
Evaluating COVID-19 Booster Vaccination Strategies in a Partially Vaccinated Population: A Modeling Study


Abstract
:1. Introduction
2. Methods
2.1. COVID-19 Transmission Model
2.2. Parametrization
2.3. Vaccine Efficacies
2.4. Vaccination Strategies
3. Results
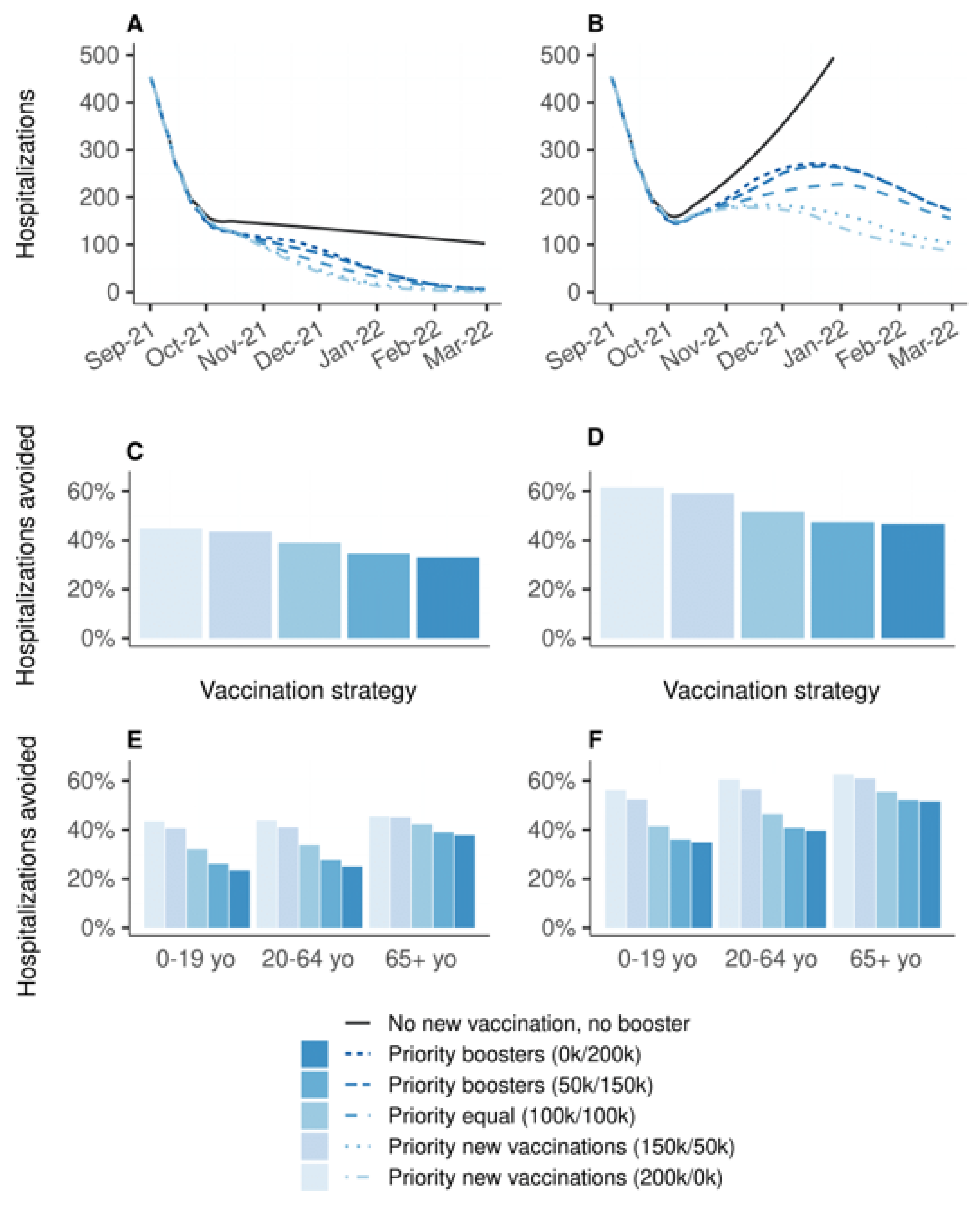
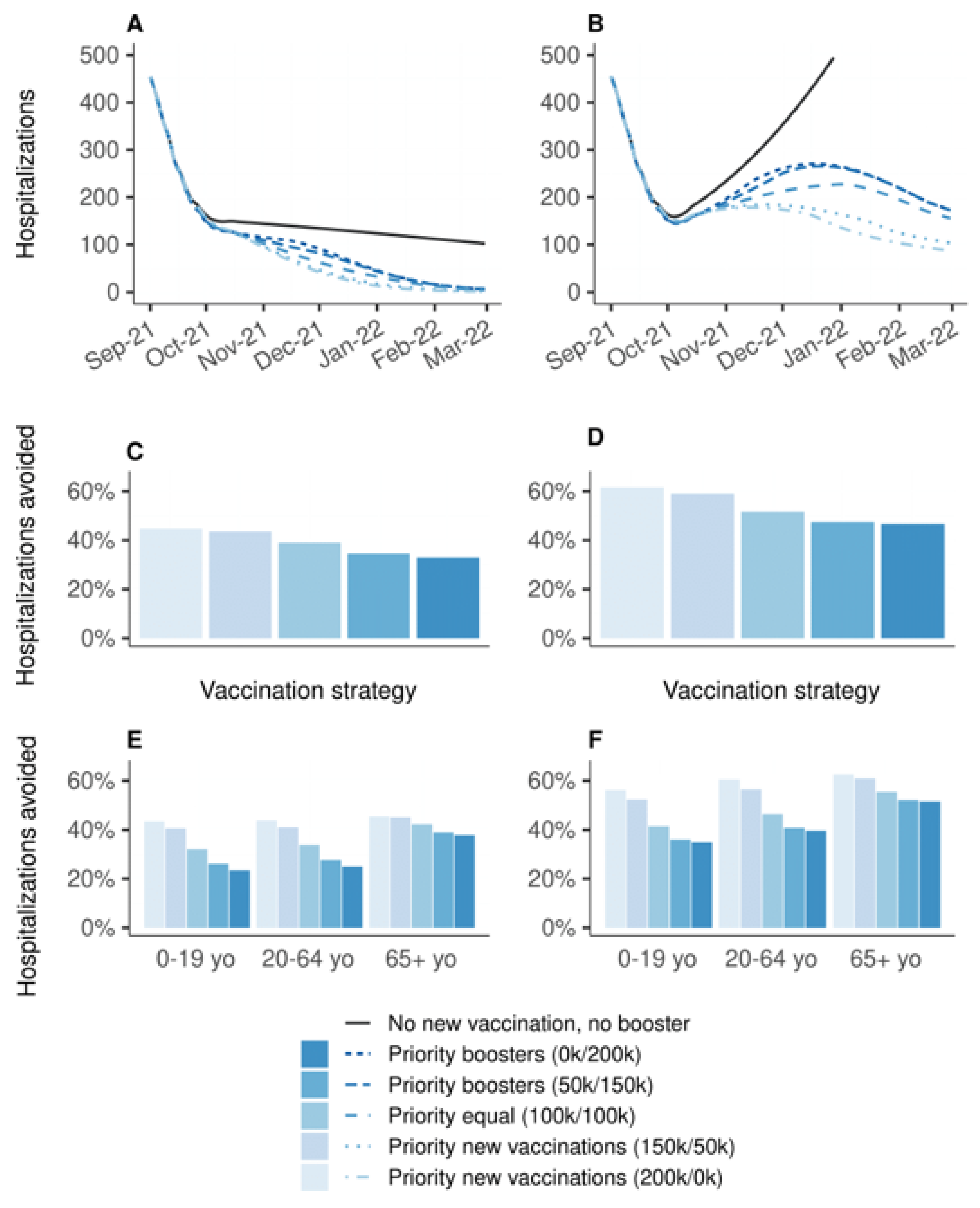
3.1. Primary Vaccination Versus Booster Doses
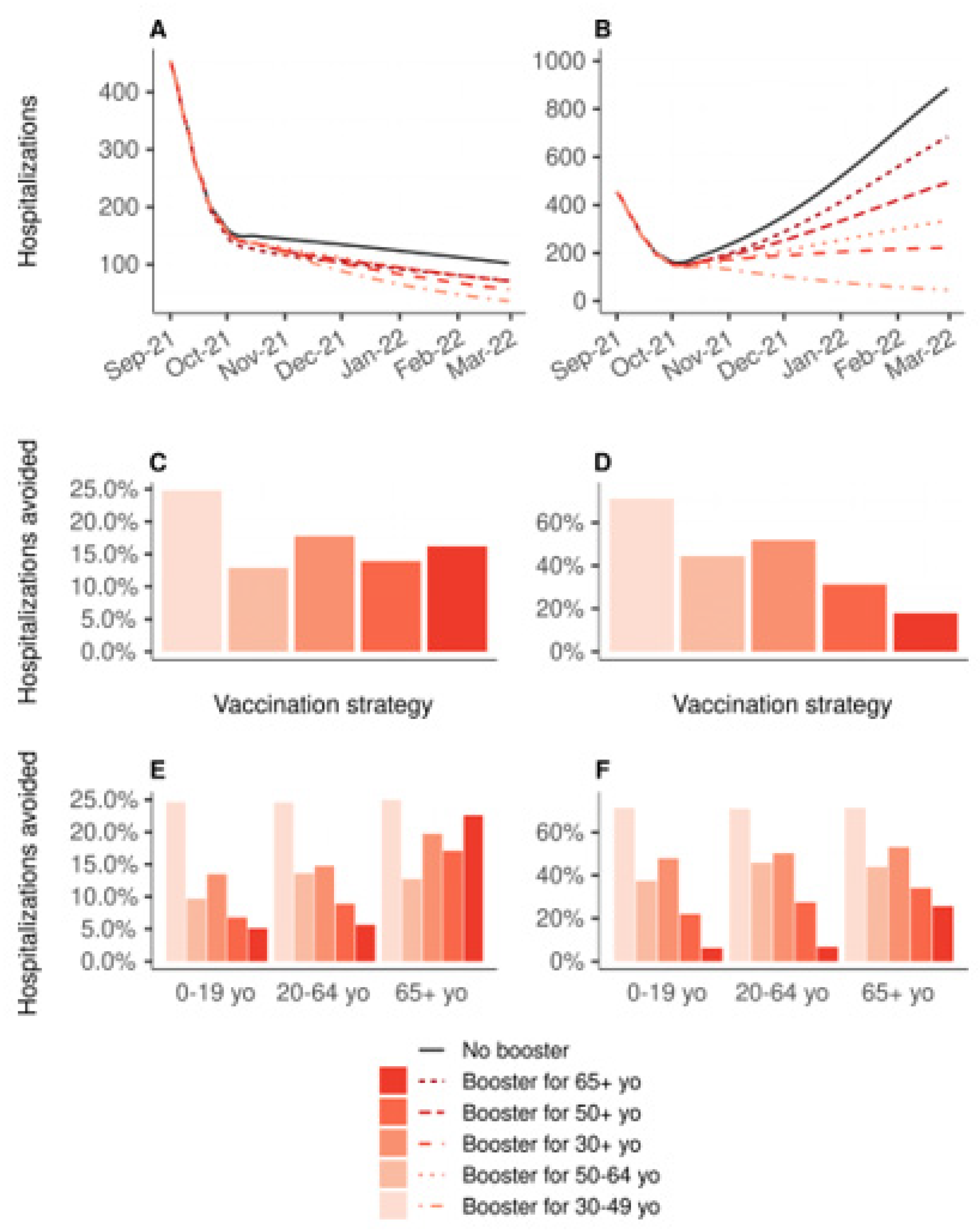
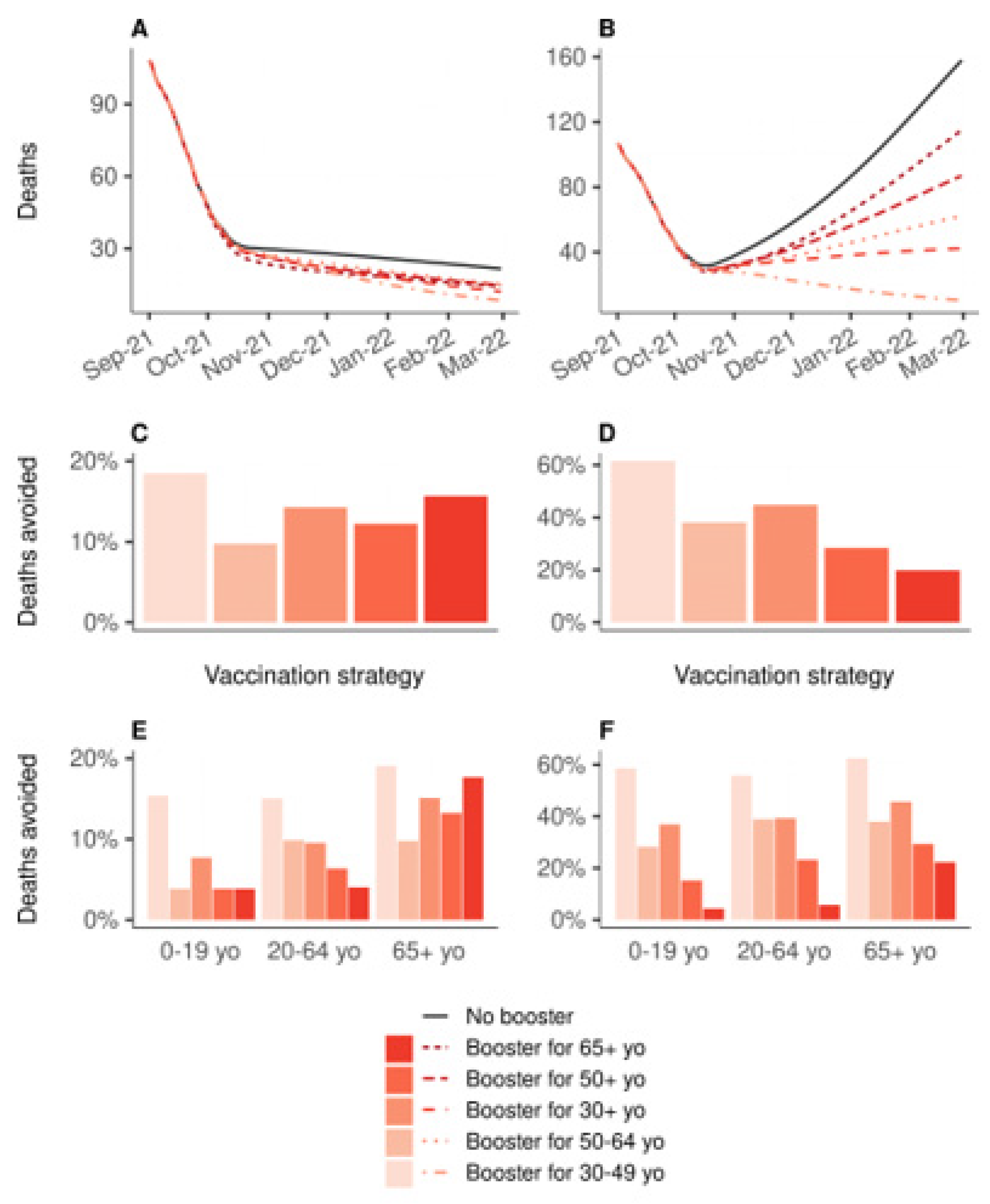
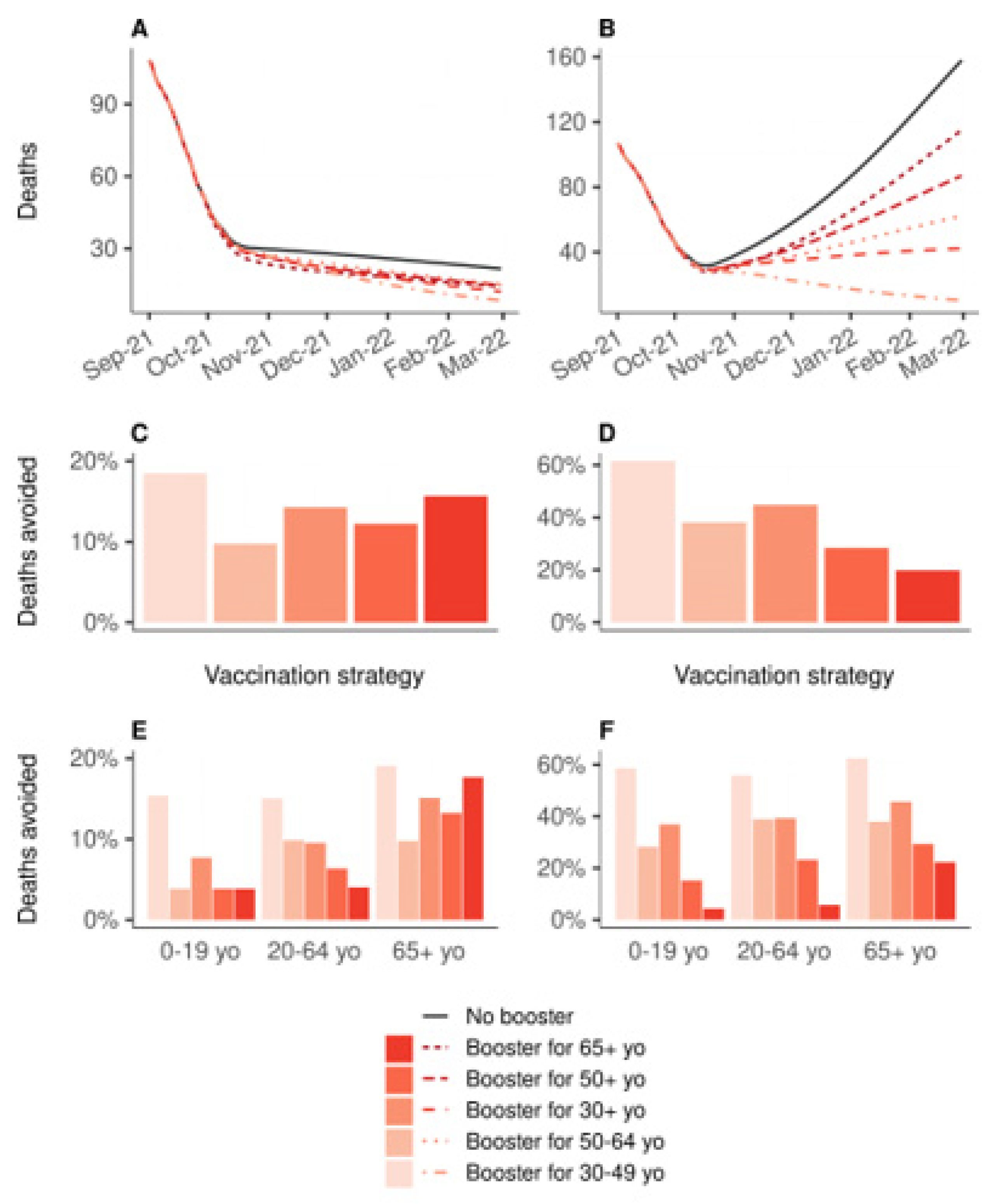
3.2. Prioritization of Booster Doses
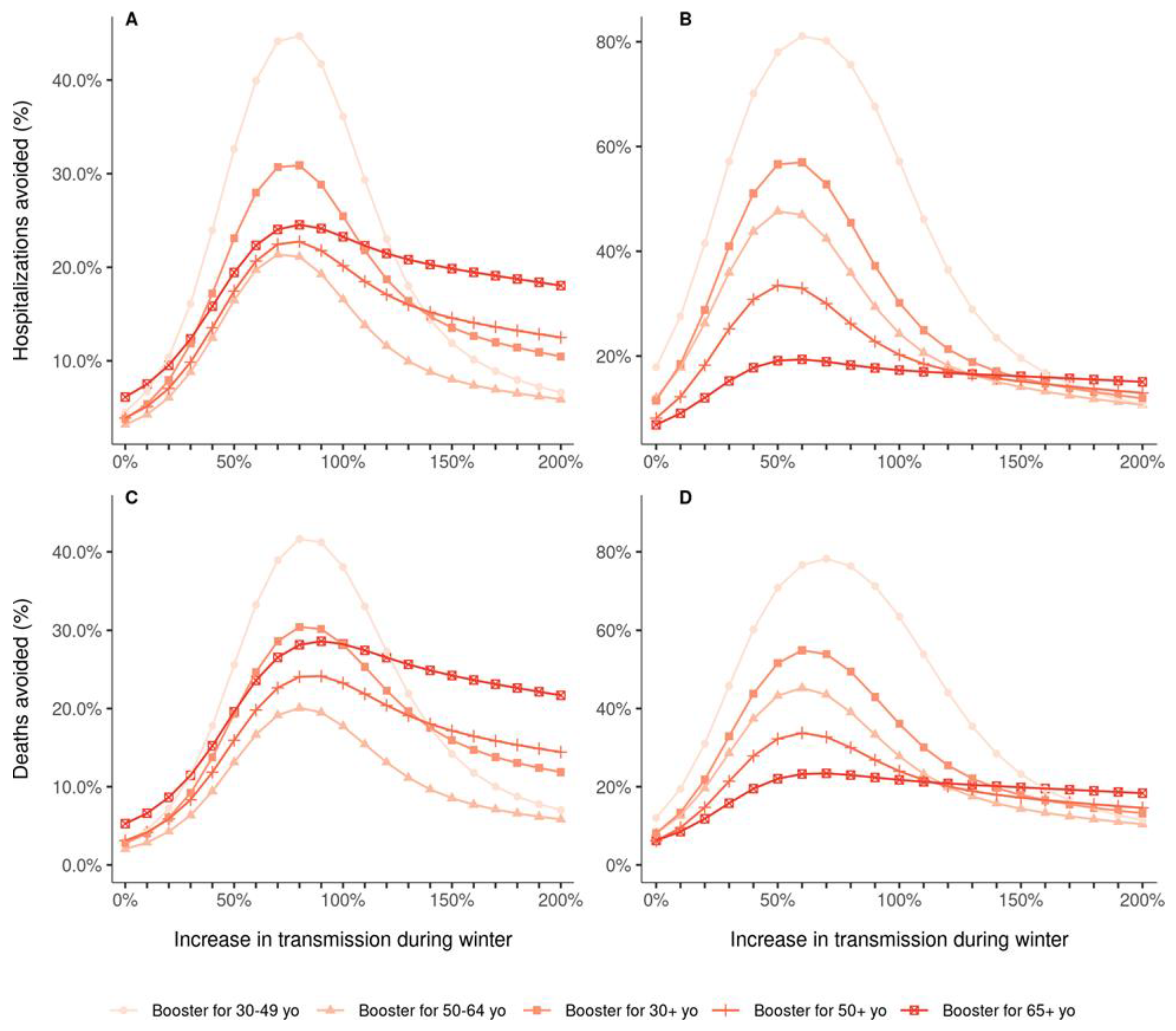
3.3. Impact of Variations of Transmissibility
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. Effectiveness of the BNT162b2 Covid-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Stowe, J.; Andrews, N.; Gower, C.; Gallagher, E.; Utsi, L.; Simmons, R.; Thelwall, S.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 vaccines against hospital admission with the Delta (B.1.617.2) variant. KHub 2021. preprint not certified by peer review. [Google Scholar]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Agence Nationale de Sécurité du Médicament. COVID-19—Vaccins Autorisés. 2021. Available online: https://ansm.sante.fr/dossiers-thematiques/covid-19-vaccins/covid-19-vaccins-autorises (accessed on 31 January 2022).
- Santé Publique France. Données Relatives Aux Personnes Vaccinées Contre la COVID-19. 2021. Available online: https://www.data.gouv.fr/fr/datasets/donnees-relatives-aux-personnes-vaccinees-contre-la-covid-19-1/ (accessed on 31 January 2022).
- Santé Publique France. COVID-19: Point Épidémiologique du 11 Mars 2021. 2021. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-11-mars-2021 (accessed on 31 January 2022).
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé. Avis n° 2021.0061/AC/SEESP du 23 août 2021 du Collège de la HAS Relatif à la Définition des Populations à Cibler par la Campagne de Rappel Vaccinal chez les Personnes Ayant eu une Primovaccination Complète Contre la COVID-19. 2021. Available online: https://www.has-sante.fr/jcms/p_3283044/fr/avis-n-2021-0061/ac/seesp-du-23-aout-2021-du-college-de-la-has-relatif-a-la-definition-des-populations-a-cibler-par-la-campagne-de-rappel-vaccinal-chez-les-personnes-ayant-eu-une-primovaccination-complete-contre-la-covid-19 (accessed on 31 January 2022).
- Roux, J.; Massonnaud, C.; Colizza, V.; Cauchemez, S.; Crépey, P. Impact of national and regional lockdowns on COVID-19 epidemic waves: Application to the 2020 spring wave in France. medRxiv 2021. [Google Scholar] [CrossRef]
- Kiem, C.T.; Massonnaud, C.R.; Levy-Bruhl, D.; Poletto, C.; Colizza, V.; Bosetti, P.; Fontanet, A.; Gabet, A.; Olié, V.; Zanetti, L.; et al. A modelling study investigating short and medium-term challenges for COVID-19 vaccination: From prioritisation to the relaxation of measures. EClinicalMedicine 2021, 38, 101001. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLOS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef] [PubMed]
- Bager, P.; Wohlfahrt, J.; Rasmussen, M.; Albertsen, M.; Grove Krause, T. Hospitalisation associated with SARS-CoV-2 delta variant in Denmark. Lancet. Infect. Dis. 2021, 21, 1351. [Google Scholar] [CrossRef]
- Collin, A.; Hejblum, B.P.; Vignals, C.; Lehot, L.; Thiébaut, R.; Moireau, P.; Prague, M. Using Population Based Kalman Estimator to Model COVID-19 Epidemic in France: Estimating the Effects of Non-Pharmaceutical Interventions on the Dynamics of Epidemic. medRxiv 2021. [Google Scholar] [CrossRef]
- Carrat, F.; de Lamballerie, X.; Rahib, D.; Blanché, H.; Lapidus, N.; Artaud, F.; Kab, S.; Renuy, A.; de Edelenyi, F.S.; Meyer, L.; et al. Antibody status and cumulative incidence of SARS-CoV-2 infection among adults in three regions of France following the first lockdown and associated risk factors: A multicohort study. Int. J. Epidemiol. 2021, 50, 1458–1472. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Haute Autorité de Santé. Stratégie de Vaccination Contre le Sars-Cov-2—Recommandations Préliminaires sur la Stratégie de Priorisation des Populations à Vacciner. 2021. Available online: https://www.has-sante.fr/jcms/p_3221338/fr/strategie-de-vaccination-contre-le-sars-cov-2-recommandations-preliminaires-sur-la-strategie-de-priorisation-des-populations-a-vacciner (accessed on 31 January 2022).
- Pfizer and BioNTech Announce Phase 3 Trial Data Showing High Efficacy of a Booster Dose of Their COVID-19 Vaccine | Pfizer. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-phase-3-trial-data-showing (accessed on 12 November 2021).
- Li, B.; Deng, A.; Li, K.; Hu, Y.; Li, Z.; Xiong, Q.; Liu, Z.; Guo, Q.; Zou, L.; Zhang, H.; et al. Viral infection and transmission in a large well-traced outbreak caused by the Delta SARS-CoV-2 variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Iwasaki, A. What reinfections mean for COVID-19. Lancet Infect. Dis. 2021, 21, 3–5. [Google Scholar] [CrossRef]
- Boyton, R.J.; Altmann, D.M. Risk of SARS-CoV-2 reinfection after natural infection. Lancet 2021, 397, 1161–1163. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on COVID-19 Vaccine Booster Doses. 2021. Available online: https://www.who.int/news/item/10-08-2021-interim-statement-on-covid-19-vaccine-booster-doses (accessed on 31 January 2022).
- WHO. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. 26 November 2021. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 31 January 2022).
- Massonnaud, C.; Roux, J.; Crépey, P. COVID-19: Forecasting short term hospital needs in France. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Roux, J.; Massonnaud, C.; Crépey, P. COVID-19: One-month impact of the French lockdown on the epidemic burden. medRxiv 2020. [Google Scholar] [CrossRef]
- INSEE. Population Légale 2017 en Vigueur au 1er Janvier. 2020. Available online: https://www.insee.fr/fr/statistiques/4265429?sommaire=4265511 (accessed on 5 March 2020).
- Tindale, L.; Coombe, M.; Stockdale, J.E.; Garlock, E.S.; Venus Lau, W.Y.; Saraswat, M.; Lee, Y.-H.B.; Zhang, L.; Chen, D.; Wallinga, J.; et al. Transmission interval estimates suggest pre-symptomatic spread of COVID-19. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef]
- Lapidus, N.; Paireau, J.; Levy-Bruhl, D.; Lamballerie, X.; Severi, G.; Touvier, M.; Zins, M.; Cauchemez, S.; Carrat, F.; Sapris-Sero Study Group. Do not neglect SARS-CoV-2 hospitalization and fatality risks in the middle-aged adult population. Infect. Dis. Now. 2021, 51, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. Données Hospitalières Relatives à L’épidémie de COVID-19. Available online: https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie-de-covid-19/ (accessed on 1 April 2020).
- Salje, H.; Tran Kiem, C.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.-L.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Bolker, B.; R Development Core Team. bbmle: Tools for General Maximum Likelihood Estimation. 2020. Available online: https://CRAN.R-project.org/package=bbmle (accessed on 1 April 2020).
- Stroustrup, B. The C++ programming language: Reference manual. In Computing Science; AT and T Bell Laboratories: Murray Hill, NJ, USA, 1984. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org (accessed on 16 March 2020).
- Lefrancq, N.; Paireau, J.; Hozé, N.; Courtejoie, N.; Yazdanpanah, Y.; Bouadma, L.; Boëlle, P.Y.; Chereau, F.; Salje, H.; Cauchemez, S. Evolution of outcomes for patients hospitalised during the first 9 months of the SARS-CoV-2 pandemic in France: A retrospective national surveillance data analysis. Lancet Reg. Health-Eur. 2021, 5, 100087. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccine | Infection | Symptomatic Case | Hospitalization | ||
|---|---|---|---|---|---|
| Efficacy against Alpha VOC | Base efficacy | Vector vaccine | 73% 4 | 75% 5 | 86% 6 |
| mRNA | 92% 4 | 94% 5 | 97% 7 | ||
| Efficacy against Delta VOC | Base efficacy | Vector vaccine | 60% 4 | 67% 5 | 92% 6 |
| mRNA | 79% 4 | 88% 5 | 96% 6 | ||
| Decreased efficacy | Vector vaccine | 53% 12 | 53% 12 | 92% * | |
| mRNA | 53% 12 | 53% 12 | 93% 12 | ||
| Efficacy after booster dose | mRNA | 92% | 94% | 97% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massonnaud, C.R.; Roux, J.; Colizza, V.; Crépey, P. Evaluating COVID-19 Booster Vaccination Strategies in a Partially Vaccinated Population: A Modeling Study. Vaccines 2022, 10, 479. https://doi.org/10.3390/vaccines10030479
Massonnaud CR, Roux J, Colizza V, Crépey P. Evaluating COVID-19 Booster Vaccination Strategies in a Partially Vaccinated Population: A Modeling Study. Vaccines. 2022; 10(3):479. https://doi.org/10.3390/vaccines10030479
Chicago/Turabian StyleMassonnaud, Clément R., Jonathan Roux, Vittoria Colizza, and Pascal Crépey. 2022. "Evaluating COVID-19 Booster Vaccination Strategies in a Partially Vaccinated Population: A Modeling Study" Vaccines 10, no. 3: 479. https://doi.org/10.3390/vaccines10030479
APA StyleMassonnaud, C. R., Roux, J., Colizza, V., & Crépey, P. (2022). Evaluating COVID-19 Booster Vaccination Strategies in a Partially Vaccinated Population: A Modeling Study. Vaccines, 10(3), 479. https://doi.org/10.3390/vaccines10030479