
COVID-19 and Influenza Coinfection Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample
 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
- Patient: age, race (White, Black, Hispanic, Native American, Asian, other), sex, insurance status (Medicare, Medicaid, private insurance, self-payment, no charge), median income based on patient’s zip code, and disposition.
- Hospital: location, teaching status, bed size, and region.
- Illness severity: length of stay (L.O.S.), mortality, hospitalization cost, comorbidities, mechanical ventilation, circulatory support, and vasopressor use.
- intubation and mechanical ventilation
- vasopressor use
- length of stay, the financial burden on healthcare, and resource utilization.
Statistical Analysis
3. Results
3.1. Demographics and Baseline Comorbidities
3.2. In-Hospital Outcomes
3.3. Propensity-Matched Demographics and Baseline Comorbidities
3.4. Propensity-Matched in-Hospital Outcomes
4. Discussion
4.1. Vaccination and Vaccine Hesitancy
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 23 October 2022).
- Hall, C.B.; Geiman, J.M.; Biggar, R.; Kotok, D.I.; Hogan, P.M.; Douglas Jr, R.G. Respiratory syncytial virus infections within families. N. Engl. J. Med. 1976, 294, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Munywoki, P.K.; Koech, D.C.; Agoti, C.N.; Lewa, C.; Cane, P.A.; Medley, G.F.; Nokes, D.J. The source of respiratory syncytial virus infection in infants: A household cohort study in rural Kenya. J. Infect. Dis. 2014, 209, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A. Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014, 134, e1474–e1502. [Google Scholar] [CrossRef] [PubMed]
- Diseases, C.o.I.; Committee, B.G.; Brady, M.T.; Byington, C.L.; Davies, H.D.; Edwards, K.M.; Jackson, M.A.; Maldonado, Y.A.; Murray, D.L.; Orenstein, W.A.; et al. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics 2014, 134, e620–e638. [Google Scholar]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Abbate, R.; Di Giuseppe, G.; Marinelli, P.; Angelillo, I.F. Knowledge, attitudes, and practices of avian influenza, poultry workers, Italy. Emerg. Infect. Dis. 2006, 12, 1762. [Google Scholar] [CrossRef]
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ. Res. 2020, 188, 109819. [Google Scholar] [CrossRef]
- Sameni, F.; Hajikhani, B.; Yaslianifard, S.; Goudarzi, M.; Owlia, P.; Nasiri, M.J.; Shokouhi, S.; Bakhtiyari, M.; Dadashi, M. COVID-19 and skin manifestations: An overview of case reports/case series and meta-analysis of prevalence studies. Front. Med. 2020, 7, 573188. [Google Scholar] [CrossRef]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef]
- Iqbal, M.M.; Abid, I.; Hussain, S.; Shahzad, N.; Waqas, M.S.; Iqbal, M.J. The effects of regional climatic condition on the spread of COVID-19 at global scale. Sci. Total Environ. 2020, 739, 140101. [Google Scholar] [CrossRef]
- Dadashi, M.; Khaleghnejad, S.; Abedi Elkhichi, P.; Goudarzi, M.; Goudarzi, H.; Taghavi, A.; Vaezjalali, M.; Hajikhani, B. COVID-19 and influenza co-infection: A systematic review and meta-analysis. Front. Med. 2021, 8, 971. [Google Scholar] [CrossRef] [PubMed]
- Alosaimi, B.; Naeem, A.; Hamed, M.E.; Alkadi, H.S.; Alanazi, T.; Al Rehily, S.S.; Almutairi, A.Z.; Zafar, A. Influenza co-infection associated with severity and mortality in COVID-19 patients. Virol. J. 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yue, H.; Zhang, M.; Xing, L.; Wang, K.; Rao, X.; Liu, H.; Tian, J.; Zhou, P.; Deng, Y.; Shang, J. The epidemiology and clinical characteristics of co-infection of SARS-CoV-2 and influenza viruses in patients during COVID-19 outbreak. J. Med. Virol. 2020, 92, 2870–2873. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bowe, B.; Maddukuri, G.; Al-Aly, Z. Comparative evaluation of clinical manifestations and risk of death in patients admitted to hospital with COVID-19 and seasonal influenza: Cohort study. BMJ 2020, 371, m4677. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, Y.H.; Chang, H.-H.; Choi, S.H.; Seo, H.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Park, J.Y.; Kim, C.H. Comparison of short-term mortality between mechanically ventilated patients with COVID-19 and influenza in a setting of sustainable healthcare system. J. Infect. 2020, 81, e76–e78. [Google Scholar] [CrossRef]
- Qu, J.; Chang, L.K.; Tang, X.; Du, Y.; Yang, X.; Liu, X.; Han, P.; Xue, Y. Clinical characteristics of COVID-19 and its comparison with influenza pneumonia. Acta Clin. Belg. 2020, 75, 348–356. [Google Scholar] [CrossRef]
- Zayet, S.; Lepiller, Q.; Zahra, H.; Royer, P.-Y.; Toko, L.; Gendrin, V.; Klopfenstein, T. Clinical features of COVID-19 and influenza: A comparative study on Nord Franche-Comte cluster. Microbes Infect. 2020, 22, 481–488. [Google Scholar] [CrossRef]
- Raedler, D.; Schaub, B. Immune mechanisms and development of childhood asthma. Lancet Respir. Med. 2014, 2, 647–656. [Google Scholar] [CrossRef]
- Yang, M.-J.; Rooks, B.J.; Le, T.-T.T.; Santiago, I.O.; Diamond, J.; Dorsey, N.L.; Mainous, A.G. Influenza vaccination and hospitalizations among COVID-19 infected adults. J. Am. Board Fam. Med. 2021, 34, S179–S182. [Google Scholar] [CrossRef]
- Tong, X.; Xu, X.; Lv, G.; Wang, H.; Cheng, A.; Wang, D.; Fan, G.; Zhang, Y.; Li, Y. Clinical characteristics and outcome of influenza virus infection among adults hospitalized with severe COVID-19: A retrospective cohort study from Wuhan, China. BMC Infect. Dis. 2021, 21, 1–8. [Google Scholar] [CrossRef]
- AHRQ. Healthcare Cost and Utilization Support. Available online: https://www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp (accessed on 23 October 2022).
- CMS.gov. Centers for Medicare and Medicaid Services. Available online: https://www.cms.gov/Medicare/Coding/ICD10 (accessed on 23 October 2022).
- Rosenbaum, P.R.; Rubin, D.B. Reducing bias in observational studies using subclassification on the propensity score. J. Am. Stat. Assoc. 1984, 79, 516–524. [Google Scholar] [CrossRef]
- Austin, P.C.; Mamdani, M.M. A comparison of propensity score methods: A case-study estimating the effectiveness of post-AMI statin use. Stat. Med. 2006, 25, 2084–2106. [Google Scholar] [CrossRef]
- Austin, P.C.; Grootendorst, P.; Anderson, G.M. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: A Monte Carlo study. Stat. Med. 2007, 26, 734–753. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Lu, J.; Liu, Y.; Zhang, Z.; Luo, L. Positive effects of COVID-19 control measures on influenza prevention. Int. J. Infect. Dis. 2020, 95, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.; Tsang, T.K.; Li, J.C.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ueda, P. Seasonal influenza activity during the SARS-CoV-2 outbreak in Japan. JAMA 2020, 323, 1969–1971. [Google Scholar] [CrossRef]
- Ozaras, R.; Cirpin, R.; Duran, A.; Duman, H.; Arslan, O.; Bakcan, Y.; Kaya, M.; Mutlu, H.; Isayeva, L.; Kebanlı, F. Influenza and COVID-19 coinfection: Report of six cases and review of the literature. J. Med. Virol. 2020, 92, 2657–2665. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. Impact of COVID-19 on the Changing Patterns of Respiratory Syncytial Virus Infections. Infect. Dis. Rep. 2022, 14, 558–568. [Google Scholar] [CrossRef]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; Van Herendael, B. Bronchiolitis in COVID-19 times: A nearly absent disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef]
- Olsen, S.J.; Winn, A.K.; Budd, A.P.; Prill, M.M.; Steel, J.; Midgley, C.M.; Kniss, K.; Burns, E.; Rowe, T.; Foust, A. Changes in influenza and other respiratory virus activity during the COVID-19 pandemic—United States, 2020–2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1013. [Google Scholar] [CrossRef]
- Zhou, X.; Ding, G.; Shu, T.; Fu, S.; Tong, W.; Tu, X.; Li, S.; Wu, D.; Qiu, Y.; Yu, J. The Outbreak of Coronavirus Disease 2019 Interfered with Influenza in Wuhan. Lancet 2020. preprint. [Google Scholar] [CrossRef]
- World Health Organization. Q&A: Influenza and COVID-19-Similarities and Differences; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novelcoronavirus-2019/question-and-answers-hub/qa-detail/qa-similarities-and-differencescovid-19-andinfluenza (accessed on 23 October 2022).
- Chotpitayasunondh, T.; Fischer, T.K.; Heraud, J.M.; Hurt, A.C.; Monto, A.S.; Osterhaus, A.; Shu, Y.; Tam, J.S. Influenza and COVID-19: What does co-existence mean? Influenza Other Respir. Viruses 2021, 15, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Wolters, F.; Grünberg, M.; Huber, M.; Kessler, H.H.; Prüller, F.; Saleh, L.; Fébreau, C.; Rahamat-Langendoen, J.; Thibault, V.; Melchers, W.J. European multicenter evaluation of Xpert® Xpress SARS-CoV-2/Flu/RSV test. J. Med. Virol. 2021, 93, 5798–5804. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Kim, J.-Y.; Shim, H.J.; Yun, S.A.; Jang, J.-H.; Huh, H.J.; Kim, J.-W.; Lee, N.Y. Comparison of the PowerChek SARS-CoV-2, Influenza A&B, RSV Multiplex Real-time PCR Kit and BioFire Respiratory Panel 2.1 for simultaneous detection of SARS-CoV-2, influenza A and B, and respiratory syncytial virus. J. Virol. Methods 2021, 298, 114304. [Google Scholar] [PubMed]
- Leung, E.C.-M.; Chow, V.C.-Y.; Lee, M.K.-P.; Tang, K.P.-S.; Li, D.K.-C.; Lai, R.W.-M. Evaluation of the xpert xpress SARS-CoV-2/Flu/RSV assay for simultaneous detection of SARS-CoV-2, influenza A and B viruses, and respiratory syncytial virus in nasopharyngeal specimens. J. Clin. Microbiol. 2021, 59, e02965-20. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.-L.; Li, Y.-Q.; Chen, X.; Lin, H.; Jiang, Z.-C.; Gu, D.-L.; Chen, X.; Tang, C.-X.; Xie, Z.-Q. Co-infection with common respiratory pathogens and SARS-CoV-2 in patients with COVID-19 pneumonia and laboratory biochemistry findings: A retrospective cross-sectional study of 78 patients from a single center in China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e929783-1–e929783-8. [Google Scholar] [CrossRef]
- John, A.L.S.; Rathore, A.P. Early insights into immune responses during COVID-19. J. Immunol. 2020, 205, 555–564. [Google Scholar] [CrossRef]
- van Riel, D.; Munster, V.J.; de Wit, E.; Rimmelzwaan, G.F.; Fouchier, R.A.; Osterhaus, A.D.; Kuiken, T. Human and avian influenza viruses target different cells in the lower respiratory tract of humans and other mammals. Am. J. Pathol. 2007, 171, 1215–1223. [Google Scholar] [CrossRef]
- Swets, M.C.; Russell, C.D.; Harrison, E.M.; Docherty, A.B.; Lone, N.; Girvan, M.; Hardwick, H.E.; Visser, L.G.; Openshaw, P.J.; Groeneveld, G.H. SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet 2022, 399, 1463–1464. [Google Scholar] [CrossRef]
- Our World in Data. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 23 October 2022).
- Wilcox, C.R.; Islam, N.; Dambha-Miller, H. Association between influenza vaccination and hospitalisation or all-cause mortality in people with COVID-19: A retrospective cohort study. BMJ Open Respir. Res. 2021, 8, e000857. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2021, 93, 64. [Google Scholar] [CrossRef] [PubMed]
- Kalantari, S.; Sadeghzadeh-Bazargan, A.; Ebrahimi, S.; Yassin, Z.; Faiz, S.H.R.; Kabir, A.; Baghestani, A.; Mashayekhi, F.; Bokharaei-Salim, F.; Goodarzi, A. The effect of influenza vaccine on severity of COVID-19 infection: An original study from Iran. Med. J. Islam. Repub. Iran 2021, 35, 114. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Liu, M.; Liu, J. The association between influenza vaccination and COVID-19 and its outcomes: A systematic review and meta-analysis of observational studies. Vaccines 2021, 9, 529. [Google Scholar] [CrossRef] [PubMed]
- Debisarun, P.A.; Gössling, K.L.; Bulut, O.; Kilic, G.; Zoodsma, M.; Liu, Z.; Oldenburg, M.; Rüchel, N.; Zhang, B.; Xu, C.-J. Induction of trained immunity by influenza vaccination-impact on COVID-19. PLoS Pathog. 2021, 17, e1009928. [Google Scholar] [CrossRef] [PubMed]
- Debisarun, P.A.; Struycken, P.; Domínguez-Andrés, J.; Moorlag, S.J.; Taks, E.; Gössling, K.L.; Ostermann, P.N.; Müller, L.; Schaal, H.; ten Oever, J. The effect of influenza vaccination on trained immunity: Impact on COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef]
- Long, B.R.; Michaelsson, J.; Loo, C.P.; Ballan, W.M.; Vu, B.-A.N.; Hecht, F.M.; Lanier, L.L.; Chapman, J.M.; Nixon, D.F. Elevated frequency of gamma interferon-producing NK cells in healthy adults vaccinated against influenza virus. Clin. Vaccine Immunol. 2008, 15, 120–130. [Google Scholar] [CrossRef]
- Covián, C.; Fernández-Fierro, A.; Retamal-Díaz, A.; Díaz, F.E.; Vasquez, A.E.; Lay, M.K.; Riedel, C.A.; González, P.A.; Bueno, S.M.; Kalergis, A.M. BCG-induced cross-protection and development of trained immunity: Implication for vaccine design. Front. Immunol. 2019, 10, 2806. [Google Scholar] [CrossRef]
- Arts, R.J.; Moorlag, S.J.; Novakovic, B.; Li, Y.; Wang, S.-Y.; Oosting, M.; Kumar, V.; Xavier, R.J.; Wijmenga, C.; Joosten, L.A. BCG vaccination protects against experimental viral infection in humans through the induction of cytokines associated with trained immunity. Cell Host Microbe 2018, 23, 89–100.e5. [Google Scholar] [CrossRef]
- Higgins, J.P.; Soares-Weiser, K.; López-López, J.A.; Kakourou, A.; Chaplin, K.; Christensen, H.; Martin, N.K.; Sterne, J.A.; Reingold, A.L. Association of BCG, DTP, and measles containing vaccines with childhood mortality: Systematic review. BMJ 2016, 355, i5170. [Google Scholar] [CrossRef]
- Yiangou, A.; Makin, S.; Cope, C.; Laycock, E. Preparing for a Challenging Winter 2020/21. 2020. Available online: https://abdn.pure.elsevier.com/en/publications/preparing-for-a-challenging-winter-202021 (accessed on 23 October 2022).
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’shaughnessy, F.; Passier, A.; Richardson, J.L. Vaccine willingness and impact of the COVID-19 pandemic on women’s perinatal experiences and practices—A multinational, cross-sectional study covering the first wave of the pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3367. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. COVID-19 vaccine in pregnant and lactating women: A review of existing evidence and practice guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Bratberg, J.; Lemay, V. COVID-19 and influenza vaccine hesitancy among college students. J. Am. Pharm. Assoc. 2021, 61, 709–714.e1. [Google Scholar] [CrossRef] [PubMed]
- Kopsidas, I.; Chorianopoulou, E.; Kourkouni, E.; Triantafyllou, C.; Molocha, N.-M.; Koniordou, M.; Maistreli, S.; Tsopela, C.-G.; Maroudi-Manta, S.; Filippou, D. COVID-19 pandemic impact on seasonal flu vaccination: A cross-sectional study. Pneumon 2021, 34, 8. [Google Scholar] [CrossRef]
- Sturm, L.; Kasting, M.L.; Head, K.J.; Hartsock, J.A.; Zimet, G.D. Influenza vaccination in the time of COVID-19: A national US survey of adults. Vaccine 2021, 39, 1921–1928. [Google Scholar] [CrossRef]
- Goldman, R.D.; McGregor, S.; Marneni, S.R.; Katsuta, T.; Griffiths, M.A.; Hall, J.E.; Seiler, M.; Klein, E.J.; Cotanda, C.P.; Gelernter, R. Willingness to vaccinate children against influenza after the Coronavirus disease 2019 pandemic. J. Pediatr. 2021, 228, 87–93.e2. [Google Scholar] [CrossRef]
- Bachtiger, P.; Adamson, A.; Chow, J.-J.; Sisodia, R.; Quint, J.K.; Peters, N.S. The impact of the COVID-19 pandemic on the uptake of influenza vaccine: UK-wide observational study. JMIR Public Health Surveill. 2021, 7, e26734. [Google Scholar] [CrossRef]
- Bonet-Esteve, A.; Muñoz-Miralles, R.; Gonzalez-Claramunt, C.; Rufas, A.M.; Cruz, X.P.; Vidal-Alaball, J. Influenza vaccination during the coronavirus pandemic: Intention to vaccinate among the at-risk population in the central Catalonia health region (VAGCOVID). BMC Fam. Pract. 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Groves, H.E.; Piché-Renaud, P.-P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg. Health-Am. 2021, 1, 100015. [Google Scholar]
- Soo, R.J.J.; Chiew, C.J.; Ma, S.; Pung, R.; Lee, V. Decreased influenza incidence under COVID-19 control measures, Singapore. Emerg. Infect. Dis. 2020, 26, 1933. [Google Scholar] [CrossRef]
- Feng, L.; Zhang, T.; Wang, Q.; Xie, Y.; Peng, Z.; Zheng, J.; Qin, Y.; Zhang, M.; Lai, S.; Wang, D. Impact of COVID-19 outbreaks and interventions on influenza in China and the United States. Nat. Commun. 2021, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ritz, N.; de Winter, J.P. COVID-19 in children: Patiently and critically evaluate the scientific evidence. Eur. J. Pediatr. 2020, 179, 1179–1180. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; MacKenzie, M.J.; Amegah, A.K.; Ezeh, A.; Gadanya, M.A.; Omigbodun, A.; Sarki, A.M.; Thistle, P.; Ziraba, A.K.; Stranges, S. The conundrum of low COVID-19 mortality burden in sub-Saharan Africa: Myth or reality? Glob. Healt: Sci. Pract. 2021, 9, 433–443. [Google Scholar] [CrossRef]
- Mulholland, K.; Kretsinger, K.; Wondwossen, L.; Crowcroft, N. Action needed now to prevent further increases in measles and measles deaths in the coming years. Lancet 2020, 396, 1782–1784. [Google Scholar] [CrossRef] [PubMed]
- Hatter, L.; Eathorne, A.; Hills, T.; Bruce, P.; Beasley, R. Respiratory syncytial virus: Paying the immunity debt with interest. Lancet Child Adolesc. Health 2021, 5, e44–e45. [Google Scholar] [CrossRef]
- Cohen, R.; Ashman, M.; Taha, M.-K.; Varon, E.; Angoulvant, F.; Levy, C.; Rybak, A.; Ouldali, N.; Guiso, N.; Grimprel, E. Pediatric Infectious Disease Group (GPIP) position paper on the immune debt of the COVID-19 pandemic in childhood, how can we fill the immunity gap? Infect. Dis. Now 2021, 51, 418–423. [Google Scholar] [CrossRef]


{kind=link}
| CHARACTERISTICS | Influenza Positive | Influenza Negative | p Value |
|---|---|---|---|
| N = 165,9040 | N = 4501 (0.27%) | N = 165,4539 (99.73%) | |
| SEX (Female) | 45.67% | 47.95% | 0.19 |
| Mean age years (SD) | 0.2 | ||
| Male | 62.88 (15.33) | 63.42 (16.2) | |
| Female | 65.2 (16.1) | 63.06 (18.8) | |
| age groups | <0.001 | ||
| ≥18–29 | 2.67% | 4.95% | |
| 30–49 | 14.44% | 16.81% | |
| 50–69 | 42.33% | 37.22% | |
| ≥70 | 40.56% | 41.02% | |
| RACE | 0.49 | ||
| Caucasians | 47.72% | 50.92% | |
| African American | 21.64% | 19.05% | |
| Hispanics | 21.53% | 21.47% | |
| Asian or Pacific Islander | 3.19% | 3.25% | |
| Native American | 1.03% | 1.03% | |
| Others | 4.9% | 4.28% | |
| median household income | <0.001 | ||
| <49,999$ | 41.89% | 34.1% | |
| 50,000–64,999$ | 26.8% | 27.2% | |
| 65,000–85,999$ | 18.02% | 22.17% | |
| >86,000$ | 13.29% | 16.53% | |
| insurance status | 0.003 | ||
| Medicare | 52.54% | 53.24% | |
| Medicaid | 11.45% | 15.17% | |
| Private | 32.23% | 27.63% | |
| Self-pay | 3.78% | 3.96% | |
| hospital division | <0.001 | ||
| New England | 1.33% | 3.8% | |
| Middle Atlantic | 8.67% | 14.63% | |
| East North Central | 7.78% | 15.56% | |
| West North Central | 4.22% | 6.75% | |
| South Atlantic | 30.56% | 20.05% | |
| East South Central | 10.33% | 6.7% | |
| West South Central | 22.78% | 14.3% | |
| Mountain | 5.22% | 6.92% | |
| Pacific | 9.11% | 11.3% | |
| hospital bedsize | 0.002 | ||
| Small | 30.11% | 24.31% | |
| Medium | 31.11% | 28.98% | |
| Large | 38.78% | 46.7% | |
| hospital teaching status | <0.001 | ||
| Rural | 16% | 9.79% | |
| Urban non-teaching | 21% | 18.65% | |
| Urban teaching | 63% | 71.56% | |
| comorbidities | |||
| CAD | 18.67% | 17.96% | 0.57 |
| CHF | 16.89% | 17.57% | 0.58 |
| HTN uncomplicated | 46.33% | 38.11% | <0.001 |
| HTN complicated | 24% | 27.07% | 0.03 |
| DM uncomplicated | 14.56% | 14.74% | 0.87 |
| DM complicated | 24.89% | 26.36% | 0.29 |
| Chronic pulmonary disease | 22.67% | 22% | 0.62 |
| Obesity | 25.67% | 25.64% | 0.98 |
| Smoking | 23.78% | 25.61% | 0.22 |
| AKI | 32.78% | 28.63% | 0.007 |
| AKI requiring HD | 3% | 2.44% | 0.31 |
| Stroke | 1.44% | 1.57% | 0.76 |
| Cardiac arrest | 3.44% | 2.79% | 0.25 |
| VARIABLE | Influenza Positive | Influenza Negative | p Value |
|---|---|---|---|
| Disposition | 0.44 | ||
| Home/Routine | 63.61% | 61.06% | |
| SNF/LTAC/Nursing home | 21.48% | 22.19% | |
| Home health | 13.95% | 15.4% | |
| AMA | 0.96% | 1.35% | |
| Vasopressor use | 2.33% | 2.65% | |
| Adjusted odds ratio 1 0.94 (95% CI 0.58–1.55) | 0.83 | ||
| Mechanical ventilation | 21.11% | 15.89% | |
| Adjusted odds ratio 1 1.42 (95% CI 1.19–1.69) | <0.001 | ||
| In-hospital mortality (N = 222,490) | 15.68% | 13.41% | |
| Adjusted odds ratio 1 1.29 (95% CI 1.05–1.58) | 0.01 | ||
| Mean total hospitalization charge ($) | 128,617$ | 91,735$ | |
| Adjusted total charge 1 39,045 $ higher | <0.001 | ||
| Mean length of stay (days) | 9.8 | 8.03 | |
| Adjusted length of stay 1 1.8 day higher | <0.001 | ||
| Variable | Influenza Positive | Influenza Negative | p Value |
|---|---|---|---|
| total died (222,490) | 706 | 221,784 | |
| sex | 0.65 | ||
| Male | 56.74% | 58.47% | |
| Female | 43.26% | 41.53% | |
| age groups | |||
| ≥18–29 | 0.71% | 0.6% | 0.86 |
| 30–49 | 5.67% | 4.93% | 0.7 |
| 50–69 | 30.5% | 30.52% | 0.99 |
| ≥70 | 63.12% | 63.94% | 0.84 |
| race | |||
| Caucasians | 44.68% | 51.51% | 0.13 |
| African American | 19.15% | 16.86% | 0.47 |
| Hispanics | 26.24% | 19.57% | 0.07 |
| Asian or Pacific Islander | 2.13% | 3.35% | 0.42 |
| Native American | 2.13% | 1.22% | 0.32 |
| Others | 4.26% | 4.4% | 0.93 |
| hospital teaching status | |||
| Rural | 12.77% | 7.81% | 0.03 |
| Urban non-teaching | 17.02% | 17.74% | 0.83 |
| Urban teaching | 70.21% | 74.45% | 0.28 |
| CHARACTERISTICS | Influenza Positive | Influenza Negative | p Value |
|---|---|---|---|
| N = 8170 | N = 4085 | N = 4085 | |
| SEX (Female) | 47% | 47.12% | 0.95 |
| Mean age years (SD) | 64.63 (10.01) | 64.67 (10.01) | 0.96 |
| age groups | 0.99 | ||
| ≥18–29 | 2.57% | 2.57% | |
| 30–49 | 13.34% | 13.22% | |
| 50–69 | 41.25% | 41.25% | |
| ≥70 | 42.84% | 42.96% | |
| race | 0.99 | ||
| Caucasians | 47.98% | 47.98% | |
| African American | 21.18% | 21.18% | |
| Hispanics | 21.91% | 21.91% | |
| Asian or Pacific Islander | 3.18% | 3.3% | |
| Native American | 0.98% | 0.73% | |
| Others | 4.77% | 4.9% | |
| median household income | 0.99 | ||
| <49,999$ | 42.47% | 42.35% | |
| 50,000–64,999$ | 26.81% | 26.81% | |
| 65,000–85,999$ | 17.75% | 17.87% | |
| >86,000$ | 12.97% | 12.97% | |
| insurance status | 0.99 | ||
| Medicare | 53.37% | 53.37% | |
| Medicaid | 11.38% | 11.38% | |
| Private | 31.46% | 31.58% | |
| Self-pay | 3.76% | 3.67% | |
| hospital division | <0.001 | ||
| New England | 12.2% | 75.4% | |
| Middle Atlantic | 9.06% | 21.91% | |
| East North Central | 7.96% | 1.1% | |
| West North Central | 4.16% | 0.37% | |
| South Atlantic | 30.48% | 0.37% | |
| East South Central | 10.53% | 0.12% | |
| West South Central | 22.64% | 0.37% | |
| Mountain | 4.9% | 0.37% | |
| Pacific | 9.06% | 0% | |
| hospital bedsize | 0.89 | ||
| Small | 29.62% | 30.48% | |
| Medium | 31.82% | 32.93% | |
| Large | 38.56% | 36.6% | |
| hospital teaching status | <0.001 | ||
| Rural | 15.91% | 3.67% | |
| Urban non-teaching | 21.42% | 13.34% | |
| Urban teaching | 62.67% | 82.99% |
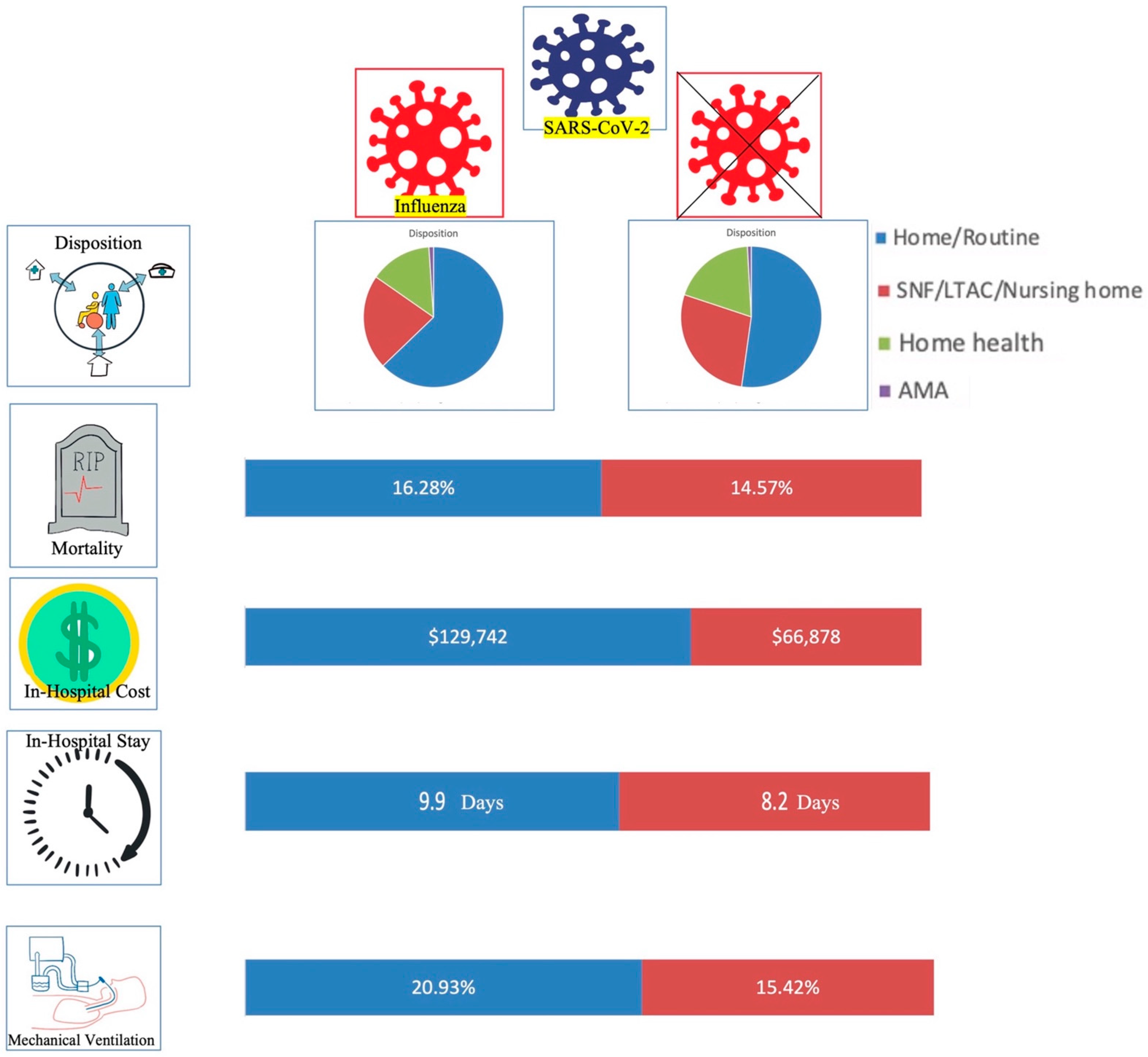
| VARIABLE | Influenza Positive | Influenza Negative | p Value |
|---|---|---|---|
| Disposition | 0.004 | ||
| Home/Routine | 62.82% | 52.21% | |
| SNF/LTAC/Nursing home | 21.85% | 27.88% | |
| Home health | 14.26% | 19.03% | |
| AMA | 1.06% | 0.88% | |
| Vasopressor use | 2.33% | 3.92% | |
| Adjusted odds ratio 1 2.12 (95% CI 0.7–6.42) | 0.18 | ||
| Mechanical ventilation | 20.93% | 15.42% | |
| Adjusted odds ratio 1 2.01 (95% CI 1.19–3.39) | 0.009 | ||
| In-hospital mortality (N = 1260) | 16.28% | 14.57% | |
| Adjusted odds ratio 1 2.09 (95% CI 1.03–4.24) | 0.04 | ||
| Mean total hospitalization charge ($) | 129,742$ | 66878$ | |
| Adjusted total charge 1 57,355 $ higher | 0.04 | ||
| Mean length of stay (days) | 9.9 | 8.2 | |
| Adjusted length of stay 1 2.7 day higher | 0.01 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garg, I.; Gangu, K.; Shuja, H.; Agahi, A.; Sharma, H.; Bobba, A.; Nasrullah, A.; Chourasia, P.; Pal, S.; Sheikh, A.B.; et al. COVID-19 and Influenza Coinfection Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample. Vaccines 2022, 10, 2159. https://doi.org/10.3390/vaccines10122159
Garg I, Gangu K, Shuja H, Agahi A, Sharma H, Bobba A, Nasrullah A, Chourasia P, Pal S, Sheikh AB, et al. COVID-19 and Influenza Coinfection Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample. Vaccines. 2022; 10(12):2159. https://doi.org/10.3390/vaccines10122159
Chicago/Turabian StyleGarg, Ishan, Karthik Gangu, Hina Shuja, Alireza Agahi, Harsh Sharma, Aniesh Bobba, Adeel Nasrullah, Prabal Chourasia, Suman Pal, Abu Baker Sheikh, and et al. 2022. "COVID-19 and Influenza Coinfection Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample" Vaccines 10, no. 12: 2159. https://doi.org/10.3390/vaccines10122159
APA StyleGarg, I., Gangu, K., Shuja, H., Agahi, A., Sharma, H., Bobba, A., Nasrullah, A., Chourasia, P., Pal, S., Sheikh, A. B., & Shekhar, R. (2022). COVID-19 and Influenza Coinfection Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample. Vaccines, 10(12), 2159. https://doi.org/10.3390/vaccines10122159