Effect of Influenza Vaccine on Prevention of Acute Attack of Chronic Airway Disease in Elderly Population


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Exposures
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Description of Participants
3.2. Comparison of Acute Exacerbation of Chronic Airway Disease in Trivalent-Influenza-Vaccination Group before and after Vaccination for One Year
3.3. Comparison of Acute Exacerbation of Chronic Airway Disease in Tetravalent-Influenza-Vaccination Group before and after Vaccination for One Year
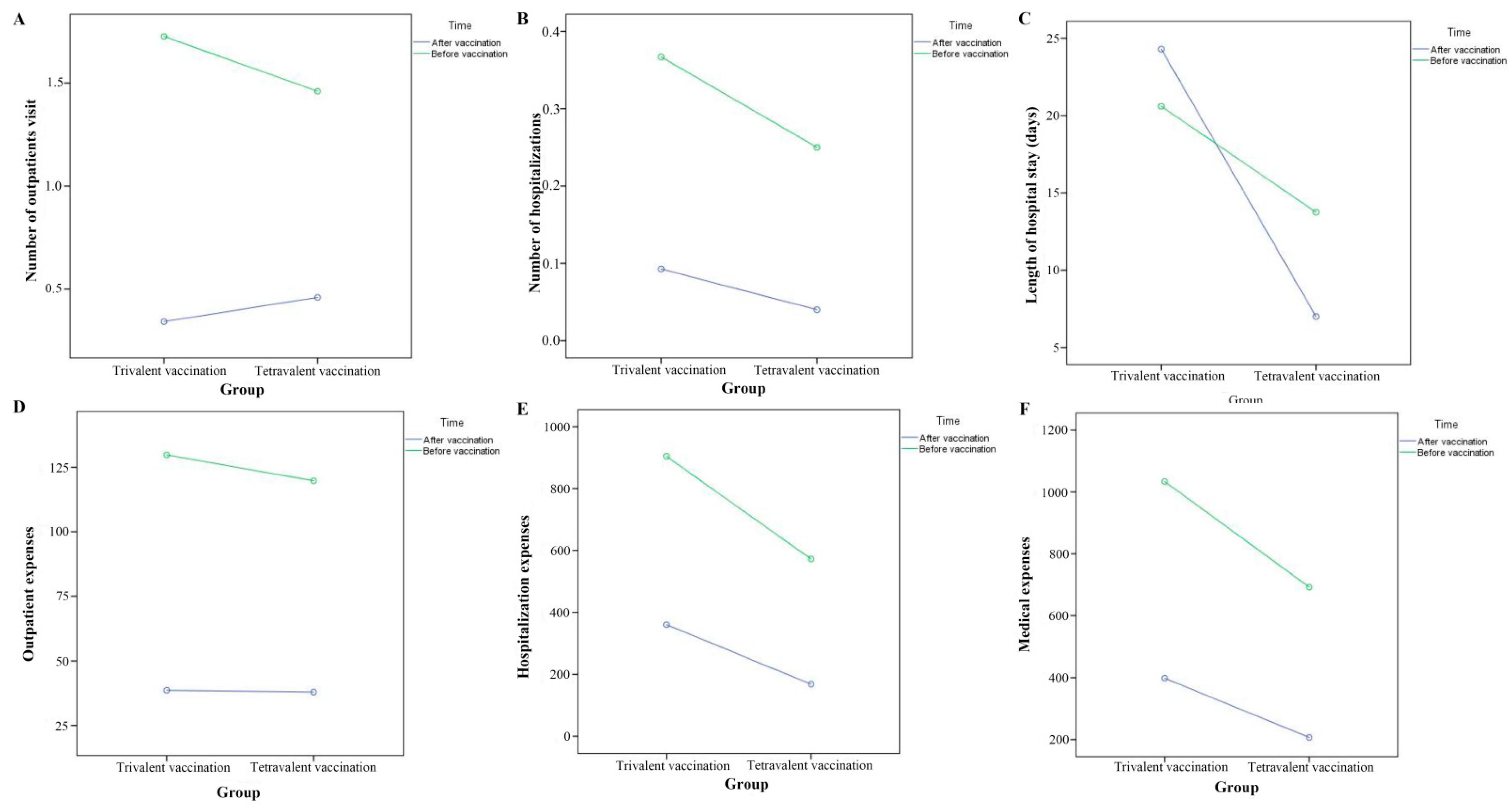
3.4. Comparison of Protection Effect in Different Influenza-Vaccination Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burgel, P.R.; Bergeron, A.; de Blic, J.; Bonniaud, P.; Bourdin, A.; Chanez, P.; Chinet, T.; Dalphin, J.-C.; Devillier, P.; Deschildre, A.; et al. Small airways diseases, excluding asthma and COPD: An overview. Eur. Respir. Rev. 2013, 22, 131–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negewo, N.A.; Gibson, P.G.; McDonald, V.M. COPD and its comorbidities: Impact, measurement and mechanisms. Respirology 2015, 20, 1160–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death/ (accessed on 9 December 2020).
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/asthma/ (accessed on 20 May 2020).
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd)/ (accessed on 1 December 2017).
- Ferkol, T.; Schraufnagel, D. The global burden of respiratory disease. Ann. Am. Thorac. Soc. 2014, 11, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, P.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Wang, L.; Liu, Y.; Yin, P.; et al. Cause-specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 251–272. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Mulpuru, S.; Li, L.; Ye, L.; Hatchette, T.; Andrew, M.K.; Ambrose, A.; Boivin, G.; Bowie, W.; Chit, A.; Santos, G.D.; et al. Effectiveness of Influenza Vaccination on Hospitalizations and Risk Factors for Severe Outcomes in Hospitalized Patients With COPD. Chest 2019, 155, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Kopsaftis, Z.; Wood-Baker, R.; Poole, P. Influenza vaccine for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst. Rev. 2018, 6, CD002733. [Google Scholar] [CrossRef]
- Bao, W.; Li, Y.; Wang, T.; Li, X.; He, J.; Wang, Y.; Wen, F.; Chen, J. Effects of influenza vaccination on clinical outcomes of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 68, 101337. [Google Scholar] [CrossRef] [PubMed]
- Chinese Center for Disease Control and Prevention. Technical Guidelines for Influenza Vaccination in China (2019–2020). Chin. J. Viral Diseases 2019, 6, 1–10. [Google Scholar]
- Chronic obstructive pulmonary Disease Group, Chinese Society of Respiratory Medicine; Chronic obstructive pulmonary Disease Working Committee of Respiratory Physicians Branch of Chinese Medical Doctor Association. Guidelines for the Diagnosis and Treatment of chronic obstructive Pulmonary Disease (revised 2021). Chin. J. Tuberc. Respir. Diseases. 2021, 44, 170–205. [Google Scholar]
- Ge, J.; Jian, Y.; Wang, C. Internal Medicine, 9th ed.; People’s Sanitary Publishing Press: Beijing, China, 2020. [Google Scholar]
- Li, Y.; Zhang, P.; An, Z.; Yue, C.; Wang, Y.; Liu, Y.; Yuan, X.; Ma, Y.; Li, K.; Yin, Z.; et al. Effectiveness of influenza and pneumococcal vaccines on chronic obstructive pulmonary disease exacerbations. Respirology. 2022, 27, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Wongsurakiat, P.; Maranetra, K.N.; Wasi, C.; Kositanont, U.; Dejsomritrutai, W.; Charoenratanakul, S. Acute respiratory illness in patients with COPD and the effectiveness of influenza vaccination: A randomized controlled study. Chest 2004, 125, 2011–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bafadhel, M.; McKenna, S.; Terry, S.; Mistry, V.; Reid, C.; Haldar, P.; McCormick, M.; Haldar, K.; Kebadze, T.; Duvoix, A.; et al. Acute exacerbations of chronic obstructive pulmonary disease: Identification of biologic clusters and their biomarkers. Am. J. Respir. Crit. Care Med. 2011, 184, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Zhang, W.; Hu, H.; Zhang, M.; He, Y.; Li, Z. Associations between ambient air pollution and hospitalizations for acute exacerbation of chronic obstructive pulmonary disease in Jinhua, 2019. Chemosphere 2021, 267, 128905. [Google Scholar] [CrossRef] [PubMed]
- Wedzicha, J.A.; Donaldson, G.C. Exacerbations of chronic obstructive pulmonary disease. Respir. Care 2003, 48, 1204–1213. [Google Scholar]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary bacterial infections associated with influenza pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef] [Green Version]
- Van der Sluijs, K.F.; van Elden, L.J.; Nijhuis, M.; Schuurman, R.; Pater, J.M.; Florquin, S.; Goldman, M.; Jansen, H.M.; Lutter, R.; van der Poll, T. IL-10 is an important mediator of the enhanced susceptibility to pneumococcal pneumonia after influenza infection. J. Immunol. 2004, 172, 7603–7609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullers, J.A.; Iverson, A.R.; McKeon, R.; Murray, P.J. The platelet activating factor receptor is not required for exacerbation of bacterial pneumonia following influenza. Scand. J. Infect. Diseases. 2008, 40, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Seki, M.; Kosai, K.; Yanagihara, K.; Higashiyama, Y.; Kurihara, S.; Izumikawa, K.; Miyazaki, Y.; Hirakata, Y.; Tashiro, T.; Kohno, S. Disease severity in patients with simultaneous influenza and bacterial pneumonia. Intern. Med. 2007, 46, 953–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voordouw, B.C.; Sturkenboom, M.C.; Dieleman, J.P.; Stijnen, T.; van der Lei, J.; Stricker, B.H. Annual influenza vaccination in community-dwelling elderly individuals and the risk of lower respiratory tract infections or pneumonia. Arch. Intern. Med. 2006, 166, 1980–1985. [Google Scholar] [CrossRef] [Green Version]
- Chow, E.J.; Rolfes, M.A.; Carrico, R.L.; Furmanek, S.; Ramirez, J.A.; Ferdinands, J.M.; Fry, A.M.; Patel, M.M. Vaccine Effectiveness Against Influenza-Associated Lower Respiratory Tract Infections in Hospitalized Adults, Louisville, Kentucky, 2010–2013. Open Forum Infect. Dis. 2020, 7, ofaa262. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.; Miravitlles, M.; Metzdorf, N.; Celli, B. Impact and prevention of severe exacerbations of COPD: A review of the evidence. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 2891–2908. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.C.; Tran, H.V.T.; Nguyen, T.H.; Vo, D.C.; Godin, I.; Michel, O. Identification of Modifiable Risk Factors of Exacerbations Chronic Respiratory Diseases with Airways Obstruction, in Vietnam. Int. J. Env. Res. Public Health 2022, 19, 11088. [Google Scholar] [CrossRef] [PubMed]
- Chinese National Influenza Center. Influenza Weekly Report. Available online: http://ivdc.chinacdc.cn/cnic/zyzx/lgzb/ (accessed on 27 June 2020).


{kind=link}
| Characteristics | All Subjects (n = 348) | Trivalent-Vaccination Group (n = 248) | Tetravalent-Vaccination Group (n = 100) | t/χ2 | P-Value |
|---|---|---|---|---|---|
| Age (years, mean ± SD) | 74.70 ± 5.46 | 74.89 ± 5.49 | 74.22 ± 5.39 | 1.038 | 0.300 |
| Age group (n, %) | |||||
| 66~70 | 92 (26.44) | 64 (25.80) | 28 (28.00) | 2.019 | 0.732 |
| 71~75 | 104 (29.89) | 71 (28.63) | 33 (33.00) | ||
| 76~80 | 98 (28.16) | 71 (28.63) | 27 (27.00) | ||
| 81~85 | 47 (13.50) | 36 (14.52) | 11 (11.00) | ||
| ≥86 | 7 (2.01) | 6 (2.42) | 1 (1.00) | ||
| Sex (n, %) | |||||
| Male | 213 (61.21) | 156 (62.90) | 57 (57.00) | 1.046 | 0.306 |
| Female | 135 (38.79) | 92 (37.10) | 43 (43.00) | ||
| Survival state | |||||
| Death | 14 (4.02) | 12 (4.84) | 2 (2.00) | 0.843 | 0.359 |
| Survival | 334 (95.98) | 236 (95.16) | 98 (98.00) | ||
| Cause of death | |||||
| COPD | 6 (42.86) | 6 (50.00) | 0 (0.00) | 1.241 | 0.265 |
| Lung cancer | 3 (21.43) | 2 (16.67) | 1 (50.00) | NA | 1.000 |
| CHD | 2 (14.29) | 2 (16.67) | 0 (0.00) | NA | 1.000 |
| Gastric cancer | 1 (7.14) | 0 (0.00) | 1 (50.00) | NA | 0.287 |
| MI | 1 (7.14) | 1 (8.33) | 0 (0.00) | NA | 1.000 |
| Suicide | 1 (7.14) | 1 (8.33) | 0 (0.00) | NA | 1.000 |
| Variables | Trivalent-Vaccination Group (n = 248) | Tetravalent-Vaccination Group (n = 100) | Comparison of the Difference between Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| After Vaccination | Before Vaccination | t/χ2 | P-Value | Difference | After Vaccination | Before Vaccination | Z/χ2 | P-Value | Difference | t/χ2 | P-Value | |
| Acute attack * (n, %) | ||||||||||||
| Yes | 37 (14.92) | 136 (54.84) | 87.00 | <0.001 | NA | 12 (12.00) | 32 (32.00) | 11.66 | 0.001 | NA | NA | NA |
| No | 211 (85.08) | 112 (45.16) | NA | 88 (88.00) | 68 (68.00) | NA | NA | NA | ||||
| Status of accessing medical service | ||||||||||||
| Outpatient visits (n, %) | ||||||||||||
| Yes | 28 (11.29) | 112 (45.16) | 70.22 | <0.001 | NA | 10 (10.00) | 22 (22.00) | 5.36 | 0.021 | NA | NA | NA |
| No | 220 (88.71) | 136 (54.84) | NA | 90 (90.00) | 78 (78.00) | NA | NA | NA | ||||
| Number of outpatient visits (mean ± SD) | 0.34 ± 1.29 | 1.73 ± 3.81 | −7.01 | <0.001 | −1.38 ± 3.11 | 0.46 ± 2.24 | 1.46 ± 4.67 | −3.53 | 0.001 | −1.00 ± 2.83 | −1.067 | 0.287 |
| Hospitalization (n, %) | ||||||||||||
| Yes | 15(6.05) | 59(23.79) | 30.75 | <0.001 | NA | 4 (4.00) | 18 (18.00) | 10.01 | 0.002 | NA | NA | NA |
| No | 233(93.95) | 189(76.21) | 96 (96.00) | 82 (82.00) | ||||||||
| Number of hospitalizations (mean ± SD) | 0.09 ± 0.42 | 0.37 ± 0.79 | −6.06 | <0.001 | −0.27 ± 0.71 | 0.04 ± 0.20 | 0.25 ± 0.63 | −3.91 | <0.001 | −0.21 ± 0.54 | −0.914 | 0.362 |
| Medical expenses # (mean ± SD) | 398.41 ± 2219.30 | 1034.03 ± 2430.27 | −3.47 | 0.001 | −635.61 ± 2887.96 | 206.57 ± 947.96 | 692.01 ± 1809.90 | −3.31 | 0.001 | −485.44 ± 1468.22 | −0.495 | 0.621 |
| Outpatient expenses (mean ± SD) | 38.63 ± 160.40 | 129.77 ± 291.80 | −5.05 | <0.001 | −91.15 ± 284.42 | 37.94 ± 200.78 | 119.76 ± 487.07 | −2.65 | 0.009 | −81.82 ± 308.54 | −0.270 | 0.787 |
| Hospitalization expenses (mean ± SD) | 359.79 ± 2196.30 | 904.25 ± 2308.07 | −2.96 | 0.003 | −544.46 ± 2892.95 | 168.63 ± 945.46 | 572.25 ± 1598.37 | −2.96 | 0.004 | −403.62 ± 1361.93 | −0.466 | 0.641 |
| Length of hospital stay (mean ± SD) | 19.79 ± 35.01 | 13.46 ± 8.19 | 0.30 | 0.770 | 3.70 ± 38.91 | 7.00 ± 2.71 | 10.06 ± 6.01 | −1.31 | 0.283 | −6.75 ± 10.34 | 0.518 | 0.614 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, K.; Qu, G.; Zhang, C.; Li, H.; Sun, L. Effect of Influenza Vaccine on Prevention of Acute Attack of Chronic Airway Disease in Elderly Population. Vaccines 2022, 10, 1750. https://doi.org/10.3390/vaccines10101750
Gao K, Qu G, Zhang C, Li H, Sun L. Effect of Influenza Vaccine on Prevention of Acute Attack of Chronic Airway Disease in Elderly Population. Vaccines. 2022; 10(10):1750. https://doi.org/10.3390/vaccines10101750
Chicago/Turabian StyleGao, Kun, Guangbo Qu, Cuihong Zhang, Huaibiao Li, and Liang Sun. 2022. "Effect of Influenza Vaccine on Prevention of Acute Attack of Chronic Airway Disease in Elderly Population" Vaccines 10, no. 10: 1750. https://doi.org/10.3390/vaccines10101750
APA StyleGao, K., Qu, G., Zhang, C., Li, H., & Sun, L. (2022). Effect of Influenza Vaccine on Prevention of Acute Attack of Chronic Airway Disease in Elderly Population. Vaccines, 10(10), 1750. https://doi.org/10.3390/vaccines10101750