
Reduced Prevalence of Measles Antibodies in a Cohort of Brazilian Children under 15 Years of Age


 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knipe, D.; Howley, P. Fields Virology, 6th ed.; Lippincott Williams & Wilkins, A Wolters Kluwer Business: Philadelphia, PA, USA, 2013. [Google Scholar]
- ICTV. Taxon Details. Species: Measles Morbillivirus. 2022. Available online: https://ictv.global/taxonomy/taxondetails?taxnode_id=20181616 (accessed on 22 August 2022).
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R0) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Moten, M.; Phillips, A.; Saliba, V.; Harding, N.; Sibal, B. Measles: Is it still a threat? Br. J. Gen. Pract. 2018, 68, 404–405. [Google Scholar] [CrossRef] [PubMed]
- Domingues, C.M.; Teixeira, A.M.; Carvalho, S.M. National immunization program: Vaccination, compliance and pharmacovigilance. Rev. Inst. Med. Trop. São Paulo 2012, 54 (Suppl. 18), 22–27. [Google Scholar] [CrossRef] [PubMed]
- Strebel, P.M.; Orenstein, W.A. Measles. N. Engl. J. Med. 2019, 381, 349–357. [Google Scholar] [CrossRef]
- Brasil DATASUS. Imunizações. Cobertura. Brasil. Sarampo. Brasilia: Sistema de Informação do Programa Nacional de Imunizações. 2022. Available online: http://tabnet.datasus.gov.br/cgi/dhdat.exe?bd_pni/cpnibr.def (accessed on 22 August 2022).
- Elidio, G.A.; De França, G.V.A.; Pacheco, F.C.; Ferreira, M.M.; Pinheiro, J.D.S.; Campos, E.N.; De Albuquerque, B.C.; Pinto, R.C.; Da Silva, A.D.C.S.; Leite, P.L.; et al. Measles outbreak: Preliminary report on a case series of the first 8070 suspected cases, Manaus, Amazonas state, Brazil, February to November 2018. Eurosurveillance 2019, 24, 1800663. [Google Scholar] [CrossRef]
- PAHO. PAHO Health Information Platform—Immunization. Number of Vaccine Preventable Disease (VDD) Cases in the Americas: PAHO; Washington, D.C. 2022. Available online: http://ais.paho.org/phip/viz/im_vaccinepreventablediseases.asp (accessed on 22 August 2022).
- PAHO. Plan of Action for Maintaining Measles, Rubella, and Congenital Rubella Syndrome Elimination in the Region of the Americas; Final Report; 55th Directing Council 68th Session of the Region Committee of WHO for the Americas; Pan American Health Organization: Washington, DC, USA, 2016. [Google Scholar]
- Ministério da Saúde. Vigilância epidemiológica do sarampo no Brasil—Semanas epidemiológicas 1 a 52 de 2021. Brasília Ministério Saúde Secr. Vigilância Saúde 2022, 53, 14. [Google Scholar]
- SBMT. Measles: Increase in the Number of Cases Worries and Lights up Alert for the Whole Brazil: Sociedade Brasileira de Medicina Tropical. 2022. Available online: https://www.sbmt.org.br/portal/sarampo-aumento-no-numero-de-casos-preocupa-e-acende-alerta-para-todo-pais/?locale=en-US〈=en (accessed on 22 August 2022).
- Ministério da Saúde. Vigilância epidemiológica do sarampo no Brasil—Semanas epidemiológicas 1 a 25 de 2022. Brasília Ministério Saúde Secr. Vigilância Saúde 2022, 53, 10. [Google Scholar]
- Estofolete, C.F.; Milhim, B.H.G.D.A.; França, C.C.G.D.; Silva, G.C.D.D.; Augusto, M.T.; Terzian, A.C.B.; Zini, N.; Durigon, E.L.; Oliveira, D.B.L.; Massad, E.; et al. Prevalence of Measles Antibodies in São José do Rio Preto, São Paulo, Brazil: A serological survey model. Sci. Rep. 2020, 10, 5179. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Vigilância epidemiológica do sarampo no Brasil—Semanas epidemiológicas 1 a 48 de 2021. Brasília Ministério Saúde Secr. Vigilância Saúde 2021, 52, 34. [Google Scholar]
- Keegan, R.; Dabbagh, A.; Strebel, P.M.; Cochi, S.L. Comparing Measles With Previous Eradication Programs: Enabling and Constraining Factors. J. Infect. Dis. 2011, 204 (Suppl. 1), S54–S61. [Google Scholar] [CrossRef] [PubMed]
- Strebel, P.; Papania, M.; Fiebelkorn, A.; Halsey, N. Measles Vaccine, 6th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2013; pp. 352–387. [Google Scholar]
- Panum, P.L.; Doull, J.A.; Petersen, J.J.; Association APH. Observations Made during the Epidemic of Measles on the Faroe Islands in the Year 1846; Delta Omega Society: Washington, DC, USA, 2003; pp. 1–48. [Google Scholar]
- Dixon, M.G.; Tapia, M.D.; Wannemuehler, K.; Luce, R.; Papania, M.; Sow, S.; Levine, M.M.; Pasetti, M.F. Measles susceptibility in maternal-infant dyads—Bamako, Mali. Vaccine 2022, 40, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- PAHO. Plan of Action for Maintaining Measles, Rubella, and Congenital Rubella Syndrome Elimination in the Region of the Americas. In Proceedings of the 28th Pan American Sanitary Conference 64th Session of the Regional Committee, Washington, DC, USA, 17–21 September 2012. [Google Scholar]
- WHO. Epidemiological Update. Measles. 6 February 2018; PAHO: Washington, DC, USA, 2018. [Google Scholar]
- WHO. Epidemiological Update. Measles. 18 January 2019; PAHO: Washington, DC, USA, 2019. [Google Scholar]
- Gupta, M.; Tripathy, J.P.; Verma, M.; Singh, M.P.; Kaur, R.; Ratho, R.; Kumar, R. Seroprevalence of measles, mumps & rubella antibodies among 5-10 years old children in north India. Indian J. Med. Res. 2019, 149, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Alemán, M.; Gutiérrez-Pérez, I.; Díaz-Salgado, N.; Zaragoza-García, O.; Olamendi-Portugal, M.; Castro-Alarcón, N.; Parra-Rojas, I.; Guzmán-Guzmán, I. Low Seroprevalence of Measles-Specific IgG in Children of Three Ethnic Groups from Mexico: Influence of Age, Sex, Malnutrition and Family Size. Vaccines 2021, 9, 295. [Google Scholar] [CrossRef] [PubMed]
- WHO. Measles Vaccination Coverage: WHO. 2022. Available online: https://immunizationdata.who.int/pages/coverage/mcv.html?CODE=Global+amr&ANTIGEN=MCV2&YEAR= (accessed on 22 August 2022).
- Díaz-Ortega, J.L.; Ferreira-Guerrero, E.; Cruz-Hervert, L.P.; Delgado-Sánchez, G.; Ferreyra-Reyes, L.; Yanes-Lane, M.; Mongua-Rodríguez, N.; Montero-Campos, R.; Castañeda-Desales, D.; García-García, L. Seroprevalence of measles antibodies and factors associated with susceptibility: A national survey in Mexico using a plaque reduction neutralization test. Sci. Rep. 2020, 10, 17488. [Google Scholar] [CrossRef] [PubMed]
- Makarenko, C.; San Pedro, A.; Paiva, N.S.; Santos, J.P.C.D.; Medronho, R.A.; Gibson, G. Measles Resurgence in Brazil: Analysis of the 2019 epidemic in the state of São Paulo. Rev. Saude Publica 2022, 56, 50. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, F.C.; França, G.V.; Elidio, G.A.; Leal, M.B.; de Oliveira, C.; Guilhem, D.B. Measles-containing vaccines in Brazil: Coverage, homogeneity of coverage and associations with contextual factors at municipal level. Vaccine 2020, 38, 1881–1887. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Global | IgG Negative | IgG Positive | ||||||
|---|---|---|---|---|---|---|---|---|
| N Total | N Positive | % | N positive | % | N Positive | % | p-Value | |
| Gender | ||||||||
| Female | 252 | 119 | 47.2% | 24 | 20.2% | 95 | 79.8% | 0.157 |
| Male | 252 | 133 | 52.8% | 37 | 27.8% | 96 | 72.2% | |
| Age Group | ||||||||
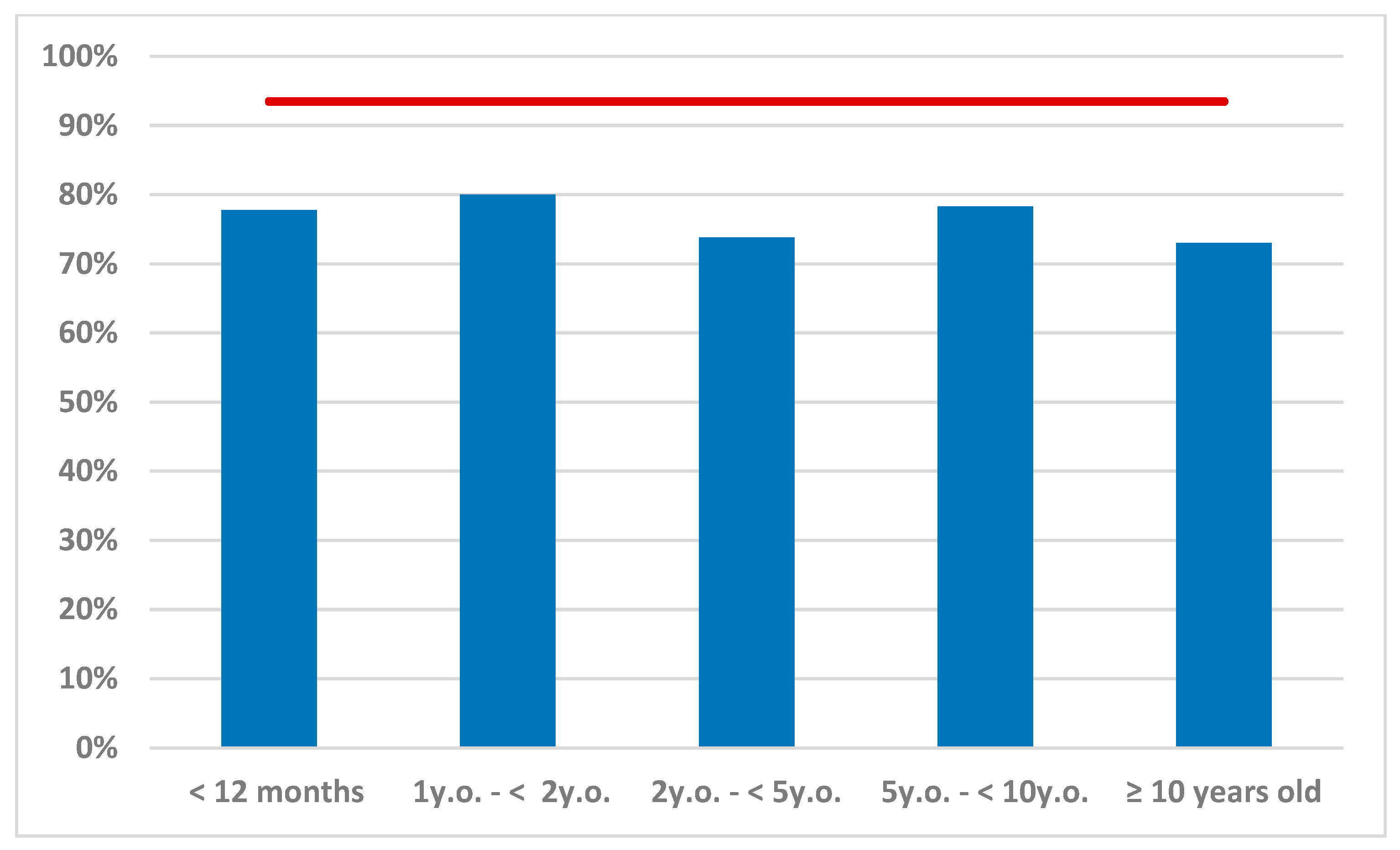
| <12 months | 252 | 18 | 7.1% | 4 | 22.2% | 14 | 77.8% | 0.913 |
| 1 y.o.–<2 y.o. | 252 | 20 | 7.9% | 4 | 20.0% | 16 | 80.0% | |
| 2 y.o.–<5 y.o. | 252 | 42 | 16.7% | 11 | 26.2% | 31 | 73.8% | |
| 5 y.o.–<10 y.o. | 252 | 83 | 32.9% | 18 | 21.7% | 65 | 78.3% | |
| ≥10 years old | 252 | 89 | 35.3% | 24 | 27.0% | 65 | 73.0% | |
| Ethnicity | ||||||||
| Caucasian | 246 | 231 | 93.9% | 55 | 23.8% | 176 | 76.2% | 0.736 |
| African-Brazilian | 246 | 15 | 6.1% | 3 | 20.0% | 12 | 80.0% | |
| Comorbidities 1 | ||||||||
| No | 252 | 216 | 85.7% | 51 | 23.6% | 165 | 76.4% | 0.589 |
| Yes | 252 | 36 | 14.3% | 10 | 27.8% | 26 | 72.2% | |
| Immunosuppression | ||||||||
| No | 252 | 241 | 95.6% | 58 | 24.1% | 183 | 75.9% | 0.808 |
| Yes | 252 | 11 | 4.4% | 3 | 27.3% | 8 | 72.7% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estofolete, C.F.; de Andrade Gandolfi, F.; de Aguiar Milhim, B.H.; da Silva, G.C.D.; Dourado, F.S.; dos Santos, B.F.; Vasilakis, N.; Nogueira, M.L. Reduced Prevalence of Measles Antibodies in a Cohort of Brazilian Children under 15 Years of Age. Vaccines 2022, 10, 1570. https://doi.org/10.3390/vaccines10101570
Estofolete CF, de Andrade Gandolfi F, de Aguiar Milhim BH, da Silva GCD, Dourado FS, dos Santos BF, Vasilakis N, Nogueira ML. Reduced Prevalence of Measles Antibodies in a Cohort of Brazilian Children under 15 Years of Age. Vaccines. 2022; 10(10):1570. https://doi.org/10.3390/vaccines10101570
Chicago/Turabian StyleEstofolete, Cassia Fernanda, Flora de Andrade Gandolfi, Bruno Henrique de Aguiar Milhim, Gislaine Celestino Dutra da Silva, Fernanda Simões Dourado, Bárbara Ferreira dos Santos, Nikos Vasilakis, and Maurício Lacerda Nogueira. 2022. "Reduced Prevalence of Measles Antibodies in a Cohort of Brazilian Children under 15 Years of Age" Vaccines 10, no. 10: 1570. https://doi.org/10.3390/vaccines10101570
APA StyleEstofolete, C. F., de Andrade Gandolfi, F., de Aguiar Milhim, B. H., da Silva, G. C. D., Dourado, F. S., dos Santos, B. F., Vasilakis, N., & Nogueira, M. L. (2022). Reduced Prevalence of Measles Antibodies in a Cohort of Brazilian Children under 15 Years of Age. Vaccines, 10(10), 1570. https://doi.org/10.3390/vaccines10101570