
Promising Efficacy of a Third Dose of mRNA SARS-CoV-2 Vaccination in Patients Treated with Anti-CD20 Antibody Who Failed 2-Dose Vaccination

 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection and Measurement of Antibody Titers against S1 Protein
3. Results
3.1. Patient Characteristics
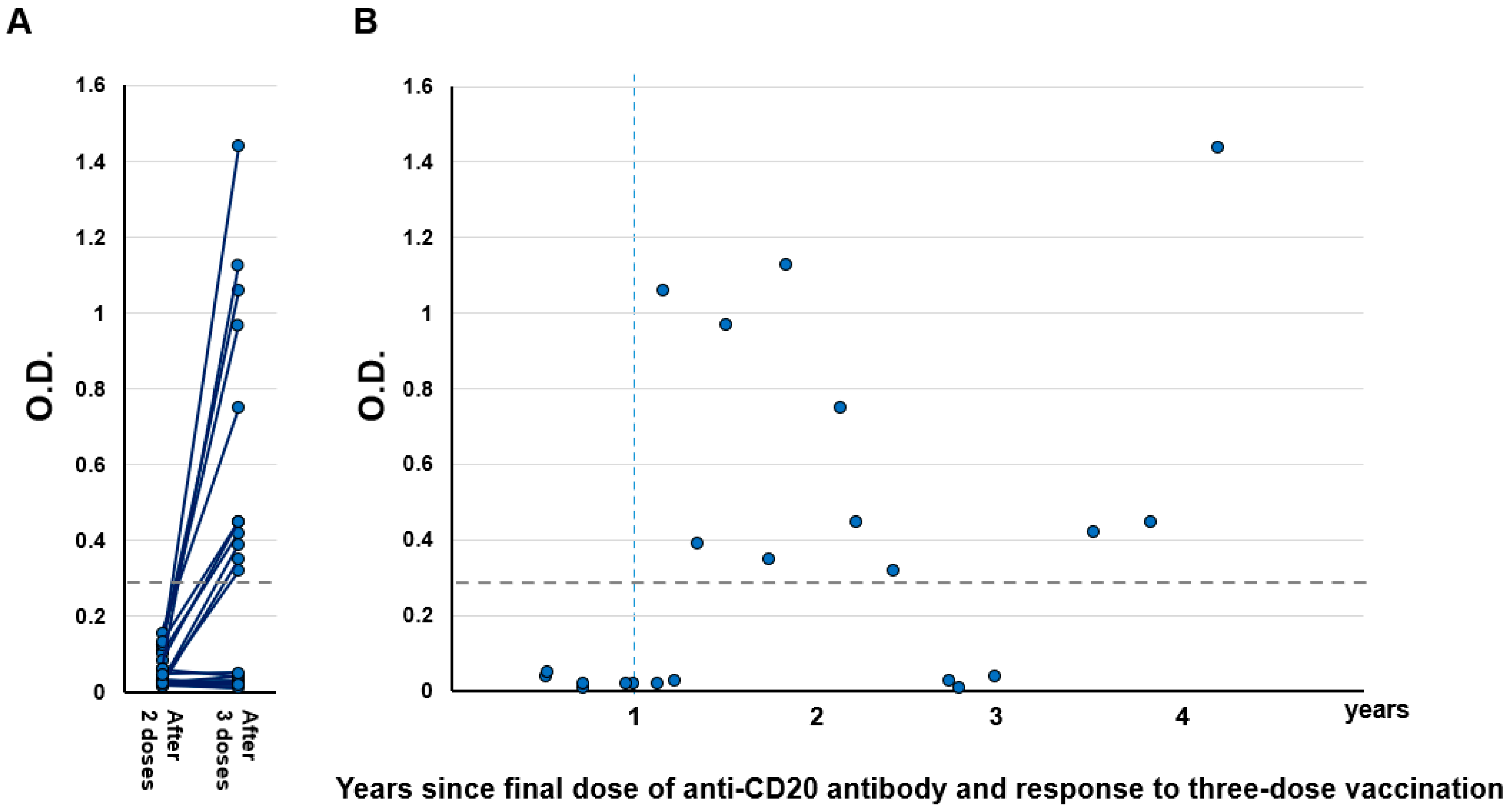
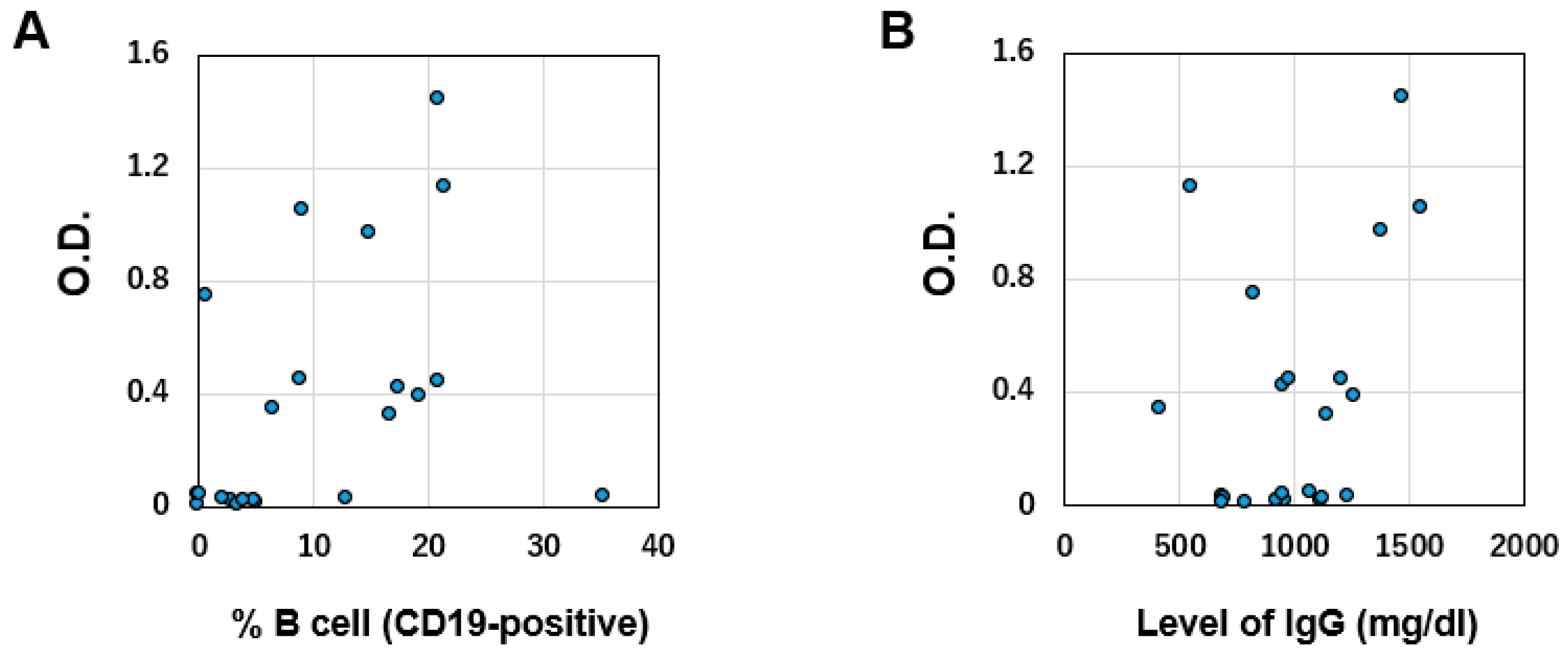
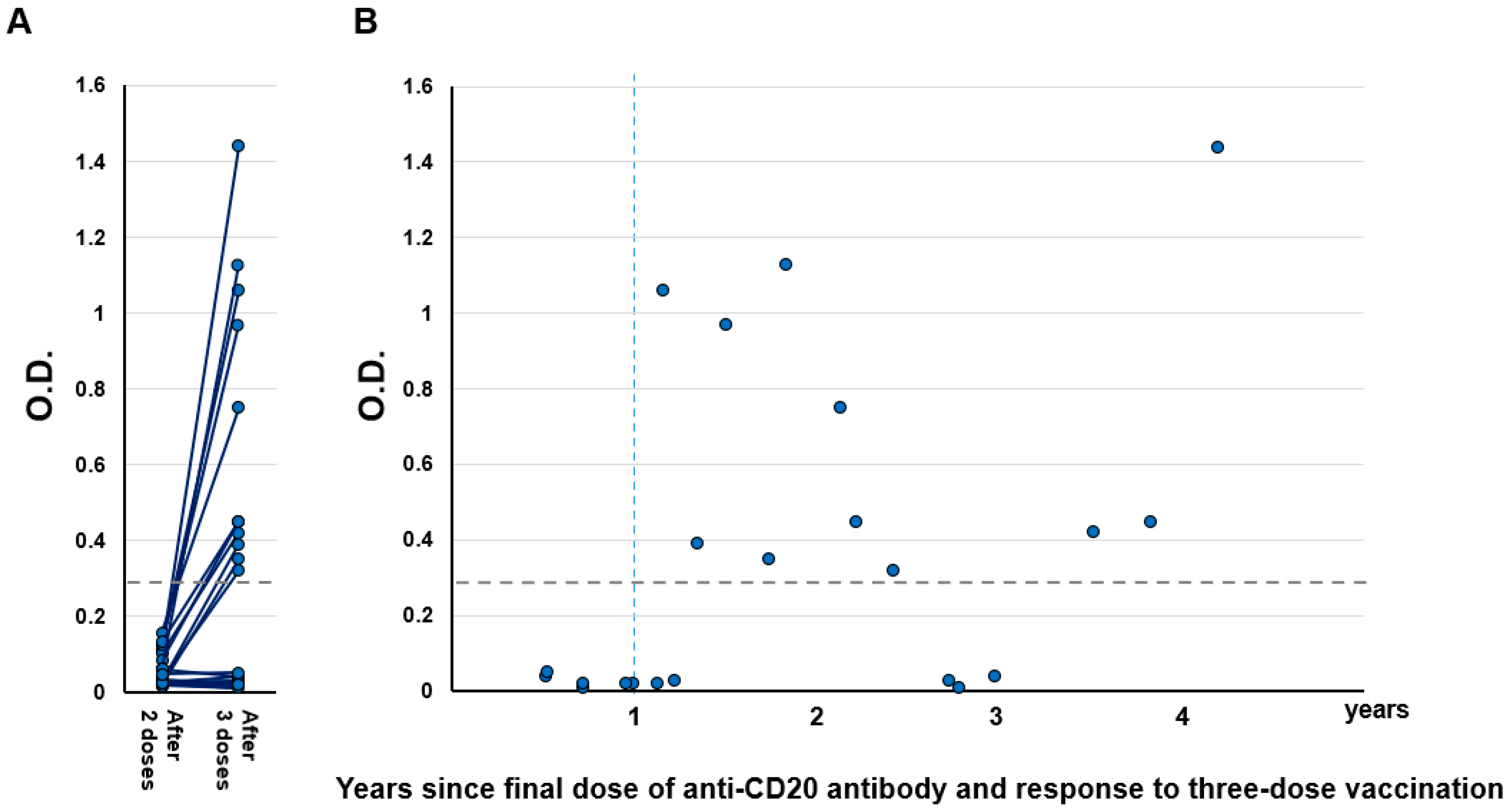
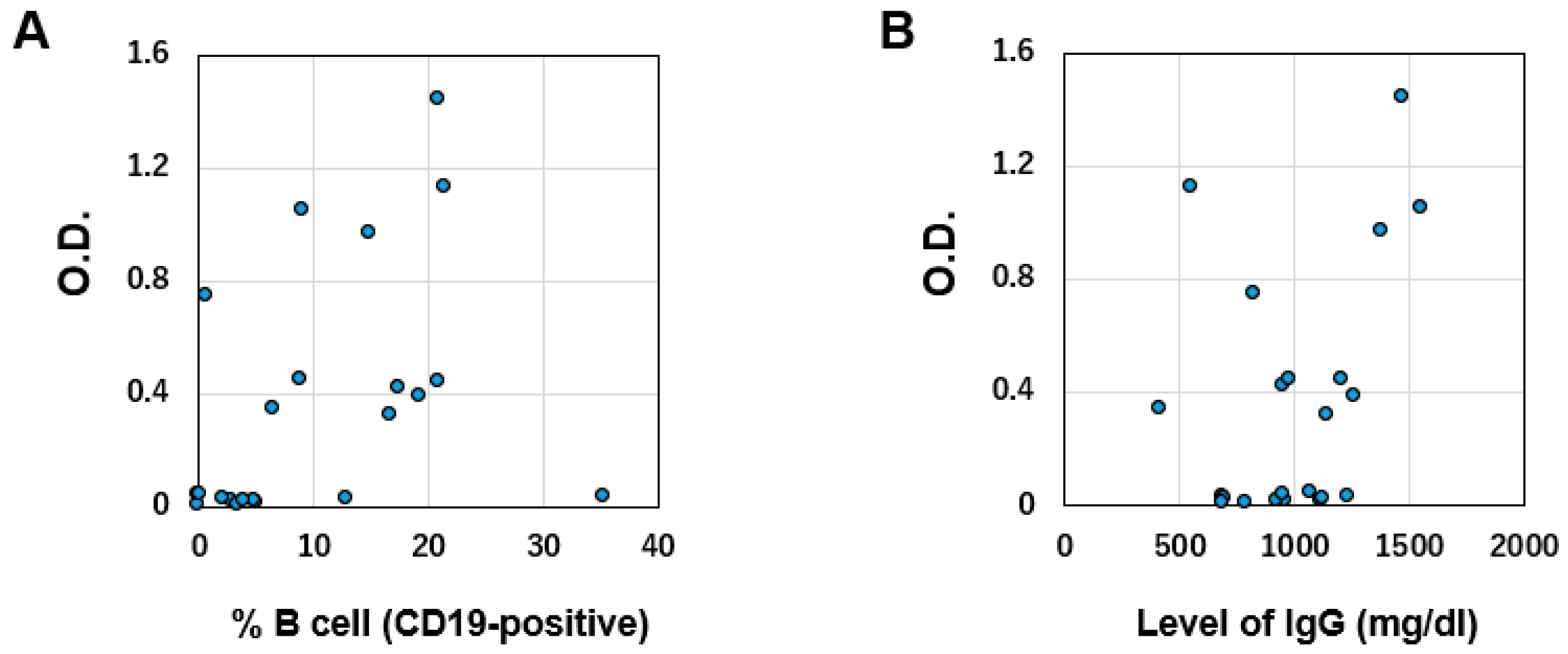
3.2. Serological Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tepasse, P.R.; Hafezi, W.; Lutz, M.; Kühn, J.; Wilms, C.; Wiewrodt, R.; Sackarnd, J.; Keller, M.; Schmidt, H.H.; Vollenberg, R. Persisting SARS-CoV-2 viraemia after rituximab therapy: Two cases with fatal outcome and a review of the literature. Br. J. Haematol. 2020, 190, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Guilpain, P.; Le Bihan, C.; Foulongne, V.; Taourel, P.; Pansu, N.; Maria, A.T.J.; Jung, B.; Larcher, R.; Klouche, K.; Le Moing, V. Rituximab for granulomatosis with polyangiitis in the pandemic of COVID-19: Lessons from a case with severe pneumonia. Ann. Rheum. Dis. 2021, 80, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze-Koops, H.; Krueger, K.; Vallbracht, I.; Hasseli, R.; Skapenko, A. Increased risk for severe COVID-19 in patients with inflammatory rheumatic diseases treated with rituximab. Ann. Rheum. Dis. 2020, 80, e67. [Google Scholar] [CrossRef] [PubMed]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, Y.; Yakushijin, K.; Ohji, G.; Hojo, W.; Sakai, H.; Watanabe, M.; Saeki, M.; Hirakawa, Y.; Sakai, R.; Matsumoto, S.; et al. Limited increase in antibody titers following mRNA SARS-CoV-2 vaccination for more than 3 years after final dose of anti-CD20 antibody. Int. J. Hematol. 2022, 115, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Herishanu, Y.; Rahav, G.; Levi, S.; Braester, A.; Itchaki, G.; Bairey, O.; Dally, N.; Shvidel, L.; Ziv-Baran, T.; Polliack, A.; et al. Efficacy of a third BNT162b2 mRNA COVID-19 vaccine dose in patients with CLL who failed standard 2-dose vaccination. Blood 2022, 139, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Tascilar, K.; Fagni, F.; Schmidt, K.; Krönke, G.; Kleyer, A.; Ramming, A.; Schoenau, V.; Bohr, D.; Knitza, J.; et al. Efficacy and safety of SARS-CoV-2 revaccination in non-responders with immune-mediated inflammatory disease. Ann. Rheum. Dis. 2021, 81, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Stuart, B.; Joseph-Pietras, D.; Johnson, M.; Campbell, N.; Kelly, A.; Jeffrey, D.; Turaj, A.H.; Rolfvondenbaumen, K.; Galloway, C.; et al. Immune responses against SARS-CoV-2 variants after two and three doses of vaccine in B-cell malignancies: UK PROSECO study. Nat. Cancer 2022, 3, 552–564. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Kitagawa, Y.; Tabata, S.; Kubota, K.; Nagura-Ikeda, M.; Matsuoka, M.; Miyoshi, K.; Sakai, J.; Ishibashi, N.; Tarumoto, N.; et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J. Med. Virol. 2021, 93, 3211–3218. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous Covid-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Tanne, J.H. COVID-19: Americans who are over 50 or immunocompromised are advised to have second booster. BMJ 2022, 376, o842. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, M.M.; Mrak, D.; Perkmann, T.; Haslacher, H.; Aletaha, D. SARS-CoV-2 vaccination in rituximab-treated patients: Evidence for impaired humoral but inducible cellular immune response. Ann. Rheum. Dis. 2021, 80, 1355–1356. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, A.; Fujigaki, H.; Iriyama, C.; Goto, N.; Yamamoto, H.; Mihara, K.; Inaguma, Y.; Miura, Y.; Furukawa, K.; Yamamoto, Y.; et al. CD19-positive lymphocyte count is critical for acquisition of anti-SARS-CoV-2 IgG after vaccination in B-cell lymphoma. Blood Adv. 2022, 6, 3230–3233. [Google Scholar] [CrossRef] [PubMed]
- Bayart, J.L.; Douxfils, J.; Gillot, C.; David, C.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Gerin, V.; et al. Waning of IgG, Total and Neutralizing Antibodies 6 Months Post-Vaccination with BNT162b2 in Healthcare Workers. Vaccines 2021, 9, 1092. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total | n = 22 |
|---|---|
| Median age (range, years) | 74 (57–86) |
| Sex | |
| Female | 8 |
| Male | 14 |
| Diagnosis | |
| DLBCL | 13 |
| FL | 6 |
| LPL/WM | 2 |
| MCL | 1 |
| Anti-CD20 antibody | |
| Rituximab-based | 21 |
| Obinutuzumab-based | 1 |
| Median course (range, courses) | 6 (3–20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Funakoshi, Y.; Yakushijin, K.; Ohji, G.; Hojo, W.; Sakai, H.; Watanabe, M.; Kitao, A.; Miyata, Y.; Saito, Y.; Kawamoto, S.; et al. Promising Efficacy of a Third Dose of mRNA SARS-CoV-2 Vaccination in Patients Treated with Anti-CD20 Antibody Who Failed 2-Dose Vaccination. Vaccines 2022, 10, 965. https://doi.org/10.3390/vaccines10060965
Funakoshi Y, Yakushijin K, Ohji G, Hojo W, Sakai H, Watanabe M, Kitao A, Miyata Y, Saito Y, Kawamoto S, et al. Promising Efficacy of a Third Dose of mRNA SARS-CoV-2 Vaccination in Patients Treated with Anti-CD20 Antibody Who Failed 2-Dose Vaccination. Vaccines. 2022; 10(6):965. https://doi.org/10.3390/vaccines10060965
Chicago/Turabian StyleFunakoshi, Yohei, Kimikazu Yakushijin, Goh Ohji, Wataru Hojo, Hironori Sakai, Marika Watanabe, Akihito Kitao, Yoshiharu Miyata, Yasuyuki Saito, Shinichiro Kawamoto, and et al. 2022. "Promising Efficacy of a Third Dose of mRNA SARS-CoV-2 Vaccination in Patients Treated with Anti-CD20 Antibody Who Failed 2-Dose Vaccination" Vaccines 10, no. 6: 965. https://doi.org/10.3390/vaccines10060965
APA StyleFunakoshi, Y., Yakushijin, K., Ohji, G., Hojo, W., Sakai, H., Watanabe, M., Kitao, A., Miyata, Y., Saito, Y., Kawamoto, S., Yamamoto, K., Ito, M., Koyama, T., Imamura, Y., Kiyota, N., Matsuoka, H., Mori, Y., & Minami, H. (2022). Promising Efficacy of a Third Dose of mRNA SARS-CoV-2 Vaccination in Patients Treated with Anti-CD20 Antibody Who Failed 2-Dose Vaccination. Vaccines, 10(6), 965. https://doi.org/10.3390/vaccines10060965