge, attitudes and practices of Australian medical students towards influenza vaccination. Vaccine 2016, 34, 6193–6199. [Google Scholar] [CrossRef]
- Klassen, A. Healthcare Worker Perceptions and Practices Regarding Influenza Vaccination, UA Campus Repository. 2016. Available online: https://repository.arizona.edu/bitstream/handle/10150/603632/Klassen_Thesis.pdf?sequence=8&isAllowed=y (accessed on 10 January 2022).
- Weston, D.; Blackburn, R.; Potts, H.W.W.; Hayward, A.C. Predictors of self and parental vaccination decisions in England during the 2009 H1N1 pandemic: Analysis of the Flu Watch pandemic cohort data. Vaccine 2017, 35, 3875–3882. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.P.; Allison, M.A.; Lindley, M.C.; Brtnikova, M.; Crane, L.A.; Beaty, B.L.; Hurley, L.P.; Kempe, A. Physician Knowledge and Attitudes About Hepatitis A and Current Practices Regarding Hepatitis A Vaccination Delivery. Acad. Pediatrics 2017, 17, 562–570. [Google Scholar] [CrossRef]
- Chang, V.C.L.; Wong, H.T.; Yeung, P.C.A.; Choi, Y.K.; Fok, M.S.Y.; Mak, O.I.; Wong, H.Y.; Wong, K.H.; Wong, S.Y.; Wong, Y.S.; et al. Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong. Int. J. Environ. Res. Public Health 2016, 13, 486. [Google Scholar] [CrossRef] [Green Version]
- Evren, E.Ü.; Evren, H.; Özcem, S.B.; Yazgan, Z.Ö.; Barış, S.A.; Yıldız, F. Knowledge of Physicians about Influenza and Pneumococcal Vaccination. Turk. Thorac. J. 2020, 21, 39–43. [Google Scholar] [CrossRef]
- Yasobant, S.; Saxena, D.; Puwar, T.; Trivedi, P.; Patel, S.; Fancy, M.J.; Patel, M. Knowledge of hepatitis B among doctors working in public health system of Gujarat, India: An interventional study. J. Family Med. Community Health 2017, 4, 1136. Available online: https://www.researchgate.net/publication/323320677_Knowledge_of_Hepatitis_B_among_Doctors_working_in_Public_Health_System_of_Gujarat_India_An_Interventional_Study (accessed on 10 January 2022).
- Bocquier, A.; Cortaredona, S.; Fressard, L.; Galtier, F.; Verger, P. Seasonal influenza vaccination among people with diabetes: Influence of patients’ characteristics and healthcare use on behavioral changes. Hum. Vaccines Immunother. 2020, 16, 2565–2572. [Google Scholar] [CrossRef] [Green Version]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiwan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in South Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Neuman-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. Available online: https://pubmed.ncbi.nlm.nih.gov/32591957/ (accessed on 4 May 2022). [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Malesza, M. Acceptance of COVID-19 Vaccination during Pandemic Phase of Coronavirus in Poland: Population Based Cross-sectional Survey. 2020. Available online: https://www.academia.edu/43690401/Acceptability_of_COVID_19_vaccination_during_pandemic_phase_of_coronavirus_in_Poland_population_based_cross_sectional_survey (accessed on 4 April 2022).


{kind=link}
| N | % | |
|---|---|---|
| Gender | ||
| Female | 326 | 80.9 |
| Male | 77 | 19.1 |
| Age | ||
| <40 | 39 | 9.6 |
| 41–50 | 66 | 16.4 |
| 51–60 | 158 | 39.2 |
| 61< | 107 | 26.6 |
| I do not want to specify | 33 | 8.2 |
| Seniority in the profession | ||
| Up to 5 years | 2 | 0.5 |
| More than 5 to 10 years | 23 | 5.7 |
| More than 10 to 15 years | 19 | 4.7 |
| Over 15 years | 359 | 89.1 |
| Self-assessment of knowledge about vaccines | ||
| Very bad | 0 | 0.0 |
| Bad | 2 | 0.5 |
| Average | 18 | 4.5 |
| Good | 211 | 52.4 |
| Very good | 168 | 41.7 |
| I do not know/hard to say | 4 | 1.0 |
| Strong Supporter of Vaccination | Moderate Supporter of Vaccination | Neither a Supporter Nor an Opponent of Vaccination | p Value | |
|---|---|---|---|---|
| N (%) | ||||
| Gender | ||||
| Female | 287 (88.0) | 39 (12.0) | 0 (0.0) | 0.024 |
| Male | 61 (79.2) | 15 (19.5) | 1 (1.3) | |
| Age | ||||
| <40 | 32 (82.1) | 7 (17.9) | 0 (0.0) | p < 0.001 |
| 41–50 | 52 (78.8) | 14 (21.2) | 0 (0.0) | |
| 51–60 | 144 (91.1) | 14 (8.9) | 0 (0.0) | |
| 61< | 91 (85.) | 16 (15.0) | 1 (0.9) | |
| I do not want to specify | 30 (90.9) | 3 (9.1) | 0 (0.0) | |
| Seniority in the profession | ||||
| Up to 5 years | 1 (50.0) | 1 (50.0) | 0 (0.0) | p = 0.863 |
| More than 5 to 10 years | 20 (87.0) | 3 (13.0) | 0 (0.0) | |
| More than 10 to 15 years | 16 (84.2) | 3 (15.8) | 0 (0.0) | |
| Over 15 years | 311 (86.6) | 47 (13.1) | 1 (0.3) | |
| Self-assessment of knowledge about vaccines | ||||
| Very bad | 0 (0.0) | 0 (0.0) | 0 (0.0) | p = 0.491 |
| Bad | 2 (100.0) | 0 (0.0) | 0 (0.0) | |
| Average | 15 (83.3) | 3 (16.7) | 0 (0.0) | |
| Good | 174 (82.5) | 36 (17.1) | 1 (0.5) | |
| Very good | 153 (91.1) | 15 (8.9) | 0 (0.0) | |
| I do not know/hard to say | 4 (100.0) | 0 (0.0) | 0 (0.0) | |
| I Vaccinate Only with Mandatory Vaccinations | I Vaccinate with Mandatory Vaccinations and Selected Recommended Vaccinations | I Vaccinate with Mandatory Vaccinations and All Recommended Vaccinations | I Do Not Vaccinate My Child at All | p Value | |
|---|---|---|---|---|---|
| N (%) | |||||
| Gender | |||||
| Female | 11 (3.4) | 154 (47.2) | 161 (49.4) | 0 (0.0) | p = 0.132 |
| Male | 1 (1.3) | 40 (51.9) | 35 (45.5) | 1 (1.3) | |
| Age | |||||
| <40 | 3 (7.7) | 19 (48.7) | 17 (43.6) | 0 (0.0) | p = 0.021 |
| 41–50 | 1 (1.5) | 34 (51.5) | 31 (47.0) | 0 (0.0) | |
| 51–60 | 3 (2.0) | 77 (48.7) | 77 (48.7) | 1 (0.6) | |
| 61< | 4 (3.7) | 47 (44.0) | 56 (52.3) | 0 (0.0) | |
| I do not want to specify | 0 (0.0) | 17 (51.5) | 16 (48.5) | 0 (0.0) | |
| Seniority in the profession | |||||
| Up to 5 years | 0 (0.0) | 2 (100.0) | 0 (0.0) | 0 (0.0) | p = 0.475 |
| More than 5 to 10 years | 0 (0.0) | 10 (43.5) | 13 (56.5) | 0 (0.0) | |
| More than 10 to 15 years | 2 (10.5) | 11 (57.9) | 6 (31.6) | 0 (0.0) | |
| Over 15 years | 10 (2.8) | 171 (47.6) | 177 (49.3) | 1 (0.3) | |
| Self-assessment of knowledge about vaccines | |||||
| Very bad | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | p = 0.383 |
| Bad | 0 (0.0) | 1 (50.0) | 1 (50.0) | 0 (0.0) | |
| Average | 1 (5.6) | 12 (66.7) | 5 (27.8) | 0 (0.0) | |
| Good | 9 (4.3) | 107 (50.7) | 94 (44.5) | 1 (0.5) | |
| Very good | 2 (1.2) | 71 (42.3) | 95 (56.5) | 0 (0.0) | |
| I do not know/hard to say | 0 (0.0) | 3 (75.0) | 1 (25.0) | 0 (0.0) | |
| Regularly Every Year or Almost Every Year | Irregularly from Time to Time | Never Get Vaccinated | p Value | |
|---|---|---|---|---|
| N (%) | ||||
| Gender | ||||
| Female | 203 (62.3) | 43 (13.2) | 80 (24.5) | p = 0.973 |
| Male | 49 (63.6) | 10 (13.0) | 18 (23.4) | |
| Age | ||||
| <40 | 21 (53.9) | 8 (20.5) | 10 (25.6) | p = 0.169 |
| 41–50 | 37 (56.0) | 10 (15.2) | 19 (28.8) | |
| 51–60 | 104 (56.8) | 19 (12.0) | 35 (22.2) | |
| 61< | 72 (66.3) | 12 (11.2) | 23 (21.5) | |
| I do not want to specify | 18 (54.5) | 4 (12.1) | 11 (33.3) | |
| Seniority in the profession | ||||
| Up to 5 years | 2 (100.0) | 0 (0.0) | 0 (0.0) | p = 0.681 |
| More than 5 to 10 years | 11 (47.8) | 5 (21.7) | 7 (30.4) | |
| More than 10 to 15 years | 13 (68.4) | 2 (10.5) | 4 (21.1) | |
| Over 15 years | 226 (63.0) | 46 (12.8) | 87 (24.2) | |
| Self-assessment of knowledge about vaccines | ||||
| Very bad | 0 (0.0) | 0 (0.0) | 0 (0.0) | p = 0.213 |
| Bad | 1 (50.0) | 1 (50.0) | 0 (0.0) | |
| Average | 13 (72.2) | 0 (0.0) | 5 (27.8) | |
| Good | 121 (57.3) | 32 (15.2) | 58 (27.5) | |
| Very good | 115 (68.5) | 19 (11.3) | 34 (20.2) | |
| I do not know/hard to say | 2 (50.0) | 1 (25.0) | 1 (25.0) | |
| Variable | Mean | SD | 1. | 2. | 3. |
|---|---|---|---|---|---|
| 1. Behavioural attitude | 2.45 | 0.568 | - | ||
| 2. Cognitive attitude | 3.86 | 0.392 | 0.285 * | - | |
| 3. Influenza self-vaccination | 1.38 | 0.851 | 0.371 * | 0.306 * | - |
| Bootstrap 95% Confidence Interval (CI) | |||||
|---|---|---|---|---|---|
| Effect (β) | SE | T | p | LLCI | ULCI |
| Total effect (βyx): cognitive attitude (X) on influenza self-vaccination (Y) | |||||
| 0.619 Fp = 35.410 R2 = 0.081 | 0.103 | 5.95 | <0.001 | 0.415 | 0.822 |
| Direct effect: cognitive attitude (X) on influenza self-vaccination (Y) | |||||
| 0.432 | 0.108 | 3.076 | <0.001 | 0.218 | 0.645 |
| Indirect effect (βyx.m): cognitive attitude (X) on influenza self-vaccination (Y) through the behavioural attitude (M) | |||||
| 0.187 | 0.046 | 0.095 | 0.279 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobierajski, T.; Bulińska-Stangrecka, H.; Wanke-Rytt, M.; Stefanoff, P.; Augustynowicz, E. Behavioural and Cognitive Attitudes of Paediatricians towards Influenza Self-Vaccination—Partial Mediation Model. Vaccines 2022, 10, 1206. https://doi.org/10.3390/vaccines10081206
Sobierajski T, Bulińska-Stangrecka H, Wanke-Rytt M, Stefanoff P, Augustynowicz E. Behavioural and Cognitive Attitudes of Paediatricians towards Influenza Self-Vaccination—Partial Mediation Model. Vaccines. 2022; 10(8):1206. https://doi.org/10.3390/vaccines10081206
Chicago/Turabian StyleSobierajski, Tomasz, Helena Bulińska-Stangrecka, Monika Wanke-Rytt, Paweł Stefanoff, and Ewa Augustynowicz. 2022. "Behavioural and Cognitive Attitudes of Paediatricians towards Influenza Self-Vaccination—Partial Mediation Model" Vaccines 10, no. 8: 1206. https://doi.org/10.3390/vaccines10081206
APA StyleSobierajski, T., Bulińska-Stangrecka, H., Wanke-Rytt, M., Stefanoff, P., & Augustynowicz, E. (2022). Behavioural and Cognitive Attitudes of Paediatricians towards Influenza Self-Vaccination—Partial Mediation Model. Vaccines, 10(8), 1206. https://doi.org/10.3390/vaccines10081206