
Evaluation of the Efficacy of COVID-19 Booster Vaccinations in Healthcare Personnel
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Materials
2.2. Study Protocol
2.3. Laboratory Protocol
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
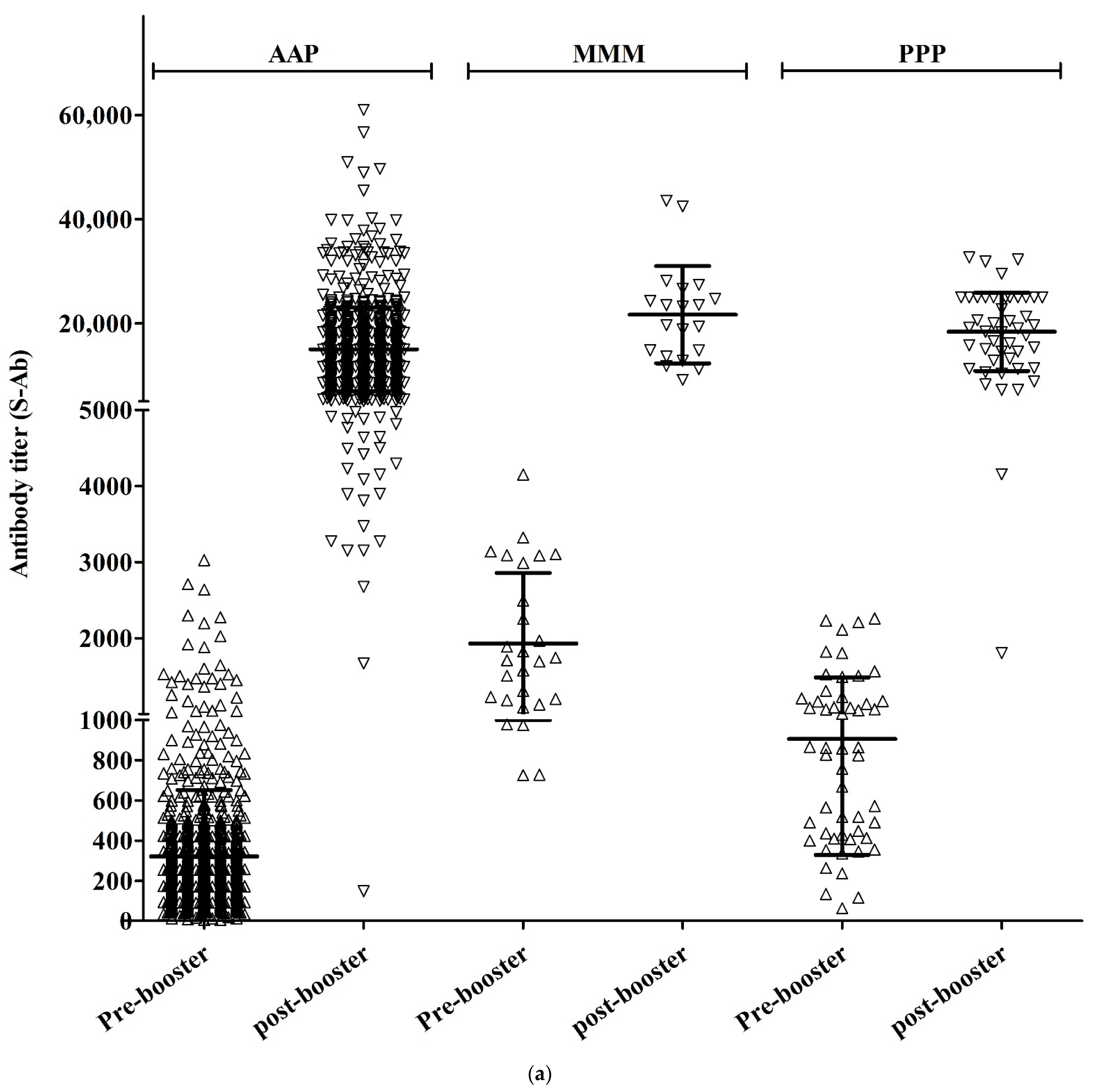
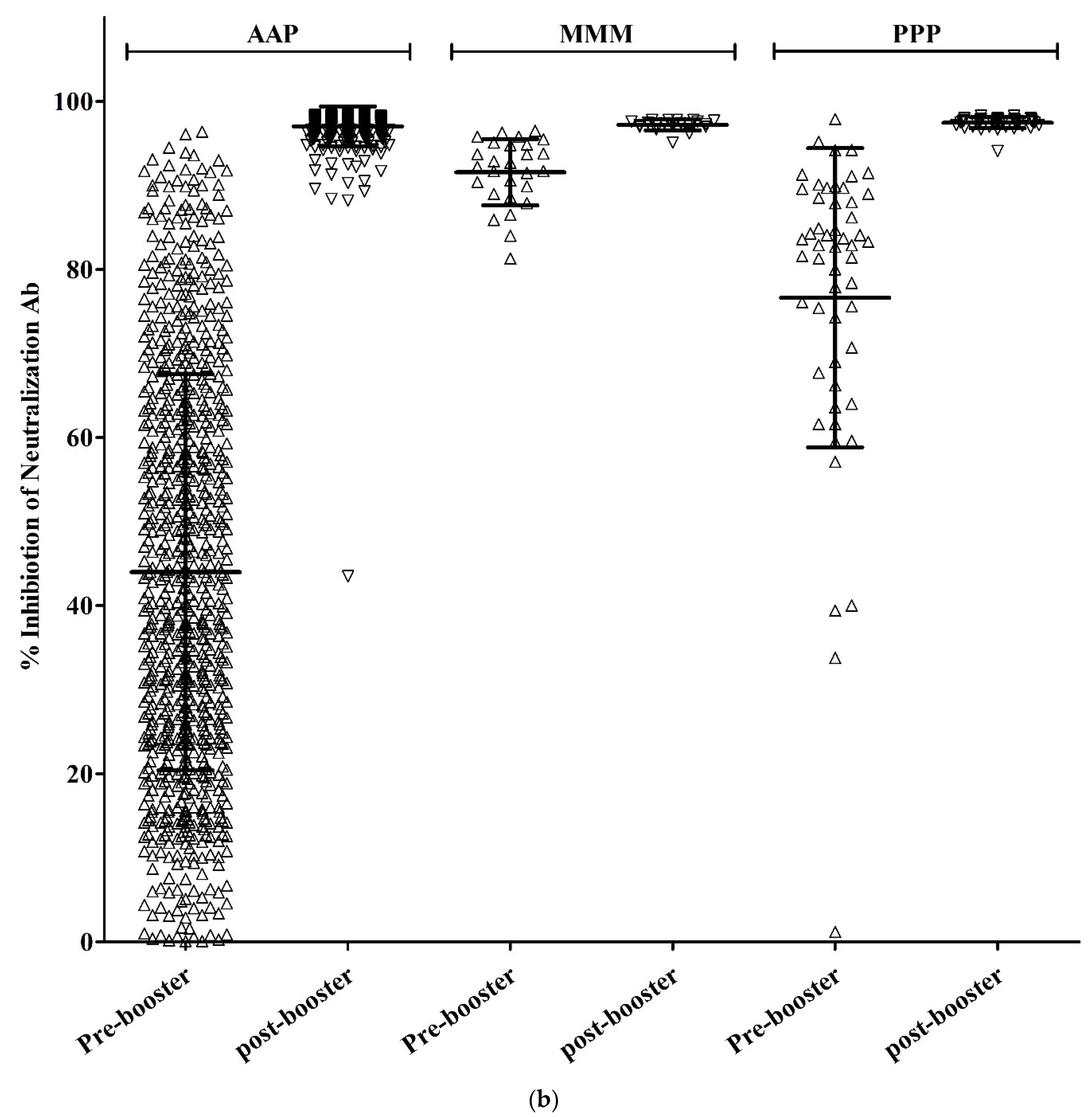
3.2. Results of Antibody Analysis
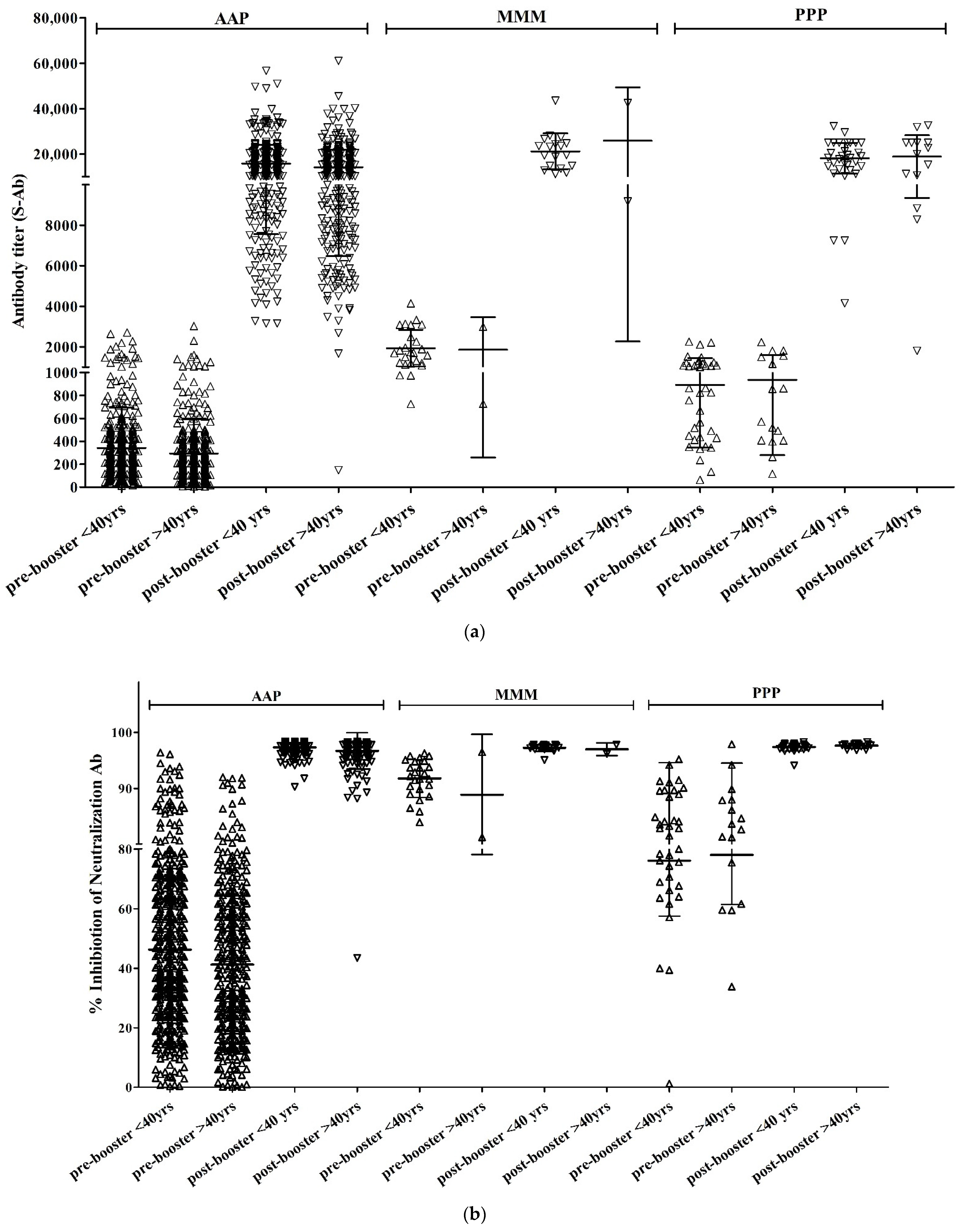
3.3. Results of Antibody Analysis by Subgroup
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Buera, F.J.; Fattal-Jaef, R.N.; Hopenhayn, H.; Neumeyer, P.A.; Shin, Y. The Economic Ripple Effects of COVID-19; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Iacus, S.M.; Natale, F.; Santamaria, C.; Spyratos, S.; Vespe, M. Estimating and projecting air passenger traffic during the COVID-19 coronavirus outbreak and its socio-economic impact. Saf. Sci. 2020, 129, 104791. [Google Scholar] [CrossRef] [PubMed]
- Salasc, F.; Lahlali, T.; Laurent, E.; Rosa-Calatrava, M.; Pizzorno, A. Treatments for COVID-19: Lessons from 2020 and new therapeutic options. Curr. Opin. Pharmacol. 2022, 62, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Okoli, G.N.; Rabbani, R.; Al-Juboori, A.; Copstein, L.; Askin, N.; Abou-Setta, A.M. Antiviral drugs for coronavirus disease 2019 (COVID-19): A systematic review with network meta-analysis. Expert Rev. Anti-Infect. Ther. 2022, 20, 267–278. [Google Scholar] [CrossRef]
- van de Veerdonk, F.L.; Giamarellos-Bourboulis, E.; Pickkers, P.; Derde, L.; Leavis, H.; van Crevel, R.; Engel, J.J.; Wiersinga, W.J.; Vlaar, A.P.J.; Shankar-Hari, M.; et al. A guide to immunotherapy for COVID-19. Nat. Med. 2022, 28, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; McPhee, R.; Huang, W.; Bennett, H.; Pajon, R.; Nestorova, B.; Leav, B.; mRNA-1273 Study Group. A preliminary report of a randomized controlled phase 2 trial of the safety and immunogenicity of mRNA-1273 SARS-CoV-2 vaccine. Vaccine 2021, 39, 2791–2799. [Google Scholar] [CrossRef] [PubMed]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A.; et al. BNT162b2 vaccine induces neutralizing antibodies and poly-specific T cells in humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Pierobon, A.; Zotto, A.D.; Antico, A.; De Antoni, M.E.; Vianello, L.; Gennari, M.; Di Caprio, A.; Russo, F.; Brambilla, G.; Saugo, M. Outbreak of SARS-CoV-2 B.1.617.2 (delta) variant in a nursing home 28 weeks after two doses of mRNA anti-COVID-19 vaccines: Evidence of a waning immunity. Clin. Microbiol. Infect. 2022, 28, 614.e5. [Google Scholar] [CrossRef]
- Scott, J.; Richterman, A.; Cevik, M. Covid-19 vaccination: Evidence of waning immunity is overstated. BMJ 2021, 374, n2320. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Moreira Jr, E.D.; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W. Safety and efficacy of a third dose of BNT162b2 COVID-19 vaccine. N. Engl. J. Med. 2022, 386, 1910–1921. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E. Homologous and heterologous Covid-19 booster vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Puzniak, L.; Hong, V.; Frankland, T.B.; Ackerson, B.K.; Takhar, H.S.; Ogun, O.A.; Simmons, S.R.; Zamparo, J.M. Effectiveness of a third dose of BNT162b2 mRNA COVID-19 vaccine in a large US health system: A retrospective cohort study. Lancet Reg. Health Am. 2022, 9, 100198. [Google Scholar] [CrossRef]
- Munro, A.P.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef]
- Du, Y.; Chen, L.; Shi, Y. Booster COVID-19 vaccination against the SARS-CoV-2 Omicron variant: A systematic review. Hum. Vaccin. Immunother. 2022, 18, 2062983. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of Covid-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Moncunill, G.; Aguilar, R.; Ribes, M.; Ortega, N.; Rubio, R.; Salmerón, G.; Molina, M.J.; Vidal, M.; Barrios, D.; Mitchell, R.A.; et al. Determinants of early antibody responses to COVID-19 mRNA vaccines in a cohort of exposed and naïve healthcare workers. eBioMedicine 2022, 75, 103805. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2–spike protein–protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Riester, E.; Majchrzak, M.; Mühlbacher, A.; Tinguely, C.; Findeisen, P.; Hegel, J.K.; Laimighofer, M.; Rank, C.M.; Schönfeld, K.; Langen, F.; et al. Multicentre Performance Evaluation of the Elecsys Anti-SARS-CoV-2 Immunoassay as an Aid in Determining Previous Exposure to SARS-CoV-2. Infect. Dis. Ther. 2021, 10, 2381–2397. [Google Scholar] [CrossRef] [PubMed]
- Hillus, D.; Schwarz, T.; Tober-Lau, P.; Vanshylla, K.; Hastor, H.; Thibeault, C.; Jentzsch, S.; Helbig, E.T.; Lippert, L.J.; Tscheak, P.; et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: A prospective cohort study. Lancet. Respir. Med. 2021, 9, 1255–1265. [Google Scholar] [CrossRef]
- Glück, V.; Tydykov, L.; Mader, A.-L.; Warda, A.-S.; Bertok, M.; Weidlich, T.; Gottwald, C.; Köstler, J.; Salzberger, B.; Wagner, R.; et al. Humoral immunity in dually vaccinated SARS-CoV-2-naïve individuals and in booster-vaccinated COVID-19-convalescent subjects. Infection 2022. [Google Scholar] [CrossRef]
- Löfström, E.; Eringfält, A.; Kötz, A.; Wickbom, F.; Tham, J.; Lingman, M.; Nygren, J.M.; Undén, J. Dynamics of IgG-avidity and antibody levels after Covid-19. J. Clin. Virol. 2021, 144, 104986. [Google Scholar] [CrossRef]
- Pratesi, F.; Caruso, T.; Testa, D.; Tarpanelli, T.; Gentili, A.; Gioè, D.; Migliorini, P. BNT162b2 mRNA SARS-CoV-2 Vaccine Elicits High Avidity and Neutralizing Antibodies in Healthcare Workers. Vaccines 2021, 9, 672. [Google Scholar] [CrossRef]
- Gilboa, M.; Regev-Yochay, G.; Mandelboim, M.; Indenbaum, V.; Asraf, K.; Fluss, R.; Amit, S.; Mendelson, E.; Doolman, R.; Afek, A.; et al. Durability of Immune Response After COVID-19 Booster Vaccination and Association with COVID-19 Omicron Infection. JAMA Netw. Open 2022, 5, e2231778. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | AAP (N = 837) | MMM (N = 27) | PPP (N = 53) | p |
|---|---|---|---|---|
| Age (mean, ±SD) | 39.5 (11.9) | 28.0 (7.3) | 35.8 (9.9) | <0.001 |
| Sex (male, n, %) | 153 (18.3) | 6 (22.2) | 13 (24.5) | 0.473 |
| Pre-booster vaccination (n, %) | ||||
| S-Ab positive | 837 (100) | 27 (100) | 53 (100) | N.A |
| N-Ab positive | 7 (0.8) | 0 | 0 | 0.714 |
| Neut.Ab positive | 566 (67.6) | 27 (100) | 52 (98.1) | <0.001 |
| Pre-booster vaccination (mean, SD) | ||||
| S-Ab titer | 228.8 (2.4) | 1723.8 (1.6) | 712.0 (2.2) | <0.001 |
| Neut.Ab titer (% of inhibition) | 44.2 (23.8) | 91.6 (3.9) | 76.6 (17.8) | <0.001 |
| S-Ab titer * | 226.1 (2.3) † | 1723.8 (1.6) | 712.0 (2.2) | <0.001 |
| Neut.Ab titer * (% of inhibition) | 44.0 (23.6) † | 91.6 (3.9) | 76.6 (17.8) | <0.001 |
| Post-booster vaccination (mean, SD) | ||||
| S-Ab titer | 13,088.6 (1.7) ‡ | 19,932.3 (1.5) § | 16,360.1 (1.7) # | <0.001 |
| Neut.Ab titer (% of inhibition) | 97.0 (2.4) ‡ | 97.2 (0.6) § | 97.5 (0.6) # | 0.400 |
| S-Ab titer * | 13,105.7 (1.7) ‡ | 19,932.3 (1.5) § | 16,360.1 (1.7) # | <0.001 |
| Neut.Ab titer * (% of inhibition) | 97.0 (2.4) ‡ | 97.2 (0.6) § | 97.5 (0.6) # | 0.404 |
| AAP | MMM | PPP | p-Value | |
|---|---|---|---|---|
| Subjects with no prior COVID-19 infection (age ≤ 40) | ||||
| No. of cases with pre-booster vaccination test | 452 | 25 | 37 | |
| No. of cases with post-booster vaccination test | 340 | 18 | 32 | |
| Pre-booster S-Ab positivity (n, %) | 452 (100%) | 25 (100%) | 37 (100%) | N.A |
| Post-booster S-Ab positivity (n, %) | 340 (100%) | 18 (100%) | 32 (100%) | N.A |
| Pre-booster S-Ab titer (mean, ±SD) | 245.8 (±2.2) | 1745.3 (±1.6) | 711.9 (±2.1) | <0.001 |
| Post-booster S-Ab titer (mean, ±SD) | 13,942.5 (±1.6) | 19,952.3 (±1.4) | 16,762.5 (±1.6) | 0.003 |
| Pre-booster Neut.Ab positivity (n, %) | 329 (72.8%) | 25 (100%) | 36 (97.3%) | <0.001 |
| Post-booster Neut.Ab positivity (n, %) | 340 (100%) | 18 (100%) | 32 (100%) | N.A |
| Pre-booster Neut.Ab titer * (mean, ±SD) | 46.3 (±23.7) | 91.8 (±3.4) | 76.1 (±18.5) | <0.001 |
| Post-booster Neut.Ab titer * (mean, ±SD) | 97.3 (±0.9) | 97.2 (±0.6) | 97.4 (±0.7) | 0.803 |
| Post-booster N-Ab positivity (n, %) | 1 (0.1%) | 0 | 0 | N.A |
| Subjects with no prior COVID-19 infection (age > 40) | ||||
| No. of cases with pre-booster vaccination test | 378 | 2 | 16 | |
| No. of cases with post-booster vaccination test | 334 | 2 | 14 | |
| Pre-booster S-Ab positivity (n, %) | 378 (100%) | 2 (100%) | 16 (100%) | N.A |
| Post-booster S-Ab positivity (n, %) | 334 (100%) | 2 (100%) | 14 (100%) | N.A |
| Pre-booster S-Ab titer (mean, ±SD) | 204.5 (±2.4) | 1475.6 (±2.7) | 712.3 (±2.3) | <0.001 |
| Post-booster S-Ab titer (mean, ±SD) | 12,303.0 (±1.8) | 19,743.9 (±3.0) | 15,473.8 (±2.2) | 0.203 |
| Pre-booster Neut.Ab positivity (n, %) | 231 (61.1%) | 2 (100%) | 16 (100%) | 0.004 |
| Post-booster Neut.Ab positivity (n, %) | 334 (100%) | 2 (100%) | 14 (100%) | N.A |
| Pre-booster Neut.Ab titer * (mean, ±SD) | 41.2 (±23.1) | 88.9 (±10.7) | 78.0 (±16.5) | <0.001 |
| Post-booster Neut.Ab titer * (mean, ±SD) | 96.7 (±3.2) | 97.0 (±1.1) | 97.6 (±0.5) | 0.566 |
| Post-booster N-Ab positivity (n, %) | 0 | 0 | 0 | N.A |
| Age 40 or Less | Age over 40 | p-Value | |
|---|---|---|---|
| AAP | |||
| Pre-booster S-Ab titer (mean, ±SD) | 245.8 (±2.2) | 204.5 (±2.4) | 0.002 |
| Post-booster S-Ab titer (mean, ±SD) | 13,942.5 (±1.6) | 12,303.0 (±1.8) | 0.003 |
| Pre-booster Neut.Ab (mean, ±SD), (% of inhibition) | 46.3 (±23.7) | 41.2 (±23.1) | 0.002 |
| Post-booster Neut.Ab (mean, ±SD), (% of inhibition) | 97.3 (±0.9) | 96.7 (±3.2) | 0.001 |
| MMM | |||
| Pre-booster S-Ab titer (mean, ±SD) | 1745.3 (±1.6) | 1475.6 (±2.7) | 0.852 |
| Post-booster S-Ab titer (mean, ±SD) | 19,952.3 (±1.4) | 19,743.9 (±3.0) | 0.974 |
| Pre-booster Neut.Ab (mean, ±SD), (% of inhibition) | 91.8 (±3.4) | 88.9 (±10.7) | 1.00 |
| Post-booster Neut.Ab (mean, ±SD), (% of inhibition) | 97.2 (±0.6) | 97.0 (±1.1) | 0.947 |
| PPP | |||
| Pre-booster S-Ab titer (mean, ±SD) | 711.9 (±2.1) | 712.3 (±2.3) | 0.998 |
| Post-booster S-Ab titer (mean, ±SD) | 16,762.5 (±1.6) | 15,473.8 (±2.2) | 0.659 |
| Pre-booster Neut.Ab (mean, ±SD), (% of inhibition) | 76.1 (±18.5) | 78.0 (±16.5) | 0.722 |
| Post-booster Neut.Ab (mean, ±SD), (% of inhibition) | 97.4 (±0.7) | 97.6 (±0.5) | 0.277 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.-J.; Bae, J.-Y.; Jun, K.-I.; Kim, J.; Son, H.-J.; Chung, H.-S.; Kim, S.-K.; Kim, S.; Minn, D.; Choi, H.-J. Evaluation of the Efficacy of COVID-19 Booster Vaccinations in Healthcare Personnel. Vaccines 2022, 10, 1797. https://doi.org/10.3390/vaccines10111797
Kim C-J, Bae J-Y, Jun K-I, Kim J, Son H-J, Chung H-S, Kim S-K, Kim S, Minn D, Choi H-J. Evaluation of the Efficacy of COVID-19 Booster Vaccinations in Healthcare Personnel. Vaccines. 2022; 10(11):1797. https://doi.org/10.3390/vaccines10111797
Chicago/Turabian StyleKim, Chung-Jong, Ji-Yun Bae, Kang-Il Jun, Jihee Kim, Hee-Jung Son, Hae-Sun Chung, Soo-Kyung Kim, Soohyun Kim, Dohsik Minn, and Hee-Jung Choi. 2022. "Evaluation of the Efficacy of COVID-19 Booster Vaccinations in Healthcare Personnel" Vaccines 10, no. 11: 1797. https://doi.org/10.3390/vaccines10111797
APA StyleKim, C.-J., Bae, J.-Y., Jun, K.-I., Kim, J., Son, H.-J., Chung, H.-S., Kim, S.-K., Kim, S., Minn, D., & Choi, H.-J. (2022). Evaluation of the Efficacy of COVID-19 Booster Vaccinations in Healthcare Personnel. Vaccines, 10(11), 1797. https://doi.org/10.3390/vaccines10111797