
Detection of Anti-SARS-CoV-2-S1 RBD-Specific Antibodies Prior to and during the Pandemic in 2011–2021 and COVID-19 Observational Study in 2019–2021

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
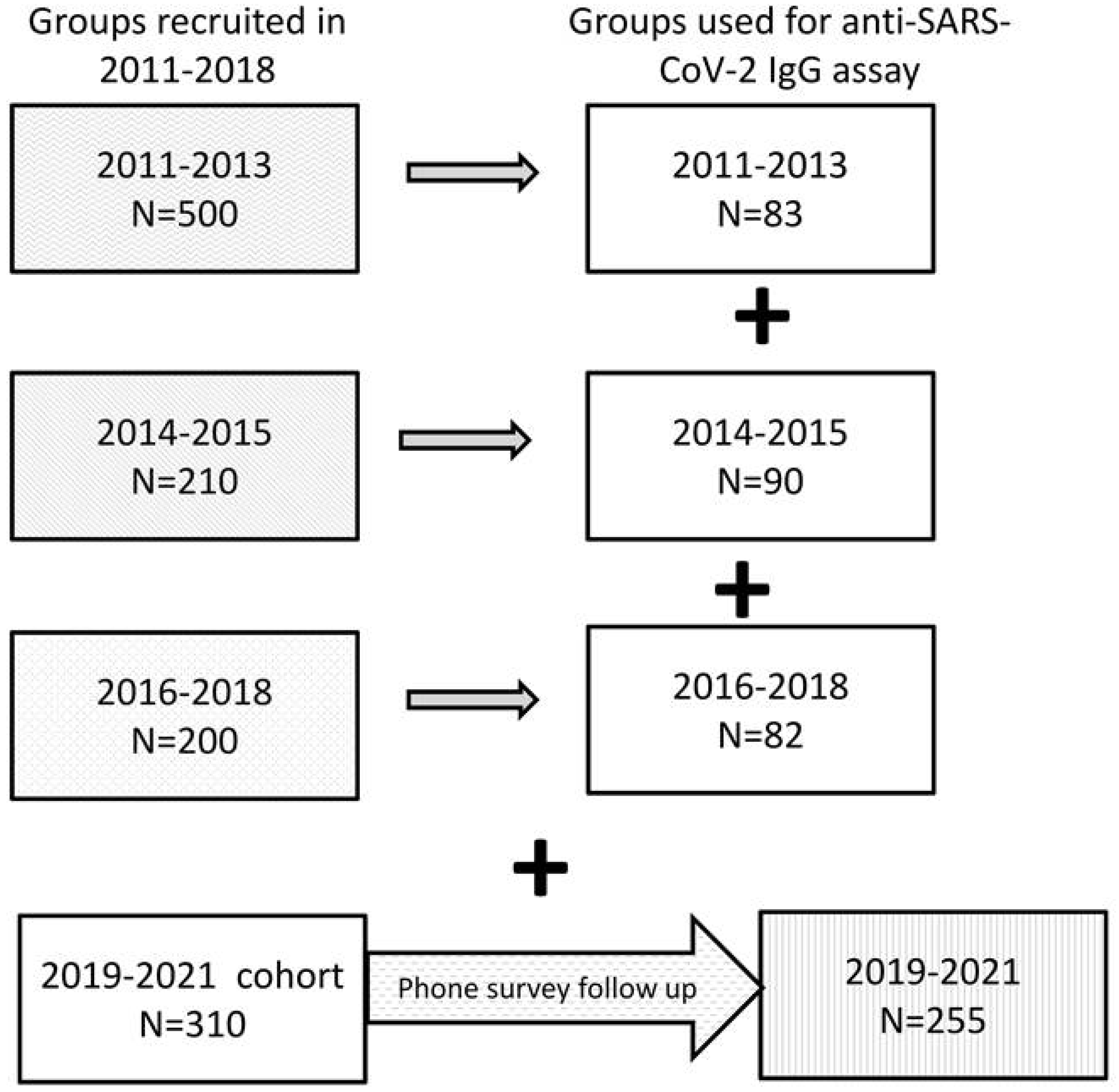
2.1. Participants
2.2. Antibody Assays
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peiris, J.; Lai, S.T.; Poon, L.; Guan, Y.; Yam, L.; Lim, W.; Nicholls, J.; Yee, W.; Yan, W.; Cheung, M.; et al. SARS study group. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 2003, 361, 1319–1325. [Google Scholar] [CrossRef] [Green Version]
- Ramshaw, R.E.; Letourneau, I.D.; Hong, A.Y.; Hon, J.; Morgan, J.D.; Osborne, C.P.; Shirude, S.; Van Kerkhove, M.D.; Hay, S.I.; Pigott, D.M. A database of geopositioned Middle East Respiratory Syndrome Coronavirus occurrences. Sci. Data 2019, 6, 318. [Google Scholar] [CrossRef] [Green Version]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Grifoni, A.; Sidney, J.; Zhang, Y.; Scheuermann, R.; Peters, B.; Setteet, A. A Sequence Homology and Bioinformatic Approach Can Predict Candidate Targets for Immune Responses to SARS-CoV-2 2020. Cell Host Microbe 2020, 27, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Galipeau, Y.; Greig, M.; Liu, G.; Driedger, M.; Langlois, M.-A. Humoral Responses and Serological Assays in SARS-CoV-2 Infections. Front. Immunol. 2020, 11, 610688. [Google Scholar] [CrossRef] [PubMed]
- Chia, W.; Tan, W.; Foo, R.; Kang, A.; Peng, Y.; Sivalingam, V.; Tiu, C.; Ong, X.-M.; Zhu, F.; Young, B.; et al. Serological differentiation between COVID-19 and SARS infections. Emerg. Microbes Infect. 2020, 9, 1497–1505. [Google Scholar] [CrossRef] [PubMed]
- Mateus, J.; Grifoni, A.; Tarke, A.; Sidney, J.; Ramirez, S.; Dan, J.; Burger, Z.; Rawlings, S.; Smith, D.; Phillips, E.; et al. Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans. Science 2020, 370, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.; Riahi, S.; Shiadeh, M.; Esfandyari, S.; Mokdad, H.; Hotez, P.; Gasser, R. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Montomoli, E.; Manenti, A.; Boeri, M.; Sabia, F.; Hyseni, I.; Mazzini, L.; Martinuzzi, D.; Cantone, L.; Milanese, G.; et al. Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy. Tumori J. 2021, 107, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C. Unexpected volume of Google searches for COVID-19 symptoms in the prepandemic period in Lombardia, Italy. Tumori J. 2021, 107, 468–469. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Faulkner, N.; Cornish, G. Preexisting and de novo humoral immunity to SARS-CoV-2 in humans. Science 2020, 370, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Pre-existing immunity to SARS-CoV-2: The knowns and unknowns. Nat. Rev. Immunol. 2020, 7, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Palermo, A.; Salvarani, C.; Sarti, M.; Boaretto, G.; Manni, L.; Mascia, M. Comments on: “Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy”. Tumori J. 2021, 107, 470–471. [Google Scholar] [CrossRef] [PubMed]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brigger, D.; Horn, M.; Pennington, L.F.; Powell, A.E.; Siegrist, D.; Weber, B.; Engler, O.; Piezzi, V.; Damonti, L.; Iseli, P.; et al. Accuracy of serological testing for SARS-CoV-2 antibodies: First results of a large mixed-method evaluation study. Allergy 2021, 76, 853–865. [Google Scholar] [CrossRef] [PubMed]
- León, T.M.; Dorabawila, V.; Nelson, L.; Lutterloh, E.; Bauer, U.; Backenson, B.; Bassett, M.; Henry, H.; Bregman, B.; Midgley, C.M.; et al. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis—California and New York, May–November 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Bradley, V.C.; Kuriwaki, S.; Isakov, M.; Sejdinovic, D.; Meng, X.L.; Flaxman, S. Unrepresentative big surveys significantly overestimated US vaccine uptake. Nature 2021, 600, 695–700. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
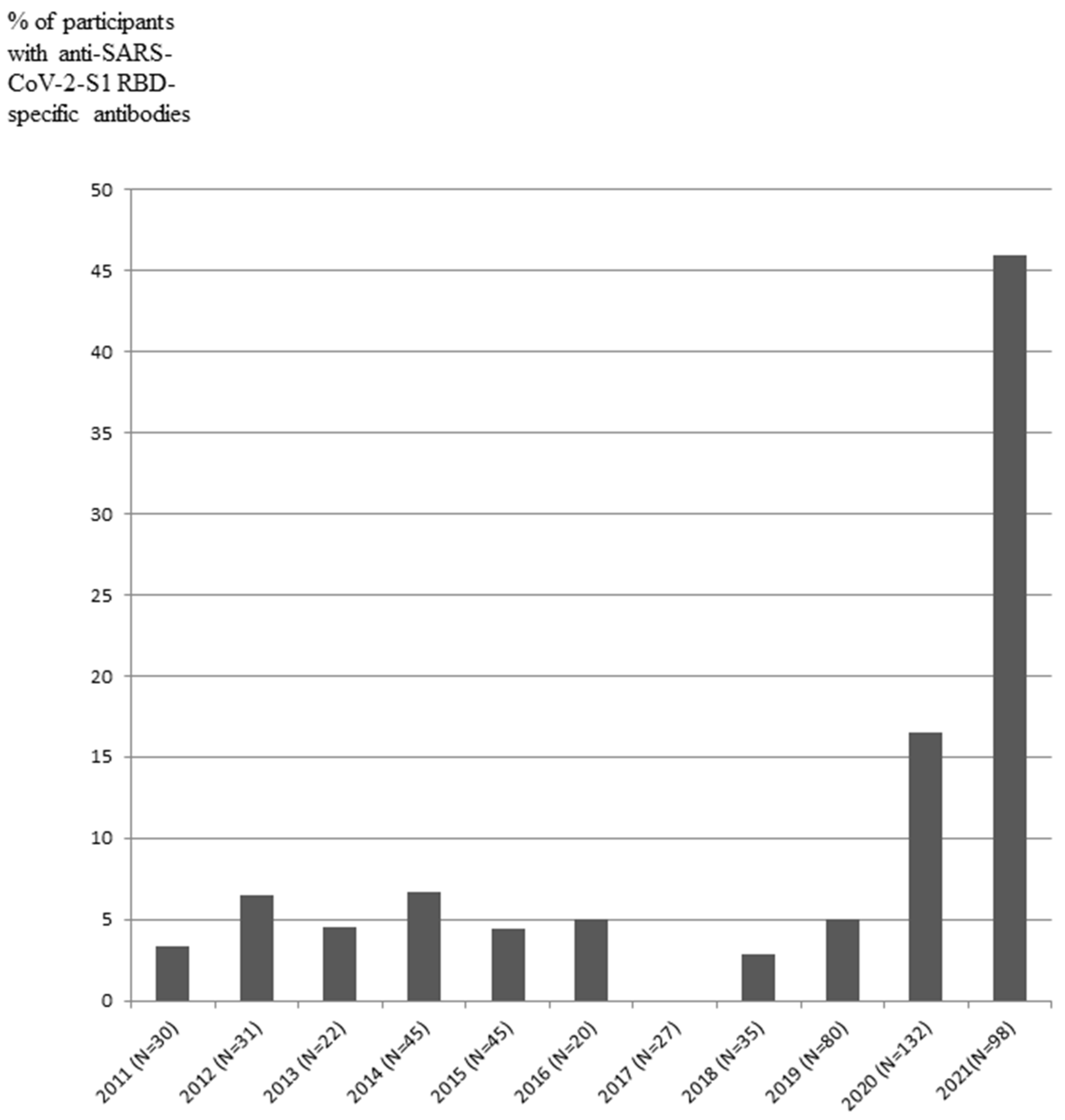
| Year-Based Groups | Total N and Age (Mean ± SD) | Year | N for Indicated Years | Serum Anti-SARS-CoV-2 (S1-RBD) IgG Antibody-Positive (N; %) |
|---|---|---|---|---|
| 2011–2013 | 83; 61.2 ± 9.4 | 2011 | 30 | 1 (3.3) |
| 2012 | 31 | 2 (6.5) | ||
| 2013 | 22 | 1 (4.5) | ||
| 2014–2015 | 90; 53.6 ± 7.4 | 2014 | 45 | 3 (6.7) |
| 2015 | 45 | 2 (4.4) | ||
| 2016–2018 | 82; 58.1 ± 11.1 | 2016 | 20 | 1 (5.0) |
| 2017 | 27 | 0 (0.0) | ||
| 2018 | 35 | 1 (2.9) | ||
| 2019–2021 | 310; 42 ± 8.7 | 2019 (from August to December) | 80 | 4 (5.0) |
| 2020 | 132 | 22 (16.5) | ||
| 2021 (from January 2021 to August 2021) | 98 | 45 (45.9) |
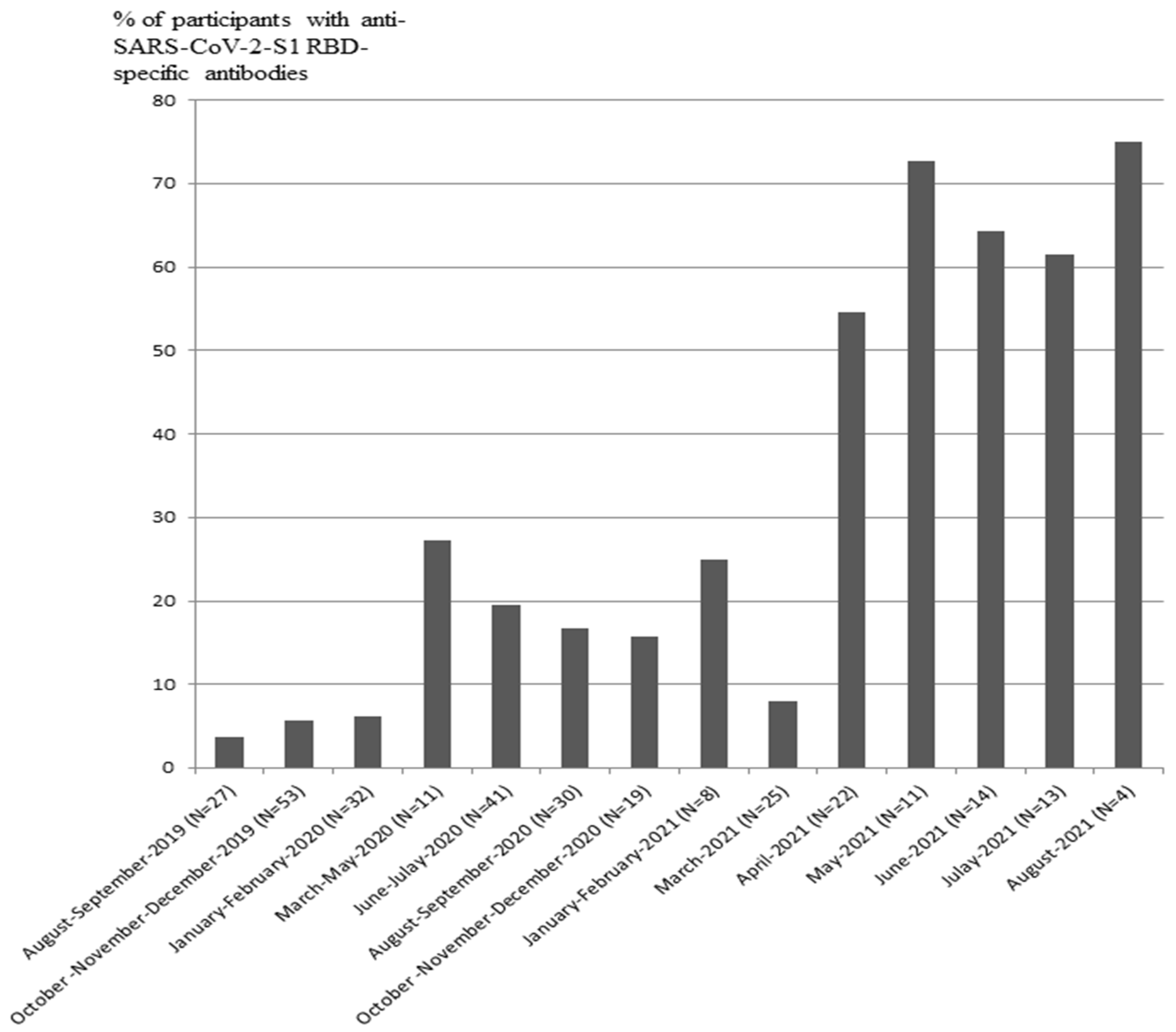
| Months | Participants (N) | Participants with Serum Anti-SARS-CoV-2-S1 IgG-Positive Status (%) |
|---|---|---|
| August–September 2019 | 27 | 3.7 |
| October–December 2019 | 53 | 5.7 |
| January–February 2020 | 32 | 6.3 |
| March–May 2020 | 11 | 27.3 |
| June–July 2020 | 41 | 19.5 |
| August–September 2020 | 30 | 16.7 |
| October–December 2020 | 19 | 15.8 |
| January–February 2021 | 8 | 25.0 |
| March 2021 | 25 | 8.0 |
| April 2021 | 22 | 54.5 |
| May 2021 | 11 | 72.7 |
| June 2021 | 14 | 64.3 |
| July 2021 | 13 | 61.5 |
| August 2021 | 4 | 75 |
| Description of Participants/Respondents | Respondents/Total Participants or Respondents (N/N; %) | IgG-Positive Respondents (N/N; %) | IgG-Negative Respondents (N/N; %) |
|---|---|---|---|
| Participants | |||
| All participants, 2019–2021 | 310 (100) | 70/310 (22.5) | 240/310 (77.5) |
| Available for phone survey | 251/310 (81) | ||
| Agreed to answer (respondents) | 238/310 (77) | 59/310 (19) | 179/310 (58) |
| Refused to answer | 13/310 (4) | ||
| Unavailable for phone survey | 59/310 (19) | ||
| Respondents | |||
| Symptoms and severity of respiratory disorders | 238 (100) | ||
| Any symptoms reported | 93/238 (39) | 30/59 (37) | 63/179 (35) |
| No symptoms reported | 145/238 (61) | 40/59 (63) | 105/179 (65) |
| COVID-19 verified by PCR | 85/93 (91) | 30/93 (32) | 55/93 (59) |
| Severity of respiratory disorders | |||
| Mild | 44/93 (47) | 15/30 (50) | 28/63 (44) |
| Medium (cough, cold, and fever) | 38/93 (41) | 12/30(40) | 26/63 (41) |
| Severe (hospitalization) | 11/93 (12) | 3/30 (10) | 9/63 (14) |
| Vaccination status | 238 (100) | 59 (100) | 179 (100) |
| Vaccinated (from September 2020 to October 2021) | 137/238 (58) | 33/59 (56) | 104/179 (58) |
| Not vaccinated | 97/238 (40) | 25/59 (42) | 72/179 (40) |
| Cannot answer | 4/238 (2) | 1/59 (2) | 3/179 (2) |
| Brand of vaccine in respondents who were able to answer | 119 (100) | ||
| Gam-COVID-Vac (Sputnik V) | 103/119 (87) | ||
| Other vaccines: | 16/119 (13) | ||
| CoviVac | 7/119 (6) | ||
| EpiVacCorona | 5/119 (4) | ||
| Sputnik Lite | 4/119 (3) | ||
| Vaccinated before enrolment, IgG-status (Gam-COVID-Vac, N = 13; CoviVac, N = 1) | 14/238 (6) | 9/14 (64) | 5/14 (36) |
| Days from vaccination to the enrollment visit | 9–151 * | 117–169 * | |
| COVID-19 disease status | 238 (100) | 59 (100) | 179 (100) |
| COVID-19 verified with PCR-tests | 94/238 (40) | 27/59 (46) | 66/179 (37) |
| Not verified | 144/238 (60) | 31/59 (54) | 113/179 (63) |
| IgG-positive respondents who were able to recall the date of respiratory disorders | 59 (100) | ||
| Reported a relapse of respiratory disorders after the enrollment visit during 10–629 days of follow-up | 12/59 (20) ** | ||
| Reported a respiratory disorder before the enrollment visit during 27–476 of days follow-up | 21/59 (36) | ||
| COVID-19 verified by PCR-tests | 16/21(76) | ||
| No respiratory disorders reported | 26/59 (44) | ||
| Asymptomatic | 2/21 (10) | ||
| Mild | 10/21(48) | ||
| Medium (cough, cold, and fever) | 8/21 (38) | ||
| Severe (hospitalization) | 1/21 (5) | ||
| Severity grade of respiratory disorders after the enrollment visit in IgG -positive respondents who were able to answer | 12 (100) | ||
| COVID-19 verified by PCR-tests | 12/12 (100) | ||
| Asymptomatic | 1/12(8) | ||
| Mild | 6/12 (50) | ||
| Medium (cough, cold, and fever) | 4/12 (33) | ||
| Severe (hospitalization) | 1/12 (8) | ||
| All vaccinated respondents | 137 (100) | ||
| Vaccinated respondents who were able to recall the date of respiratory disorders | 118/137 (86) | ||
| Respondents with reported respiratory disorders before vaccination | 39/118 (33) | ||
| Respondents with reported relapse of COVID-19 in vaccinated subjects verified by PCR-tests (from 92 to 183 days after the vaccination; mean 152 days) | 3/79 (4) ** | 1/3 (33.3) | 2/3 (66.7) |
| Severity grade of relapse respiratory disorders in vaccinated respondents | |||
| Mild | 2/79 (3) | ||
| Medium (cough, cold, and fever) | 1/79 (1) | ||
| Severe (hospitalization) | - | ||
| Groups | Vaccinated | IgG-Positive | Not Vaccinated | IgG-Negative | ||||
|---|---|---|---|---|---|---|---|---|
| Chi Squared Test | p | Chi Squared Test | p | Chi Squared Test | p | Chi Squared Test | p | |
| Vaccinated | 20.75 | 0.001 | 51.20 | 0.001 | 20.93 | 0.001 | ||
| IgG-positive | 20.75 | 0.001 | 1.59 | 0.21 | 1.31 | 0.25 | ||
| Not vaccinated | 51.20 | 0.001 | 1.59 | 0.21 | 19.74 | 0.001 | ||
| IgG-negative | 20.93 | 0.001 | 1.30 | 0.25 | 19.73 | 0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gumanova, N.G.; Gorshkov, A.U.; Bogdanova, N.L.; Korolev, A.I.; Drapkina, O.M. Detection of Anti-SARS-CoV-2-S1 RBD-Specific Antibodies Prior to and during the Pandemic in 2011–2021 and COVID-19 Observational Study in 2019–2021. Vaccines 2022, 10, 581. https://doi.org/10.3390/vaccines10040581
Gumanova NG, Gorshkov AU, Bogdanova NL, Korolev AI, Drapkina OM. Detection of Anti-SARS-CoV-2-S1 RBD-Specific Antibodies Prior to and during the Pandemic in 2011–2021 and COVID-19 Observational Study in 2019–2021. Vaccines. 2022; 10(4):581. https://doi.org/10.3390/vaccines10040581
Chicago/Turabian StyleGumanova, Nadezhda G., Alexander U. Gorshkov, Natalya L. Bogdanova, Andrew I. Korolev, and Oxana M. Drapkina. 2022. "Detection of Anti-SARS-CoV-2-S1 RBD-Specific Antibodies Prior to and during the Pandemic in 2011–2021 and COVID-19 Observational Study in 2019–2021" Vaccines 10, no. 4: 581. https://doi.org/10.3390/vaccines10040581
APA StyleGumanova, N. G., Gorshkov, A. U., Bogdanova, N. L., Korolev, A. I., & Drapkina, O. M. (2022). Detection of Anti-SARS-CoV-2-S1 RBD-Specific Antibodies Prior to and during the Pandemic in 2011–2021 and COVID-19 Observational Study in 2019–2021. Vaccines, 10(4), 581. https://doi.org/10.3390/vaccines10040581