
Humoral Response in Hemodialysis Patients Following COVID-19 Vaccination and Breakthrough Infections during Delta and Omicron Variant Predominance

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
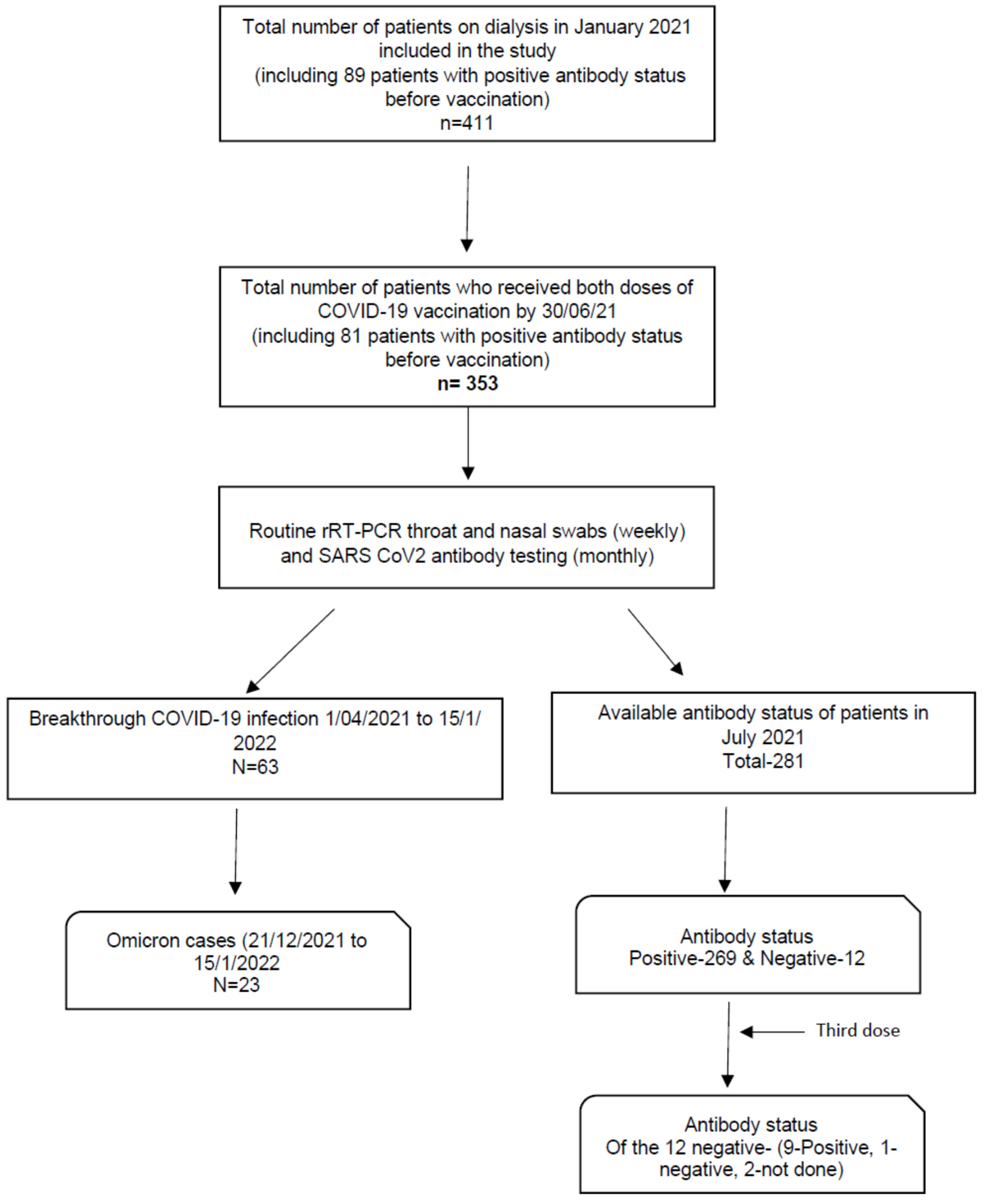
2.1. Study Population
2.2. Assays
2.3. Vaccination
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
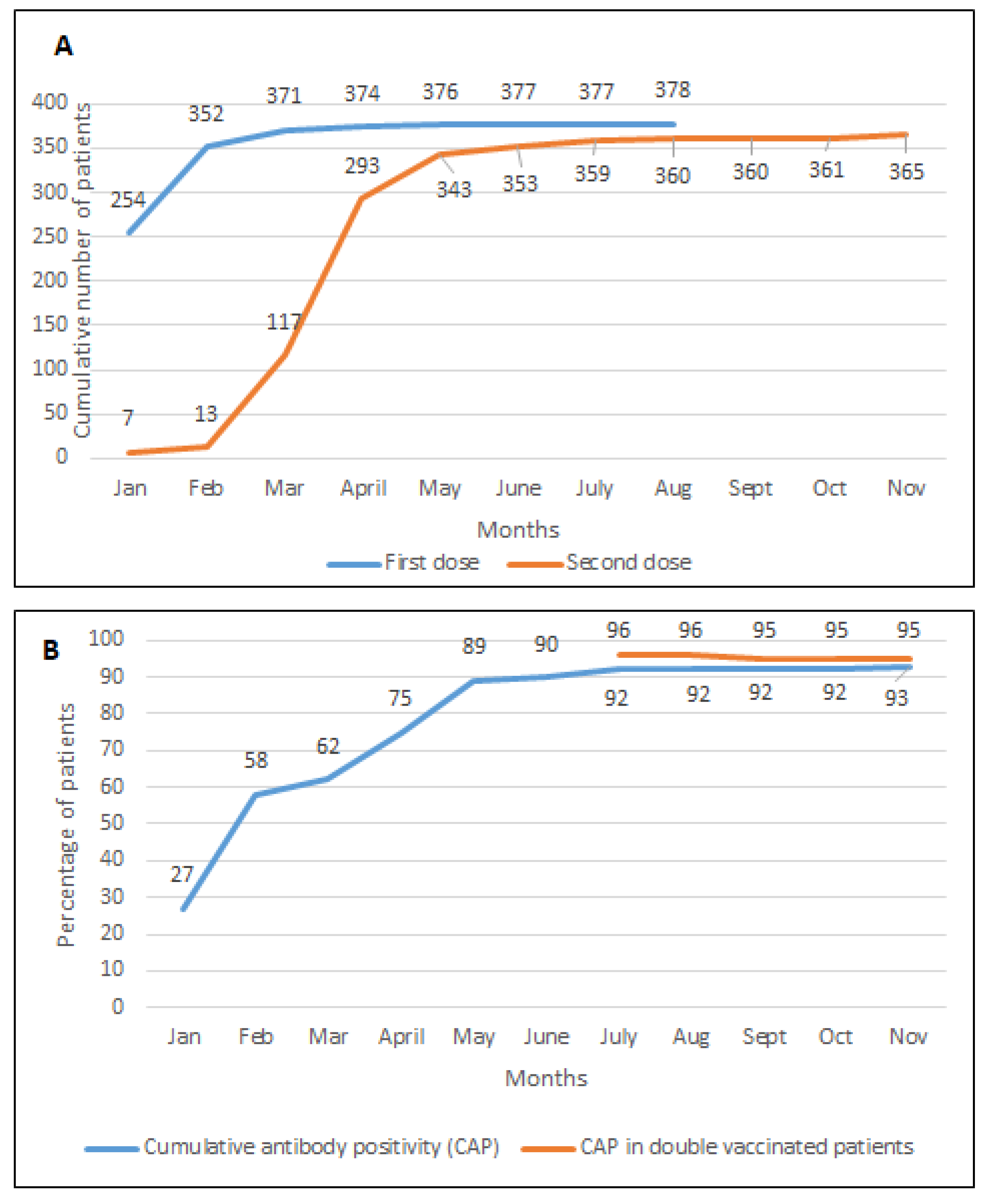
3.2. Vaccination Status
3.3. Antibody Status
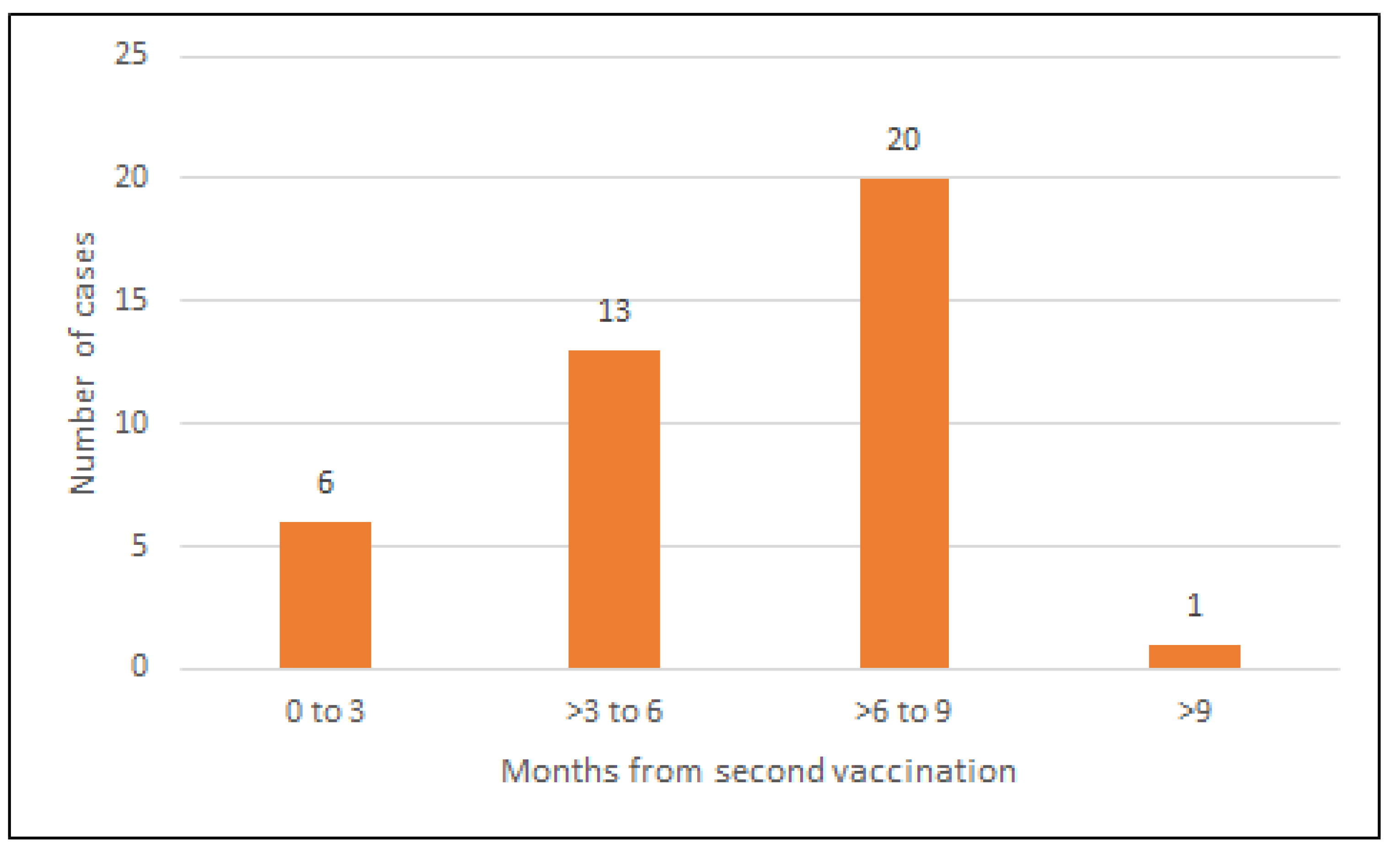
3.4. Breakthrough Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruchfeld, A. The COVID-19 pandemic: Consequences for nephrology. Nat. Rev. Nephrol. 2021, 17, 81–82. [Google Scholar] [CrossRef] [PubMed]
- Craig-Schapiro, R.; Salinas, T.; Lubetzky, M.; Abel, B.T.; Sultan, S.; Lee, J.R.; Kapur, S.; Aull, M.J.; Dadhania, D.M. COVID-19 outcomes in patients waitlisted for kidney transplantation and kidney transplant recipients. Am. J. Transplant. 2021, 21, 1576–1585. [Google Scholar] [CrossRef] [PubMed]
- UK Kidney Association. UK Kidney Association Guidance on COVID-19 Vaccination in Highly Vulnerable People with Kidney Disease. 2021. Available online: https://ukkidney.org/sites/renal.org/files/UKKA%20COVID19%20Vaccination%20Guidance%20for%20HCPs%2006.07.21.pdf (accessed on 10 February 2022).
- Speer, C.; Göth, D.; Benning, L.; Buylaert, M.; Schaier, M.; Grenz, J.; Nusshag, C.; Kälble, F.; Kreysing, M.; Reichel, P.; et al. Early humoral responses of hemodialysis patients after COVID-19 vaccination with BNT162b2. Clin. J. Am. Soc. Nephrol. 2021, 16, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.; Abe, K.T.; Naimark, D.; Oliver, M.J.; Perl, J.; Leis, J.A.; Bolotin, S.; Tran, V.; Mullin, S.I.; Shadowitz, E.; et al. Evaluation of the SARS-CoV-2 Antibody Response to the BNT162b2 Vaccine in Patients Undergoing Hemodialysis. JAMA Netw. Open 2021, 4, e2123622. [Google Scholar] [CrossRef] [PubMed]
- Simon, B.; Rubey, H.; Treipl, A.; Gromann, M.; Hemedi, B.; Zehetmayer, S.; Kirsch, B. Haemodialysis patients show a highly diminished antibody response after COVID-19 mRNA vaccination compared with healthy controls. Nephrol. Dial. Transplant. 2021, 36, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Carr, E.J.; Wu, M.; Harvey, R.; Wall, E.C.; Kelly, G.; Hussain, S.; Howell, M.; Kassiotis, G.; Swanton, C.; Gandhi, S.; et al. Neutralising antibodies after COVID-19 vaccination in UK haemodialysis patients. Lancet 2021, 398, 1038–1041. [Google Scholar] [CrossRef]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Morgan, C.; Kerschmann, R.; Beyer, P.; Dittrich, M.; et al. SARS-CoV-2 Vaccine Antibody Response and Breakthrough Infection in Patients Receiving Dialysis. Ann. Internal. Med. 2022. in print. [Google Scholar] [CrossRef] [PubMed]
- Poulikakos, D.; Chinnadurai, R.; McGee, Y.; Gray, S.; Clough, T.; Clarke, N.; Murphy, T.; Wickens, O.; Mitchell, C.; Darby, D.; et al. A Quality Improvement Project to Minimize COVID-19 Infections in Patients Receiving Haemodialysis and the Role of Routine Surveillance Using Nose and Throat Swabs for SARS-CoV-2 rRT-PCR and Serum Antibody Testing. Nephron 2021, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics. Coronavirus (COVID-19) Infection Survey Headline Results, UK. 5 January 2022. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronaviruscovid19infectionsurveypilot/5january2022 (accessed on 10 February 2022).
- Wang, L.; Davis, P.B.; Kaelber, D.C.; Volkow, N.D.; Xu, R. Comparison of mRNA-1273 and BNT162b2 Vaccines on Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Death during the Delta-Predominant Period. JAMA 2022. in print. [Google Scholar] [CrossRef] [PubMed]
- Buti, M.; Viladomiu, L.; Jardi, R.; Olmos, A.; Rodriguez, J.A.; Bartolome, J.; Esteban, R.; Guardia, J. Long-term immunogenicity and efficacy of hepatitis B vaccine in hemodialysis patients. Am. J. Nephrol. 1992, 12, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Broeders, N.E.; Hombrouck, A.; Lemy, A.; Wissing, K.M.; Racapé, J.; Gastaldello, K.; Massart, A.; Van Gucht, S.; Weichselbaum, L.; De Mul, A.; et al. Influenza A/H1N1 vaccine in patients treated by kidney transplant or dialysis: A cohort study. Clin. J. Am. Soc. Nephrol. 2011, 6, 2573–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peces, R.; de la Torre, M.; Alcázar, R.; Urra, J. Prospective analysis of the factors influencing the antibody response to hepatitis B vaccine in hemodialysis patients. Am. J. Kidney Dis. 1997, 29, 239–245. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet 2021, 9, 100178. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, U.; Katikireddi, S.V.; McCowan, C.; Mulholland, R.H.; Azcoaga-Lorenzo, A.; Amele, S.; Fagbamigbe, A.F.; Vasileiou, E.; Grange, Z.; Shi, T.; et al. COVID-19 hospital admissions and deaths after BNT162b2 and ChAdOx1 nCoV-19 vaccinations in 2· 57 million people in Scotland (EAVE II): A prospective cohort study. Lancet Resp. Med. 2021, 9, 1439–1449. [Google Scholar] [CrossRef]
- Pérez-Then, E.; Lucas, C.; Monteiro, V.S.; Miric, M.; Brache, V.; Cochon, L.; Vogels, C.B.; Malik, A.A.; De la Cruz, E.; Jorge, A.; et al. Neutralizing antibodies against the SARS-CoV-2 Delta and Omicron variants following heterologous CoronaVac plus BNT162b2 booster vaccination. Nat. Med. 2022. in print. [Google Scholar] [CrossRef] [PubMed]
- Nealon, J.; Cowling, B.J. Omicron severity: Milder but not mild. Lancet 2022, 399, 412–413. [Google Scholar] [CrossRef]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of immunosuppression on the immunogenicity of mRNA vaccines to SARS-CoV-2: A prospective cohort study. Ann. Internal. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef] [PubMed]
- Nacasch, N.; Erez, D.; Lishner, M.; Benchetrit, S.; Rozenberg, I.; Sarel, E.; Shitrit, P.; Wand, O.; Cohen-Hagai, K. Long-term Antibody Response to the BNT162b2 Vaccine Among Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2022, 79, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Espinosa, D.; Monzó, J.J.; Casals, Q.; Piñeiro, G.J.; Rodas, L.; Vera, M.; Maduell, F. Fatal SARS-CoV-2 reinfection in an immunosuppressed patient on hemodialysis. J. Nephrol. 2021, 34, 1041–1043. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Patients | n = 411 |
|---|---|
| Age, years | 61 (49–72) |
| Ethnicity | |
| Caucasian | 271 (65.9%) |
| Black Asian Minority Ethnic | 140 (34.1%) |
| Gender, Male | 263 (64%) |
| Diabetes Mellitus | 202 (49.1%) |
| Hypertension | 295 (71.8%) |
| Cardiovascular disease | 118 (28.7%) |
| Cancer | 39 (9.5%) |
| Previous kidney transplant | 63 (15.3%) |
| Immunosuppression | |
| Current | 34 (8.3%) |
| Previous | 41 (10%) |
| None | 336 (81.8%) |
| Vaccination status by June 2021 | |
| Received first vaccination | 377 (91.7%) |
| Received two vaccinations | 353 (85.8%) |
| Refused vaccination/unknown | 34 (8.3%) |
| Vaccination type (of the 377 vaccinated) | |
| Pfizer BioNTech | 236 (62.6%) |
| Oxford AstraZeneca | 135 (35.8%) |
| Unknown | 6 (1.59%) |
| Analysis A (Comparative Analysis) | Analysis B (Logistic Regression Analysis) | ||||
|---|---|---|---|---|---|
| Variables Total n = 281 | Positive n = 269 | Negative n = 12 | p-Value | OR (95% CI) | p-Value |
| Age | 62 (51–74) | 69.5 (64–79) | 0.093 | 0.97 (0.93–1.01) | 0.18 |
| Gender (Male) | 173 (64.3%) | 10 (83.3%) | 0.176 | 0.36 (0.07–1.67) | 0.19 |
| Ethnicity (Caucasian) | 173 (64.3%) | 10 (83.3%) | 0.200 | 2.62 (0.56–12.3) | 0.21 |
| Diabetes | 127 (47.2%) | 5 (41.6%) | 0.706 | 1.25 (0.38–4.04) | 0.71 |
| Hypertension | 209 (77.7%) | 7 (58.3%) | 0.120 | 2.48 (0.76–8.12) | 0.13 |
| Cardiovascular disease | 78 (29%) | 3 (25%) | 0.765 | 1.22 (0.32–4.64) | 0.76 |
| Cancer | 27 (10%) | 3 (25%) | 0.101 | 0.35 (0.08–1.31) | 0.12 |
| Immunosuppression | 52 (19.3%) | 3 (25%) | 0.427 | 0.71 (0.18–2.74) | 0.63 |
| Previous transplant | 44 (16.4%) | 1 (8%) | 0.458 | 2.15 (0.27–17.1) | 0.46 |
| Vaccination type | 0.935 | ||||
| Pfizer BioNTech | 170 (63%) | 8 (66.6%) | |||
| Oxford AstraZeneca | 97 (36%) | 4 (33.3%) | |||
| Unknown | 2 (0.8%) | 0 |
| Variables Total n = 353 | COVID Positive n = 63 | COVID Negative n = 290 | p-Value |
|---|---|---|---|
| Age | 61 (49.5–73.5) | 62 (52–73) | 0.738 |
| Gender (Male) | 39 (61.9%) | 200 (68.9%) | 0.277 |
| Ethnicity (Caucasian) | 38 (60.3%) | 188 (64.8%) | 0.499 |
| Diabetes | 34 (53.9%) | 137 (47.2%) | 0.333 |
| Hypertension | 48 (76.1%) | 210 (72.4%) | 0.540 |
| Cardiovascular disease | 19 (30.1%) | 85 (29.3%) | 0.893 |
| Cancer | 5 (7.9%) | 32 (11%) | 0.467 |
| Immunosuppression | 10 (15.8%) | 58 (20%) | 0.452 |
| Previous transplant | 8 (12.6%) | 45 (15.5%) | 0.570 |
| Pre-vaccination antibody status | |||
| Positive | 6 (9.5%) | 75 (29%) | 0.005 |
| Negative | 57 (90.5%) | 215 (71%) | - |
| Antibody Status (July 2021) | |||
| Positive | 53 (84.1%) | 216 (74.5%) | - |
| Negative | 2 (3.1%) | 10 (3.4%) | - |
| Unknown | 8 (12.6%) | 64 (22.1%) | 0.238 |
| Vaccination type | |||
| Pfizer BioNTech | 38 (60.3%) | 186 (64.1%) | 0.501 |
| Oxford AstraZeneca | 25 (39.6%) | 100 (34.4%) | - |
| Unknown | 0 (0) | 4 (1.4%) | - |
| Total Patients n = 63 (Out of 353 Patients) | Before Omicron (1 April 2021 to 20 December 2021) n = 40 | Omicron Period (21 December 2021 to 15 January 2022) n = 23 | p-Value |
|---|---|---|---|
| Age, years | 61 (52–74) | 61 (40–74) | 0.568 |
| Caucasian | 25 (62.5%) | 14 (60.9%) | 0.898 |
| Gender, Male | 23 (57.5%) | 15 (65.2%) | 0.547 |
| Diabetes Mellitus | 24 (60%) | 10 (43.4%) | 0.205 |
| Hypertension | 29 (72.5%) | 19 (82.6%) | 0.364 |
| Cardiovascular disease | 12 (30%) | 7 (30.4%) | 0.971 |
| Cancer | 3 (7.5%) | 2 (8.7%) | 0.866 |
| Previous kidney transplant | 2 (5%) | 6 (26.1%) | 0.016 |
| Immunosuppression | 8 (20%) | 7 (30.4%) | 0.349 |
| Vaccination status | |||
| Received first dose | 40 (100%) | 23 (100%) | - |
| Received second dose | 40 (100%) | 23 (100%) | - |
| Received third dose | 4 (10%) | 17 (74%) | - |
| Vaccination type | |||
| Pfizer BioNTech | 24 (60%) | 14 (%) | - |
| Oxford AstraZeneca | 16 (40%) | 9 (%) | - |
| Antibody status in Nov 2021 | |||
| Positive | 30 | 17 | - |
| Not done | 10 | 6 | - |
| COVID-related hospitalisation | 5 (12.5%) | 0 | - |
| COVID-related death | 2 (5%) | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinnadurai, R.; Wu, H.H.L.; Cox, E.; Moore, J.; Clough, T.; Lamerton, E.; Donne, R.; O’Riordan, E.; Poulikakos, D. Humoral Response in Hemodialysis Patients Following COVID-19 Vaccination and Breakthrough Infections during Delta and Omicron Variant Predominance. Vaccines 2022, 10, 498. https://doi.org/10.3390/vaccines10040498
Chinnadurai R, Wu HHL, Cox E, Moore J, Clough T, Lamerton E, Donne R, O’Riordan E, Poulikakos D. Humoral Response in Hemodialysis Patients Following COVID-19 Vaccination and Breakthrough Infections during Delta and Omicron Variant Predominance. Vaccines. 2022; 10(4):498. https://doi.org/10.3390/vaccines10040498
Chicago/Turabian StyleChinnadurai, Rajkumar, Henry H. L. Wu, Eleanor Cox, Jayne Moore, Toni Clough, Elizabeth Lamerton, Rosie Donne, Edmond O’Riordan, and Dimitrios Poulikakos. 2022. "Humoral Response in Hemodialysis Patients Following COVID-19 Vaccination and Breakthrough Infections during Delta and Omicron Variant Predominance" Vaccines 10, no. 4: 498. https://doi.org/10.3390/vaccines10040498
APA StyleChinnadurai, R., Wu, H. H. L., Cox, E., Moore, J., Clough, T., Lamerton, E., Donne, R., O’Riordan, E., & Poulikakos, D. (2022). Humoral Response in Hemodialysis Patients Following COVID-19 Vaccination and Breakthrough Infections during Delta and Omicron Variant Predominance. Vaccines, 10(4), 498. https://doi.org/10.3390/vaccines10040498