
Effectiveness of Prophylactic Human Papillomavirus Vaccine in the Prevention of Recurrence in Women Conized for HSIL/CIN 2-3: The VENUS Study

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
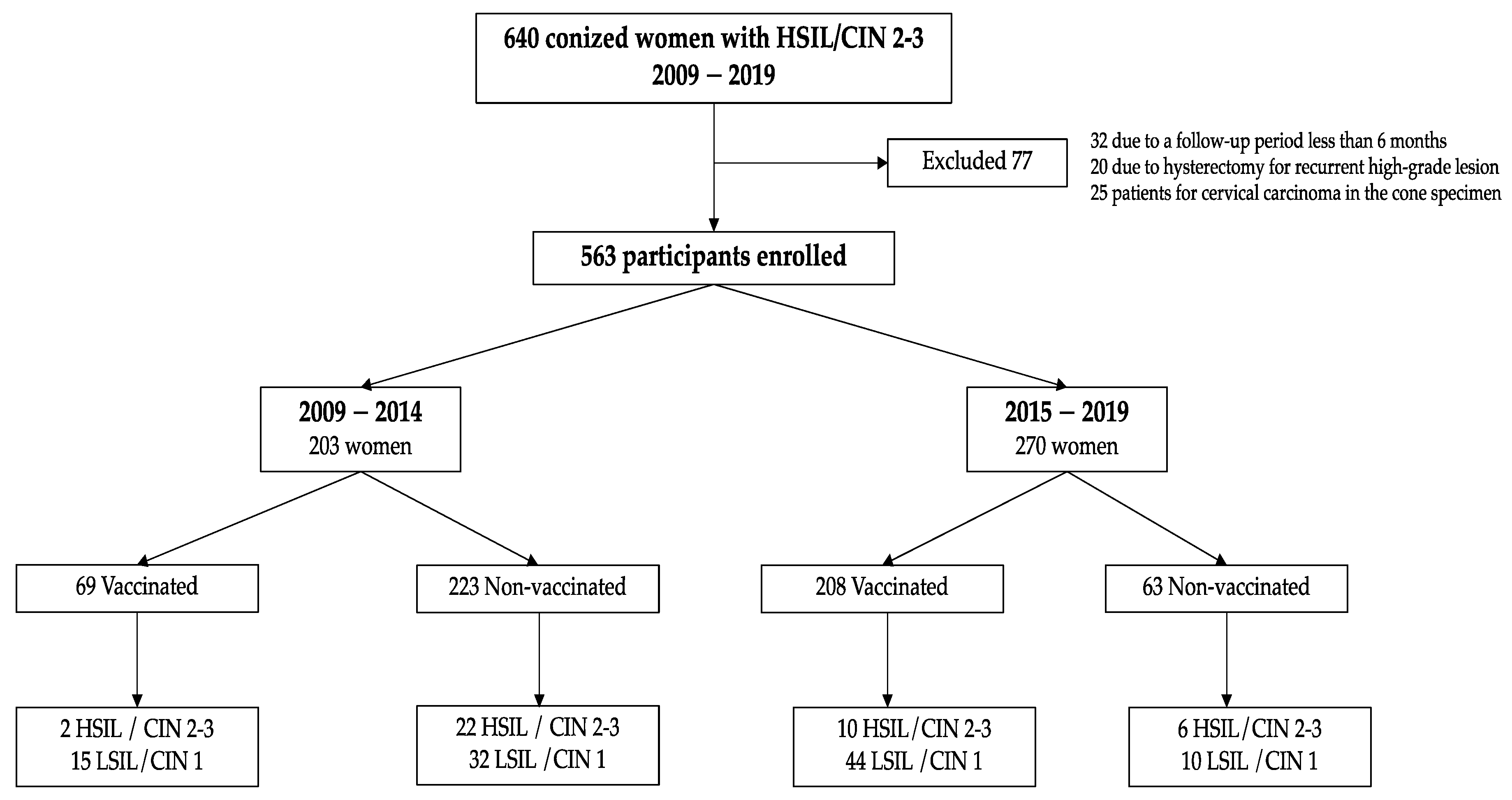
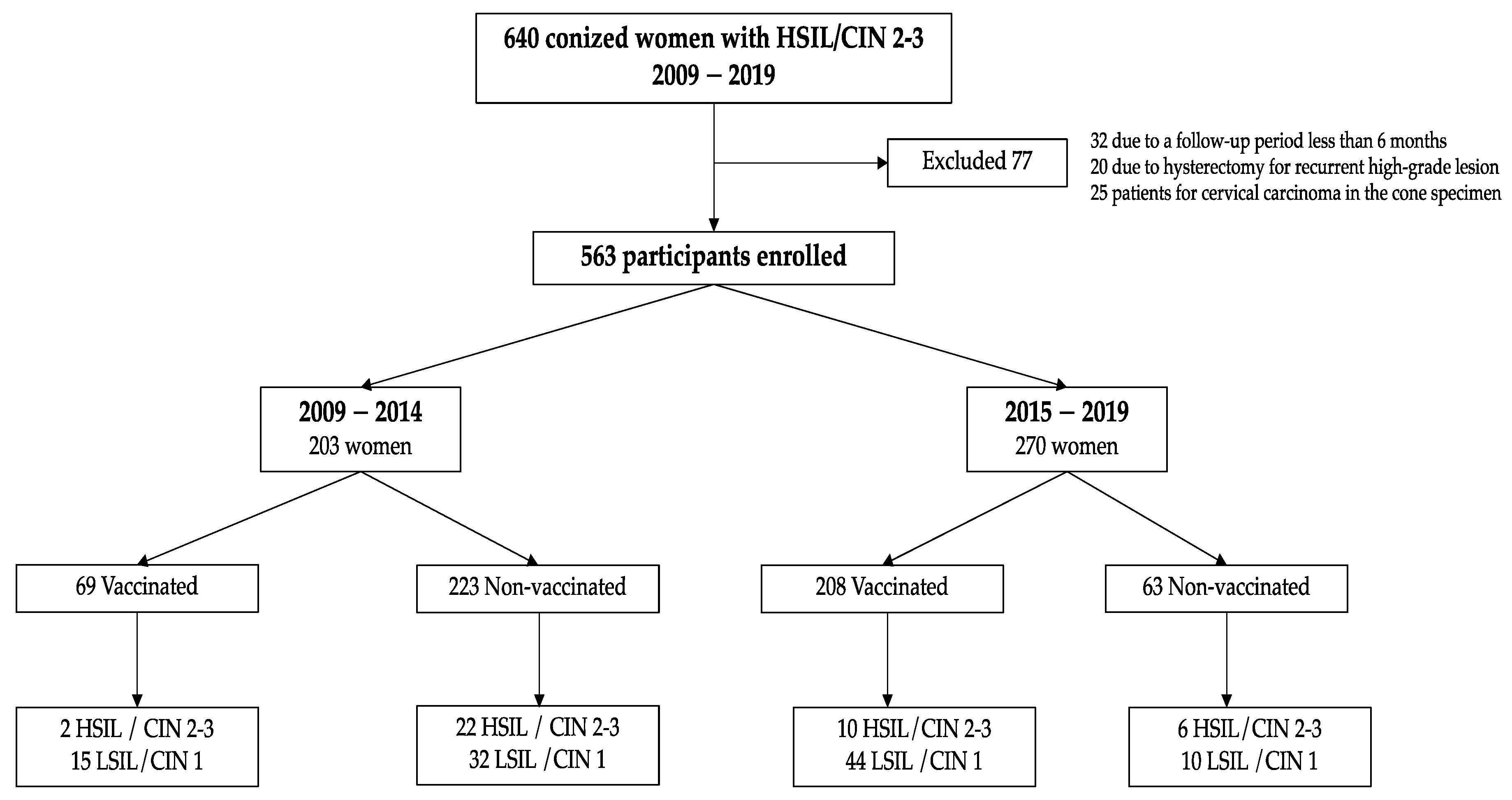
2.2. Sample Study
2.3. Pre-Surgical Evaluation
2.4. Surgical Treatment
2.5. Clinical Follow Up
2.6. Vaccination Status
2.7. Ethical Approval
2.8. Data Analysis
3. Results
3.1. Population Characteristics
3.2. Characteristics of Vaccinated and Non-Vaccinated Women
3.3. Vaccination Scheme
3.4. Results at 6-Month Follow-Up Visit
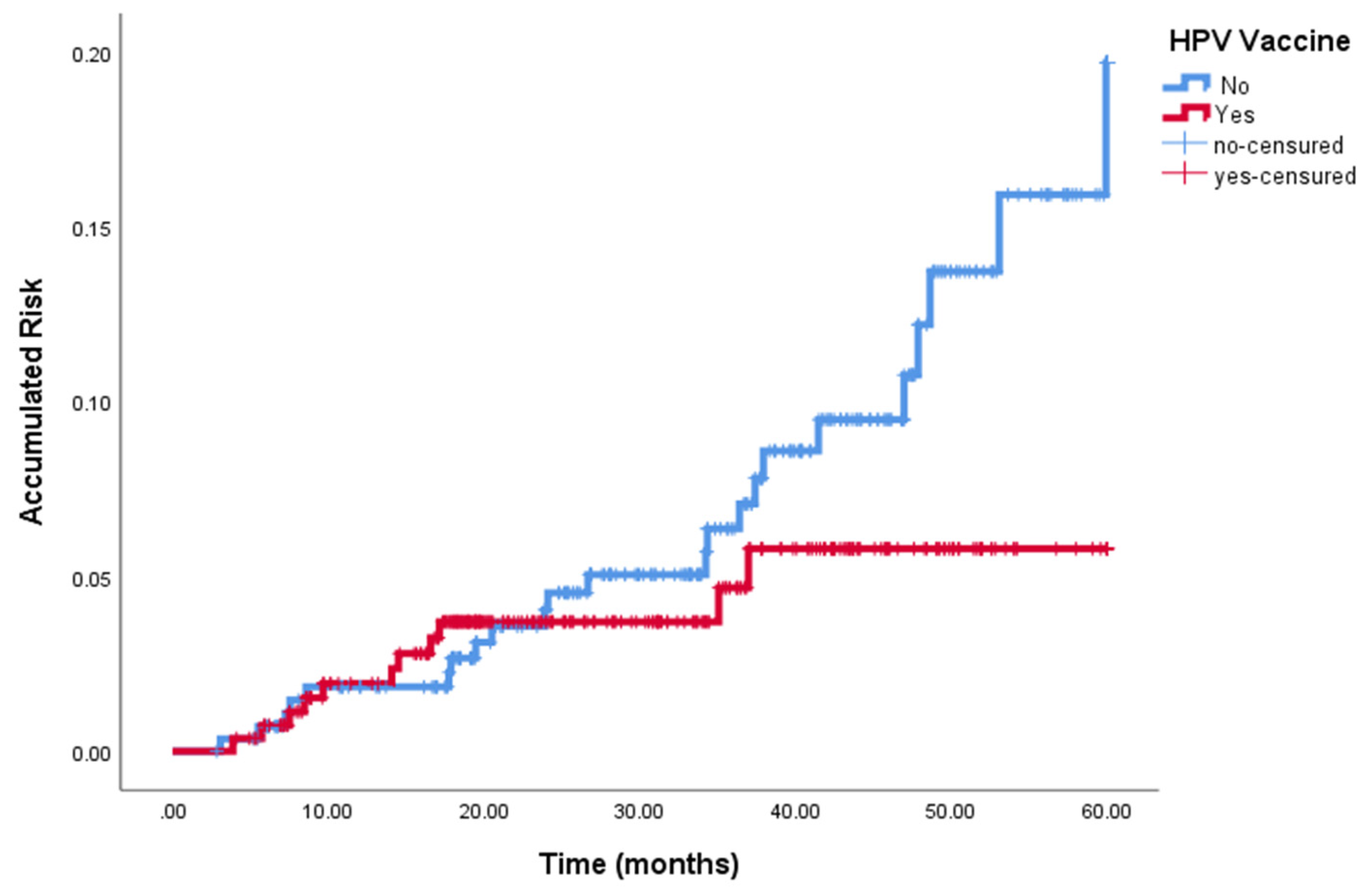
3.5. Clinical Outcome at the End of Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schlecht, N.F.; Kulaga, S.; Robitaille, J.; Ferreira, S.; Santos, M.; Miyamura, R.A.; Duarte-Franco, E.; Rohan, T.E.; Ferenczy, A.; Villa, L.L.; et al. Persistent human papillomavirus infection as a predictor of cervical intraepithelial neoplasia. JAMA 2001, 286, 3106–3114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dyne, E.A.; Henley, S.J.; Saraiya, M.; Thomas, C.C.; Markowitz, L.E.; Benard, V.B. Trends in Human Papillomavirus-Associated Cancers United States, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 918–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, P.; Kelly, D.; Medeiros, R. Viral Protection: A Four Step Plan for Eliminating HPV Cancers in Europe; European Cancer Organisation: Brussels, Belgium, 2020. [Google Scholar]
- Torné, A.; Secretaria, D.; Pino, M.; Alameda, F.; Andía, D.; Castellsagué, X. AEPCC-Guía: Prevención del Cáncer de Cuello de Útero; Publicaciones AEPCC: Madrid, Spain, 2015. [Google Scholar]
- Torné, A.; Secretaria, D.; Pino, M.; Autores, T.A.; Andía, D.; Bruni, L.; Centeno, C.; Coronado, P.; Cruz Quílez, J.; de la Fuente, J.; et al. AEPCC-Guía: Prevención Secundaria del Cancer de Cuello del Útero, Conducta Clínica Anteresultados Anormales de Las Pruebas de Cribado; Publicaciones AEPCC: Madrid, Spain, 2022. [Google Scholar]
- Ochoa-Carrillo, F.J. Virus del papiloma humano. Desde su descubrimiento hasta el desarrollo de una vacuna. Parte I/III. Gac. Mex. Oncol. 2014, 13, 308–315. [Google Scholar]
- Torné Bladé, A.; del Pino Saladrigues, M.; Cusidó Gimferrer, M.; Ponce Sebastià, J. Oncoguía SEGO: Prevención del cáncer de cuello de útero. In Guías de Práctica Clínica en Cáncer Ginecológico y Mamario; Publicaciones SEGO: Spain, 2014. [Google Scholar]
- Kang, W.D.; Choi, H.S.; Kim, S.M. Is vaccination with quadrivalent HPV vaccine after loop electrosurgical excision procedure effective in preventing recurrence in patients with high-grade cervical intraepithelial neoplasia (CIN2-3)? Gynecol. Oncol. 2013, 130, 264–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelardi, A.; Parazzini, F.; Martella, F.; Pieralli, A. SPERANZA project: HPV vaccination after treatment for CIN2+. Gynecol. Oncol. 2018, 151, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Velentzis, L.S.; Brotherton, J.M.L.; Canfell, K. Recurrent disease after treatment for cervical pre-cancer: Determining whether prophylactic HPVvaccination could play a role in prevention of secondary lesions. Climacteric 2019, 22, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Del Pino, M.; Martí, C.; Torras, I.; Henere, C.; Munmany, M.; Marimon, L.; Saco, A.; Torné, A.; Ordi, J. HPV Vaccination as Adjuvant to Conization in Women with Cervical Intraepithelial Neoplasia: A Study under Real-Life Conditions. Vaccines 2020, 8, 245. [Google Scholar] [CrossRef] [PubMed]
- Saftlas, A.F.; Spracklen, C.N.; Ryckman, K.K.; Stockdale, C.K.; Penrose, K.; Ault, K.; Rubenstein, L.M.; Pinto, L.A. Influence of a loop electrosurgical excision procedure (LEEP) on levels of cytokines in cervical secretions. J. Reprod. Immunol. 2015, 109, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.E.; Shvetsov, Y.B.; Thompson, P.J.; Hernandez, B.Y.; Zhu, X.; Wilkens, L.R.; Killeen, J.; Vo, D.D.; Moscicki, A.B.; Goodman, M.T. Cervical cytokines and clearance of incident human papillomavirus infection: Hawaii HPV cohort study. Int. J. Cancer 2013, 133, 1187–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jentschke, M.; Kampers, J.; Becker, J.; Sibbertsen, P.; Hillemanns, P. Prophylactic HPV vaccination after conization: A systematic review and meta-analysis. Vaccine 2020, 38, 6402–6409. [Google Scholar] [CrossRef] [PubMed]
- Servicio de Prevención de la Enfermedad. Calendario de Vacunación del Adulto; Dirección General de Salud Pública. Consejería de Sanidad Comunidad de Madrid: Madrid, Spain, 2019.
- Puig-Tintoré, L.M.; Cortés, J.; Castellsagué, X.; Torné, A.; Ordi, J.; de San José, S.; Alonso, I.; Cararach, M.; Vidart, J.A.; Alba, A. Prevención del cáncer de cuello uterino ante la vacunación frente al virus del papiloma humano. Prog. Obs. Ginecol. 2006, 49, 5–62. [Google Scholar]
- Genomica: Línea CLART® HPV [internet]. Available online: https://genomica.com/linea-clart-hpv (accessed on 14 April 2016).
- Gómez de la Rosa, A.G.; Quesada López-Fe, A.; Vilar Chesa, M.; Ferrer Machín, A.; Gimeno Gil, A.; Molina Bethancourt, A.; García Bello, M.Á.; Pérez-Méndez, L.I. Efficacy of Human Papillomavirus Vaccination 4 Years After Conization for High-Grade Cervical Neoplasia. J. Low. Genit. Tract Dis. 2021, 25, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Joura, E.A.; Giuliano, A.R.; Iversen, O.E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D.J.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef] [PubMed]
- The Future II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N. Engl. J. Med. 2007, 356, 1915–1927. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.T.; Palefsky, J.M. Human Papillomavirus Vaccination. Available online: https://www.uptodate.com/contents/human-papillomavirus-vaccination (accessed on 10 February 2022).
- Hildesheim, A.; Wacholder, S.; Catteau, G.; Struyf, F.; Dubin, G.; Herrero, R.; CVT Group. Efficacy of the HPV-16/18 vaccine: Final according to protocol results from the blinded phase of the randomized Costa Rica HPV-16/18 vaccine trial. Vaccine 2014, 32, 5087–5097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einstein, M.H.; Takacs, P.; Chatterjee, A.; Sperling, R.S.; Chakhtoura, N.; Blatter, M.M.; Lalezari, J.; David, M.P.; Lin, L.; Struyf, F.; et al. Comparison of long-term immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine and HPV-6/11/16/18 vaccine in healthy women aged 18–45 years: End-of-study analysis of a Phase III randomized trial. Hum. Vaccines Immunother. 2014, 10, 3435–3445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Dillner, J.; Tryggvadottir, L.; Munk, C.; Berger, S.; Enerly, E.; Hortlund, M.; Ágústsson, Á.I.; et al. Final analysis of a 14-year long-term follow-up study of the effectiveness and immunogenicity of the quadrivalent human papillomavirus vaccine in women from four nordic countries. EClinicalMedicine 2020, 23, 100401. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Clinical Characteristics | Vaccinated Group (%) (n = 277) | Non-Vaccinated Group (%) (n = 286) | p |
|---|---|---|---|
| Age | 0.060 | ||
| <35 years | 128 (46.2) | 109 (38.2) | |
| ≥35 years | 149 (53.8) | 176 (61.8) | |
| Smokers | 0.077 | ||
| No | 122 (44) | 118 (41.3) | |
| Yes | 61 (22) | 47 (16.4) | |
| Unknown | 94 (34) | 121 (42.3) | |
| History of pregnancies | 0.079 | ||
| No | 153 (55.4) | 133 (46.5) | |
| Yes | 123 (44.6) | 150 (55.4) | |
| Unknown | 1(0.3) | 3 (1.1) | |
| HPV Genotype | 0.187 | ||
| 16/18 HPV | 66 (23.8) | 39 (13.7) | |
| Other HR HPV | 51 (18.4) | 42 (14.7) | |
| Non-HR HPV | 11 (4.0) | 14 (4.9) | |
| Indication of conization | 0.908 | ||
| Persistent LSIN/CIN1 | 17 (6) | 16 (5.8) | |
| HSIL/CIN 2-3 | 266 (94) | 261 (94.2) | |
| Margin status | 0.270 | ||
| Negative | 221 (79.8) | 239 (83.5) | |
| Positive | 56 (20.2) | 47 (16.6) |
| Status at 6 Months | Vaccinated Group (%) (n = 277) | Non-Vaccinated Group (%) (n = 286) | p |
|---|---|---|---|
| Cytology | 0.490 | ||
| Negative | 239 (86.3) | 246 (86) | |
| LSIL/ASCUS | 34 (12.3) | 34 (12.3) | |
| HSIL | 4 (1.4) | 6 (2.1) | |
| HR-HPV testing | 0.707 | ||
| Positive | 83 (30) | 84 (29.4) | |
| Negative | 194 (70) | 202 (70.6) | |
| Cotesting | 0.657 | ||
| Negative | 184 (66.4) | 195 (68.2) | |
| Positive 1 | 93 (33.6) | 91 (31.8) |
| (A) 563 Conized Women with HSIL/CIN 2-3 | |||
| Vaccinated Women 277 (49.2%) | Non-Vaccinated Women 286 (50.8%) | OR (95% CI) | |
| No subsequent disease | 206 (74.4%) | 216 (75.5%) | 1 |
| Persistent/Recurrent | 59 | 42 | 1.5 (0.9–2.3) |
| LSIL/CIN 1 | (21.3%) | (14.7%) | |
| Persistent/Recurrent | 12 | 28 | 0.4 (0.2–0.9) 1 |
| HSIL/CIN 2-3 | (4.3%) | (9.8%) | |
| (B) 379 Women Treated for HSIL/CIN 2-3 with No Disease at 6-Month Follow-Up Visit | |||
|---|---|---|---|
| Vaccinated Women 184 (48.5%) | Non Vaccinated Women 195 (51.4%) | OR (95% CI) | |
| No subsequent disease | 161 (87.5%) | 182 (93.3%) | 1 |
| Persistent/Recurrent | 21 | 10 | 2.4 (1.1–5.2) 1 |
| LSIL/CIN 1 | (11.4%) | (5.1%) | |
| Persistent/Recurrent | 2 | 3 | 0.7 (0.1–4.5) |
| HSIL/CIN 2-3 | (1.1%) | (1.5%) | |
| Variable | Persistent/Recurrent HSIL/CIN 2-3 at the End of Follow-Up (Univariate Analysis) | ||
|---|---|---|---|
| HR | 95% CI | p | |
| Age | 0.281 | ||
| <35 years | 1 | ||
| ≥35 years | 0.70 | 0.37–1.37 | |
| Currently Smoke | 0.367 | ||
| No | 1 | ||
| Yes | 0.64 | 0.25–168 | |
| Presence of HR-HPV | 0.340 | ||
| No | 1 | ||
| Yes | 0.44 | 0.08–2.35 | |
| Margin in conization specimen | 0.475 | ||
| Negative | 1 | ||
| Positive | 1.30 | 0.63–2.70 | |
| Vaccination Status | 0.014 | ||
| No | 1 | ||
| Yes | 0.42 | 0.21–0.84 | |
| 6-month follow-up visit | 0.001 | ||
| Negative co-test | |||
| Positive co-test | 22.62 | 7.91–64.67 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casajuana-Pérez, A.; Ramírez-Mena, M.; Ruipérez-Pacheco, E.; Gil-Prados, I.; García-Santos, J.; Bellón-del Amo, M.; Hernández-Aguado, J.J.; de la Fuente-Valero, J.; Zapardiel, I.; Coronado-Martín, P.J. Effectiveness of Prophylactic Human Papillomavirus Vaccine in the Prevention of Recurrence in Women Conized for HSIL/CIN 2-3: The VENUS Study. Vaccines 2022, 10, 288. https://doi.org/10.3390/vaccines10020288
Casajuana-Pérez A, Ramírez-Mena M, Ruipérez-Pacheco E, Gil-Prados I, García-Santos J, Bellón-del Amo M, Hernández-Aguado JJ, de la Fuente-Valero J, Zapardiel I, Coronado-Martín PJ. Effectiveness of Prophylactic Human Papillomavirus Vaccine in the Prevention of Recurrence in Women Conized for HSIL/CIN 2-3: The VENUS Study. Vaccines. 2022; 10(2):288. https://doi.org/10.3390/vaccines10020288
Chicago/Turabian StyleCasajuana-Pérez, Andrea, Mar Ramírez-Mena, Estefanía Ruipérez-Pacheco, Inés Gil-Prados, Javier García-Santos, Mónica Bellón-del Amo, Juan J. Hernández-Aguado, Jesus de la Fuente-Valero, Ignacio Zapardiel, and Pluvio J. Coronado-Martín. 2022. "Effectiveness of Prophylactic Human Papillomavirus Vaccine in the Prevention of Recurrence in Women Conized for HSIL/CIN 2-3: The VENUS Study" Vaccines 10, no. 2: 288. https://doi.org/10.3390/vaccines10020288
APA StyleCasajuana-Pérez, A., Ramírez-Mena, M., Ruipérez-Pacheco, E., Gil-Prados, I., García-Santos, J., Bellón-del Amo, M., Hernández-Aguado, J. J., de la Fuente-Valero, J., Zapardiel, I., & Coronado-Martín, P. J. (2022). Effectiveness of Prophylactic Human Papillomavirus Vaccine in the Prevention of Recurrence in Women Conized for HSIL/CIN 2-3: The VENUS Study. Vaccines, 10(2), 288. https://doi.org/10.3390/vaccines10020288