
Immunogenicity against the Omicron Variant after mRNA-Based COVID-19 Booster Vaccination in Medical Students Who Received Two Primary Doses of the mRNA-1273 Vaccine
 ,
,  and
and
Abstract
:1. Introduction
2. Methods
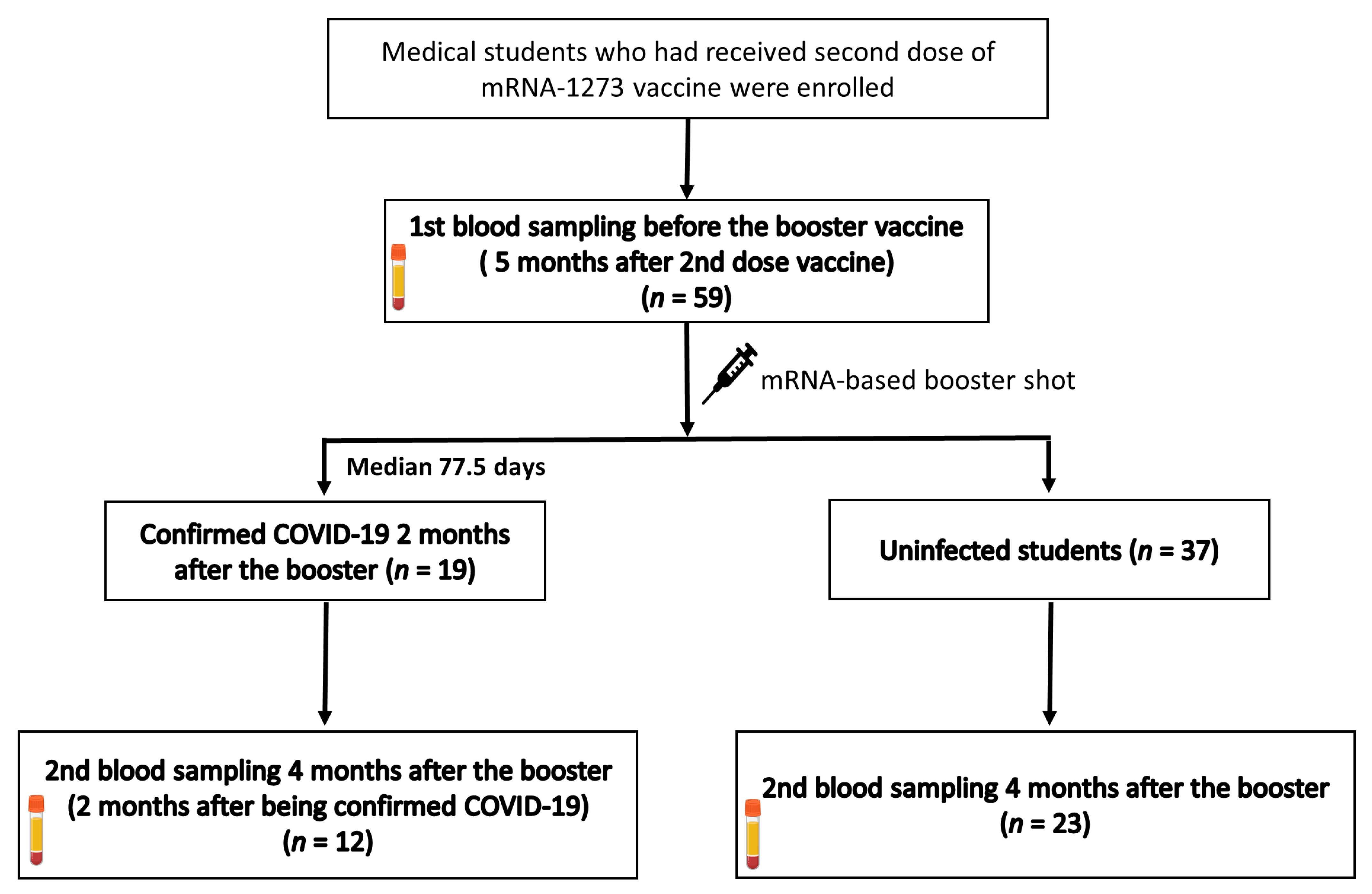
2.1. Study Design
2.2. Measurement of SARS-CoV-2 Spike-Specific Immunoglobulin G
2.3. Measurement of Neutralizing Antibody Response
2.4. Measurement of SARS-CoV-2-Specific Cellular Response
2.5. Statistical Analysis
3. Results
3.1. Study Population
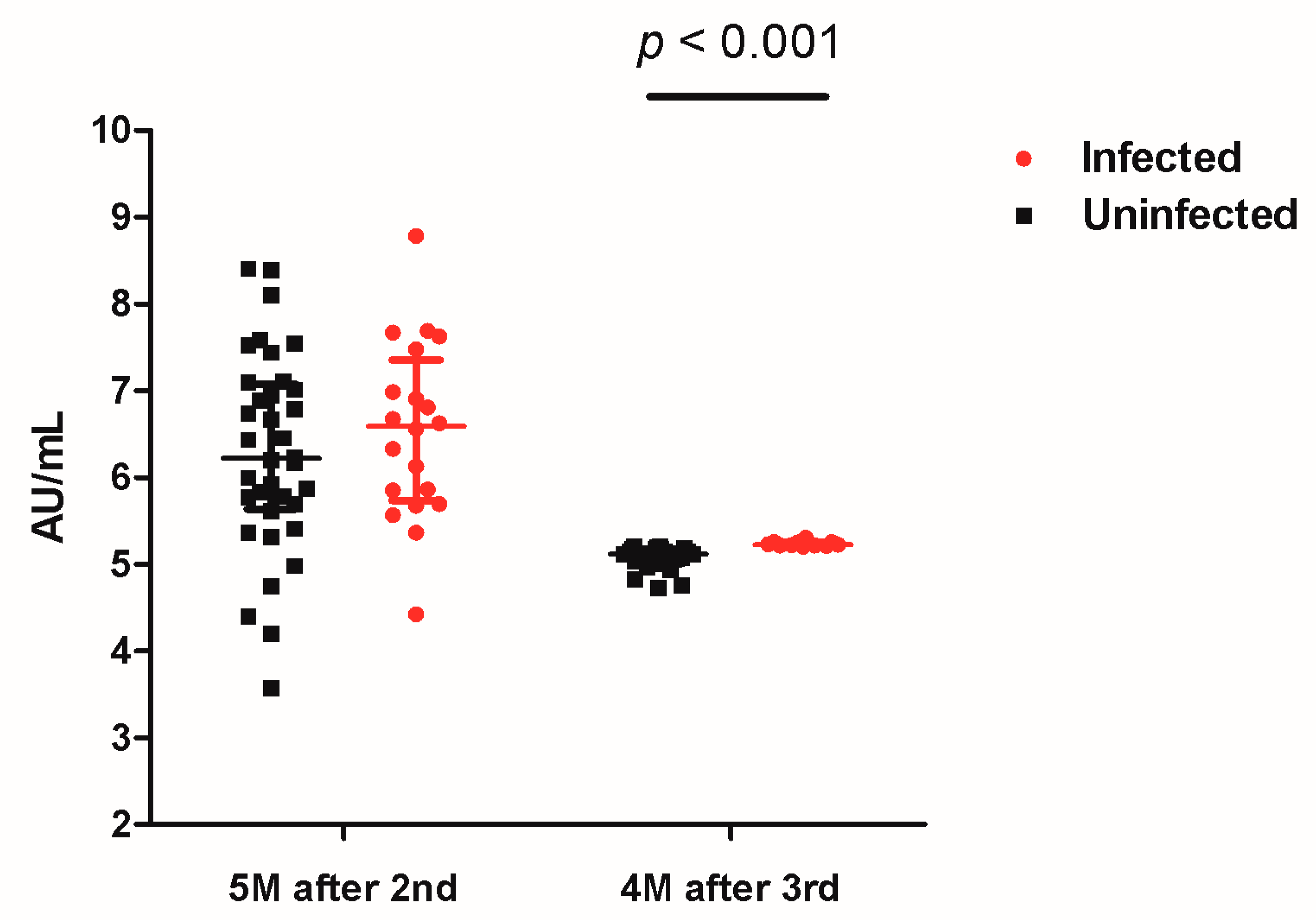
3.2. SARS-CoV-2 Spike-Specific IgG
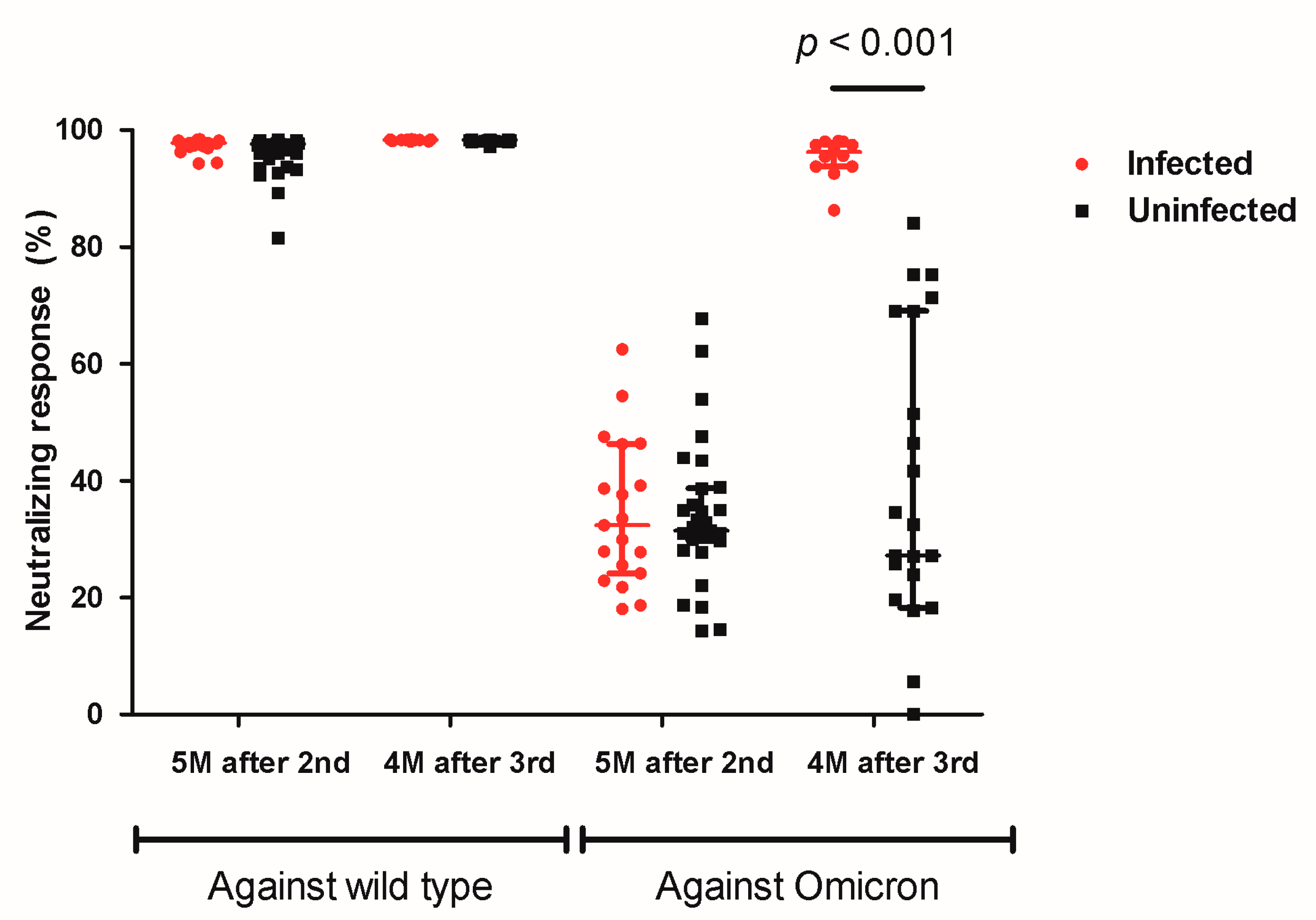
3.3. Neutralizing Antibody Response against Wild-Type and OMICRON Variant
3.4. SARS-CoV-2-Specific Cellular Response
3.5. Vaccine Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saxena, S.K.; Kumar, S.; Ansari, S.; Paweska, J.T.; Maurya, V.K.; Tripathi, A.K.; Abdel-Moneim, A.S. Characterization of the novel SARS-CoV-2 Omicron (B.1.1.529) variant of concern and its global perspective. J. Med. Virol. 2022, 94, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat. Med. 2022, 28, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Lassaunière, R.; Polacek, C.; Frische, A.; Boding, L.; Sækmose, S.G.; Rasmussen, M.; Fomsgaard, A. Neutralizing Antibodies Against the SARS-CoV-2 Omicron Variant (BA.1) 1 to 18 Weeks After the Second and Third Doses of the BNT162b2 mRNA Vaccine. JAMA Netw. Open 2022, 5, e2212073. [Google Scholar] [CrossRef] [PubMed]
- Um, J.; Choi, Y.Y.; Kim, G.; Kim, M.K.; Lee, K.S.; Sung, H.K.; Kim, B.C.; Lee, Y.K.; Jang, H.C.; Bang, J.H.; et al. Booster BNT162b2 COVID-19 Vaccination Increases Neutralizing Antibody Titers Against the SARS-CoV-2 Omicron Variant in Both Young and Elderly Adults. J. Korean Med. Sci. 2022, 37, e70. [Google Scholar] [CrossRef] [PubMed]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health (Oxf.) 2021, 43, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 2021, 149, e132. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.J.; Choi, S.H.; Park, J.Y.; Song, J.S.; Chung, J.W.; Choi, S.T. SARS-CoV-2 Omicron escapes mRNA vaccine booster-induced antibody neutralisation in patients with autoimmune rheumatic diseases: An observational cohort study. Ann. Rheum. Dis. 2022, 81, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Park, S.; Kim, J.Y.; Kim, S.; Jee, Y.; Kim, S.H. Comparison of Waning Neutralizing Antibody Responses Against the Omicron Variant 6 Months After Natural SARS-CoV-2 Infection (With/Without subsequent COVID-19 Vaccination) Versus 2-dose COVID-19 Vaccination. Clin. Infect. Dis. 2022, ciac435. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Choe, Y.J.; Jeong, H.; Kim, M.; Kim, S.; Yoo, H.; Park, K.; Kim, C.; Choi, S.; Sim, J.; et al. Importation and Transmission of SARS-CoV-2 B.1.1.529 (Omicron) Variant of Concern in Korea, November 2021. J. Korean Med. Sci. 2021, 36, e346. [Google Scholar] [CrossRef] [PubMed]
- WHOCOVID-19 Dashboard. Available online: https://covid19whoint/region/wpro/country/kr (accessed on 13 November 2022).
- Pajon, R.; Doria-Rose, N.A.; Shen, X.; Schmidt, S.D.; O’Dell, S.; McDanal, C.; Feng, W.; Tong, J.; Eaton, A.; Maglinao, M.; et al. SARS-CoV-2 Omicron Variant Neutralization after mRNA-1273 Booster Vaccination. N. Engl. J. Med. 2022, 386, 1088–1091. [Google Scholar] [CrossRef] [PubMed]
- Barouch, D.H. COVID-19 vaccines—Immunity, Variants, Boosters. N. Engl. J. Med. 2022, 387, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef] [PubMed]
- Straus, W.; Urdaneta, V.; Esposito, D.B.; Mansi, J.A.; Rodriguez, C.S.; Burton, P.; Vega, J.M. Analysis of Myocarditis Among 252 Million mRNA-1273 Recipients Worldwide. Clin. Infect. Dis. 2022, ciac446. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Side Effects | Second Dose (n = 56) | Booster (n = 35) | p Value |
|---|---|---|---|
| Fever | 41 (73.2) | 8 (22.9) | <0.001 |
| Headache | 26 (46.4) | 8 (22.9) | 0.02 |
| Chilling sense | 36 (64.3) | 9 (25.7) | <0.001 |
| Nausea | 6 (10.7) | 2 (5.7) | 0.71 |
| Vomiting | 1 (1.8) | 0 | >0.99 |
| Diarrhea | 1 (1.8) | 2 (5.7) | 0.56 |
| Myalgia arthralgia | 40 (71.4) | 18 (51.4) | 0.054 |
| General weakness | 36 (64.3) | 14 (40.0) | 0.02 |
| Injection site pain | 43 (76.8) | 18 (51.4) | 0.01 |
| Injection site tenderness | 12 (21.4) | 4 (11.4) | 0.22 |
| Injection site swelling | 11 (19.6) | 5 (14.3) | 0.51 |
| Needs nonsteroidal anti-inflammatory drugs or acetaminophens | 44 (78.6) | 21 (60.0) | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, H.; Lee, J.; Minn, K.; Lee, J.; Yun, S.; Park, J.H.; Kim, M.-C.; Choi, S.-H.; Chung, J.-W. Immunogenicity against the Omicron Variant after mRNA-Based COVID-19 Booster Vaccination in Medical Students Who Received Two Primary Doses of the mRNA-1273 Vaccine. Vaccines 2022, 10, 2102. https://doi.org/10.3390/vaccines10122102
Chung H, Lee J, Minn K, Lee J, Yun S, Park JH, Kim M-C, Choi S-H, Chung J-W. Immunogenicity against the Omicron Variant after mRNA-Based COVID-19 Booster Vaccination in Medical Students Who Received Two Primary Doses of the mRNA-1273 Vaccine. Vaccines. 2022; 10(12):2102. https://doi.org/10.3390/vaccines10122102
Chicago/Turabian StyleChung, Hyemin, Jongsung Lee, Kyungrok Minn, Jiyoung Lee, Soyoung Yun, Joung Ha Park, Min-Chul Kim, Seong-Ho Choi, and Jin-Won Chung. 2022. "Immunogenicity against the Omicron Variant after mRNA-Based COVID-19 Booster Vaccination in Medical Students Who Received Two Primary Doses of the mRNA-1273 Vaccine" Vaccines 10, no. 12: 2102. https://doi.org/10.3390/vaccines10122102
APA StyleChung, H., Lee, J., Minn, K., Lee, J., Yun, S., Park, J. H., Kim, M.-C., Choi, S.-H., & Chung, J.-W. (2022). Immunogenicity against the Omicron Variant after mRNA-Based COVID-19 Booster Vaccination in Medical Students Who Received Two Primary Doses of the mRNA-1273 Vaccine. Vaccines, 10(12), 2102. https://doi.org/10.3390/vaccines10122102