
Influenza Vaccination Effectiveness in Paediatric ‘Healthy’ Patients: A Population-Based Study in Italy

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Cohort Selection
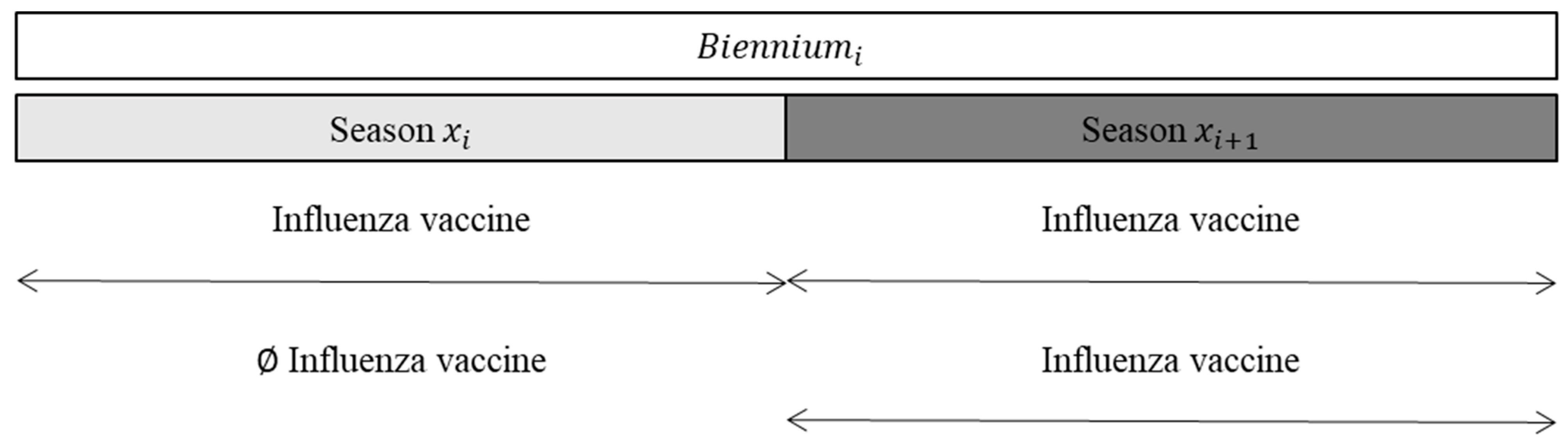
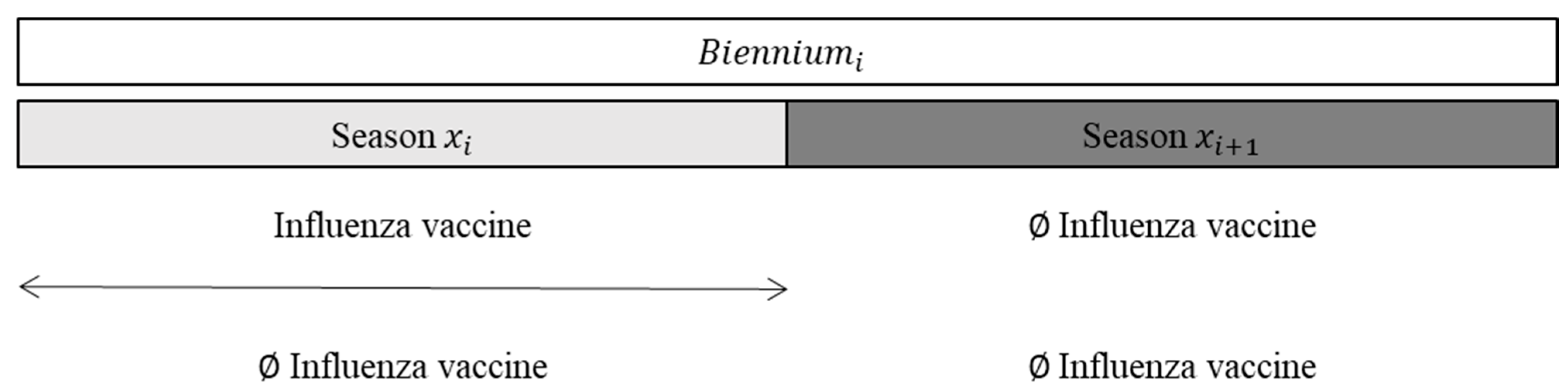
2.3. Exposure to Influenza Vaccine
2.4. Outcome
2.5. Covariates
2.6. Statistical Analysis
2.7. Sensitivity Analysis
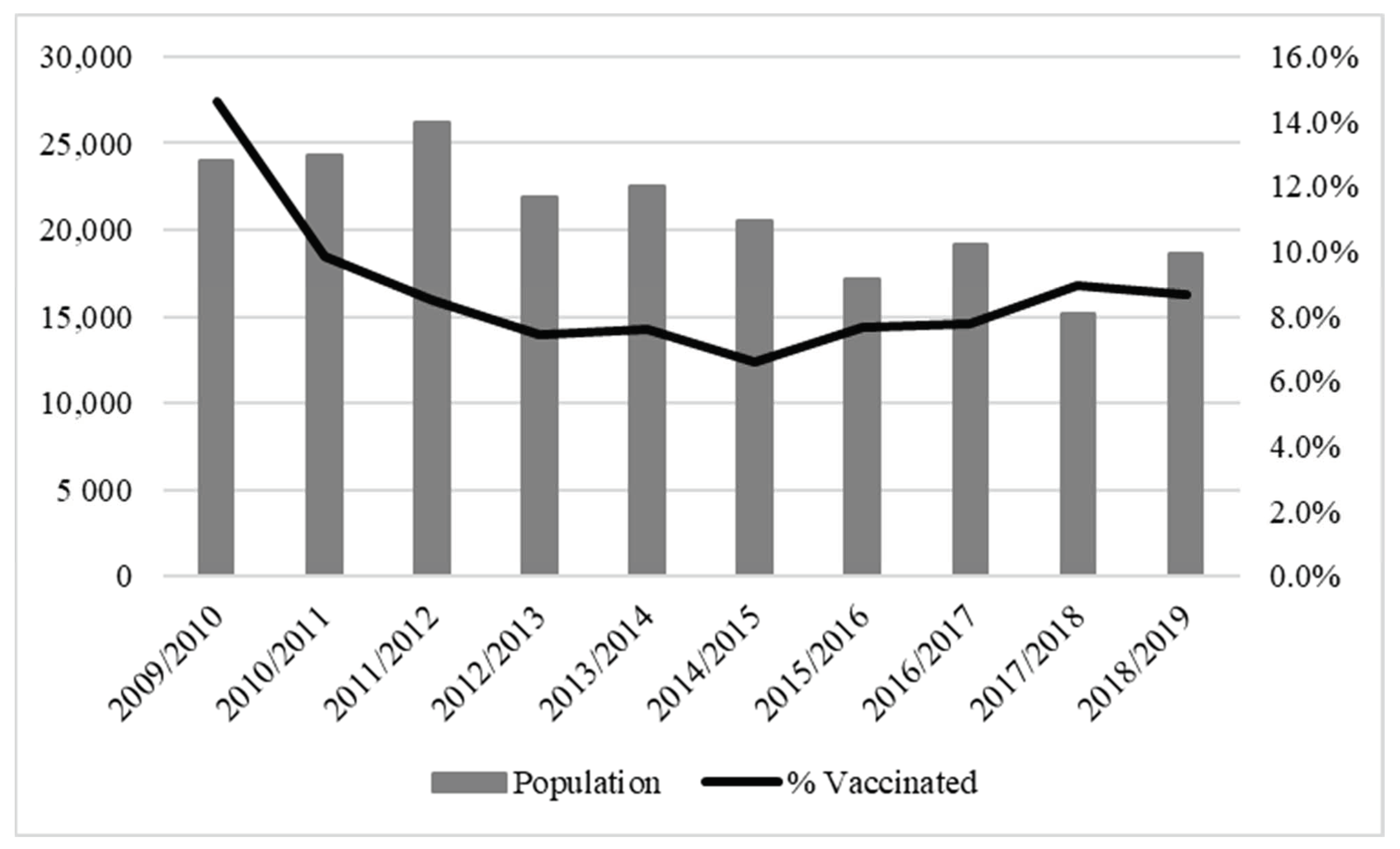
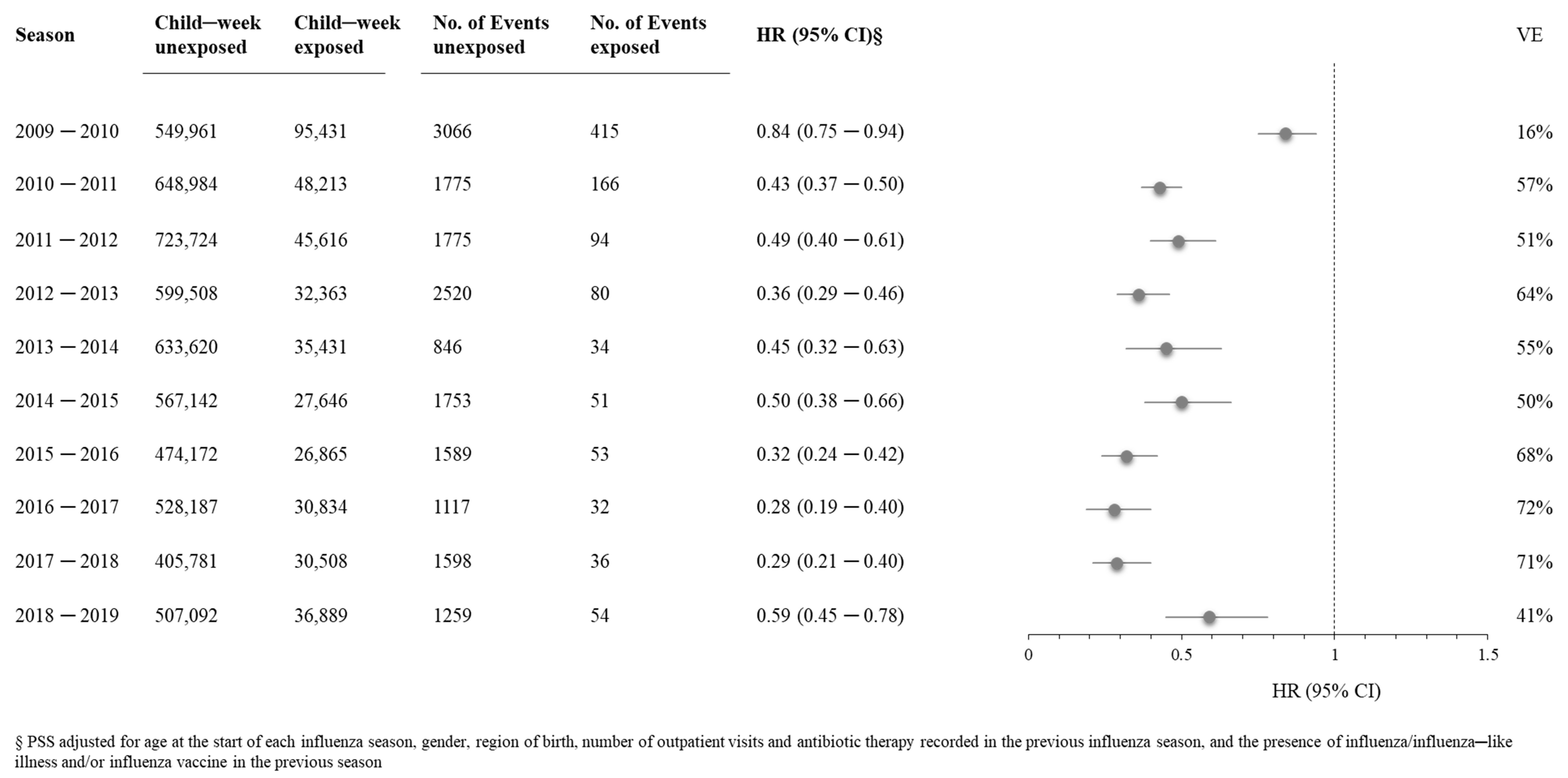
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grohskopf, L.A.; Sokolow, L.Z.; Broder, K.R.; Walter, E.B.; Bresee, J.S.; Fry, A.M.; Jernigan, D.B. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices-United States, 2017–2018 Influenza Season. MMWR Recomm. Rep. 2017, 66, 2970–2982. [Google Scholar] [CrossRef] [PubMed]
- Molinari, N.-A.M.; Ortega-Sanchez, I.R.; Messonnier, M.L.; Thompson, W.W.; Wortley, P.M.; Weintraub, E.; Bridges, C.B. The annual impact of seasonal influenza in the US: Measuring disease burden and costs. Vaccine 2007, 25, 5086–5096. [Google Scholar] [CrossRef] [PubMed]
- Keane, V.A.; Hudson, A.R.; King, J.C. Pediatrician attitudes concerning school-located vaccination clinics for seasonal influenza. Pediatrics 2012, 129 (Suppl. 2), S96–S100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempe, A.; Barrow, J.; Stokley, S.; Saville, A.; Glazner, J.E.; Suh, C.; Federico, S.; Abrams, L.; Seewald, L.; Beaty, B.; et al. Effectiveness and cost of immunization recall at school-based health centers. Pediatrics 2012, 129, e1446–e1452. [Google Scholar] [CrossRef] [Green Version]
- Middleman, A.B.; Short, M.B.; Doak, J.S. School-located influenza immunization programs: Factors important to parents and students. Vaccine 2012, 30, 4993–4999. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; O’Brien, K.L.; Madhi, S.A.; Widdowson, M.-A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet. Glob. Health 2020, 8, e497–e510. [Google Scholar] [CrossRef] [Green Version]
- Rosano, A.; Bella, A.; Gesualdo, F.; Acampora, A.; Pezzotti, P.; Marchetti, S.; Ricciardi, W.; Rizzo, C. Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14–2016/17 seasons). Int. J. Infect. Dis. 2019, 88, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Pitrelli, A. Introduction of a quadrivalent influenza vaccine in Italy: A budget impact analysis. J. Prev. Med. Hyg. 2016, 57, E34–E44. [Google Scholar]
- Available online: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination/types-of-seasonal-influenza-vaccine (accessed on 1 March 2022).
- Mameli, C.; Cocchi, I.; Fumagalli, M.; Zuccotti, G. Influenza Vaccination: Effectiveness, Indications, and Limits in the Pediatric Population. Front. Pediatr. 2019, 7, 317. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.salute.gov.it/portale/p5_1_2.jsp?lingua=italiano&id=103 (accessed on 1 March 2022).
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States—Overview of Vaccine Recommendations for 2017–2018 and Vaccination Coverage Rates for 2015–2016 and 2016–2017 Influenza Seasons; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Available online: http://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2018&codLeg=64381&parte=1%20&serie=null (accessed on 1 March 2022).
- Available online: https://sip.it/2020/10/13/vaccinazione-antinfluenzale-la-mappa-ditalia/ (accessed on 1 March 2022).
- Möst, J.; Redlberger-Fritz, M.; Weiss, G. Multiple Influenza Virus Infections in 4 Consecutive Epidemiological Seasons: A Retrospective Study in Children and Adolescents. Open Forum. Infect. Dis. 2019, 6, ofz195. [Google Scholar] [CrossRef]
- Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2222_allegato.pdf (accessed on 1 March 2022).
- European Comission. Comission implementing decissions (EU) 2018/945 of June 22 2018 on the communicable diseases and related special health issues to be covered by epidemiological surveillance as well as relevant case definitions. Off. J. Eur. Union 2018, 170, 1–74. [Google Scholar]
- Matok, I.; Azoulay, L.; Yin, H.; Suissa, S. Immortal Time Bias in Observational Studies of Drug Effects in Pregnancy. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Corrao, G.; Rea, F.; Franchi, M.; Beccalli, B.; Locatelli, A.; Cantarutti, A. Warning of Immortal Time Bias When Studying Drug Safety in Pregnancy: Application to Late Use of Antibiotics and Preterm Delivery. Int. J. Environ. Res. Public Health 2020, 17, 6465. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.J.; Rothman, K.J.; Bateman, B.T.; Hernandez-Diaz, S.; Huybrechts, K.F. A propensity-score-based fine stratification approach for confounding adjustment when exposure is infrequent. Epidemiology 2017, 28, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Ritzwoller, D.P.; Bridges, C.B.; Shetterly, S.; Yamasaki, K.; Kolczak, M.; France, E.K. Effectiveness of the 2003–2004 influenza vaccine among children 6 months to 8 years of age, with 1 versus 2 doses. Pediatrics 2005, 116, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.J.; Hak, E.; Stalman, W.A.B.; VAN Essen, G.A.; Hoes, A.W.; Verheij, T.J.M. Clinical effectiveness of conventional influenza vaccination in asthmatic children. Epidemiol. Infect. 2002, 128, 205–211. [Google Scholar] [CrossRef]
- Kawai, N.; Ikematsu, H.; Iwaki, N.; Satoh, I.; Kawashima, T.; Tsuchimoto, T.; Kashiwagi, S. A prospective, internet-based study of the effectiveness and safety of influenza vaccination in the 2001–2002 influenza season. Vaccine 2003, 21, 4507–4513. [Google Scholar] [CrossRef]
- Hurwitz, E.S.; Haber, M.; Chang, A.; Shope, T.; Teo, S.T.; Giesick, J.S.; Ginsberg, M.M.; Cox, N.J. Studies of the 1996–1997 inactivated influenza vaccine among children attending day care: Immunologic response, protection against infection, and clinical effectiveness. J. Infect. Dis. 2000, 182, 1218–1221. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/emergencies/situations/influenza-a-(h1n1)-outbreak (accessed on 1 March 2022).
- Baldo, V.; Bertoncello, C.; Cocchio, S.; Fonzo, M.; Pillon, P.; Buja, A.; Baldovin, T. The new pandemic influenza A/(H1N1)pdm09 virus: Is it really “new”? J. Prev. Med. Hyg. 2016, 57, E19–E22. [Google Scholar]
- Available online: https://www.ema.europa.eu/en/news/european-medicines-agency-recommends-authorisation-additional-vaccine-influenza-pandemic-h1n1-2009 (accessed on 1 March 2022).
- Available online: https://www.epicentro.iss.it/focus/h1n1/15-10-2009 (accessed on 1 March 2022).
- Rizzo, C.; Bella, A.; Alfonsi, V.; Puzelli, S.; Palmieri, A.P.; Chironna, M.; Pariani, E.; Piatti, A.; Tiberti, D.; Ghisetti, V.; et al. Influenza vaccine effectiveness in Italy: Age, subtype-specific and vaccine type estimates 2014/15 season. Vaccine 2016, 34, 3102–3108. [Google Scholar] [CrossRef]
- Available online: https://www.ecdc.europa.eu/sites/default/files/documents/seasonal-influenza-annual-epidemiological-report-2018.pdf (accessed on 1 March 2022).
- Kissling, E.; Pozo, F.; Buda, S.; Vilcu, A.-M.; Gherasim, A.; Brytting, M.; Domegan, L.; Gómez, V.; Meijer, A.; Lazar, M.; et al. Low 2018/19 vaccine effectiveness against influenza A(H3N2) among 15–64-year-olds in Europe: Exploration by birth cohort. Eurosurveillance 2019, 24, 1900604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutsakos, M.; Wheatley, A.K.; Laurie, K.; Kent, S.J.; Rockman, S. Influenza lineage extinction during the COVID-19 pandemic? Nat. Rev. Microbiol. 2021, 19, 741–742. [Google Scholar] [CrossRef] [PubMed]
- Ando, S. Estimation of the Effectiveness of Quadrivalent Influenza Vaccines by Distinguishing Between Influenza A (H1N1) pdm09 and Influenza A (H3N2) Using Rapid Influenza Diagnostic Tests During the 2018–2019 Season. Intern. Med. 2020, 59, 933–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, J.R.; Flannery, B.; Gaglani, M.; Smith, M.E.; Reis, E.C.; Hickey, R.W.; Jackson, M.L.; Jackson, L.A.; Belongia, E.A.; McLean, H.Q.; et al. Patterns of Influenza Vaccination and Vaccine Effectiveness Among Young US Children Who Receive Outpatient Care for Acute Respiratory Tract Illness. JAMA Pediatr. 2020, 174, 705–713. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Children | Influenza and ILI | |||||
|---|---|---|---|---|---|---|
| Exposed | Unexposed | Exposed | Unexposed | HR | (95% CI) | |
| Additive effect | 10,202 | 3128 | 388 | 129 | 0.91 | (0.74–1.11) |
| Prolonged effect | 5138 | 133,838 | 524 | 11,953 | 0.97 | (0.89–1.06) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantarutti, A.; Barbieri, E.; Didonè, F.; Scamarcia, A.; Giaquinto, C.; Corrao, G. Influenza Vaccination Effectiveness in Paediatric ‘Healthy’ Patients: A Population-Based Study in Italy. Vaccines 2022, 10, 582. https://doi.org/10.3390/vaccines10040582
Cantarutti A, Barbieri E, Didonè F, Scamarcia A, Giaquinto C, Corrao G. Influenza Vaccination Effectiveness in Paediatric ‘Healthy’ Patients: A Population-Based Study in Italy. Vaccines. 2022; 10(4):582. https://doi.org/10.3390/vaccines10040582
Chicago/Turabian StyleCantarutti, Anna, Elisa Barbieri, Fabio Didonè, Antonio Scamarcia, Carlo Giaquinto, and Giovanni Corrao. 2022. "Influenza Vaccination Effectiveness in Paediatric ‘Healthy’ Patients: A Population-Based Study in Italy" Vaccines 10, no. 4: 582. https://doi.org/10.3390/vaccines10040582
APA StyleCantarutti, A., Barbieri, E., Didonè, F., Scamarcia, A., Giaquinto, C., & Corrao, G. (2022). Influenza Vaccination Effectiveness in Paediatric ‘Healthy’ Patients: A Population-Based Study in Italy. Vaccines, 10(4), 582. https://doi.org/10.3390/vaccines10040582