
Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report
 , , and
, , and 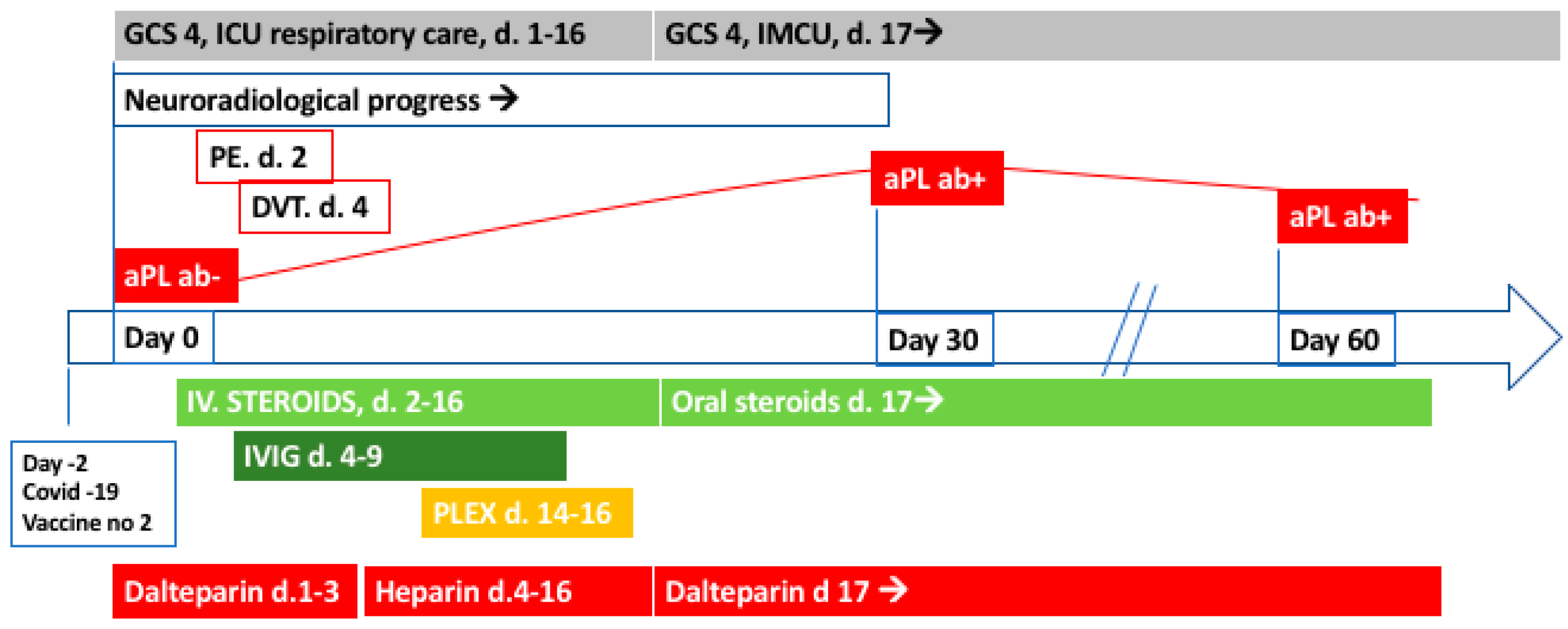{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
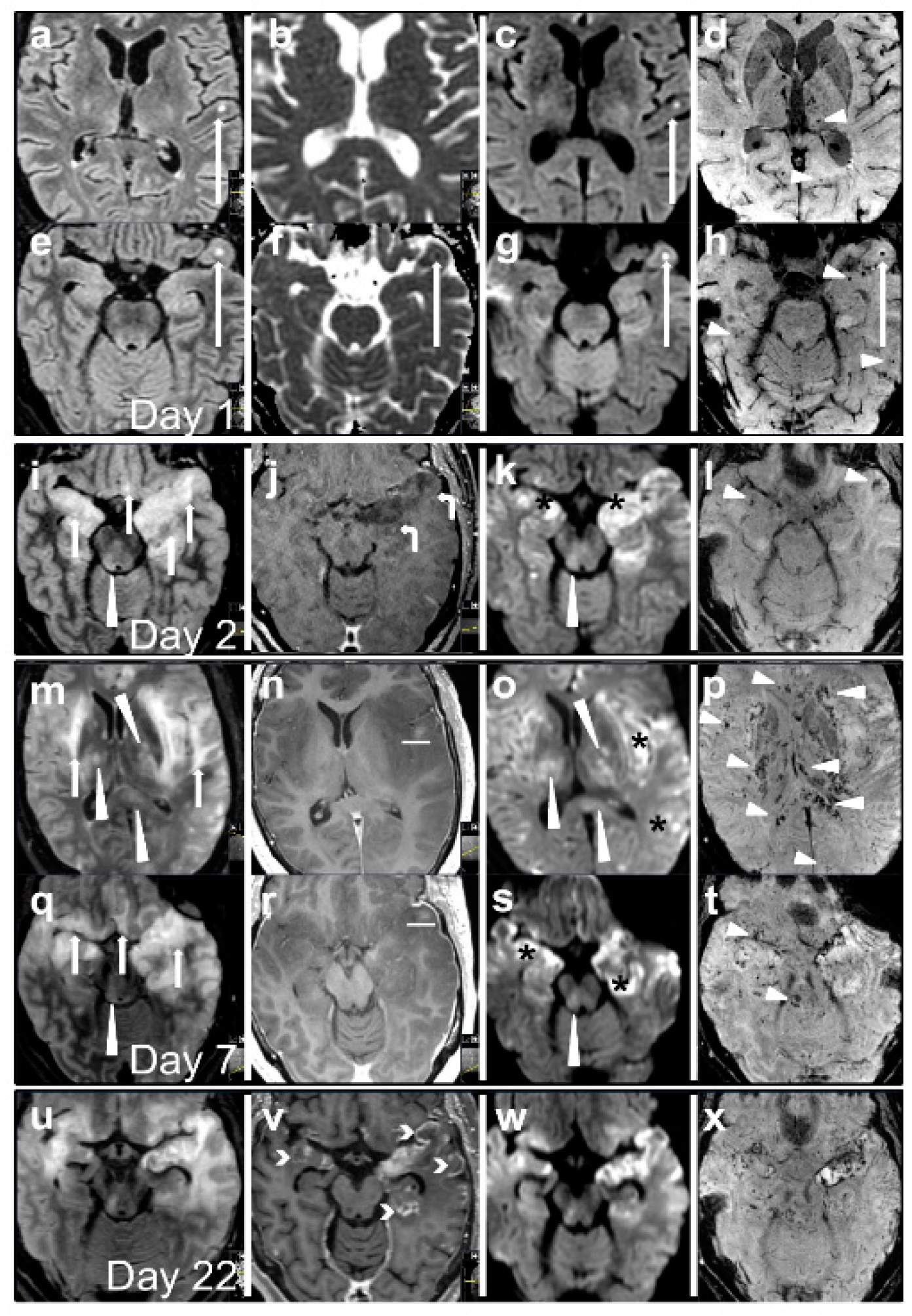
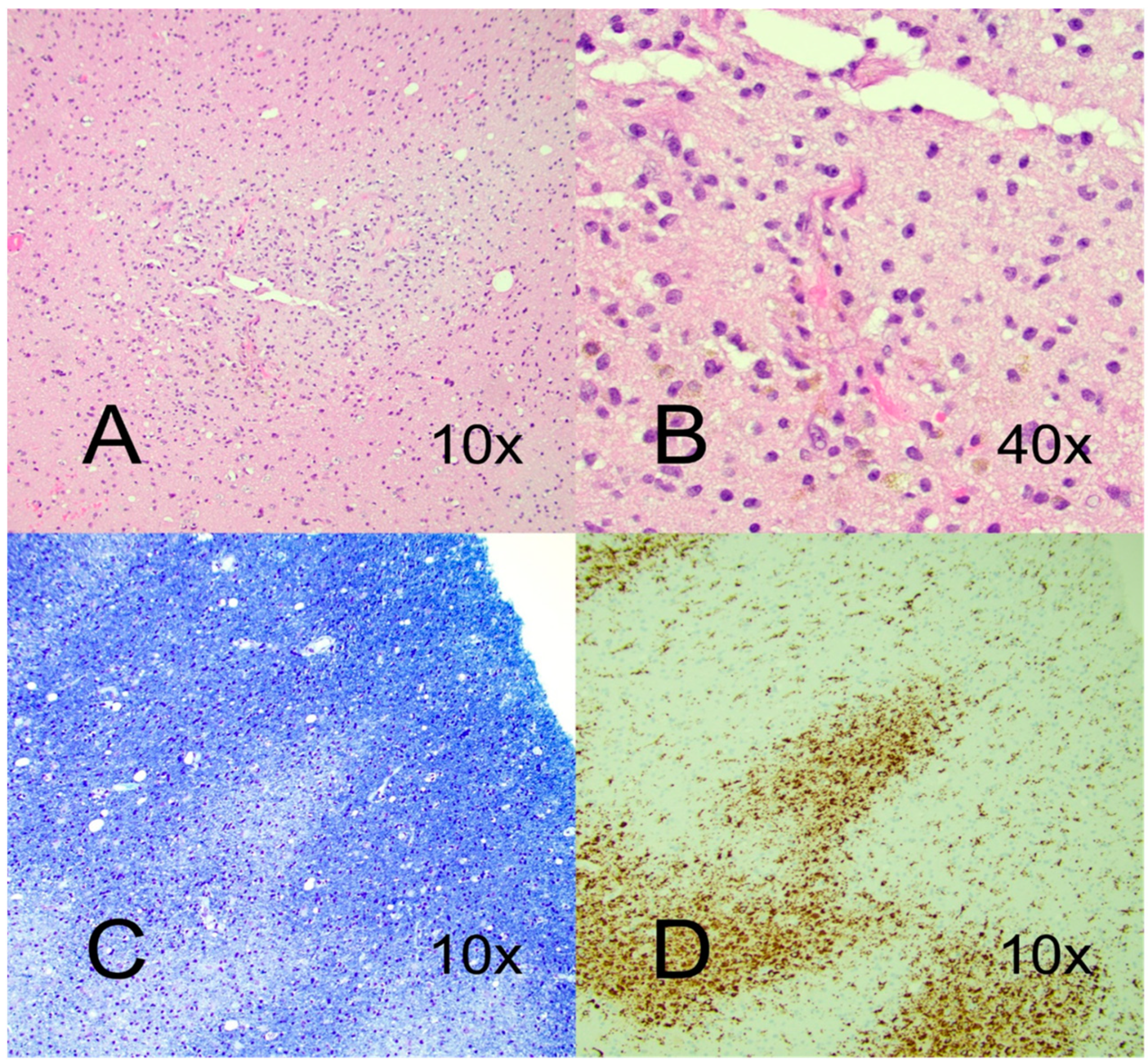
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuperan, S.; Ostrow, P.; Landi, M.K.; Bakshi, R. Acute hemorrhagic leukoencephalitis vs ADEM: FLAIR MRI and neuropathology findings. Neurology 2003, 60, 721–722. [Google Scholar] [CrossRef] [PubMed]
- Sejvar, J.J.; Kohl, K.S.; Bilynsky, R.; Blumberg, D.; Cvetkovich, T.; Galama, J.; Gidudu, J.; Katikaneni, L.; Khuri-Bulos, N.; Oleske, J.; et al. Encephalitis, myelitis, and acute disseminated encephalomyelitis (ADEM): Case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine 2007, 25, 5771–5792. [Google Scholar] [CrossRef] [PubMed]
- Ancau, M.; Liesche-Starnecker, F.; Niederschweiberer, J.; Krieg, S.M.; Zimmer, C.; Lingg, C.; Kumpfmuller, D.; Ikenberg, B.; Ploner, M.; Hemmer, B.; et al. Case Series: Acute Hemorrhagic Encephalomyelitis after SARS-CoV-2 Vaccination. Front. Neurol. 2021, 12, 820049. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.M.; Gilbert, A.R.; Bieniek, K.F.; Richardson, T.E. COVID-19 Patients with CNS Complications and Neuropathologic Features of Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalopathy. J. Neuropathol. Exp. Neurol. 2021, 80, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.; Samavati, L. Antiphospholipid antibodies in COVID-19: A meta-analysis and systematic review. RMD Open 2021, 7, e001580. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, L.A.; Paterson, R.W.; Moll, R.; Pericleous, C.; Brown, R.; Mehta, P.R.; Athauda, D.; Ziff, O.J.; Heaney, J.; Checkley, A.M.; et al. Antiphospholipid antibodies and neurological manifestations in acute COVID-19: A single-centre cross-sectional study. EClinicalMedicine 2021, 39, 101070. [Google Scholar] [CrossRef] [PubMed]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera RH, W.M.; Krilis, S.A. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Garcia, A.; Pham, M.M.; Crowson, C.S.; Amin, S.; Moder, K.G.; Pruthi, R.K.; Warrington, K.J.; Matteson, E.L. The Epidemiology of Antiphospholipid Syndrome: A Population-Based Study. Arthritis Rheumatol. 2019, 71, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Graf, J. Central Nervous System Manifestations of Antiphospholipid Syndrome. Rheum. Dis. Clin. N. Am. 2017, 43, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Tardieu, M.; Banwell, B.; Wolinsky, J.S.; Pohl, D.; Krupp, L.B. Consensus definitions for pediatric MS and other demyelinating disorders in childhood. Neurology 2016, 87, S8–S11. [Google Scholar] [CrossRef] [PubMed]
- Martins, H.M.; Teixeira, A.L., Jr.; Lana-Peixoto, M.A.; Brazilian Committee for, T.; Research in Multiple, S. Acute hemorrhagic leukoencephalitis mimicking herpes simplex encephalitis: Case report. Arq. Neuropsiquiatr. 2004, 62, 139–143. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Boulouis, G.; de Boysson, H.; Zuber, M.; Guillevin, L.; Meary, E.; Costalat, V.; Pagnoux, C.; Naggara, O.; French Vasculitis, G. Primary Angiitis of the Central Nervous System: Magnetic Resonance Imaging Spectrum of Parenchymal, Meningeal, and Vascular Lesions at Baseline. Stroke 2017, 48, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Borghi, M.O.; Bombaci, M.; Bodio, C.; Lonati, P.A.; Gobbini, A.; Lorenzo, M.; Torresani, E.; Dubini, A.; Bulgarelli, I. Anti-Phospholipid Antibodies and Coronavirus Disease 2019: Vaccination Does Not Trigger Early Autoantibody Production in Healthcare Workers. Front. Immunol. 2022, 13, 930074. [Google Scholar] [CrossRef] [PubMed]
- Karakaş, Ö.; Erden, A.; Armağan, B.; Güven, S.C.; Atalar, E.; Polat, B.; Omma, A.; Küçükşahin, O. Evaluation of patients with antiphospholipid syndrome subsequently COVID-19 vaccinations: A retrospective cohort study. Int. J. Rheum. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.E.; Gorman, M.J.; Zhu, D.Y.; Carreno, J.M.; Yuan, D.; VanBlargan, L.A.; Burdess, S.; Lauffenburger, D.A.; Kim, W.; Turner, J.S.; et al. Reduced antibody activity against SARS-CoV-2 B.1.617.2 delta virus in serum of mRNA-vaccinated individuals receiving tumor necrosis factor-alpha inhibitors. Med 2021, 2, 1327–1341.e4. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Mohamed, M.S.; Moulin, T.C.; Schioth, H.B. Neurological manifestations of COVID-19: A comprehensive literature review and discussion of mechanisms. J. Neuroimmunol. 2021, 358, 577658. [Google Scholar] [CrossRef] [PubMed]
- Talotta, R.; Robertson, E.S. Antiphospholipid antibodies and risk of post-COVID-19 vaccination thrombophilia: The straw that breaks the camel’s back? Cytokine Growth Factor Rev. 2021, 60, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Torres, V.; Gutiérrez, Á.; Valdenebro, M.; Ortega, A.; Cítores, M.J.; Montero, E. Catastrophic antiphospholipid syndrome triggered by mRNA COVID-19 vaccin. Clin. Exp. Rheumatol. 2022, 40, 1054–1055. [Google Scholar] [CrossRef] [PubMed]
- Jinno, S.; Naka, I.; Nakazawa, T. Catastrophic antiphospholipid syndrome complicated with essential thrombocythaemia after COVID-19 vaccination: In search of the underlying mechanism. Rheumatol. Adv. Pract. 2021, 5, rkab096. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kits, A.; Pantalone, M.R.; Illies, C.; Antovic, A.; Landtblom, A.-M.; Iacobaeus, E. Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report. Vaccines 2022, 10, 2046. https://doi.org/10.3390/vaccines10122046
Kits A, Pantalone MR, Illies C, Antovic A, Landtblom A-M, Iacobaeus E. Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report. Vaccines. 2022; 10(12):2046. https://doi.org/10.3390/vaccines10122046
Chicago/Turabian StyleKits, Annika, Mattia Russel Pantalone, Christopher Illies, Aleksandra Antovic, Anne-Marie Landtblom, and Ellen Iacobaeus. 2022. "Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report" Vaccines 10, no. 12: 2046. https://doi.org/10.3390/vaccines10122046
APA StyleKits, A., Pantalone, M. R., Illies, C., Antovic, A., Landtblom, A.-M., & Iacobaeus, E. (2022). Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report. Vaccines, 10(12), 2046. https://doi.org/10.3390/vaccines10122046