1. Introduction
Since the mid-20th century, vaccination has been an essential component of national strategies to eradicate or reduce the impact of infectious diseases [
1]. After the Severe Acute Respiratory Syndrome (SARS) coronavirus (COVID-19) pandemic commenced in December 2019, the Australian Commonwealth Government, along with state and territory governments, employed comprehensive social restrictions to contain disease spread and minimise healthcare system pressures [
2]. As of November 2022, the pandemic is estimated to have resulted in 642 million confirmed cases and 6.63 million deaths [
3]; in Australia, this has been estimated to be 10.7 million cases and 16,119 deaths (i.e., approximately 0.15% of all cases) [
4]. The pandemic has led not only to significant adverse health outcomes and healthcare system strains, but global contraction in economic activity, with Australia experiencing its first recession since 1991 [
5]. This subsequently led Australia’s Government to enact large-scale fiscal policy measures to support its economy and healthcare system [
6].
Subsequently, like other countries, Australia’s Government sought to rapidly acquire and distribute vaccines, bypassing established health technology assessment (HTA) procurement processes [
7] and using Advanced Purchase Agreements to secure vaccine supply [
8,
9]. HTA is a formal process that uses explicit methods to determine the value of a health technology, with considerations of value ‘often including clinical effectiveness, safety, costs and economic implications, ethical, social, cultural and legal issues, organizational and environmental aspects, as well as wider implications for the patient, relatives, caregivers, and the population’ [
10]. Over time, it has become increasingly used by independent agencies and payers such as governments to inform, recommend or make funding decisions by evaluating health intervention (including vaccines) ‘value for money’ relative to existing medical management approaches. HTA is well established in Australia [
11], the United Kingdom (UK) [
12], Europe [
13], Canada [
14], some parts of the United States healthcare system [
15], and increasingly, in Asia [
16].
In Australia, vaccines reimbursement follows a lengthy, multi-stepped process. After initial clinical consideration by the Australian Technical Advisory Group on Immunisation [
17], the Pharmaceutical Benefits Advisory Committee (PBAC), an independent expert advisory body, undertakes formal HTA [
18]. A positive PBAC recommendation, with cost-effectiveness a key quantitative PBAC decision making criteria [
19], followed by Commonwealth Government approval, is required before a vaccine can be listed on the National Immunisation Program [
20] for subsidised use by eligible patients. As of November 2022, the PBAC has not considered COVID-19 vaccination funding submissions. However, it has considered COVID-19 therapies for mild-to-moderate patients at risk of hospitalisation, as well as pre-exposure prophylaxis for individuals who are severely immunocompromised or for whom available funded vaccinations were contraindicated [
21,
22,
23]. In the UK, HTA advice processes have been used to inform COVID-19 vaccine coverage recommendations [
24], albeit without inclusion of cost-effectiveness analysis (in contrast to prior vaccine funding decisions [
25]). As the world moves from pandemic to pandemic recovery, it remains to be seen when and how COVID-19 vaccines will be evaluated as a manner of course through established HTA processes.
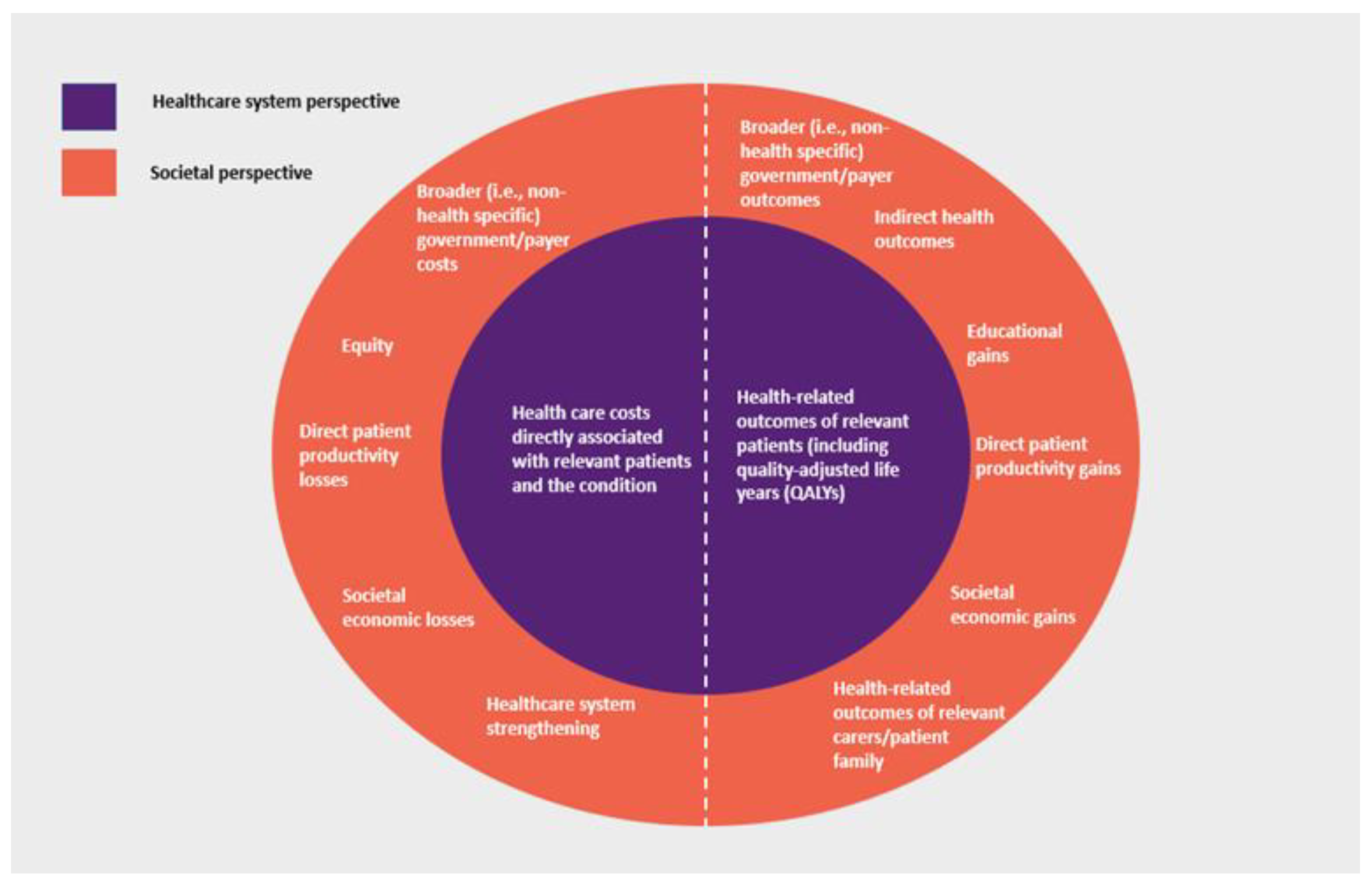
A key methodological consideration of HTA is defining the evaluation ‘perspective’, i.e., the scope of costs and outcomes considered. While there may be practical variations, HTA generally takes one of two approaches, reflecting where costs and outcomes occur and whether they are directly or indirectly attributable to the condition and medical intervention being considered. The narrower ‘healthcare system perspective’ generally includes health care costs (including those incurred by the patient) and health-related outcomes directly attributable to the treatment, disease and patient being considered. In many countries, this perspective reflects the government role as ‘payer’ for health care (i.e., a ‘payer perspective’). In addition to these, the broader ‘societal perspective’ may also consider additional costs and outcomes that impact patients, family and carers of patients, governments and payers, and society overall, with potentially various elements of value being able to be considered [
26] (
Figure 1).
HTA methods in many countries, including Australia, generally only consider direct patient health outcomes and healthcare system-related costs directly associated with the patient and condition, with broader impacts on society not necessarily included in ‘base case’ analysis [
27,
28]. Therefore, depending on the relative distribution or ‘location’ of costs and outcomes for a particular condition and treatment, this may affect HTA economic evaluation outcomes and ultimately, societal resource allocation decisions.
This is especially relevant for vaccines. Infectious diseases, including COVID-19, have unique characteristics that must be considered when valuing vaccine interventions: disease transmissibility, evolution in their nature over time, large-scale population health outcome impacts and as COVID-19 has demonstrated, the risk of widespread societal effects, including those which are felt beyond the immediate patient. Similarly, the positive effects of vaccines may be felt beyond the scope of health and the healthcare system and be long term in nature.
We believe, therefore, that as a HTA methodological consideration, an appropriate perspective is critical to ensuring the conferral of the broad range of positive effects and outcomes of vaccines to society. With the COVID-19 pandemic, it is timely to consider the broader economic and societal impacts of vaccines and the importance of considering these in HTA. This study estimates the economic impacts of the COVID-19 pandemic and the subsequent mitigating effects of population-wide COVID vaccination in Australia. Current HTA approaches for assessing the value of vaccines (both for COVID-19 vaccines and more generally), along with recent efforts to consider broader HTA valuation frameworks to capture the true value of medical interventions, are then considered. In doing so, we demonstrate the value of vaccines extends beyond the traditional dimensions of direct health and healthcare system impacts, that current HTA value frameworks are too limited and that they should be expanded to capture the true broader societal value of vaccines.
4. Discussion
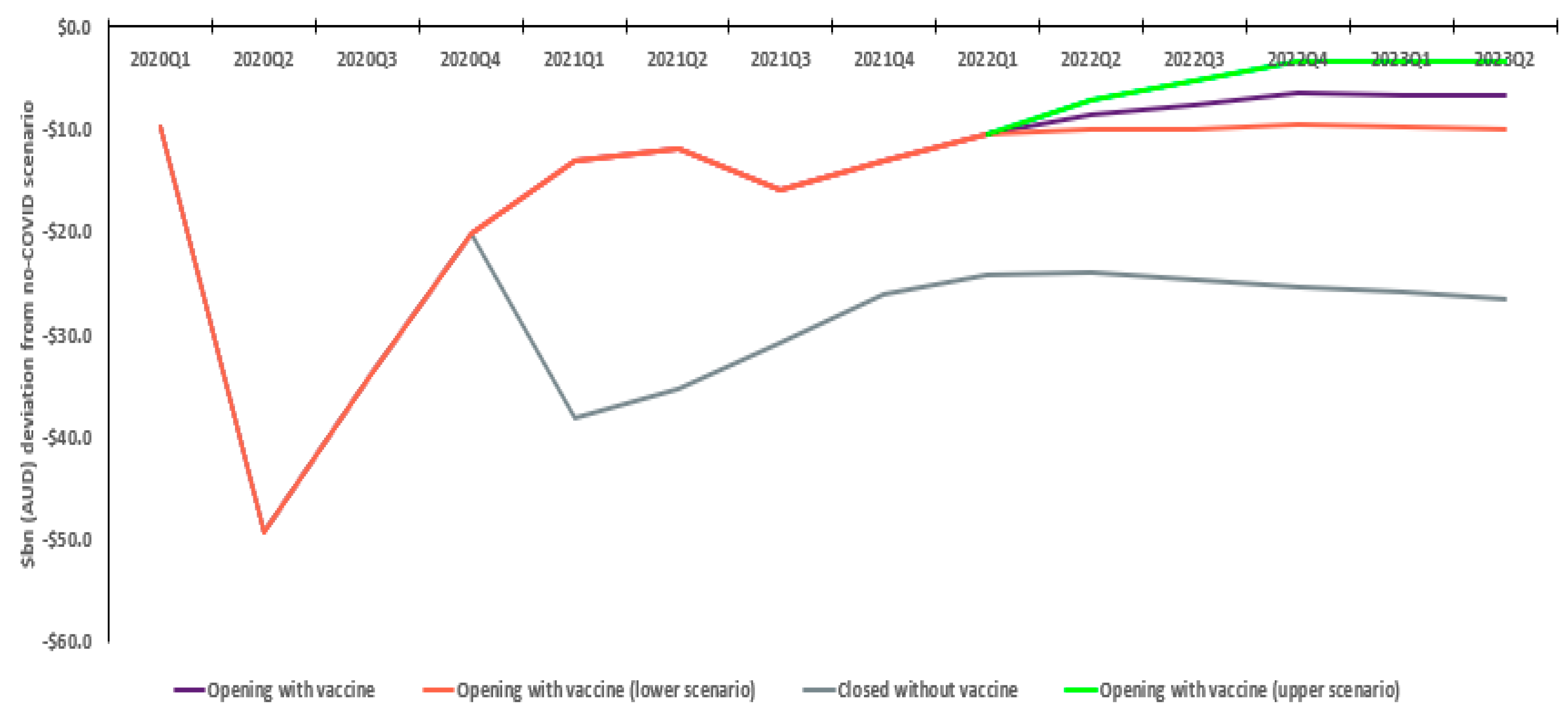
Throughout the pandemic, Australian government policy has prioritised population health and prevention of healthcare system overwhelm. Prior to population-wide vaccination rollout, this was achieved through social and border restrictions. However, our modelling demonstrates this came at a significant cost to the Australian economy. Eventual restrictions removal and the opening up of society saw the Australian economy recover, with modelling showing material positive GDP and employment outcomes.
In particular, Australia’s education and tourism sectors, both reliant on the physical movement of international populations, were seriously impacted by the pandemic, with modelling showing their significant recovery. Sensitivity analysis reinforces this, demonstrating the material effect the timely availability of effective vaccines, vis-à-vis other countries, may have on the Australian economy.
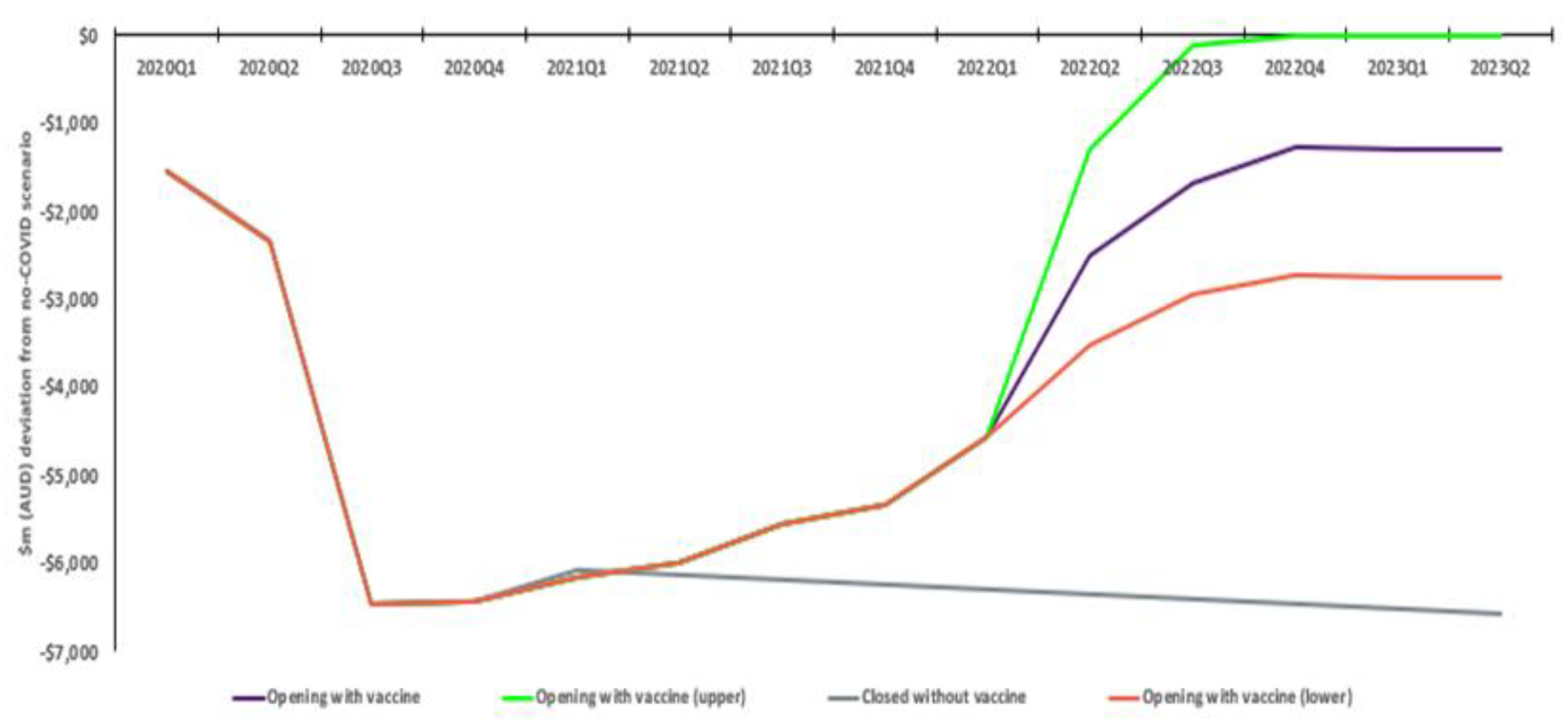
Modelling shows rollout of vaccination from quarter one of 2021 seeing positive projected employment benefits (reflecting actual Australian employment outcomes) relative to the non-vaccination scenario. While the incremental benefit declines over time, it nonetheless remains at a significant level (greater than 100,000 jobs). This reflects recovery in conditions as work-from-home restrictions, school closures, and other physical distancing measures are lifted, naturally reversing the productivity and demand-driven losses assumed for 2020. It is relevant to note that employment levels, which were sharply depressed through the middle quarters of 2020, approached no COVID levels by the end of 2021.
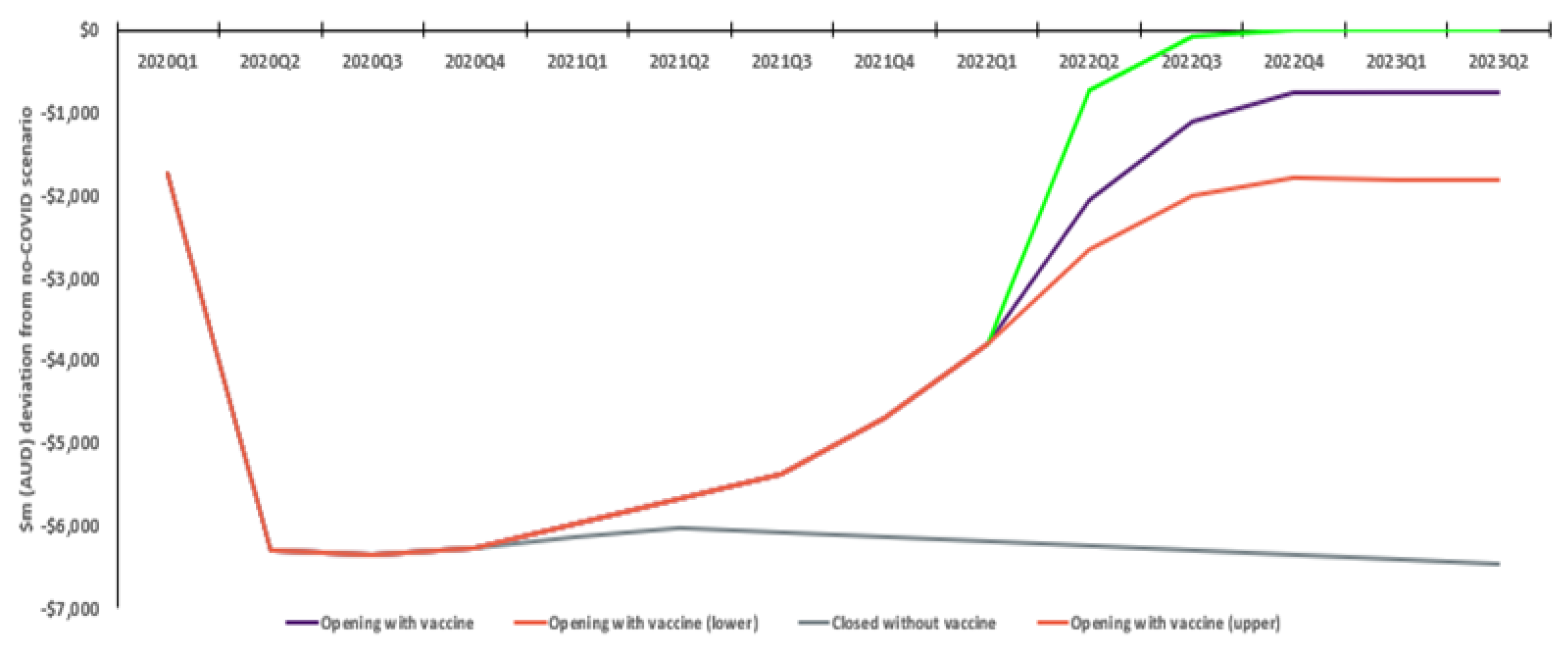
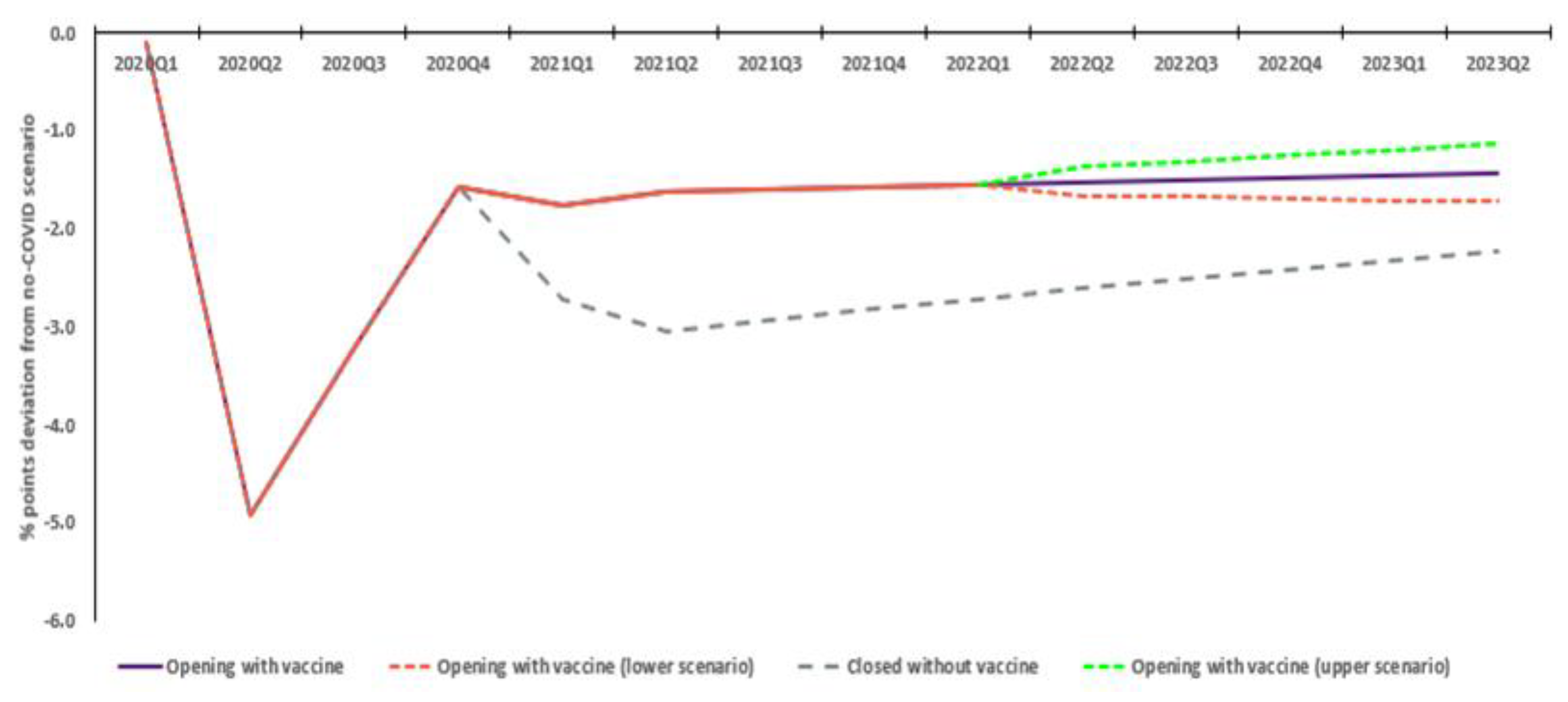
The analysis also provides insight into longer term effects on the Australian economy. For example, Australia’s population declines via net migration under both scenarios, with an estimated 2.7% less than a no COVID scenario in quarter 2 2023, compared to 1.4% less with vaccination. The permanent reduction in Australia’s workforce across 30 months shows the positive effect of readily available vaccines on Australia’s long-term economic landscape.
The model employs a time horizon (30 months) much shorter than that typically used in HTA (potentially up to a lifetime, particularly for vaccines) [
28]. Several points should be noted. Firstly, the CGE modelling aimed to estimate the incremental economic outcomes as the vaccination programme was rolled out. CGE modelling is a complex forecasting tool reliant on dozens of general assumptions and inputs regarding the operation of an economy. The modelling incorporated adjustments to capture the impact of the COVID ‘shock’ on the economy. At the time modelling simulations were computed (start of 2022), these shock assumptions were largely set, reflecting the understood COVID ‘decision problem’. That is, Australia had achieved the required levels of population-wide vaccination to enable removal of most restrictions and it was anticipated that the COVID pandemic would over time transition to a seasonal endemic virus that generally, would not involve ongoing restriction measures. The model also benefits from using actual economic data for a material proportion of the analysis period and as results demonstrate, the incremental economic impacts following rollout largely reach ‘steady state’ by early to mid-2023. In summary, this means the time horizon appropriately captures the decision problem reflecting the specified COVID shock, with analysis demonstrating the magnitude of economic impacts following a vaccination rollout.
In this regard, model results demonstrate the significant negative impacts on tourism and education sectors, which are reliant on physical movement of people. It is intuitive that without removal of restrictions, these sectors would see negative longer term economic impacts. There is also the potential that an opening up of Australia at a later date than that used in the model would still see relative economic losses, as consumers permanently re-orient their demand to other international markets. Further, as highlighted above, the pandemic is likely to have sufficient long-term effects on Australia’s economic capabilities (i.e., net migration).
It may be suggested that the actual economic activity after the onset of COVID compared to the economic situation immediately prior might yield an empirical measure of the impacts of COVID and of vaccination, and that this could be used for comparison purposes. However, the historical record through to quarter 2 of 2021 reflects a large number of factors (past investments, non-COVID related changes in world trading conditions, etc.) having no connection with the pandemic. For example, while a vaccination rollout ultimately facilitated people movement, it does not compel tourists and students to return to Australia; as economic agents (‘consumers’), they still have their own individual (and as a collective) decision making processes.
As such, economic outcomes are not solely attributable to vaccination and indeed reflect many influences including national and international government policies, prevailing economic trends, and resulting independent consumer behaviour. Indeed, as 2022 has unfolded, Australian and international economic outcomes have been subject to forces both domestic and international that have been only partly related to the pandemic, or alternatively, largely unrelated to the pandemic (e.g., global conflicts).
Nevertheless, the timely population-wide rollout of effective COVID vaccines was clearly an integral component in ‘unlocking’ society and opening the economy. Australia’s GDP performance since early 2021 tends to suggest that the economy has been on a path of recovery, with the ABS noting the contribution that domestic and international border opening has had [
38], which in turn was predicated largely on Australia collectively reaching a specified population-wide vaccination level.
The pandemic evolved unpredictably, with continual shifts in the prevailing variant, health outcomes, healthcare system capacity and government policy responses. Economic modelling presented reflects ultimately prevailing pandemic circumstances, but it is possible circumstances could have unfolded differently (e.g., with different order of pandemic waves (Omicron and Delta), or more or less serious waves). However, analysis can largely be only based on the ultimate scenarios experienced. Further, the pandemic and the analysis crucially demonstrate the existence of the potential for infectious diseases to have uncertain, unpredictable and large-scale impacts on society.
Analysis, predicated on the exogenous shock of the pandemic, indicates the difference between the vaccination and no-vaccination scenarios steadies by early 2023. The pandemic has seen the Australian economy adapt over this time, with reallocation of resources and structural adjustments. The exact pathway after mid-2023 cannot be predicted with certainty. Potentially significant exogenous shocks could occur subsequently, however these cannot be forecast, and it is desirable that analysis assess the ‘state of play’ as it was best known. Ceteris paribus, in the future there may be a gradual convergence of economic outcomes under the ‘with’ and ‘without’ vaccination scenarios. Nonetheless, a material economic benefit of vaccination is expected to be evident for some period of time, including due to the underlying nature of the industries particularly affected and the cumulative long-term effect the pandemic has had on Australian economic capabilities (e.g., on net migration).
The pandemic has clearly demonstrated that infectious diseases and associated vaccines have unique characteristics with the potential to affect society at large, causing impacts beyond health and the healthcare system. Despite this, current HTA methodologies do not incorporate these broader value dimensions. In many senses, it is the capability for HTA valuation frameworks to capture the true value of impacts such uncertainty may generate that is of relevance.
The COVID-19 pandemic represents a historically unique situation, with the urgency and nature of government policy responses reflecting the speed, range, and depth of impacts. As such, it is acknowledged that practically, it would have been infeasible for vaccine procurement decisions to have occurred via standard HTA processes. Nonetheless, the VURM modelling analysis illustrates societal effects such as broader macroeconomic impacts clearly demonstrate the value of the timely availability of vaccines.
Reflecting the largely unpredicted original COVID-19 outbreak, there is therefore a continued risk that COVID in various forms may be present for years to come and in potentially equally serious (or worse) forms. Although society is transitioning to a ‘pandemic recovery’ phase, the dynamic nature of the virus means that having a valuation framework that provides for the uncertainty such virus waves may present is appropriate.
Even for conditions of a smaller epidemiological scale, economic productivity impacts can be a particularly relevant issue where broader societal effects may influence the assessed value of an intervention. In part, this relates to how HTA decision makers regarding such broader societal impact evidence. At present, many HTA agencies, including Australia’s PBAC, only consider such analyses as ‘supplementary’ [
28], with PBAC decisions, e.g., for vaccines, demonstrating they do not shape decision making [
55].
With an increasing trend towards personalised medicines, cell and gene therapies expected in Australia [
66], this may create challenges for timely reimbursement and availability of new cutting-edge therapies. For example, patients for who these treatments may be applicable (e.g., those with rare diseases) may face considerable, lifelong costs which fall outside of the traditional healthcare system and experience severely reduced quality of life, including employment and economic productivity, due to the debilitating nature of their conditions.
Since pandemic commencement, the Commonwealth Government has spent AUD 311bn on economic stimulus and AUD 31bn to support the healthcare system [
6], an explicit acknowledgement of the need to address the pandemic’s impact on Australia’s society, economy, health, and wellbeing. Under current PBAC HTA Guidelines, such large-scale expenditures would not be considered in base case analysis [
28]. In comparison, the costs of vaccination deployment, including vaccine procurement [
74], and administration and distribution costs [
75,
76], estimated in total at AUD 12.6 billion, would appear to be a fraction of such support measures.
The expected transition of COVID-19 to an endemic disease emphasises the rationale for taking a broader societal perspective for the HTA applied to vaccines. As literature review shows, there has been increasing international consideration of potential HTA approaches to valuation that provide for a broader scope.
The COVID-19 pandemic serves as a strong exemplar for a broader HTA perspective, with similar principles potentially applicable to other infectious diseases and other therapeutic areas. Failure to incorporate broader societal benefits risks undervaluing important medical innovations, limiting the utility of HTA as a timely decision-making instrument to facilitate investments in the Australian population’s health. With a future likely to increasingly feature innovative medicines, this risks the overall health outcomes of Australians.
While beyond the scope of this paper, there are issues worth noting that would need to be addressed to progress broader HTA valuation frameworks in practice. Firstly, there is a clear need to engage with key government and HTA agencies to progress policy development on this issue, as currently most efforts appear to be coming from industry organisations and academics. Secondly, there is a fundamental need to define both the scope of broader societal impacts (with consideration potentially of quantitative and qualitative factors), as well as how they would be identified, measured and valued individually. Thirdly, it is worth noting that HTA may require consideration of a range of approaches (novel models etc.). It seems that current HTA analysis approaches are too narrow to truly elucidate these types of economic impacts and value, with modelling software potentially being required to be adapted to be fit to capture broader elements of value.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




