
COVID-19 Neutralizing Antibodies in Breast Milk of Mothers Vaccinated with Three Different Vaccines in Mexico



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Samples Collection and Preparation
2.3. Cell Culture and Viral Strain
2.4. SARS-CoV-2 Neutralization
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Neutralizing Antibodies Titer
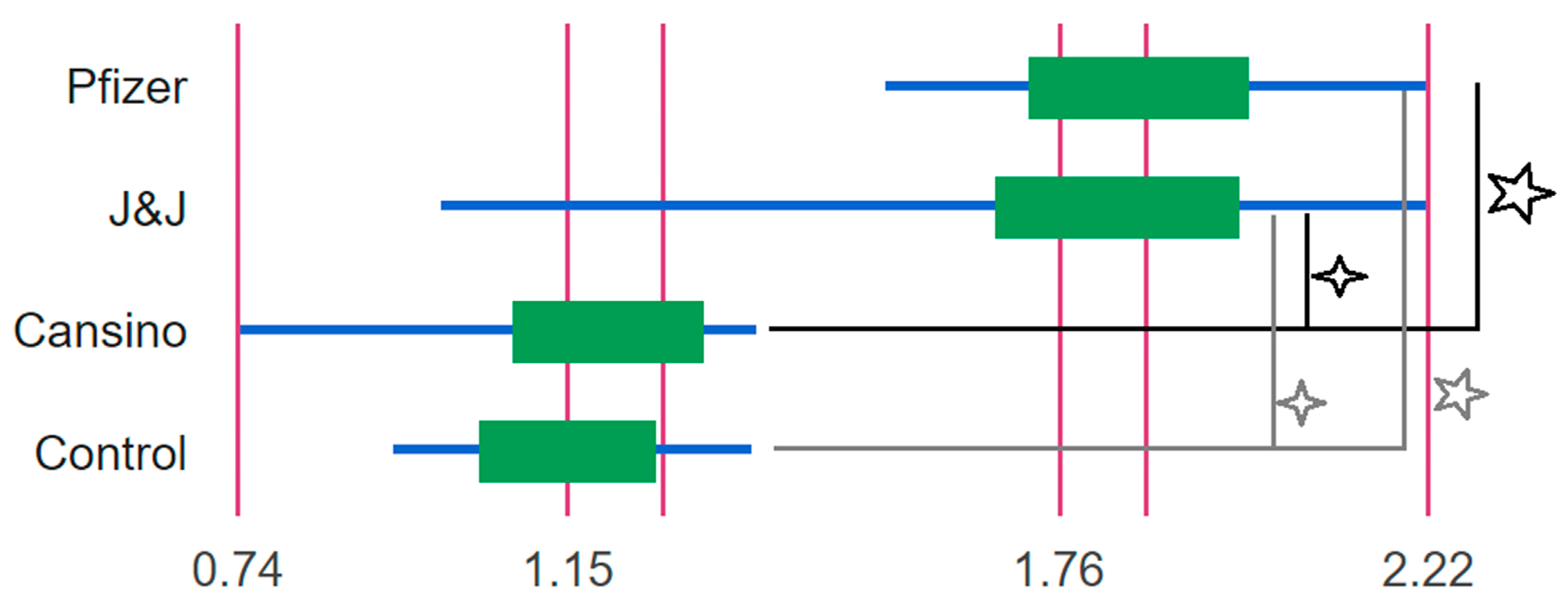
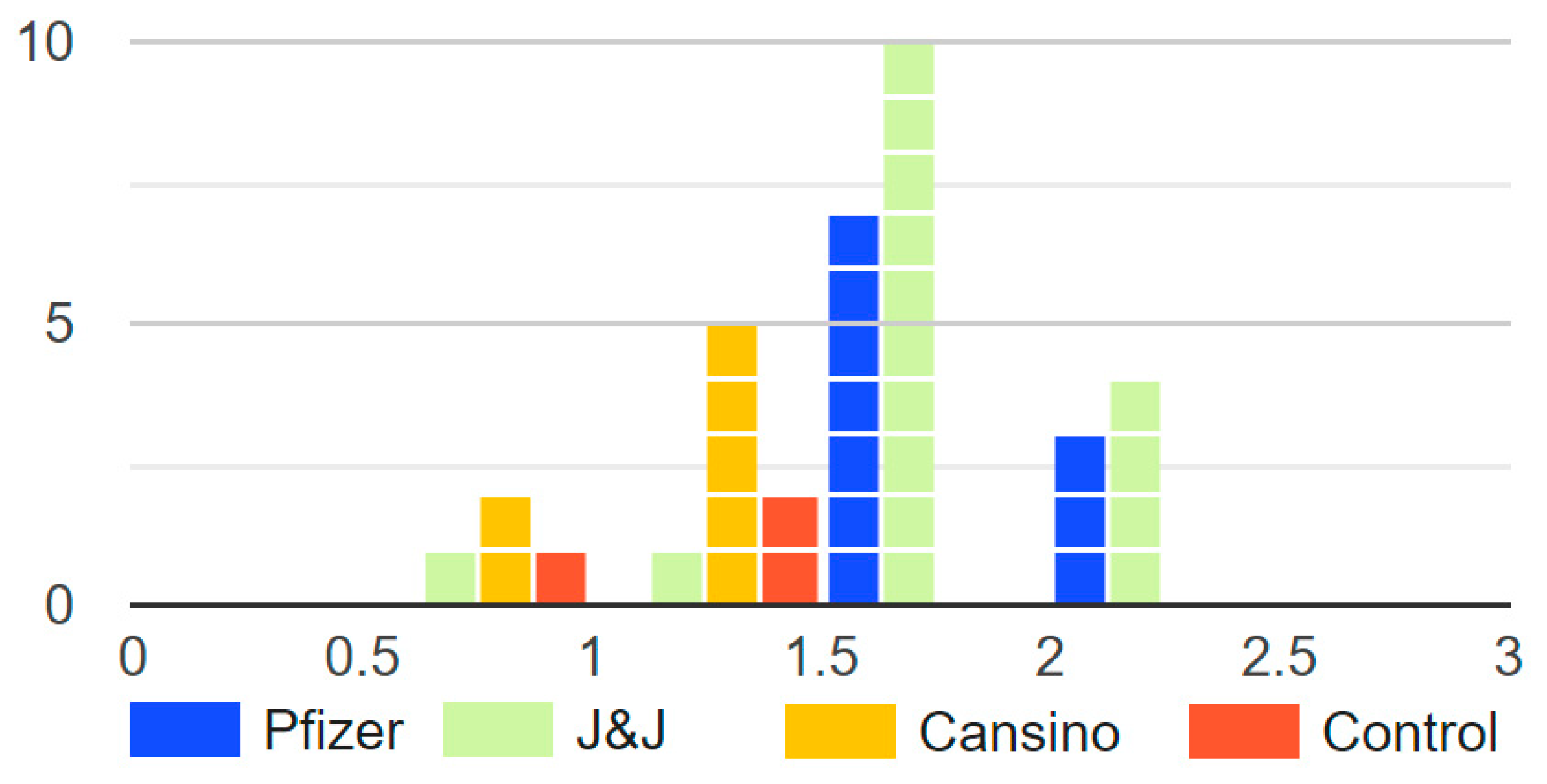
3.3. Statistics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Anderson, P.O. Maternal Vaccination and Breastfeeding. Breastfeed. Med. 2019, 14, 215–217. [Google Scholar] [CrossRef]
- Cabinian, A.; Sinsimer, D.; Tang, M.; Zumba, O.; Mehta, H.; Toma, A.; Sant’Angelo, D.; Laouar, Y.; Laouar, A. Transfer of Maternal Immune Cells by Breastfeeding: Maternal Cytotoxic T Lymphocytes Present in Breast Milk Localize in the Peyer’s Patches of the Nursed Infant. PLoS ONE 2016, 11, e0156762. [Google Scholar] [CrossRef]
- Adkins, B.; Leclerc, C.; Marshall-Clarke, S. Neonatal adaptive immunity comes of age. Nat. Rev. Immunol. 2004, 4, 553–564. [Google Scholar] [CrossRef]
- Van de Perre, P. Transfer of antibody via mother’s milk. Vaccine 2003, 21, 3374–3376. [Google Scholar] [CrossRef]
- Yan, H.; Lamm, M.E.; Björling, E.; Huang, Y.T. Multiple Functions of Immunoglobulin A in Mucosal Defense against Viruses: An in Vitro Measles Virus Model. J. Virol. 2002, 76, 10972–10979. [Google Scholar] [CrossRef] [PubMed]
- Schlaudecker, E.P.; Steinhoff, M.C.; Omer, S.B.; McNeal, M.M.; Roy, E.; Arifeen, S.E.; Dodd, C.N.; Raqib, R.; Breiman, R.F.; Zaman, K. IgA and Neutralizing Antibodies to Influenza A Virus in Human Milk: A Randomized Trial of Antenatal Influenza Immunization. PLoS ONE 2013, 8, e70867. [Google Scholar] [CrossRef] [PubMed]
- van Keulen, B.J.; Romijn, M.; Bondt, A.; van der Straten, K.; den Boer, M.A.; Bosch, B.J.; Brouwer, P.J.M.; de Groot, C.J.M.; Hoek, M.; Li, W.; et al. Human milk from previouslly COVID-19-infected mothers: The effect oof pasteurization on specific antibodies and neutralization capacity. Nutrients 2021, 13, 1645. [Google Scholar] [CrossRef] [PubMed]
- Baird, J.K.; Jensen, S.M.; Urba, W.J.; Fox, B.A.; Baird, J.R. SARS-CoV-2 antibodies detected in mother’s milk post-vaccination. J. Hum. Lact. 2021, 37, 492–498. [Google Scholar] [CrossRef]
- Charepe, N.; Gonçalves, J.; Juliano, A.M.; Lopes, D.G.; Canhão, H.; Soares, H.; Serrano, e.F. COVID-19 mRNA vaccine and antibody response in lactating women: A prospective cohort study. BMC Pregnancy Childbirth 2021, 21, 632. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef]
- Golan, Y.; Prahl, M.; Cassidy, A.G.; Gay, C.; Wu, A.H.B.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; Basilio, E.; Chidboy, M.A.; et al. COVID-19 mRNA Vaccination in Lactation: Assessment of Adverse Events and Vaccine Related Antibodies in Mother-Infant Dyads. Front. Immunol. 2021, 12, 777103. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2–Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013. [Google Scholar] [CrossRef]
- Kelly, J.C.; Carter, E.B.; Raghuraman, N.; Nolan, L.S.; Gong, Q.; Lewis, A.N.; Good, M. Anti–severe acute respiratory syndrome coronavirus 2 antibodies induced in breast milk after Pfizer-BioNTech/BNT162b2 vaccination. Am. J. Obstet. Gynecol. 2021, 225, 101–103. [Google Scholar] [CrossRef]
- Rosenberg-Friedman, M.; Kigel, A.; Bahar, Y.; Werbner, M.; Alter, J.; Yogev, Y.; Dror, Y.; Lubetzky, R.; Dessau, M.; Gal-Tanamy, M.; et al. BNT162b2 mRNA vaccine elicited antibody response in blood and milk of breastfeeding women. Nat. Commun. 2021, 12, 6222. [Google Scholar] [CrossRef]
- Calil, V.M.L.T.; Palmeira, P.; Zheng, Y.; Krebs, V.L.J.; de Carvalho, W.B.; Carneiro-Sampaio, M. CoronaVac can induce the production of anti-SARS-CoV-2 IgA antibodies in human milk. Clinics 2021, 76, e3185. [Google Scholar] [CrossRef] [PubMed]
- Alisa, F.; DeCarlo, C.; Yang, X.; Norris, C.; Powell, R. Comparative profiles of SARS-CoV-2 Spike-specific milk antibodies elicited by COVID-19 vaccines currently authorized in the USA. medRxiv 2020, 6, 1–13. [Google Scholar]
- Rumbo, M.; Chirdo, F.G.; Añón, M.C.; Fossati, C.A. Detection and characterization of antibodies specific to food antigens (gliadin, ovalbumin and β-lactoglobulin) in human serum, saliva, colostrum and milk. Clin. Exp. Immunol. 1998, 112, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Manenti, A.; Maggetti, M.; Casa, E.; Martinuzzi, D.; Torelli, A.; Trombetta, C.M.; Marchi, S.; Montomoli, E. Evaluation of SARS-CoV-2 neutralizing antibodies using a CPE-based colorimetric live virus micro-neutralization assay in human serum samples. J. Med. Virol. 2020, 92, 2096–2104. [Google Scholar] [CrossRef] [PubMed]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.W.; Lackey, K.A.; Gogel, A.C.; Nguyen-contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. Characterization of SARS-CoV-2 RNA, Antibodies, and Neutralizing Capacity in Milk Produced by Women with COVID-19. mBio 2021, 12, e03192-20. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Bello, J.; Morales-Núñez, J.J.; Machado-Sulbarán, A.C.; Díaz-Pérez, S.A.; Torres-Hernández, P.C.; Balcázar-Félix, P.; Gutiérrez-Brito, J.A.; Lomelí-Nieto, J.A.; Muñoz-Valle, J.F. Neutralizing Antibodies against SARS-CoV-2, Anti-Ad5 Antibodies, and Reactogenicity in Response to Ad5-nCoV (CanSino Biologics) Vaccine in Individuals with and without Prior SARS-CoV-2. Vaccines 2021, 9, 1047. [Google Scholar] [CrossRef]
- Guzmán-Martínez, O.; Guardado, K.; de Guevara, E.L.; Navarro, S.; Hernández, C.; Zenteno-Cuevas, R.; Montero, H. IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population. Vaccines 2021, 9, 999. [Google Scholar] [CrossRef]
- WHO. Global Strategy for Infant and Ypung ChildFeeding, 1st ed.; Brundtland, G., Bellamy, C., Eds.; World Health Organization: Geneva, Switzerland, 2003; Volume 3.
- Jones, T.D.; Carter, P.J.; Pl, A.; Max, V.; Holgate, R.G.E.; Isidro, H.; Popplewell, A.G.; Parren, P.W.H.I.; Enzelberger, M.; Rademaker, H.J.; et al. The INNs and outs of antibody nonproprietary names. MAbs 2016, 8, 1–9. [Google Scholar] [CrossRef]
- Christensen, N.; Bruun, S.; Søndergaard, J.; Christesen, H.T.; Fisker, N.; Zachariassen, G.; Sangild, P.T.; Husby, S. Breastfeeding and Infections in Early Childhood: A Cohort Study. Pediatrics 2020, 146, e20191892. [Google Scholar] [CrossRef]
- Kleist, S.A.; Knoop, K.A. Understanding the Elements of Maternal Protection from Systemic Bacterial Infections during Early Life. Nutrients 2020, 12, 1045. [Google Scholar] [CrossRef]
- Zdanowski, W.; Waśniewski, T. Evaluation of SARS-CoV-2 Spike Protein Antibody Titers in Cord Blood after COVID-19 Vaccination during Pregnancy in Polish Healthcare Workers: Preliminary Results. Vaccines 2021, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Pratama, N.R.; Wafa, I.A.; Budi, D.S.; Putra, M.; Wardhana, M.P.; Wungu, C.D.K. mRNA COVID-19 vaccines in pregnancy: A systematic review. PLoS ONE 2022, 17, e0261350. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample | Neutralizing Antibodies Titer | COVID-19 Positive Diagnostic | |||
|---|---|---|---|---|---|
| Vaccine | |||||
| No Vaccine | Pfizer | J&J | CanSino | ||
| M1 | 80 | ||||
| M2 | 20 | ||||
| M3 | 10 | ||||
| M4 | 20 | ||||
| M5 | 10 | ||||
| M6 | 20 | + | |||
| M7 | 20 | ||||
| M8 | 80 | ||||
| M9 | 20 | ||||
| M10 | 10 | ||||
| M11 | 20 | ||||
| M12 | 20 | ||||
| M13 | 40 | + | |||
| M14 | 40 | ||||
| M15 | 40 | ||||
| M16 | 40 | + | |||
| M17 | 80 | ||||
| M18 | 160 | ||||
| M19 | 80 | + | |||
| M20 | 80 | + | |||
| M21 | 20 | ||||
| M22 | 80 | ||||
| M23 | 40 | ||||
| M24 | 40 | ||||
| M25 | 20 | ||||
| M26 | 80 | ||||
| M27 | 40 | ||||
| M28 | 40 | ||||
| M29 | 40 | + | |||
| M30 | 20 | + | |||
| M31 | 40 | ||||
| M32 | 80 | + | |||
| M33 | 40 | ||||
| M34 | 20 | ||||
| M35 | 20 | ||||
| M36 | 20 | ||||
| M37 | 20 | ||||
| M38 | 20 | ||||
| Mean | 20 | 63 | 39 | 21 | |
| % Samples with NAbs | 73% | 65% | 14% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabanillas-Bernal, O.; Cervantes-Luevano, K.; Flores-Acosta, G.I.; Bernáldez-Sarabia, J.; Licea-Navarro, A.F. COVID-19 Neutralizing Antibodies in Breast Milk of Mothers Vaccinated with Three Different Vaccines in Mexico. Vaccines 2022, 10, 629. https://doi.org/10.3390/vaccines10040629
Cabanillas-Bernal O, Cervantes-Luevano K, Flores-Acosta GI, Bernáldez-Sarabia J, Licea-Navarro AF. COVID-19 Neutralizing Antibodies in Breast Milk of Mothers Vaccinated with Three Different Vaccines in Mexico. Vaccines. 2022; 10(4):629. https://doi.org/10.3390/vaccines10040629
Chicago/Turabian StyleCabanillas-Bernal, Olivia, Karla Cervantes-Luevano, Gonzalo Isai Flores-Acosta, Johanna Bernáldez-Sarabia, and Alexei F. Licea-Navarro. 2022. "COVID-19 Neutralizing Antibodies in Breast Milk of Mothers Vaccinated with Three Different Vaccines in Mexico" Vaccines 10, no. 4: 629. https://doi.org/10.3390/vaccines10040629
APA StyleCabanillas-Bernal, O., Cervantes-Luevano, K., Flores-Acosta, G. I., Bernáldez-Sarabia, J., & Licea-Navarro, A. F. (2022). COVID-19 Neutralizing Antibodies in Breast Milk of Mothers Vaccinated with Three Different Vaccines in Mexico. Vaccines, 10(4), 629. https://doi.org/10.3390/vaccines10040629