
How Does Digital Media Search for COVID-19 Influence Vaccine Hesitancy? Exploring the Trade-off between Google Trends, Infodemics, Conspiracy Beliefs and Religious Fatalism


 ,
,  , , and
, , and
Abstract
1. Introduction
2. Literature Review
2.1. Background: Digital Media Ecology and Health Behavior
2.2. Hypotheses Development
2.2.1. Impact of Infodemics on Vaccine Hesitancy towards COVID-19
2.2.2. Influence of Conspiracy Beliefs on VHC
2.2.3. Impact of Religious Fatalism on Vaccine Hesitancy towards COVID-19
2.2.4. The Moderating Role of Gender
3. Materials and Methods
3.1. Design, Participants, and Procedure
3.2. Instrumentation
4. Results
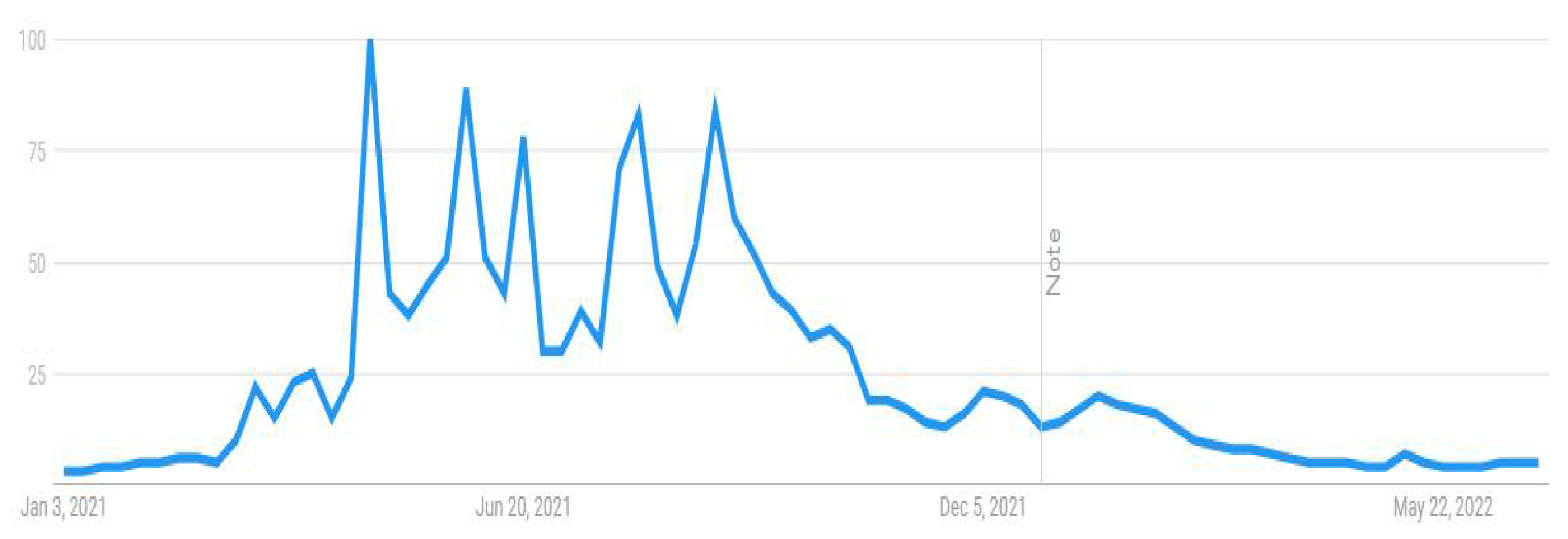
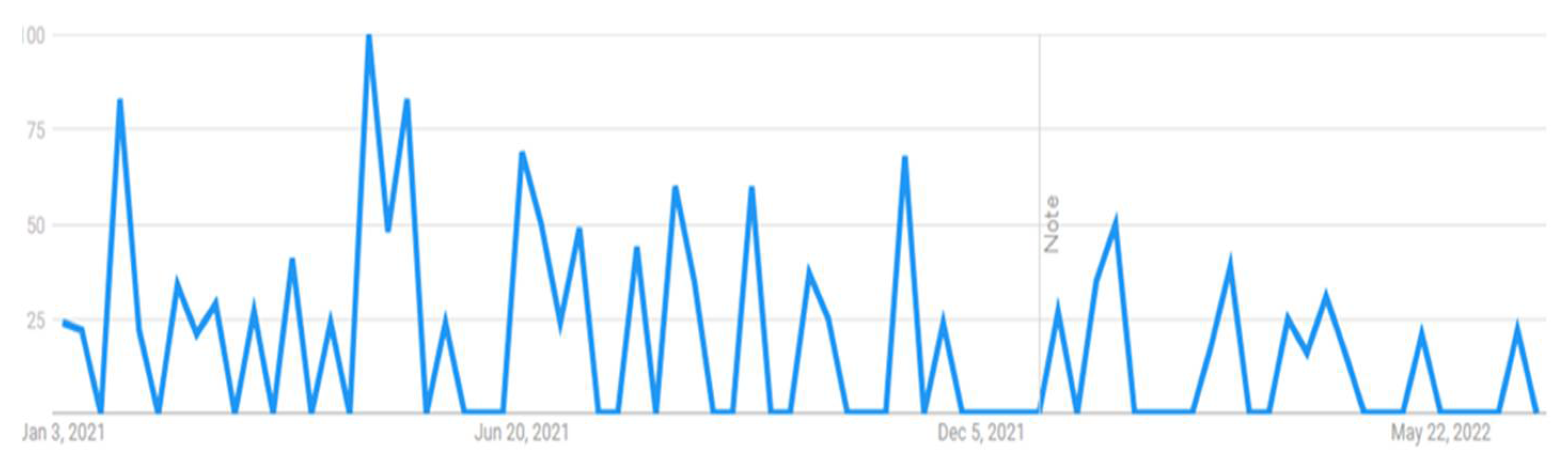
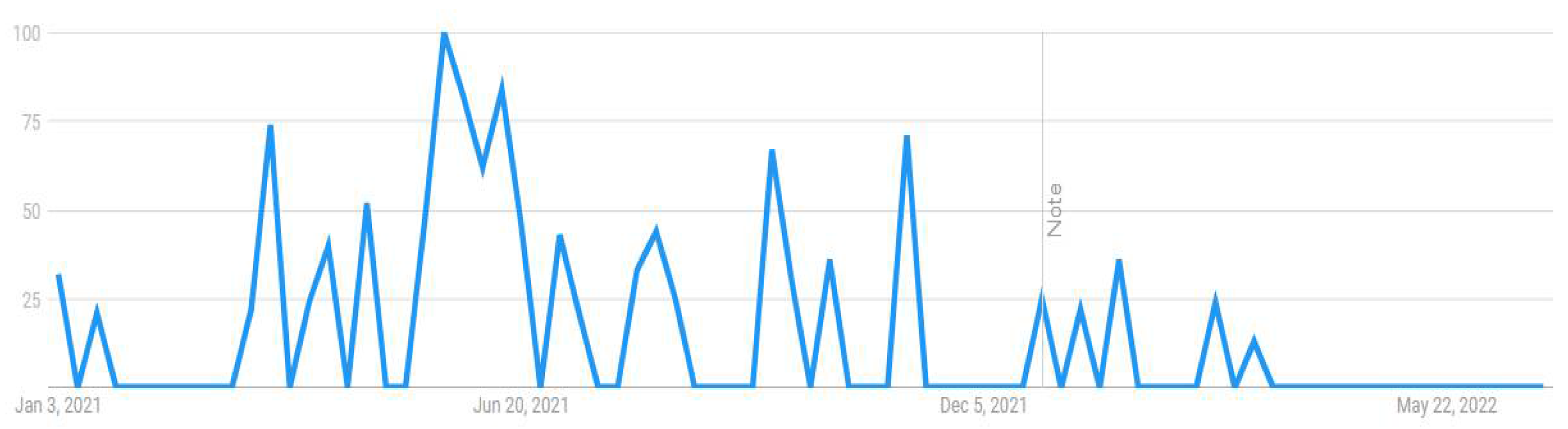
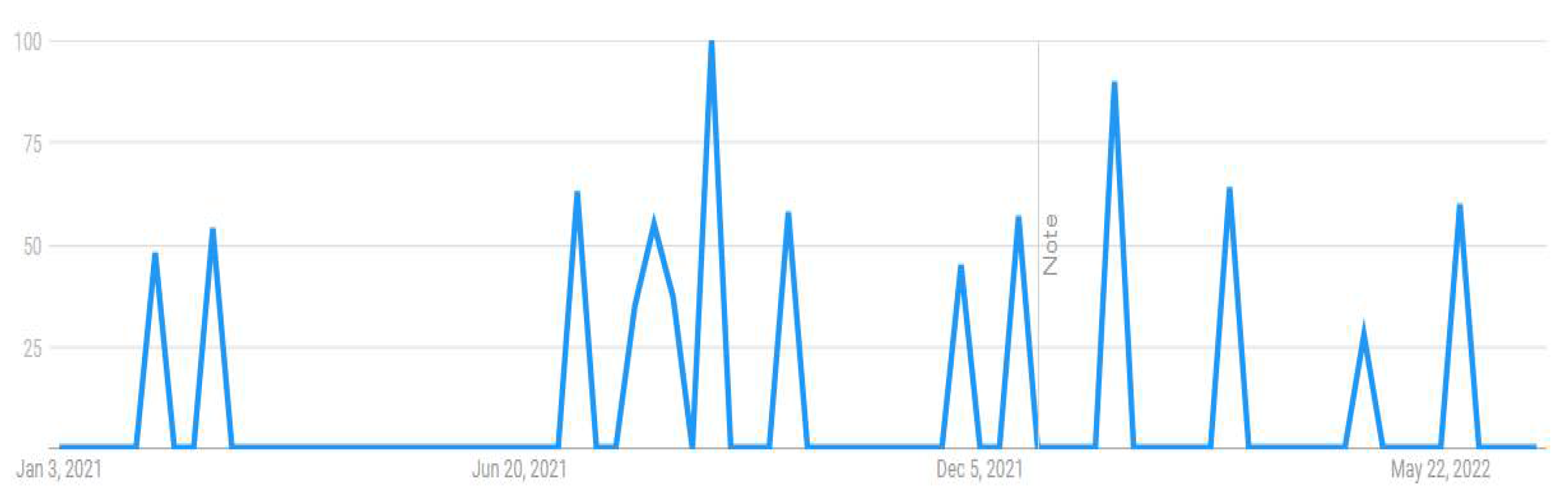
4.1. Google Trends Tool Results for Study 1
4.2. Survey Results for Study 2: Demographic and Descriptive Statistics
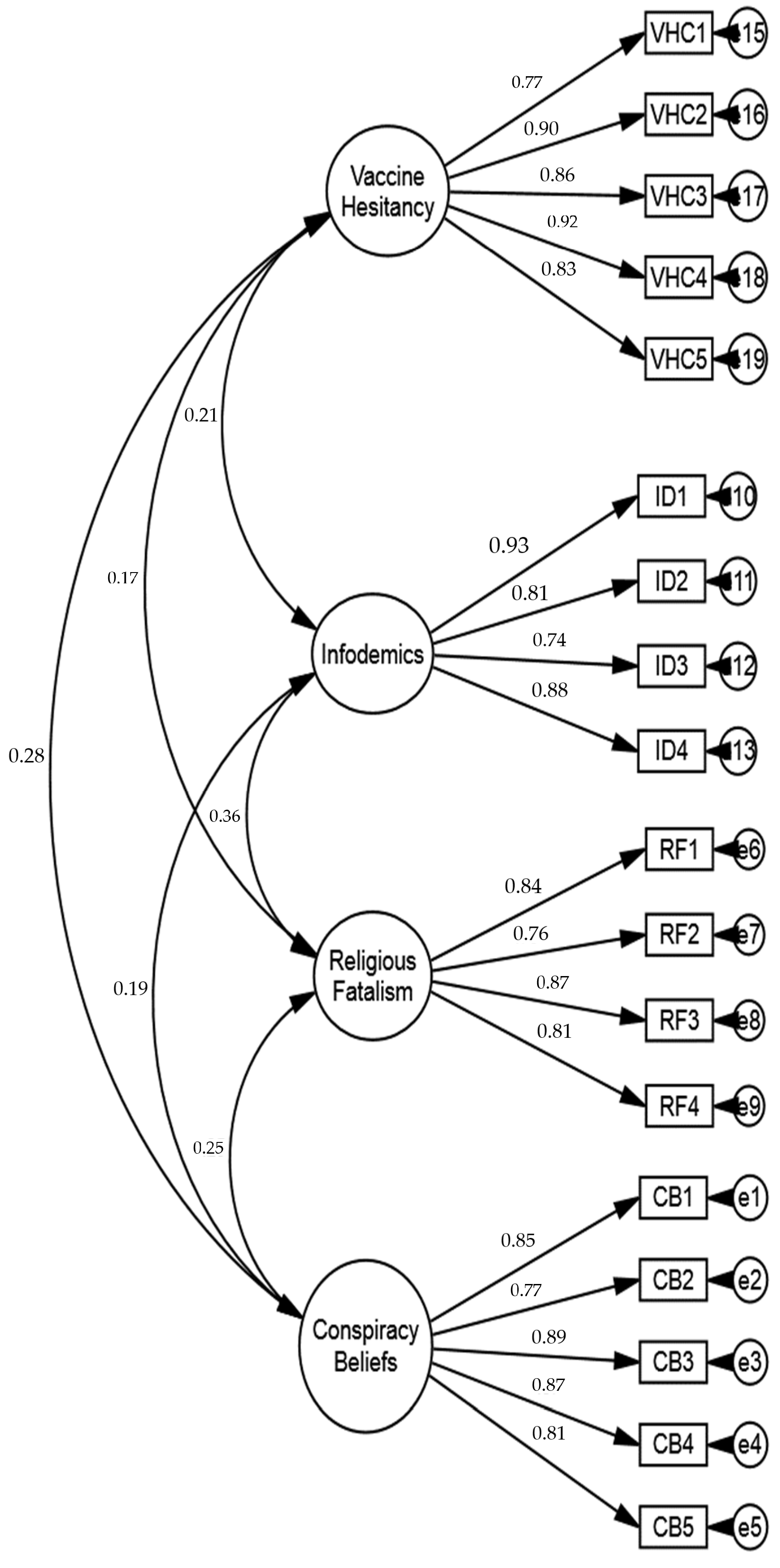
4.3. Confirmatory Factor Analysis
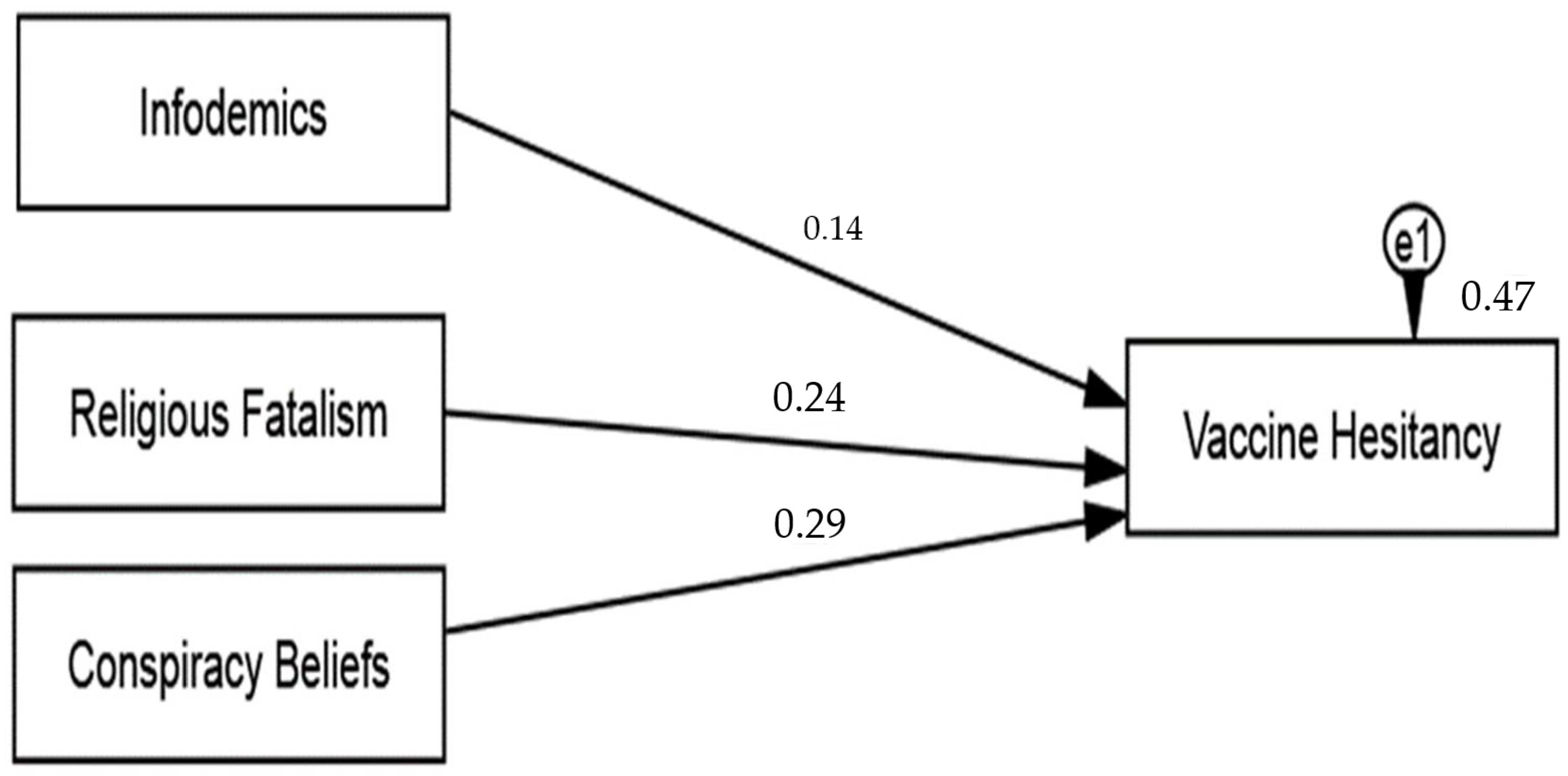
4.4. Hypothesis Testing
4.5. Moderating Analysis
5. Discussion
5.1. Infodemic and Vaccine Hesitancy towards COVID-19
5.2. Conspiracy Belief and Vaccine Hesitancy towards COVID-19
5.3. Religious Fatalism and Vaccine Hesitancy towards COVID-19
5.4. Demographics
5.5. Managerial Implications
5.6. Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barchielli, B.; Cricenti, C.; Gallè, F.; Sabella, E.A.; Liguori, F.; Da Molin, G.; Liguori, G.; Orsi, G.B.; Giannini, A.M.; Ferracuti, S.; et al. Climate changes, natural resources depletion, COVID-19 pandemic, and Russian-Ukrainian war: What is the impact on habits change and mental health? Int. J. Environ. Res. Public Health 2022, 19, 11929. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19) Pandemic. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=CjwKCAjwqJSaBhBUEiwAg5W9p7_L4iwEpXwqQlZyZdSjgRPfrXV0cqCSmYgnrYpzWzL8kR8vFFJ_vxoCGRkQAvD_BwE (accessed on 21 November 2022).
- Gallotti, R.; Valle, F.; Castaldo, N.; Sacco, P.; De Domenico, M. Assessing the risks of ‘infodemics’ in response to COVID-19 epidemics. Nat. Hum. Behav. 2020, 4, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Tangcharoensathien, V.; Calleja, N.; Nguyen, T.; Purnat, T.; D’Agostino, M.; Garcia-Saiso, S.; Landry, M.; Rashidian, A.; Hamilton, C.; Abdallah, A.; et al. Framework for Managing the COVID-19 Infodemic: Methods and Results of an Online, Crowdsourced WHO Technical Consultation. J. Med. Internet Res. 2020, 22, e19659. [Google Scholar] [CrossRef]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Fetzer, J.H. Disinformation: The Use of False Information. Minds Mach. 2004, 14, 231–240. [Google Scholar] [CrossRef]
- Datta, R.; Yadav, A.; Singh, A.; Datta, K.; Bansal, A. The infodemics of COVID-19 amongst healthcare professionals in India. Med. J. Armed Forces India 2020, 76, 276–283. [Google Scholar] [CrossRef]
- Gottlieb, M.; Dyer, S. Information and Disinformation: Social Media in the COVID-19 Crisis. Acad. Emerg. Med. 2020, 27, 640–641. [Google Scholar] [CrossRef] [PubMed]
- Sheng, A.Y.; Gottlieb, M.; Welsh, L. Leveraging learner-centered educational frameworks to combat health mis/disinformation. AEM Educ. Train. 2021, 5, e10711. [Google Scholar] [CrossRef] [PubMed]
- Gelfert, A. Fake News: A Definition. Informal Log. 2018, 38, 84–117. [Google Scholar] [CrossRef]
- Gisondi, M.A.; Barber, R.; Faust, J.S.; Raja, A.; Strehlow, M.C.; Westafer, L.M.; Gottlieb, M. A Deadly Infodemic: Social Media and the Power of COVID-19 Misinformation. J. Med. Internet Res. 2022, 24, e35552. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- WHO. Munich Security Conference. 2020. Available online: https://www.who.int/director-general/speeches/detail/munich-security-conference (accessed on 21 November 2022).
- WHO. Coronavirus COVID-19 Dashboard. 2022. Available online: https://covid19.who.int (accessed on 21 November 2022).
- Raza, S.H.; Yousaf, M.; Sohail, F.; Munawar, R.; Ogadimma, E.C.; Siang, J.M.L.D. Investigating Binge-Watching Adverse Mental Health Outcomes during COVID-19 Pandemic: Moderating Role of Screen Time for Web Series Using Online Streaming. Psychol. Res. Behav. Manag. 2021, 14, 1615–1629. [Google Scholar] [CrossRef]
- Cinelli, M.; Quattrociocchi, W.; Galeazzi, A.; Valensise, C.M.; Brugnoli, E.; Schmidt, A.L.; Zola, P.; Zollo, F.; Scala, A. The COVID-19 social media infodemic. Sci. Rep. 2020, 10, 16598. [Google Scholar] [CrossRef]
- Zhao, Y.; Cheng, S.; Yu, X.; Xu, H. Chinese public’s attention to the COVID-19 epidemic on social media: Observational descriptive study. J. Med. Internet Res. 2020, 22, e18825. [Google Scholar] [CrossRef]
- Larson, H.J. The biggest pandemic risk? Viral misinformation. Nature 2018, 562, 309. [Google Scholar] [CrossRef]
- Mheidly, N.; Fares, J. Leveraging media and health communication strategies to overcome the COVID-19 infodemic. J. Public Health Policy 2020, 41, 410–420. [Google Scholar] [CrossRef]
- Del Vicario, M.; Bessi, A.; Zollo, F.; Petroni, F.; Scala, A.; Caldarelli, G.; Stanley, H.E.; Quattrociocchi, W. The spreading of misinformation online. Proc. Natl. Acad. Sci. USA 2016, 113, 554–559. [Google Scholar] [CrossRef]
- Lazer, D.M.J.; Baum, M.A.; Benkler, Y.; Berinsky, A.J.; Greenhill, K.M.; Menczer, F.; Metzger, M.J.; Nyhan, B.; Pennycook, G.; Rothschild, D.; et al. The science of fake news. Science 2018, 359, 1094–1096. [Google Scholar] [CrossRef]
- Lewandowsky, S.; Ecker, U.K.; Seifert, C.M.; Schwarz, N.; Cook, J. Misinformation and its correction: Continued influence and successful debiasing. Psychol. Sci. Public Interest 2012, 13, 106–131. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, M.; Raza, S.H.; Mahmood, N.; Core, R.; Zaman, U.; Malik, A. Immunity debt or vaccination crisis? A multi-method evidence on vaccine acceptance and media framing for emerging COVID-19 variants. Vaccine 2022, 40, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Raza, S.; Yousaf, M.; Zaman, U.; Siang, J. Can Communication Strategies Combat COVID-19 Vaccine Hesitancy with Trade-Off between Public Service Messages and Public Skepticism? Experimental Evidence from Pakistan. Vaccines 2021, 9, 757. [Google Scholar] [CrossRef] [PubMed]
- Dixon, S. Number of Global Social Network Users 2018–2027. 2022. Available online: https://www.statista.com/statistics/278414/number-of-worldwide-social-network-users/ (accessed on 21 November 2022).
- Uscinski, J.E.; Parent, J.M. American Conspiracy Theories; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Imhoff, R.; Lamberty, P. A Bioweapon or a Hoax? The Link Between Distinct Conspiracy Beliefs About the Coronavirus Disease (COVID-19) Outbreak and Pandemic Behavior. Soc. Psychol. Pers. Sci. 2020, 11, 1110–1118. [Google Scholar] [CrossRef]
- Lazić, A.; Žeželj, I. A systematic review of narrative interventions: Lessons for countering anti-vaccination conspiracy theories and misinformation. Public Underst. Sci. 2021, 30, 644–670. [Google Scholar] [CrossRef]
- Diaz, A.A.; Celedón, J.C. COVID-19 vaccination: Helping the latinx community to come forward. eClinicalMedicine 2021, 35, 100860. [Google Scholar] [CrossRef]
- DW. How Denial and Conspiracy Theories Fuel Coronavirus Crisis in Pakistan. 2020. Available online: https://www.taiwannews.com.tw/en/news/3952923 (accessed on 21 November 2022).
- WHO. Pakistan Situation; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Andrade, G.E.; Hussain, A. Polio in Pakistan: Political, Sociological, and Epidemiological Factors. Cureus 2018, 10, e3502. [Google Scholar] [CrossRef]
- Ittefaq, M.; Baines, A.; Abwao, M.; Shah, S.F.A.; Ramzan, T. “Does Pakistan still have polio cases?”: Exploring discussions on polio and polio vaccine in online news comments in Pakistan. Vaccine 2021, 39, 480–486. [Google Scholar] [CrossRef]
- Raza, S.H.; Emenyeonu, O.C.; Yousaf, M.; Iftikhar, M. Citizen journalism practices during COVID-19 in spotlight: Influence of user-generated contents about economic policies in perceiving government performance. Inf. Discov. Deliv. 2021, 50, 142–154. [Google Scholar] [CrossRef]
- Neely, S.; Eldredge, C.; Sanders, R. Health information seeking behaviors on social media during the COVID-19 pandemic among American social networking site users: Survey study. J. Med. Internet Res. 2021, 23, e29802. [Google Scholar] [CrossRef]
- Melki, J.; Tamim, H.; Hadid, D.; Makki, M.; El Amine, J.; Hitti, E. Mitigating infodemics: The relationship between news exposure and trust and belief in COVID-19 fake news and social media spreading. PLoS ONE 2021, 16, e0252830. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Hmielowski, J.; Yan, W. Clearing the smog? Examining the relationship between traditional media versus nontraditional internet-based media and risk information seeking in China. Int. J. Commun. 2021, 15, 22. [Google Scholar]
- Zhao, Y.C.; Zhao, M.; Song, S. Online Health Information Seeking Behaviors Among Older Adults: Systematic Scoping Review. J. Med. Internet Res. 2022, 24, e34790. [Google Scholar] [CrossRef] [PubMed]
- Assis, S.S.D.d.; Gerlin, M.N.M. Impacts of covid-19 pandemic in the Brazilian research scenario on misinformation: Analysis of publications from information science journals. J. Librariansh. Inf. Sci. 2022, 09610006221133565. [Google Scholar]
- Ngai, C.S.B.; Singh, R.G.; Yao, L. Impact of COVID-19 Vaccine Misinformation on Social Media Virality: Content Analysis of Message Themes and Writing Strategies. J. Med. Internet Res. 2022, 24, e37806. [Google Scholar] [CrossRef]
- Bapaye, J.A.; Bapaye, H.A. Demographic Factors Influencing the Impact of Coronavirus-Related Misinformation on WhatsApp: Cross-sectional Questionnaire Study. JMIR Public Health Surveill. 2021, 7, e19858. [Google Scholar] [CrossRef]
- Ghosh, R.; Ghosh, A. Vaccine equity: A key to global economic recovery. Int. J. Community Med. Public Health 2021, 8, 5837. [Google Scholar] [CrossRef]
- Balakrishnan, V.; Zhen, N.W.; Chong, S.M.; Han, G.J.; Lee, T.J. Infodemic and fake news—A comprehensive overview of its global magnitude during the COVID-19 pandemic in 2021: A scoping review. Int. J. Disaster Risk Reduct. 2022, 78, 103144. [Google Scholar] [CrossRef]
- Allcott, H.; Gentzkow, M. Social Media and Fake News in the 2016 Election. J. Econ. Perspect. 2017, 31, 211–236. [Google Scholar] [CrossRef]
- Visentin, M.; Pizzi, G.; Pichierri, M. Fake news, real problems for brands: The impact of content truthfulness and source credibility on consumers’ behavioral intentions toward the advertised brands. J. Interact. Mark. 2019, 45, 99–112. [Google Scholar] [CrossRef]
- Wang, Y.; McKee, M.; Torbica, A.; Stuckler, D. Systematic Literature Review on the Spread of Health-related Misinformation on Social Media. Soc. Sci. Med. 2019, 240, 112552. [Google Scholar] [CrossRef]
- Faustini, P.H.A.; Covões, T.F. Fake news detection in multiple platforms and languages. Expert Syst. Appl. 2020, 158, 113503. [Google Scholar] [CrossRef]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The Effect of COVID-19 on Youth Mental Health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2020, 51, 1763–1769. [Google Scholar] [CrossRef]
- Karić, T.; Međedović, J. Covid-19 conspiracy beliefs and containment-related behaviour: The role of political trust. Pers. Individ. Differ. 2021, 175, 110697. [Google Scholar] [CrossRef]
- Li, H.O.Y.; Bailey, A.; Huynh, D.; Chan, J. YouTube as a source of information on COVID-19: A pandemic of misinformation? BMJ Glob. Health 2020, 5, e002604. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Douglas, K.M. COVID-19 conspiracy theories. Group Process. Intergroup Relat. 2021, 24, 270–275. [Google Scholar] [CrossRef]
- Barua, Z.; Barua, S.; Aktar, S.; Kabir, N.; Li, M. Effects of misinformation on COVID-19 individual responses and recommendations for resilience of disastrous consequences of misinformation. Prog. Disaster Sci. 2020, 8, 100119. [Google Scholar] [CrossRef]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef]
- Chen, X.; Lin, F.; Cheng, E.W. Stratified Impacts of the Infodemic During the COVID-19 Pandemic: Cross-sectional Survey in 6 Asian Jurisdictions. J. Med. Internet Res. 2022, 24, e31088. [Google Scholar] [CrossRef]
- Lin, F.; Chen, X.; Cheng, E.W. Contextualized impacts of an infodemic on vaccine hesitancy: The moderating role of socioeconomic and cultural factors. Inf. Process. Manag. 2022, 59, 103013. [Google Scholar] [CrossRef]
- Franklin, M.D.; Schlundt, D.G.; Wallston, K.A. Development and Validation of a Religious Health Fatalism Measure for the African-American Faith Community. J. Health Psychol. 2008, 13, 323–335. [Google Scholar] [CrossRef]
- Dettenborn, L.; Duhamel, K.; Butts, G.; Thompson, H.; Jandorf, L. Cancer fatalism and its demographic correlates among African American and Hispanic women: Effects on adherence to cancer screening. J. Psychosoc. Oncol. 2004, 22, 47–60. [Google Scholar] [CrossRef]
- Grinberg, N.; Joseph, K.; Friedland, L.; Swire-Thompson, B.; Lazer, D. Fake news on Twitter during the 2016 U.S. presidential election. Science 2019, 363, 374–378. [Google Scholar] [CrossRef]
- van Prooijen, J.W. Why education predicts decreased belief in conspiracy theories. Appl. Cogn. Psychol. 2017, 31, 50–58. [Google Scholar] [CrossRef]
- Lagoe, C.; Atkin, D. Health anxiety in the digital age: An exploration of psychological determinants of online health information seeking. Comput. Hum. Behav. 2015, 52, 484–491. [Google Scholar] [CrossRef]
- Nghiem, L.T.P.; Papworth, S.; Lim, F.K.S.; Carrasco, L.R. Analysis of the Capacity of Google Trends to Measure Interest in Conservation Topics and the Role of Online News. PLoS ONE 2016, 11, e0152802. [Google Scholar] [CrossRef]
- Faoury, M.; Upile, T.; Patel, N. Using Google Trends to understand information-seeking behaviour about throat cancer. J. Laryngol. Otol. 2019, 133, 610–614. [Google Scholar] [CrossRef]
- Kamiński, M.; Łoniewski, I.; Marlicz, W. Global Internet Data on the Interest in Antibiotics and Probiotics Generated by Google Trends. Antibiotics 2019, 8, 147. [Google Scholar] [CrossRef]
- Mangono, T.; Smittenaar, P.; Caplan, Y.; Huang, V.S.; Sutermaster, S.; Kemp, H.; Sgaier, S.K. Information-Seeking Patterns during the COVID-19 Pandemic across the United States: Longitudinal Analysis of Google Trends Data. J. Med. Internet Res. 2021, 23, e22933. [Google Scholar] [CrossRef] [PubMed]
- Baxter, K.; Courage, C.; Caine, K. Understanding Your Users: A Practical Guide to User Research Methods Interactive Technologies, 2nd ed.; Morgan Kaufmann: Boston, MA, USA, 2015; pp. 264–301. [Google Scholar]
- PBS. Brief on Census -2017; PBS: Islamabad, Pakistan, 2017. [Google Scholar]
- DP, Digital 2022: Pakistan. 2022. Available online: https://datareportal.com/reports/digital-2022-pakistan (accessed on 21 November 2022).
- Islam, M.S.; Sarkar, T.; Khan, S.H.; Kamal, A.H.M.; Hasan, S.M.; Kabir, A.; Yeasmin, D.; Islam, M.A.; Chowdhury, K.I.A.; Anwar, K.S.; et al. COVID-19–related infodemic and its impact on public health: A global social media analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1621. [Google Scholar] [CrossRef] [PubMed]
- Nageeb, S.; Vu, M.; Malik, S.; Quinn, M.T.; Cursio, J.; Padela, A.I. Adapting a religious health fatalism measure for use in Muslim populations. PLoS ONE 2018, 13, e0206898. [Google Scholar] [CrossRef] [PubMed]
- Duong, M.C.; Nguyen, H.; Duong, M. Evaluating COVID-19 vaccine hesitancy: A qualitative study from Vietnam. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102363. [Google Scholar] [CrossRef] [PubMed]
- Almanasreh, E.; Moles, R.; Chen, T.F. Evaluation of methods used for estimating content validity. Res. Soc. Adm. Pharm. 2019, 15, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F. Multivariate Data Analysis: A Global Perspective; Pearson: Upper Saddle River, NJ, USA, 2010; Volume 7. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Dawson, J.F. Moderation in Management Research: What, Why, When, and How. J. Bus. Psychol. 2014, 29, 1–19. [Google Scholar] [CrossRef]
- Hossain, M.B.; Alam, Z.; Islam, S.; Sultan, S.; Faysal, M.; Rima, S.; Hossain, A.; Al Mamun, A. COVID-19 vaccine hesitancy among the adult population in Bangladesh: A nationwide cross-sectional survey. PLoS ONE 2021, 16, e0260821. [Google Scholar] [CrossRef] [PubMed]
- Fisman, D.; Patrozou, E.; Carmeli, Y.; Perencevich, E.; Tuite, A.R.; Mermel, L.A. The Geographical Variability of Bacteremia Study Group Geographical Variability in the Likelihood of Bloodstream Infections Due to Gram-Negative Bacteria: Correlation with Proximity to the Equator and Health Care Expenditure. PLoS ONE 2014, 9, e114548. [Google Scholar] [CrossRef]
- Elkalmi, R.M.; Dyab, E.; Suhaimi, A.M.; Blebil, A.Q.; Elnaem, M.H.; Jamshed, S.; Gajdács, M. Attitude, Familiarity and Religious Beliefs about Vaccination among Health Science and Non-Health Science Students in a Malaysian Public University. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1462–1473. [Google Scholar] [CrossRef]
- Khan, S.; Siddique, R.; Shereen, M.A.; Ali, A.; Liu, J.; Bai, Q.; Bashir, N.; Xue, M. Emergence of a novel coronavirus, severe acute respiratory syndrome coronavirus 2: Biology and therapeutic options. J. Clin. Microbiol. 2020, 58, e00187-20. [Google Scholar] [CrossRef] [PubMed]
- Arshad, M.; Hussain, I.; Mahmood, T.; Hayat, K.; Majeed, A.; Imran, I.; Saeed, H.; Iqbal, M.; Uzair, M.; Rehman, A.; et al. A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan. Vaccines 2021, 9, 720. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.Y.; Shin, T.; Son, Y.; Choi, J. Psycho-behavioural factors influencing COVID-19 vaccine hesitancy among Korean adults: The moderating role of age. J. Adv. Nurs. 2022. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S.; Imam, T.; Khushi, M.; Khan, A.; Moni, M.A. How did socio-demographic status and personal attributes influence compliance to COVID-19 preventive behaviours during the early outbreak in Japan? Lessons for pandemic management. Pers. Individ. Differ. 2021, 175, 110692. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Xu, S.; Li, Z.; Liu, G.; Dai, D.; Dong, C. The Evolution and Disparities of Online Attitudes toward COVID-19 Vaccines: Year-long Longitudinal and Cross-sectional Study. J. Med. Internet Res. 2022, 24, e32394. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jain, G.; Tiwari, A.A. Polarised social media discourse during COVID-19 pandemic: Evidence from YouTube. Behav. Inf. Technol. 2022, 1–22. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Mean | SD | |
|---|---|---|---|
| Age (years) | 34.5 | 12.0 | |
| Frequency | Percentage | ||
| Gender | Male | 1344 | 63.4% |
| Female | 776 | 36.6% | |
| Marita status | Single | 850 | 41.1% |
| Married | 1245 | 58.7% | |
| Divorced | 29 | 1.4% | |
| Education | Primary | 307 | 14.5% |
| Secondary | 289 | 14.9% | |
| High school | 308 | 14.5% | |
| Undergraduate | 854 | 40.3% | |
| Postgraduate | 362 | 17.1% | |
| Family Income | Lower class | 253 | 11.9% |
| Middle class | 328 | 15.5% | |
| Upper MC | 519 | 24.5% | |
| Upper class | 1020 | 48.1% | |
| Variables | Infodemics Status | Conspiracy Belief | Religious Fatalism | Vaccine Hesitancy |
|---|---|---|---|---|
| Infodemics | 1 | |||
| Conspiracy belief | 0.130 | 1 | ||
| Religious fatalism | 0.344 | 0.255 | 1 | |
| Vaccine hesitancy | 0.184 | 0.283 | 0.179 | 1 |
| Variables | Estimate |
|---|---|
| Infodemics | |
| ID1 | 0.93 |
| ID2 | 0.81 |
| ID3 | 0.74 |
| ID4 | 0.88 |
| ID5 | 0.47 * |
| Conspiracy Beliefs | |
| CB1 | 0.85 |
| CB2 | 0.77 |
| CB3 | 0.89 |
| CB4 | 0.87 |
| CB5 | 0.81 |
| CB6 | 0.39 * |
| Religious Fatalism | |
| RF1 | 0.84 |
| RF2 | 0.76 |
| RF3 | 0.87 |
| RF4 | 0.81 |
| Vaccine Hesitancy | |
| VHC1 | 0.77 |
| VHC2 | 0.90 |
| VHC3 | 0.86 |
| VHC4 | 0.92 |
| VHC5 | 0.83 |
| Variables | CR | AVE | VHC | CB | ID | RF |
|---|---|---|---|---|---|---|
| Vaccine Hesitancy | 0.932 | 0.736 | 0.877 | |||
| Conspiracy Beliefs | 0.922 | 0.704 | 0.281 | 0.855 | ||
| Infodemics | 0.907 | 0.710 | 0.206 | 0.187 | 0.863 | |
| Religious Fatalism | 0.891 | 0.674 | 0.175 | 0.254 | 0.356 | 0.958 |
| β | T-Value | p | Hypotheses | |||
|---|---|---|---|---|---|---|
| Infodemics- > Vaccine Hesitancy | 0.14 | 3.81 | 0.001 | H1 Accepted | ||
| Conspiracy beliefs- > Vaccine Hesitancy | 0.29 | 7.91 | 0.001 | H2 Accepted | ||
| Religious fatalism- > Vaccine Hesitancy | 0.24 | 4.45 | 0.001 | H3 Accepted | ||
| Moderation Effects | β | Standard Bootstrap Outcomes | Hypothesis | ||||
|---|---|---|---|---|---|---|---|
| T Value | p Value | Male Gradient | Female Gradient | Durbin Watsons Test | |||
| (Gender X Infodemics) → VH | 0.18 | 3.12 | 0.01 | 0.13 | 0.19 | 1.89 | H4(a) Accepted |
| (Gender X CB) → VH | 0.26 | 4.87 | 0.03 | 0.21 | 0.34 | 2.05 | H4(b) Accepted |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, J.; Raza, S.H.; Yousaf, M.; Shah, A.A.; Hussain, I.; Malik, A. How Does Digital Media Search for COVID-19 Influence Vaccine Hesitancy? Exploring the Trade-off between Google Trends, Infodemics, Conspiracy Beliefs and Religious Fatalism. Vaccines 2023, 11, 114. https://doi.org/10.3390/vaccines11010114
Gao J, Raza SH, Yousaf M, Shah AA, Hussain I, Malik A. How Does Digital Media Search for COVID-19 Influence Vaccine Hesitancy? Exploring the Trade-off between Google Trends, Infodemics, Conspiracy Beliefs and Religious Fatalism. Vaccines. 2023; 11(1):114. https://doi.org/10.3390/vaccines11010114
Chicago/Turabian StyleGao, Jiayue, Syed Hassan Raza, Muhammad Yousaf, Amjad Ali Shah, Iltaf Hussain, and Aqdas Malik. 2023. "How Does Digital Media Search for COVID-19 Influence Vaccine Hesitancy? Exploring the Trade-off between Google Trends, Infodemics, Conspiracy Beliefs and Religious Fatalism" Vaccines 11, no. 1: 114. https://doi.org/10.3390/vaccines11010114
APA StyleGao, J., Raza, S. H., Yousaf, M., Shah, A. A., Hussain, I., & Malik, A. (2023). How Does Digital Media Search for COVID-19 Influence Vaccine Hesitancy? Exploring the Trade-off between Google Trends, Infodemics, Conspiracy Beliefs and Religious Fatalism. Vaccines, 11(1), 114. https://doi.org/10.3390/vaccines11010114