


Vaccine Uptake to Prevent Meningitis and Encephalitis in Shanghai, China


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire Design and Distribution
2.3. Measurement of Outcomes
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
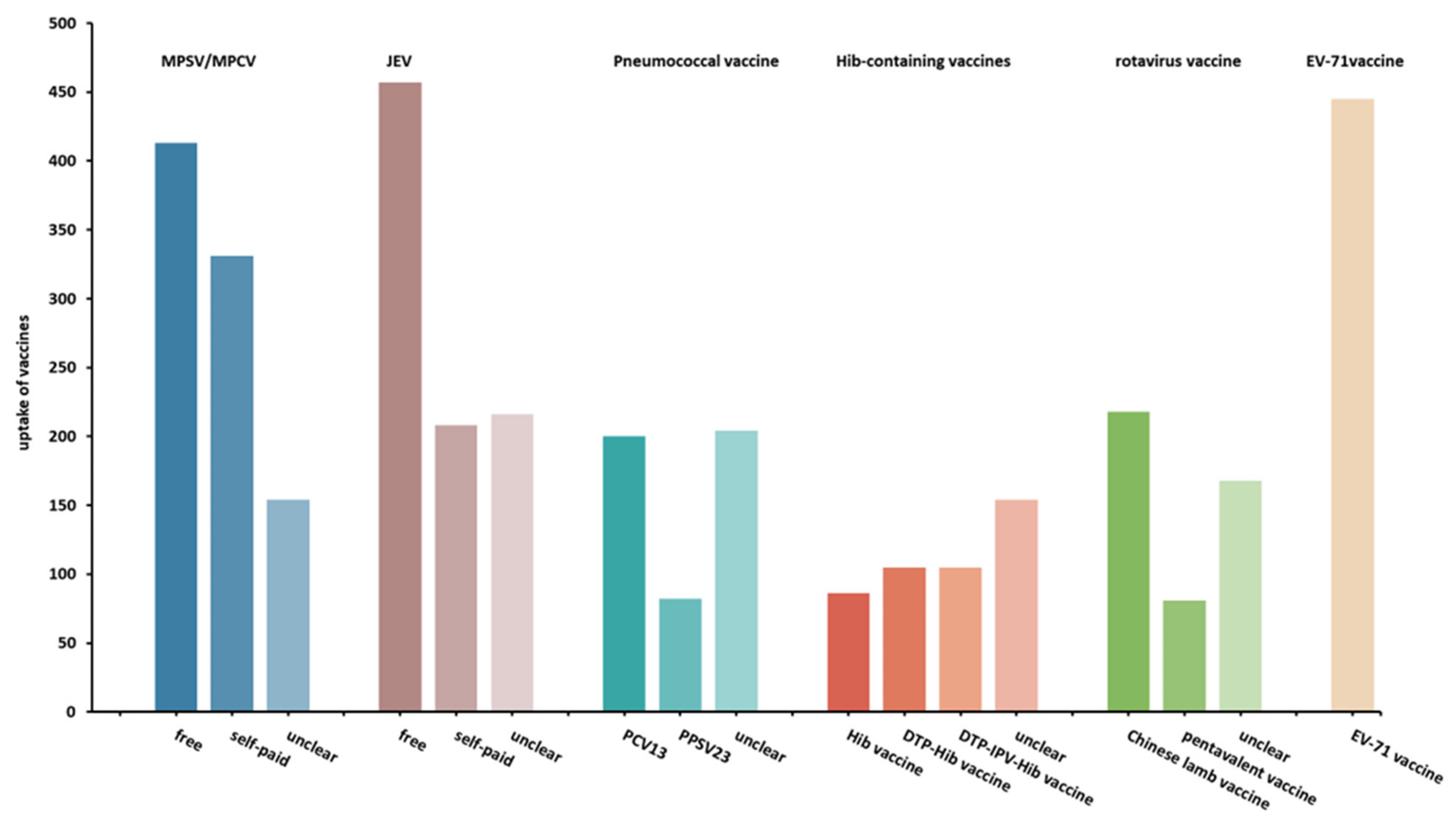
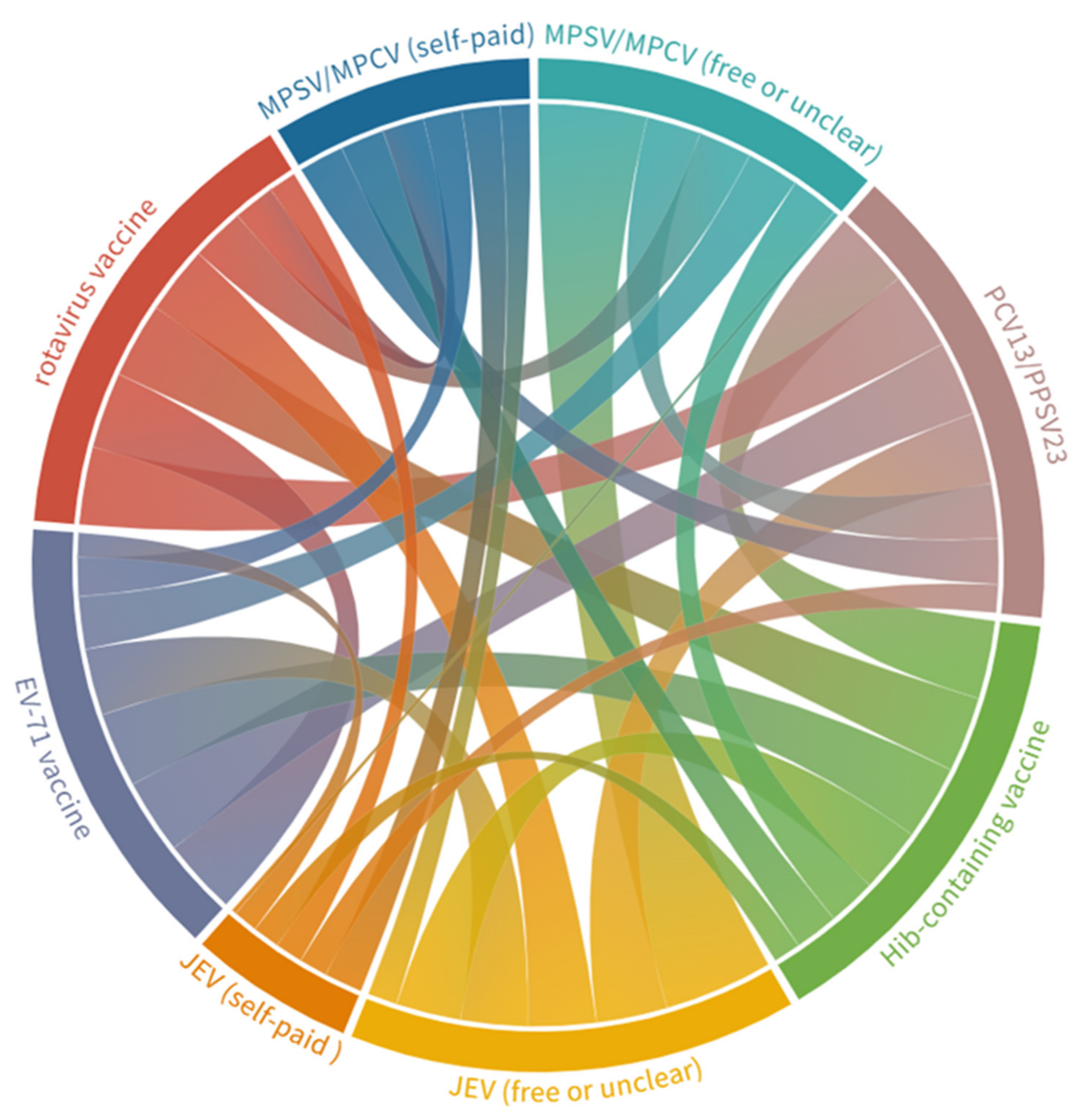
3.1. Vaccine Uptake
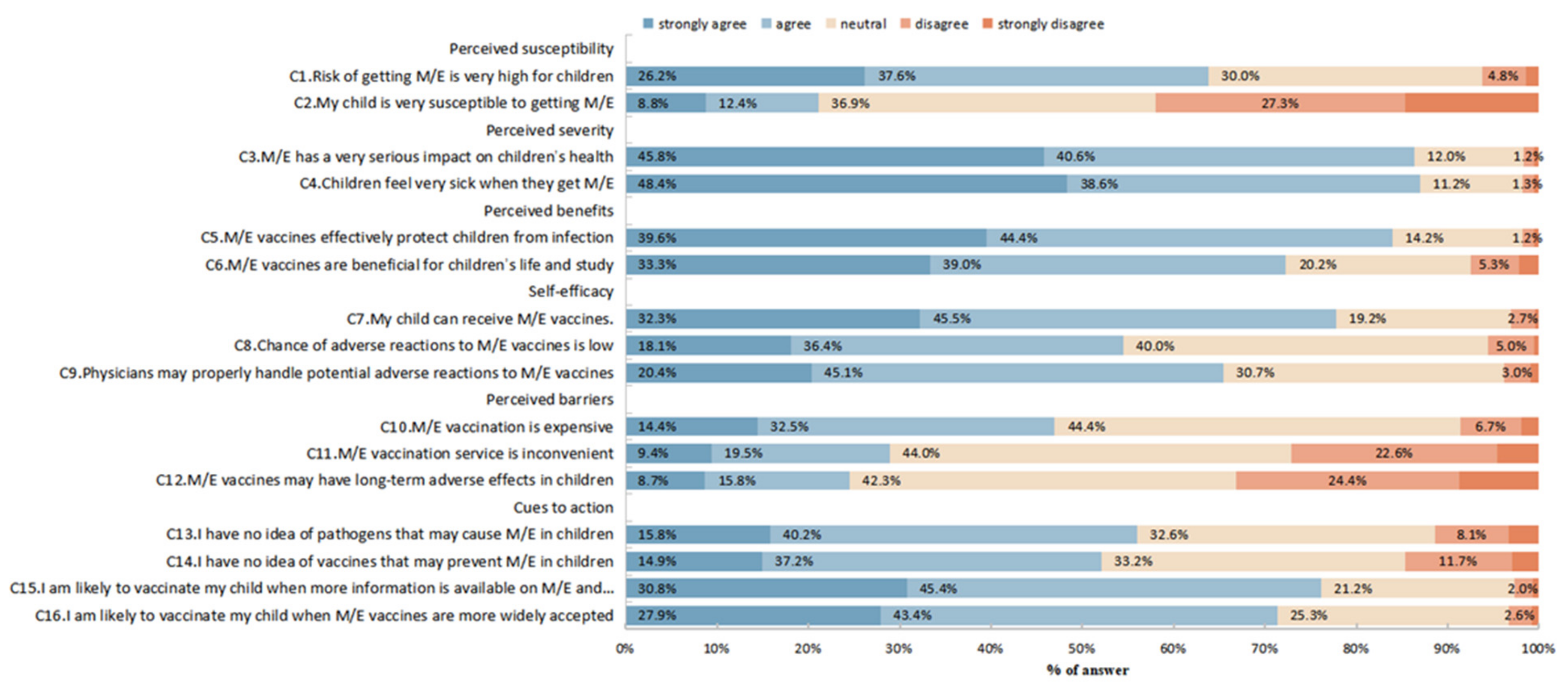
3.2. Knowledge and Health Beliefs
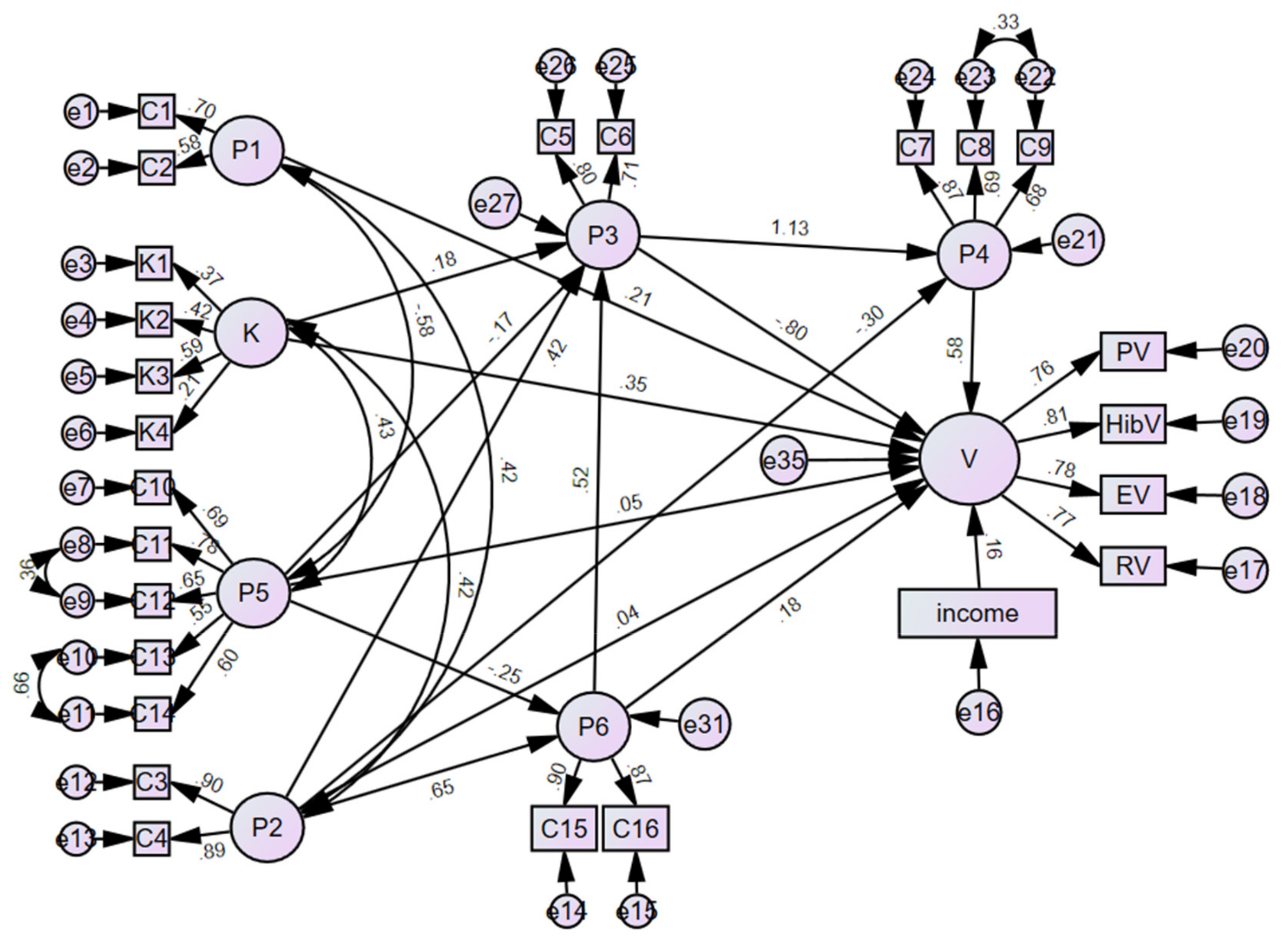
3.3. Factors Associated with Vaccine Uptake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Redenbaugh, V.; Flanagan, E.P. Understanding the etiology and epidemiology of meningitis and encephalitis: Now and into the future. Lancet Reg. Health. West. Pac. 2022, 20, 100380. [Google Scholar] [CrossRef] [PubMed]
- Pommier, J.D.; Gorman, C.; Crabol, Y.; Bleakley, K.; Sothy, H.; Santy, K.; Tran, H.T.T.; Nguyen, L.V.; Bunnakea, E.; Hlaing, C.S.; et al. Childhood encephalitis in the Greater Mekong region (the SouthEast Asia Encephalitis Project): A multicentre prospective study. Lancet Glob. Health 2022, 10, e989–e1002. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Xie, Z.; Liu, G.; Chen, Z.; Yang, Y.; Li, Y.; Chen, J.; Zheng, G.; Shen, K. Etiology and prognosis of acute viral encephalitis and meningitis in Chinese children: A multicentre prospective study. BMC Infect. Dis. 2017, 17, 494. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.; Jung, J.; Britton, P.N.; King, C.; Yin, J.K.; Jones, C.A. Long-term outcomes of infective encephalitis in children: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2016, 58, 1108–1115. [Google Scholar] [CrossRef]
- Julia Granerod, A.E.; Nicholas, D.; Benedict, M.; Tom, S.; Ava, E. Encephalitis: An In-Depth Review and Gap Analysis of Key Variables Affecting Global Disease Burden. Available online: https://www.encephalitis.info/Handlers/Download.ashx?IDMF=a9afbb99-dbae-4dbb-8a5d-8d55cef2e8c3 (accessed on 20 September 2022).
- GBD Results Tool. Available online: https://vizhub.healthdata.org/gbd-results/?params=gbd-api-2016-permalink/0cd2fe7b521ecd03d0da0a7b726b4d1c (accessed on 17 August 2022).
- Li, Y.; Yin, Z.; Shao, Z.; Li, M.; Liang, X.; Sandhu, H.S.; Hadler, S.C.; Li, J.; Sun, Y.; Li, J.; et al. Population-based surveillance for bacterial meningitis in China, September 2006-December 2009. Emerg. Infect. Dis. 2014, 20, 61–69. [Google Scholar] [CrossRef]
- Zhao, L.; Zhou, M.; Wang, B.; Guo, J.; Chen, N.; He, L. Clinical characteristics and outcome of clinically diagnosed viral encephalitis in southwest China. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2015, 36, 2191–2197. [Google Scholar] [CrossRef]
- Wang, C.; Xu, H.; Deng, J.; Yu, H.; Chen, Y.; Wang, S.; Huang, W.; Hao, J.; Wang, C.; Deng, H.; et al. Prognostic factors in pediatric pneumococcal meningitis patients in mainland China: A retrospective multicenter study. Infect. Drug Resist. 2019, 12, 1501–1512. [Google Scholar] [CrossRef]
- Ma, J.; Jiang, L. Outcome of children with Japanese encephalitis and predictors of outcome in southwestern China. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 660–665. [Google Scholar] [CrossRef]
- Defeating Meningitis 2030: Baseline Situation Analysis. Available online: https://www.who.int/publications/m/item/defeating-meningitis-2030-baseline-situation-analysis (accessed on 20 September 2022).
- Presa, J.; Serra, L.; Weil-Olivier, C.; York, L. Preventing invasive meningococcal disease in early infancy. Hum. Vaccines Immunother. 2022, 18, 1979846. [Google Scholar] [CrossRef]
- Christensen, H.; Al-Janabi, H.; Levy, P.; Postma, M.J.; Bloom, D.E.; Landa, P.; Damm, O.; Salisbury, D.M.; Diez-Domingo, J.; Towse, A.K.; et al. Economic evaluation of meningococcal vaccines: Considerations for the future. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care 2020, 21, 297–309. [Google Scholar] [CrossRef]
- Che, X.; Liu, Y.; Wang, J.; Xu, Y.; Zhang, X.; Gu, W.; Jiang, W.; Du, J.; Zhang, X. Primary immunization of meningococcal meningitis vaccine among children in Hangzhou, China, 2008–2017. Hum. Vaccines Immunother. 2021, 17, 1239–1243. [Google Scholar] [CrossRef]
- Parpia, A.S.; Li, Y.; Chen, C.; Dhar, B.; Crowcroft, N.S. Encephalitis, Ontario, Canada, 2002–2013. Emerg. Infect. Dis. 2016, 22, 426–432. [Google Scholar] [CrossRef]
- Tsolenyanu, E.; Bancroft, R.E.; Sesay, A.K.; Senghore, M.; Fiawoo, M.; Akolly, D.; Godonou, M.A.; Tsogbale, N.; Tigossou, S.D.; Tientcheu, L.; et al. Etiology of Pediatric Bacterial Meningitis Pre- and Post-PCV13 Introduction Among Children Under 5 Years Old in Lomé, Togo. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 69, S97–s104. [Google Scholar] [CrossRef]
- Soeters, H.M.; Kambiré, D.; Sawadogo, G.; Ouédraogo-Traoré, R.; Bicaba, B.; Medah, I.; Sangaré, L.; Ouédraogo, A.S.; Ouangraoua, S.; Yaméogo, I.; et al. Impact of 13-Valent Pneumococcal Conjugate Vaccine on Pneumococcal Meningitis, Burkina Faso, 2016–2017. J. Infect. Dis. 2019, 220, S253–s262. [Google Scholar] [CrossRef]
- Ruiz-Contreras, J.; Picazo, J.; Casado-Flores, J.; Baquero-Artigao, F.; Hernández-Sampelayo, T.; Otheo, E.; Méndez, C.; Del Amo, M.; Balseiro, C. Impact of 13-valent pneumococcal conjugate vaccine on pneumococcal meningitis in children. Vaccine 2017, 35, 4646–4651. [Google Scholar] [CrossRef]
- Braikat, M.; Barkia, A.; El Mdaghri, N.; Rainey, J.J.; Cohen, A.L.; Teleb, N. Vaccination with Haemophilus influenzae type b conjugate vaccine reduces bacterial meningitis in Morocco. Vaccine 2012, 30, 2594–2599. [Google Scholar] [CrossRef]
- Hattori, F.; Kawamura, Y.; Kawada, J.I.; Kojima, S.; Natsume, J.; Ito, K.; Saito, S.; Kitagawa, Y.; Okumura, A.; Yoshikawa, T. Survey of rotavirus-associated severe complications in Aichi Prefecture. Pediatrics Int. Off. J. Jpn. Pediatric Soc. 2018, 60, 259–263. [Google Scholar] [CrossRef]
- Jiang, L.; Wang, J.; Zhang, C.; He, W.; Mo, J.; Zeng, J.; Chen, M.; Tan, Y.; Ning, C. Effectiveness of enterovirus A71 vaccine in severe hand, foot, and mouth disease cases in Guangxi, China. Vaccine 2020, 38, 1804–1809. [Google Scholar] [CrossRef]
- Xu, M.; Ye, C.; Ye, Y.; Li, Q. Analysis on the Status and Influencing Factors of Second-class Vaccinations for Children Aged 0-3 Years Old in Conghua District of Guangzhou City. J. Prev. Med. Inf. 2020, 36, 854–858. [Google Scholar]
- Qi, L.; Su, K.; Xia, Y.; Tang, W.; Shen, T.; Li, Q. Enterovirus 71 vaccine acceptance among parents of children < 5 years old and their knowledge of hand, foot and mouth disease, Chongqing, China, 2017. PLoS ONE 2019, 14, e0225569. [Google Scholar] [CrossRef]
- Wu, L.; Liu, J.; Shao, H.; Sun, X. Surveillance for coverage of inactivated enterovirus 71 (EV71) vaccine and adverse events following immunization with EV71 vaccine among children in Shanghai. Chin. J. Vaccines Immun. 2020, 26, 62–66+81. [Google Scholar] [CrossRef]
- Wagner, A.L.; Sun, X.; Montgomery, J.P.; Huang, Z.; Boulton, M.L. The impact of residency and urbanicity on Haemophilus influenzae Type b and pneumococcal immunization in Shanghai Children: A Retrospective Cohort Study. PLoS ONE 2014, 9, e97800. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; John Wiley & Sons: New York, NY, USA, 2003. [Google Scholar]
- Liu, Y.; Yue, C.Y.; Li, Y.; Wang, Y.M.; Gao, S.R.; Wang, Z.G.; Xie, X.; Zhao, H.P.; Wang, D.; Liang, X.F.; et al. [Analysis of vaccination situation of orial live attenuated rotavirus vaccine (LLR strain) among children in 6 provinces of China]. Zhonghua Yu Fang Yi Xue Za Zhi [Chin. J. Prev. Med.] 2018, 52, 282–286. [Google Scholar] [CrossRef]
- Chen, J.; Sun, X.; Huang, Z. Status quo analysis on non-immunization program vaccination among children in Shanghai. Shanghai J. Prev. Med. 2020, 32, 622–626. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Tarkar, P. Predicting intentions to get the COVID-19 vaccine in India: An integration of theory of planned behaviour and health belief model. Int. J. Health Plan. Manag. 2022. [Google Scholar] [CrossRef]
- Rajamoorthy, Y.; Radam, A.; Taib, N.M.; Rahim, K.A.; Wagner, A.L.; Mudatsir, M.; Munusamy, S.; Harapan, H. The relationship between perceptions and self-paid hepatitis B vaccination: A structural equation modeling approach. PLoS ONE 2018, 13, e0208402. [Google Scholar] [CrossRef]
- Donadiki, E.M.; Jiménez-García, R.; Hernández-Barrera, V.; Sourtzi, P.; Carrasco-Garrido, P.; López de Andrés, A.; Jimenez-Trujillo, I.; Velonakis, E.G. Health Belief Model applied to non-compliance with HPV vaccine among female university students. Public Health 2014, 128, 268–273. [Google Scholar] [CrossRef]
- Nitzl, C. The use of partial least squares structural equation modelling (PLS-SEM) in management accounting research: Directions for future theory development. J. Account. Lit. 2016, 37, 19–35. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar] [CrossRef]
- Jadil, Y.; Ouzir, M. Exploring the predictors of health-protective behavior during the COVID-19 pandemic: A multi-country comparison. Environ. Res. 2021, 199, 111376. [Google Scholar] [CrossRef]
- Wang, Q.; Yue, N.; Zheng, M.; Wang, D.; Duan, C.; Yu, X.; Zhang, X.; Bao, C.; Jin, H. Influenza vaccination coverage of population and the factors influencing influenza vaccination in mainland China: A meta-analysis. Vaccine 2018, 36, 7262–7269. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, J.; Zhang, S.; Li, J.; Sun, Y. Characteristics and pathogeny spectrum of acute meningitis and encephalitis among children less than 5 years old. J. Med. Pest. Control 2018, 34, 242–245. [Google Scholar]
- Wang, L.P.; Yuan, Y.; Liu, Y.L.; Lu, Q.B.; Shi, L.S.; Ren, X.; Zhou, S.X.; Zhang, H.Y.; Zhang, X.A.; Wang, X.; et al. Etiological and epidemiological features of acute meningitis or encephalitis in China: A nationwide active surveillance study. Lancet Reg. Health. West. Pac. 2022, 20, 100361. [Google Scholar] [CrossRef]
- Li, Z.Q.; Qin, Z.Q.; Tan, H.F.; Zhang, C.H.; Xu, J.X.; Chen, J.; Ni, L.H.; Yun, X.X.; Cui, M.; Huang, Y.; et al. Analysis of the coverage of inactivated enterovirus 71 (EV71) vaccine and adverse events following immunization with the EV71 vaccine among children from 2016 to 2019 in Guangzhou. Expert Rev. Vaccines 2021, 20, 907–918. [Google Scholar] [CrossRef]
- Ganczak, M.; Dmytrzyk-Daniłów, G.; Karakiewicz, B.; Korzeń, M.; Szych, Z. Determinants influencing self-paid vaccination coverage, in 0-5 years old Polish children. Vaccine 2013, 31, 5687–5692. [Google Scholar] [CrossRef]
- Hong, J.Y.; Ki, M.R.; Hwang, H.J.; Sinny, D.; Park, Y.J.; Bae, G.R.; Lee, M.S. Factors related to completed status and seropositivity of hepatitis a immunization among children aged 1–3 years and 6–8 years in South Korea. Osong Public Health Res. Perspect. 2013, 4, 93–98. [Google Scholar] [CrossRef]
- Zhang, X.; Meng, Q.; Chen, S.; Wang, C.; Chen, X.; Zhang, X. An analysis on parents’ acceptance of charge vaccines and its influencing factors. Prev. Med. 2016, 28, 336–339. [Google Scholar] [CrossRef]
- Lei, H.; Qiu-Yan, L.; You-Qi, H.; Shuo, F.; Xiao-Ming, Z. Parents’ Perception and their Decision on their Children’s Vaccination Against Seasonal Influenza in Guangzhou. Chin. Med. J. 2015, 128, 327–341. [Google Scholar]
- Wagner, A.L.; Gordon, A.; Tallo, V.L.; Simaku, A.; Porter, R.M.; Edwards, L.J.; Duka, E.; Abu-Khader, I.; Gresh, L.; Sciuto, C.; et al. Intent to obtain pediatric influenza vaccine among mothers in four middle income countries. Vaccine 2020, 38, 4325–4335. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Lu, J.; Zhang, L.; Mei, K.; Guan, B.; Lu, Y. Gap between willingness and behavior in the vaccination against influenza, pneumonia, and herpes zoster among Chinese aged 50–69 years. Expert Rev. Vaccines 2021, 20, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Kabir, K.M.A.; Hagishima, A.; Tanimoto, J. Hypothetical assessment of efficiency, willingness-to-accept and willingness-to-pay for dengue vaccine and treatment: A contingent valuation survey in Bangladesh. Hum. Vaccines Immunother. 2021, 17, 773–784. [Google Scholar] [CrossRef] [PubMed]
- Redondo Margüello, E.; Trilla, A.; Munguira, I.L.B.; López-Herce, A.J.; Cotarelo Suárez, M. Knowledge, attitudes, beliefs and barriers of healthcare professionals and adults ≥ 65 years about vaccine-preventable diseases in Spain: The ADult Vaccination drIverS and barriErs (ADVISE) study. Hum. Vaccines Immunother. 2022, 18, 2025007. [Google Scholar] [CrossRef]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef]
- Wagner, A.L.; Boulton, M.L.; Sun, X.; Mukherjee, B.; Huang, Z.; Harmsen, I.A.; Ren, J.; Zikmund-Fisher, B.J. Perceptions of measles, pneumonia, and meningitis vaccines among caregivers in Shanghai, China, and the health belief model: A cross-sectional study. BMC Pediatrics 2017, 17, 143. [Google Scholar] [CrossRef]
- Li, Z.; Ji, Y.; Sun, X. The impact of vaccine hesitation on the intentions to get COVID-19 vaccines: The use of the health belief model and the theory of planned behavior model. Front. Public Health 2022, 10, 882909. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccines | Types | Immunization Schedules |
|---|---|---|
| Meningococcal polysaccharide vaccine (MPSV)/meningococcal polysaccharide conjugate vaccine (MPCV) | EPI and non-EPI (surrogate) | Four doses administered at 6 months, 9 months, 3 years, and 6 years. EPI (free), non-EPI (self-paid) vaccines, or combined, are optional.Three doses of non-EPI vaccines at 6 months, 9 months, and 3 years are optional. |
| Japanese encephalitis vaccine (JEV) (live attenuated and inactivated vaccines) | EPI and non-EPI (surrogate) | Two doses, administered at 2 months and 2 years. EPI (live attenuated) or non-EPI (inactivated) vaccines are optional. Additionally, the third dose of the non-EPI vaccine is optional at 6 years. |
| 13-valent pneumococcal conjugate vaccine (PCV13)/23-valent pneumococcal polysaccharide vaccine (PPSV23) | Non-EPI (non-surrogate) | PCV13: four doses administered at 1, 3, 5 months, and 1 year. PPSV23: one dose administered at 2 years. |
| Haemophilus influenzae type b (Hib)-containing vaccines (Hib vaccine, DTP-Hib vaccine, and DTP-IPV-Hib vaccine) | Non-EPI (non-surrogate) | Hib vaccine and DTP-IPV-Hib vaccine: four doses administered at 2, 3, and 4 months, and 1.5 years. DTP-Hib vaccine: four doses administered at 3, 4, and 5 months, and 1.5 years. |
| Oral live attenuated rotavirus vaccine (Chinese lamb rotavirus vaccine and pentavalent rotavirus vaccine) | Non-EPI (non-surrogate) | Chinese lamb vaccine: one dose administered for children aged from 2 months to 3 years, per year. Pentavalent vaccine: three doses administered at 1, 2, and 3 months. |
| Inactivated enterovirus 71 (EV-71) vaccine | Non-EPI (non-surrogate) | Two doses administered at 6 months and 7 months. |
| Pathogens | Correct Answer (%) | ||
|---|---|---|---|
| Pathogens May Cause M/E | Possible Transmission Routes of Pathogens * | M/E May Be Prevented by Possible Vaccines ** | |
| Meningococcus | 93.0 | 19.3 | 91.0 |
| Streptococcus pneumonia | 45.0 | 19.0 | 29.7 |
| Haemophilus influenzae type b (Hib) | 40.0 | 20.3 | 54.7 |
| Japanese encephalitis virus | 59.9 | 36.8 | 85.2 |
| Enterovirus 71 (EV-71) | 14.1 | 31.2 | 34.4 |
| Rotavirus | 14.3 | 33.5 | 31.2 |
| Factors | Category | Number of Respondents | Knowledge | Health Beliefs | ||
|---|---|---|---|---|---|---|
| Mean (SD) | p Value | Mean (SD) | p Value | |||
| Family caregivers | Mother | 693 | 27.37 (5.84) | 0.5073 | 56.05 (6.30) | 0.1080 |
| Father | 294 | 26.87 (6.86) | 56.99 (6.63) | |||
| Grandparents | 24 | 27.13 (8.45) | 56.05 (6.30) | |||
| Gender | Male | 307 | 26.82 (7.01) | 0.2077 | 56.90 (6.69) | 0.0625 |
| Female | 704 | 27.39 (5.84) | 56.08 (6.31) | |||
| Ethnicity | Han Chinese | 890 | 26.82 (7.01) | 0.1635 | 56.51 (6.54) | 0.0063 |
| Minority Chinese | 121 | 27.12 (6.21) | 55.02 (5.41) | |||
| Age (year) | ≤30 | 238 | 26.67 (6.19) | 0.0178 | 56.16 (6.92) | 0.3558 |
| 31–35 | 531 | 27.03 (6.13) | 56.17 (6.01) | |||
| ≥36 | 242 | 28.17 (6.37) | 56.85 (6.82) | |||
| Children’s age (years) | <3 | 185 | 28.56 (6.32) | 0.0012 | 57.43 (6.88) | 0.0101 |
| ≥3 | 826 | 26.92 (6.16) | 56.08 (6.31) | |||
| Number of children | 1 | 513 | 27.12 (6.21) | 0.5981 | 56.83 (6.29) | 0.0111 |
| ≥2 | 498 | 27.32 (6.23) | 55.81 (6.54) | |||
| Monthly family income (CNY) | <5000 | 210 | 26.02 (6.51) | 0.0097 | 54.64 (6.34) | <0.0001 |
| 5000–9999 | 347 | 27.63 (6.09) | 56.93 (6.14) | |||
| ≥10,000 | 295 | 27.71 (6.26) | 57.60 (6.56) | |||
| No disclosure | 159 | 26.98 (5.84) | 54.89 (6.25) | |||
| Educational level | Below the college | 305 | 25.64 (6.00) | <0.0001 | 54.39 (5.96) | <0.0001 |
| College and above | 706 | 27.90 (6.19) | 57.16 (6.45) | |||
| History of communicable diseases | No history | 623 | 26.61 (6.33) | 0.0001 | 55.80 (6.51) | 0.0027 |
| 1 | 245 | 27.80 (5.99) | 56.95 (6.25) | |||
| ≥2 | 143 | 28.86 (5.73) | 57.57 (6.17) | |||
| Uptake of MPSV/MPCV | Self-paid vaccine | 331 | 27.86 (6.24) | 0.0008 | 57.45 (6.94) | <0.0001 |
| Free vaccine or unclear | 567 | 27.22 (6.08) | 56.14 (6.05) | |||
| No uptake | 113 | 25.30 (6.47) | 54.02 (6.12) | |||
| Uptake of JEV | Self-paid vaccine | 208 | 27.10 (5.92) | 0.0621 | 56.40 (6.31) | <0.0001 |
| Free vaccine or unclear | 673 | 27.48 (6.22) | 56.78 (6.53) | |||
| No uptake | 130 | 26.08 (6.58) | 53.88 (5.55) | |||
| Uptake of four other vaccines | 3–4 | 397 | 28.45 (6.10) | <0.0001 | 57.96 (6.90) | <0.0001 |
| 1–2 | 238 | 27.94 (5.68) | 56.48 (5.77) | |||
| No uptake | 376 | 25.47 (6.28) | 54.50 (5.83) | |||
| Factors * | Category | Odds Ratio (OR) and 95% Confidence Interval (CI) | |||||
|---|---|---|---|---|---|---|---|
| MPSV/MPCV | JEV | PCV13/PPSV23 | Hib-Containing Vaccine | Rotavirus Vaccine | EV-71 Vaccine | ||
| Number of children | 1 | 1.66 (1.30, 2.45) | 1.29 (0.99, 1.68) | 1.37 (1.05, 1.78) | |||
| ≥2 | 1.00 | 1.00 | 1.00 | ||||
| Age (years) | ≤30 | 1.91 (1.31, 2.79) | |||||
| 31–35 | 1.39 (1.01, 1.92) | ||||||
| ≥36 | 1.00 | ||||||
| Ethnicity | Han Chinese | 2.02 (1.32, 3.10) | 2.53 (1.59, 4.00) | 1.89 (1.24, 2.89) | 1.99 (1.29, 3.07) | ||
| Minority Chinese | 1.00 | 1.00 | 1.00 | 1.00 | |||
| Family income (CNY) | <5000 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 5000–9999 | 1.82 (1.08, 3.05) | 2.81 (1.50, 5.26) | 1.61 (1.00, 2.61) | 1.87 (1.27, 2.76) | 1.90 (1.31, 2.76) | 1.42 (0.98, 2.06) | |
| ≥10,000 | 2.96 (1.60, 5.46) | 4.07 (2.16, 7.67) | 2.83 (1.59, 5.04) | 2.98 (1.98, 4.47) | 2.44 (1.65, 3.62) | 1.85 (1.25, 2.74) | |
| No disclosure | 0.99 (0.57, 1.73) | 1.21 (0.70, 2.08) | 1.32 (0.85, 2.05) | 1.79 (1.14, 2.81) | 1.65 (1.06, 2.55) | 1.11 (0.72, 1.74) | |
| Educational level | Below the college | 1.00 | 1.00 | 1.00 | 1.00 | ||
| College and above | 0.62 (0.46,0.84) | 0.70 (0.51, 0.94) | 0.61 (0.45, 0.82) | 0.62 (0.46, 0.84) | |||
| Knowledge score | Per 1 incremental score | 1.04 (1.00, 1.07) | 1.05 (1.02, 1.07) | 1.05 (1.03, 1.08) | 1.02 (1.00, 1.05) | 1.06 (1.03, 1.08) | |
| Health belief score | Per 1 incremental score | 1.05 (1.01, 1.08) | 1.06 (1.03, 1.10) | 1.05 (1.03, 1.08) | 1.06 (1.03, 1.08) | 1.04 (1.02, 1.06) | 1.04 (1.02, 1.06) |
| Goodness-of-Fit Index (GFI) | Adjusted Goodness-of-Fit Index (AGFI) | Comparative Fit Index (CFI) | Incremental Fit Index (IFI) | Tucker-Lewis Index (TLI) | Parsimony Normed Fit Index (PNFI) | Root Mean Square Error of Approximation (RMSER) | |
|---|---|---|---|---|---|---|---|
| Fitting value | 0.925 | 0.903 | 0.933 | 0.933 | 0.920 | 0.770 | 0.056 |
| Reference value [37] | >0.9 | >0.9 | >0.8 | >0.9 | >0.9 | >0.5 | <0.1 |
| Hypothesis | Path Coefficient | p Value | Cutoff Ratio |
|---|---|---|---|
| Vaccine uptake ← knowledge | 0.354 | <0.001 | 3.355 |
| Vaccine uptake ← perceived susceptibility | 0.212 | 0.010 | 2.590 |
| Vaccine uptake ← perceived severity | 0.039 | 0.811 | 0.239 |
| Vaccine uptake ← perceived benefits | −0.804 | 0.054 | −1.956 |
| Vaccine uptake ← self-efficacy | 0.584 | 0.001 | 3.314 |
| Vaccine uptake ← perceived barriers | 0.054 | 0.589 | 0.541 |
| Vaccine uptake ← cues to action | 0.181 | 0.238 | 1.179 |
| Vaccine uptake ← family income | 0.159 | <0.001 | 4.899 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maimaiti, H.; Lu, J.; Guo, X.; Zhou, L.; Hu, L.; Lu, Y. Vaccine Uptake to Prevent Meningitis and Encephalitis in Shanghai, China. Vaccines 2022, 10, 2054. https://doi.org/10.3390/vaccines10122054
Maimaiti H, Lu J, Guo X, Zhou L, Hu L, Lu Y. Vaccine Uptake to Prevent Meningitis and Encephalitis in Shanghai, China. Vaccines. 2022; 10(12):2054. https://doi.org/10.3390/vaccines10122054
Chicago/Turabian StyleMaimaiti, Hairenguli, Jia Lu, Xiang Guo, Lu Zhou, Linjie Hu, and Yihan Lu. 2022. "Vaccine Uptake to Prevent Meningitis and Encephalitis in Shanghai, China" Vaccines 10, no. 12: 2054. https://doi.org/10.3390/vaccines10122054
APA StyleMaimaiti, H., Lu, J., Guo, X., Zhou, L., Hu, L., & Lu, Y. (2022). Vaccine Uptake to Prevent Meningitis and Encephalitis in Shanghai, China. Vaccines, 10(12), 2054. https://doi.org/10.3390/vaccines10122054