
Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Participants
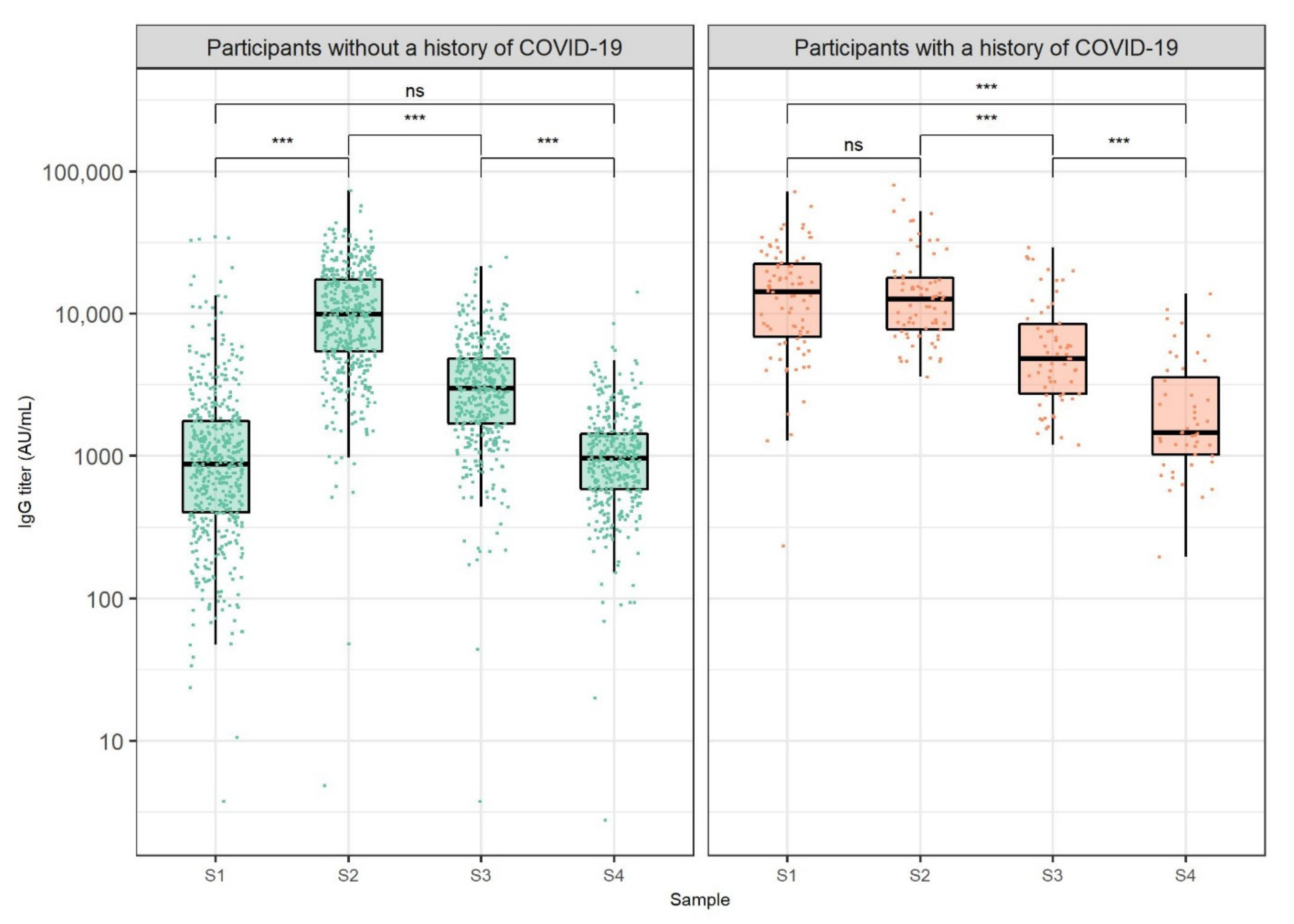
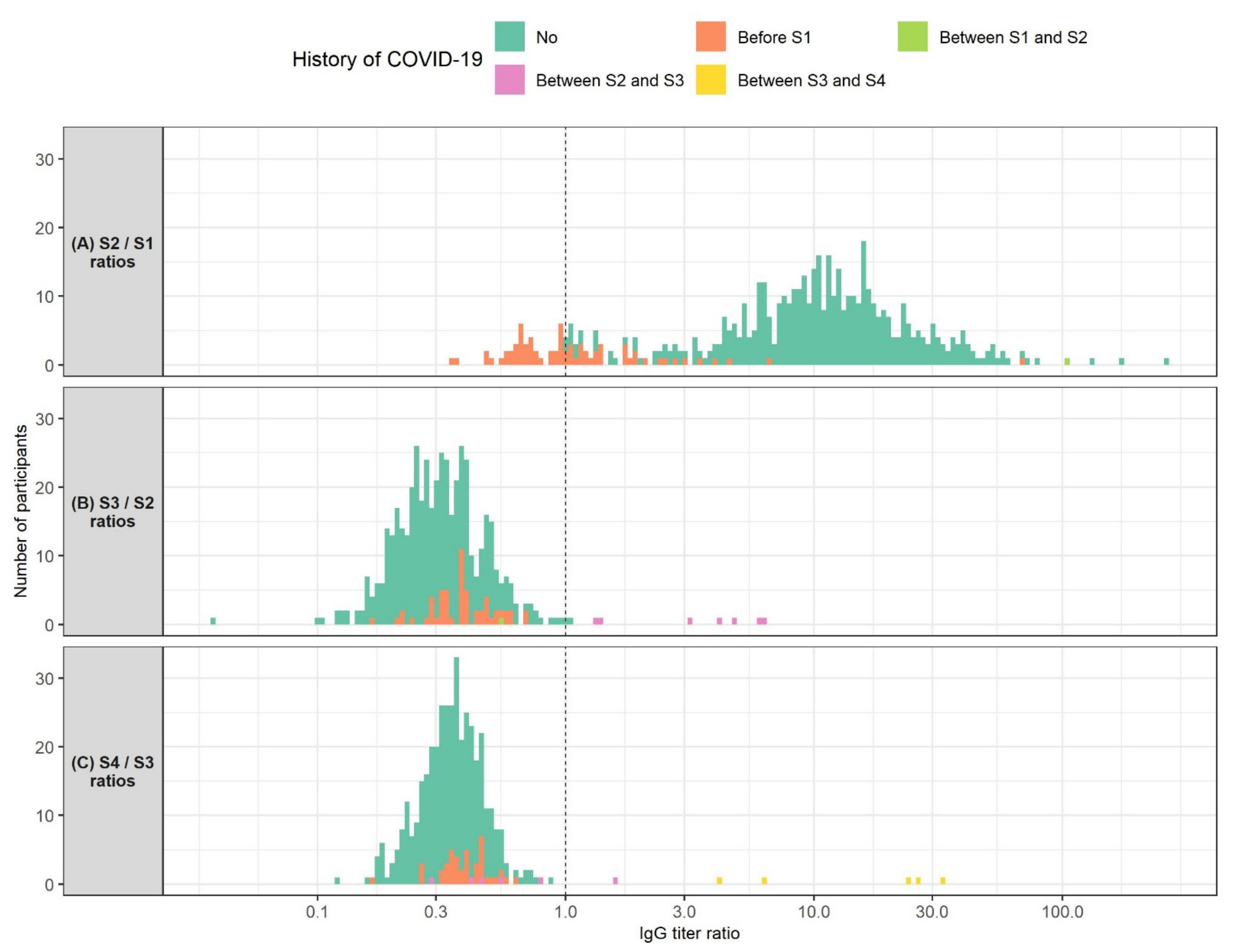
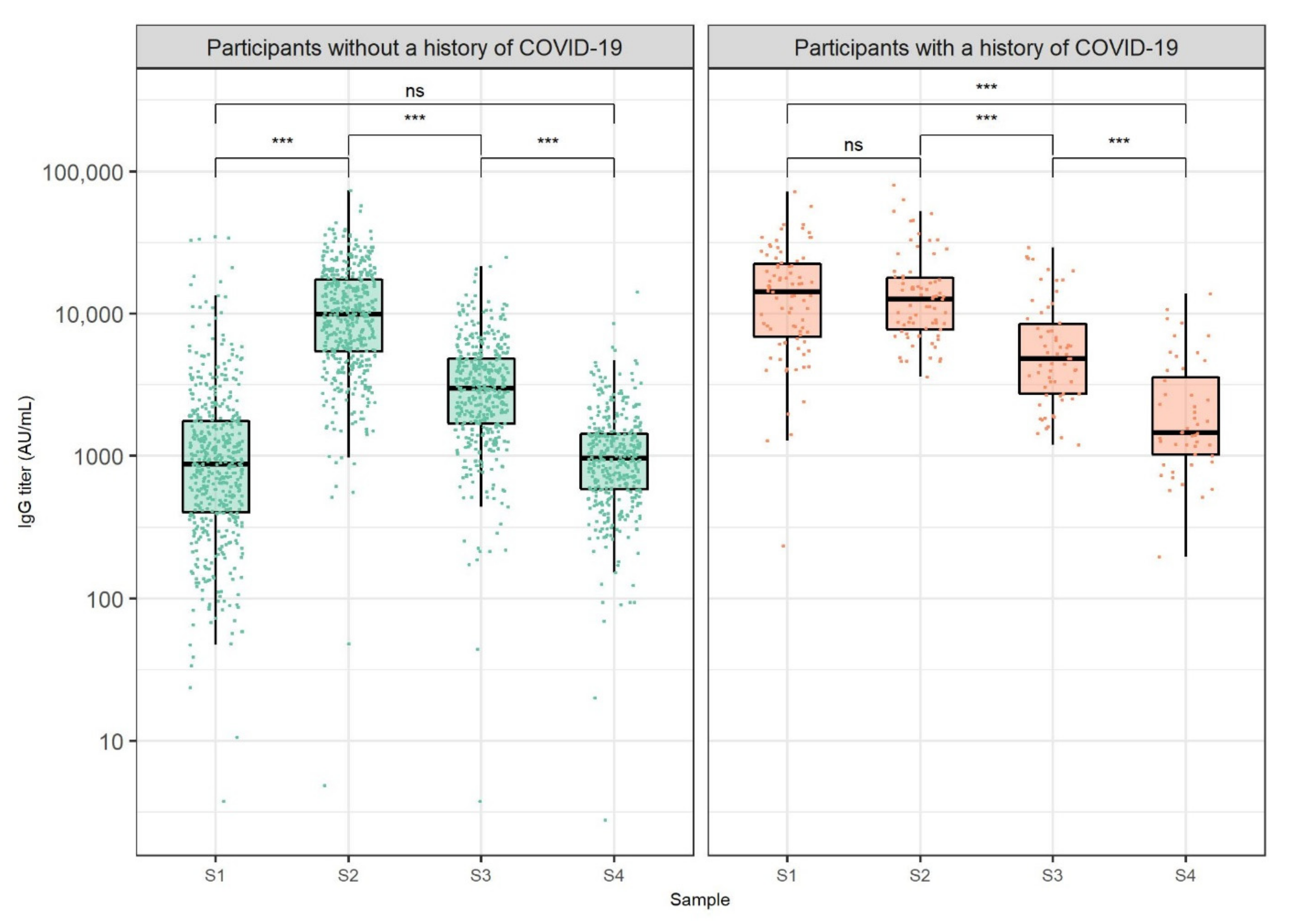
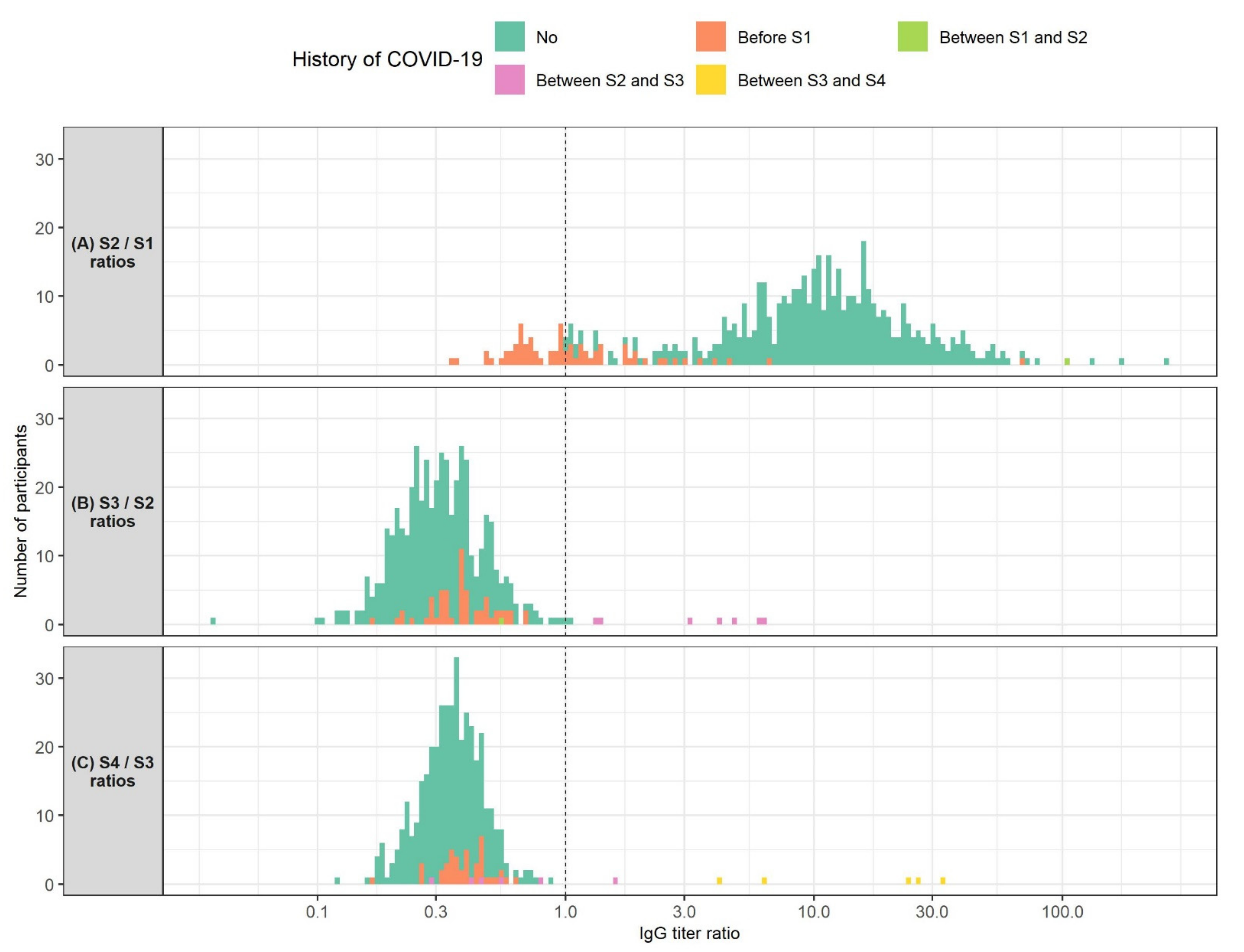
3.2. Anti-SARS-CoV-2 IgG Antibody Dynamics
3.3. Anti-SARS-CoV-2 IgG Antibody Levels by Age, Sex, and COVID-19 Patient Contact
3.4. Multiple Regression Models of Anti-SARS-CoV-2 IgG Antibody Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, A.; Singh, R.; Kaur, J.; Pandey, S.; Sharma, V.; Thakur, L.; Sati, S.; Mani, S.; Asthana, S.; Sharma, T.K.; et al. Wuhan to World: The COVID-19 Pandemic. Front. Cell Infect. Microbiol. 2021, 11, 596201. [Google Scholar] [CrossRef] [PubMed]
- Fergie, J.; Srivastava, A. Immunity to SARS-CoV-2: Lessons Learned. Front. Immunol. 2021, 12, 654165. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. The Promise and Peril of Antibody Testing for COVID-19. JAMA 2020, 323, 1881–1883. [Google Scholar] [CrossRef] [PubMed]
- Dopico, X.C.; Ols, S.; Loré, K.; Hedestam, G.B.K. Immunity to SARS-CoV-2 induced by infection or vaccination. J. Intern. Med. 2021, 291, 32–50. [Google Scholar] [CrossRef]
- Đaković Rode, O.; Kurolt, I.C.; Puljiz, I.; Čivljak, R.; Cetinić Balent, N.; Laškaj, R.; Tiljak, M.K.; Mikulić, R.; Markotić, A. Antibody response and the clinical presentation of patients with COVID-19 in Croatia: The importance of a two-step testing approach. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 261–268. [Google Scholar] [CrossRef]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Newton, J.N.; Farrar, J.; Diamond, I.; Rourke, E.; et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef]
- De Greef, J.; Scohy, A.; Zech, F.; Aboubakar, F.; Pilette, C.; Gerard, L.; Pothen, L.; Yildiz, H.; Belkhir, L.; Yombi, J.C. Determinants of IgG antibodies kinetics after severe and critical COVID-19. J. Med. Virol. 2021, 93, 5416–5424. [Google Scholar] [CrossRef]
- Muecksch, F.; Wise, H.; Batchelor, B.; Squires, M.; Semple, E.; Richardson, C.; McGuire, J.; Clearly, S.; Furrie, E.; Greig, N.; et al. Longitudinal serological analysis and neutralizing antibody levels in coronavirus disease 2019 convalescent patients. J. Infect. Dis. 2021, 223, 389–398. [Google Scholar] [CrossRef]
- Muecksch, F.; Wise, H.; Templeton, K.; Batchelor, B.; Squires, M.; McCance, K.; Jarvis, L.; Malloy, K.; Furrie, E.; Richardson, C.; et al. Longitudinal variation in SARS-CoV-2 antibody levels and emergence of viral variants: Implications for the ability of serological assays to predict immunity. Longitudinal variation in SARS-CoV-2 antibody levels and emergence of viral variants: Implications for the ability of serological assays to predict immunity. MedRxiv 2021. Preprint. [Google Scholar]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Narasimhan, M.; Mahimainathan, L.; Araj, E.; Clark, A.E.; Markantonis, J.; Green, A.; Xu, J.; SoRelle, J.A.; Alexis, C.; Fankhauser, K.; et al. Clinical evaluation of the Abbott Alinity SARS-CoV-2 spike-specific quantitative IgG and IgM assays among infected, recovered, and vaccinated groups. J. Clin. Microbiol. 2021, 59, e0038821. [Google Scholar] [CrossRef] [PubMed]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef]
- Sasikala, M.; Shashidhar, J.; Deepika, G.; Ravikanth, V.; Krishna, V.V.; Sadhana, Y.; Pragathi, K.; Reddy, D.N. Immunological memory and neutralizing activity to a single dose of COVID-19 vaccine in previously infected individuals. Int. J. Infect. Dis. 2021, 108, 183–186. [Google Scholar] [CrossRef]
- Vicenti, I.; Gatti, F.; Scaggiante, R.; Boccuto, A.; Zago, D.; Basso, M.; Dragoni, F.; Zazzi, M.; Parisi, S.G. Single-dose BNT162b2 mRNA COVID-19 vaccine significantly boosts neutralizing antibody response in health care workers recovering from asymptomatic or mild natural SARS-CoV-2 infection. Int. J. Infect. Dis. 2021, 108, 176–178. [Google Scholar] [CrossRef]
- Eyre, D.W.; Lumley, S.F.; Wei, J.; Cox, S.; James, T.; Justice, A.; Jesuthasan, G.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; et al. Quantitative SARS-CoV-2 anti-spike responses to Pfizer–BioNTech and Oxford–AstraZeneca vaccines by previous infection status. Clin. Microbiol. Infect. 2021, 27, 1516.e7–1516.e14. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Khatib, H.A.A.; Coyle, P.; Ayoub, H.H.; Kanaani, Z.A.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Pawłowska, M.; Rogalska-Płońska, M.; Bociąga-Jasik, M.; Kłos, K.; Piekarska, A.; Zarębska-Michaluk, D. Effect of COVID-19 on Anti-S Antibody Response in Healthcare Workers Six Months Post-Vaccination. Vaccines 2021, 9, 1325. [Google Scholar] [CrossRef] [PubMed]
- Carbonare, L.D.; Valenti, M.T.; Bisoffi, Z.; Piubelli, C.; Pizzato, M.; Accordini, S.; Mariotto, S.; Ferrari, S.; Minoia, A.; Bertacco, J.; et al. Serology study after BTN162b2 vaccination in participants previously infected with SARS-CoV-2 in two different waves versus naïve. Commun. Med. 2021, 1, 38. [Google Scholar] [CrossRef]
- Bayram, A.; Demirbakan, H.; Karadeniz, P.G.; Erdoğan, M.; Koçer, I. Quantitation of antibodies against SARS-CoV-2 spike protein after two doses of CoronaVac in healthcare workers. J. Med. Virol. 2021, 93, 5560–5567. [Google Scholar] [CrossRef]
- Amodio, E.; Capra, G.; Casuccio, A.; De Grazia, S.; Genovese, D.; Pizzo, S.; Calamusa, G.; Ferraro, D.; Giammanco, G.M.; Vitale, F.; et al. Antibodies responses to SARS-CoV-2 in a large cohort of vaccinated subjects and seropositive patients. Vaccines 2021, 9, 714. [Google Scholar] [CrossRef] [PubMed]
- Barchuk, A.; Shirokov, D.; Sergeeva, M.; Tursun zade, R.; Dudkina, O.; Tychkova, V.; Barabanova, L.; Skougarevskiy, D.; Danilenko, D. Evaluation of the performance of SARS CoV-2 antibody assays for a longitudinal population based study of COVID 19 spread in St. Petersburg, Russia. J. Med. Virol. 2021, 93, 5846–5852. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org/ (accessed on 2 December 2021).
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, T.G.; Zisaki, S.; Mitroulis, I.; Konstantinidou, E.; Kontekaki, E.G.; Romanidou, G.; Karvelas, A.; Nanousi, I.; Lazidis, L.; Cassimos, D.; et al. Levels of produced antibodies after vaccination with mrna vaccine; effect of previous infection with SARS-CoV-2. J. Clin. Med. 2021, 10, 2842. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; De Falco, T.; Oreni, L.; Pedroli, A.; Ridolfo, A.L.; Calabrò, E.; Carrozzo, G.; Bonazzetti, C.; Antinori, S.; Brucato, A. Impact of gender on patients hospitalized for SARS-COV-2 infection: A prospective observational study. J. Med. Virol. 2021, 93, 4597–4602. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Čivljak, R.; Markotić, A.; Capak, K. Earthquake in the time of COVID-19: The story from Croatia (CROVID-20). J. Glob. Health 2020, 10, 010349. [Google Scholar] [CrossRef] [PubMed]
- Amanat, F.; Stadlbauer, D.; Strohmeier, S.; Nguyen, T.H.O.; Chromikova, V.; McMahon, M.; Jiang, K.; Arunkumar, G.A.; Jurczyszak, D.; Polanco, J.; et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nat. Med. 2020, 26, 1033–1036. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Post- Vaccination IgG Titer | Anti-SARS-CoV-2 IgG Titer (AU/mL Median (IQR)) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (n = 587) | Pre-Vaccination COVID-19 History | Age (years) | Sex | Workplace with Patient Contacts | ||||||||
| Yes (n = 86) | No (n = 501) | 18–30 (n = 143) | 31–40 (n = 96) | 41–50 (n = 177) | 51–60 (n = 142) | >60 (n = 29) | Male (n = 105) | Female (n = 482) | Yes (n = 417) | No (n = 170) | ||
| S1 (N = 575) | 1050.8 (460.4–3138.5) | 14,280.2 (6913.4–22347.7) | 873.5 (402.9–1753.3) | 1951.9 (1064.9–4775.6) | 1140.4 (565.0–3484.6) | 851.2 (289.8–1986.3) | 751.7 (298.5–1654.8) | 460.2 (151.1–1161.0) | 931.6 (350.0–2274.8) | 1071.4 (494.0–3155.4) | 1140.4 (565.0–3484.6) | 851.2 (289.8–1986.3) |
| p-value | <0.001 | <0.001 | 0.087 | <0.001 | ||||||||
| p-adj # | <0.001 | <0.001 | 0.990 | 0.011 | ||||||||
| S2 * (N = 529) | 10,238.6 (5736.4–17,693.0) | 12,700.0 (7760.0–17,871.0) | 9927.2 (5461.3–17,414.2) | 12,700.0 (8586.0–19,509.0) | 10,645.3 (6052.1–17,870.9) | 8700.0 (4663.1–16,907.7) | 9133.8 (4747.7–16,546.6) | 8057.6 (2997.1–15,146.6) | 8300.0 (4003.0–17,441.0) | 10,465.3 (6009.5–17,600.1) | 10,645.3 (6052.1–17,870.9) | 8700.0 (4663.1–16,907.7) |
| p-value | 0.016 | <0.001 | 0.068 | 0.034 | ||||||||
| p-adj # | 0.176 | 0.006 | 0.990 | 0.544 | ||||||||
| S3 *,# (N = 491) | 3176.6 (1787.1–5247.2) | 4831.0 (2738.0–8480.0) | 2976.7 (1689.8–4838.2) | 4151.6 (2574.3–6179.4) | 3323.1 (2068.6–5475.1) | 2285.3 (1237.3–4795.7) | 2806.8 (1404.4–5171.9) | 2740.9 (1106.7–4583.0) | 2920.1 (1423.5–5026.2) | 3238.3 (1906.9–5255.8) | 3323.1 (2068.6–5475.1) | 2285.3 (1237.3–4795.7) |
| p-value | <0.001 | <0.001 | 0.470 | <0.001 | ||||||||
| p-adj # | <0.001 | <0.001 | 0.990 | 0.008 | ||||||||
| S4 * (N = 423) | 1025.6 (614.8–1508.0) | 1465.2 (1021.0–3559.1) | 966.0 (583.6–1431.8) | 1300.5 (948.7–1889.5) | 1069.7 (686.7–1671.6) | 819.4 (469.6–1411.5) | 928.5 (579.7–1420.2) | 816.6 (372.7–2156.6) | 1033.0 (543.0–6997.0) | 1025.6 (629.7–1494.1) | 1069.7 (686.7–1671.6) | 819.4 (469.6–1411.5) |
| p-value | <0.001 | <0.001 | 0.990 | <0.001 | ||||||||
| p-adj # | <0.001 | 0.003 | 0.990 | 0.002 | ||||||||
| Multiple Linear Regression Models | ||||||||||||
| Response variable | Best model formula | Adjusted R2 | p-value | Predictors’ significance in the model containing all predictors | ||||||||
| S1 | log(S1) = 11.190−1.277 × log (Age) + 2.217 × COVID-19 before vaccination (0 = no, 1 = yes) | 0.372 | <0.001 | COVID-19 before vaccination (p < 0.001), age (p < 0.001), patient contact (p = 0.136), sex (p = 0.166) | ||||||||
| S4 | log(S4) = 0.145 × log (S1) + 0.628 × log (S2) | 0.709 | <0.001 | S2 (p < 0.0001), S1 (p < 0.001), patient contact (p = 0.069), sex (p = 0.067), COVID-19 before vaccination (p = 0.224), age (p = 0.980) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Đaković Rode, O.; Bodulić, K.; Zember, S.; Cetinić Balent, N.; Novokmet, A.; Čulo, M.; Rašić, Ž.; Mikulić, R.; Markotić, A. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines 2022, 10, 153. https://doi.org/10.3390/vaccines10020153
Đaković Rode O, Bodulić K, Zember S, Cetinić Balent N, Novokmet A, Čulo M, Rašić Ž, Mikulić R, Markotić A. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines. 2022; 10(2):153. https://doi.org/10.3390/vaccines10020153
Chicago/Turabian StyleĐaković Rode, Oktavija, Kristian Bodulić, Sanja Zember, Nataša Cetinić Balent, Anđa Novokmet, Marija Čulo, Željka Rašić, Radojka Mikulić, and Alemka Markotić. 2022. "Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose" Vaccines 10, no. 2: 153. https://doi.org/10.3390/vaccines10020153
APA StyleĐaković Rode, O., Bodulić, K., Zember, S., Cetinić Balent, N., Novokmet, A., Čulo, M., Rašić, Ž., Mikulić, R., & Markotić, A. (2022). Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines, 10(2), 153. https://doi.org/10.3390/vaccines10020153