Nigella Sativa’s Anti-Inflammatory and Antioxidative Effects in Experimental Inflammation

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Gas Chromatography Coupled with Mass Spectroscopy (GC-MS) Analysis of Nigella Sativa Iil
2.3. Animals
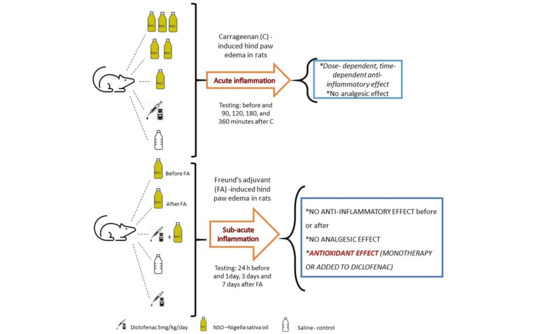
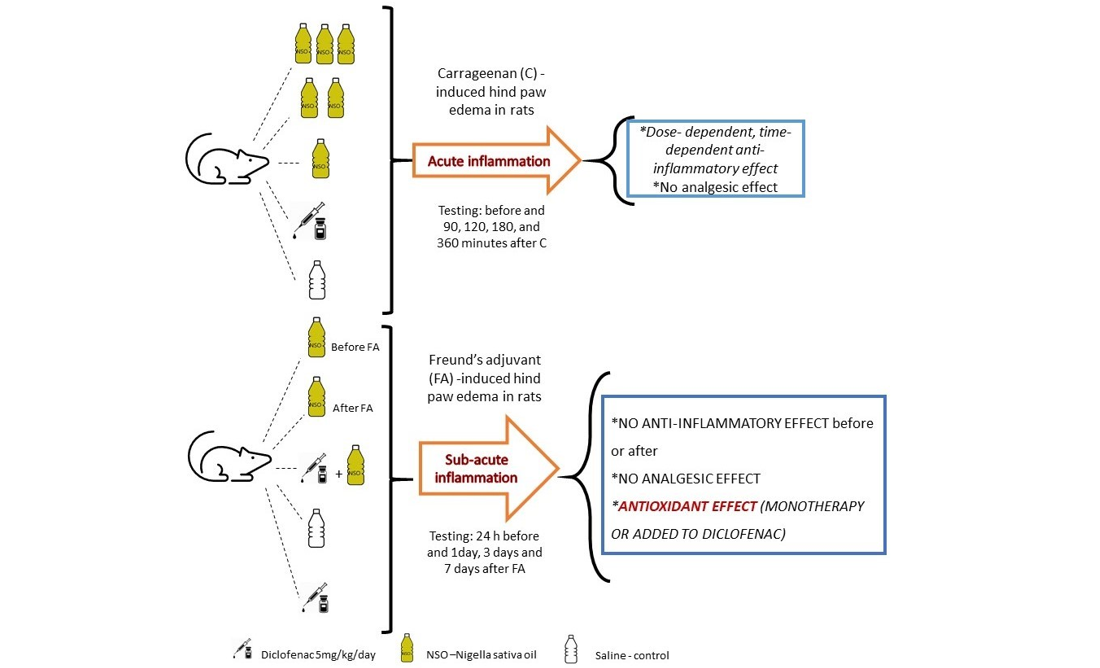
2.4. Carrageenan-Induced Hind Paw Edema in Rats
2.5. Inflammatory Edema Assessment
2.6. Mechanical Nociceptive Response Measurement
2.7. Time Point Measurements
2.8. Freund’s Adjuvant (FA)-Induced Hind Paw Edema in Rats
2.9. Inflammation and Nociceptive Response Measurements
2.10. Time Point Measurements
2.11. Oxidative Stress Analysis
2.12. Statistical Analysis
3. Results
3.1. GS-MS Analysis of Nigella Sativa Oil
3.2. Paw Edema in Acute Inflammation
3.3. Antinociceptive Effect of NSO on Acute Inflammation
3.4. Paw Edema in Sub-Acute Inflammation
3.5. Antinociceptive Effect of NSO on Sub-Acute Inflammation—Mechanical Hyperalgesia Evaluation
3.6. Antinociceptive Effect of NSO on Sub-Acute Inflammation—Thermal Hyperalgesia Evaluation
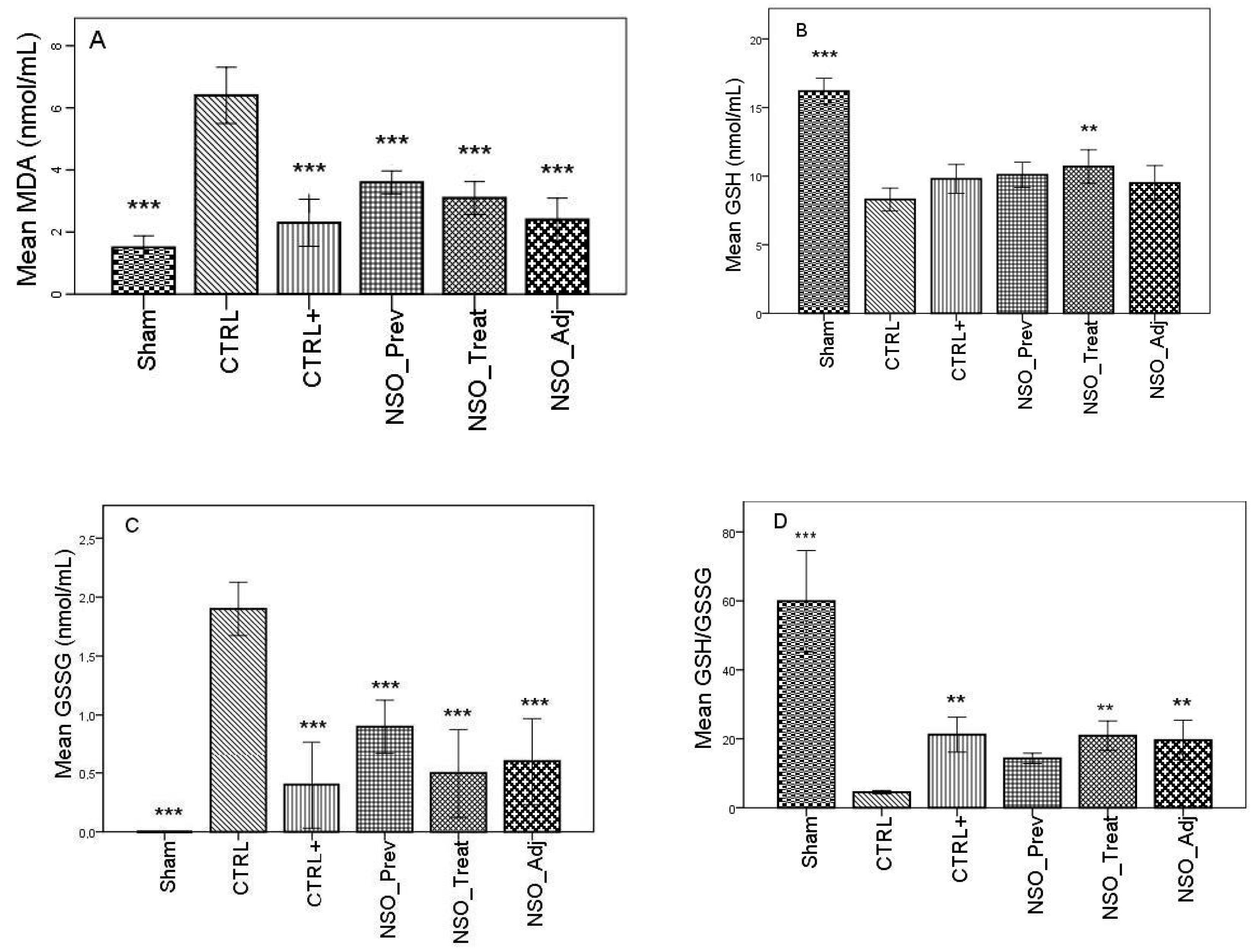
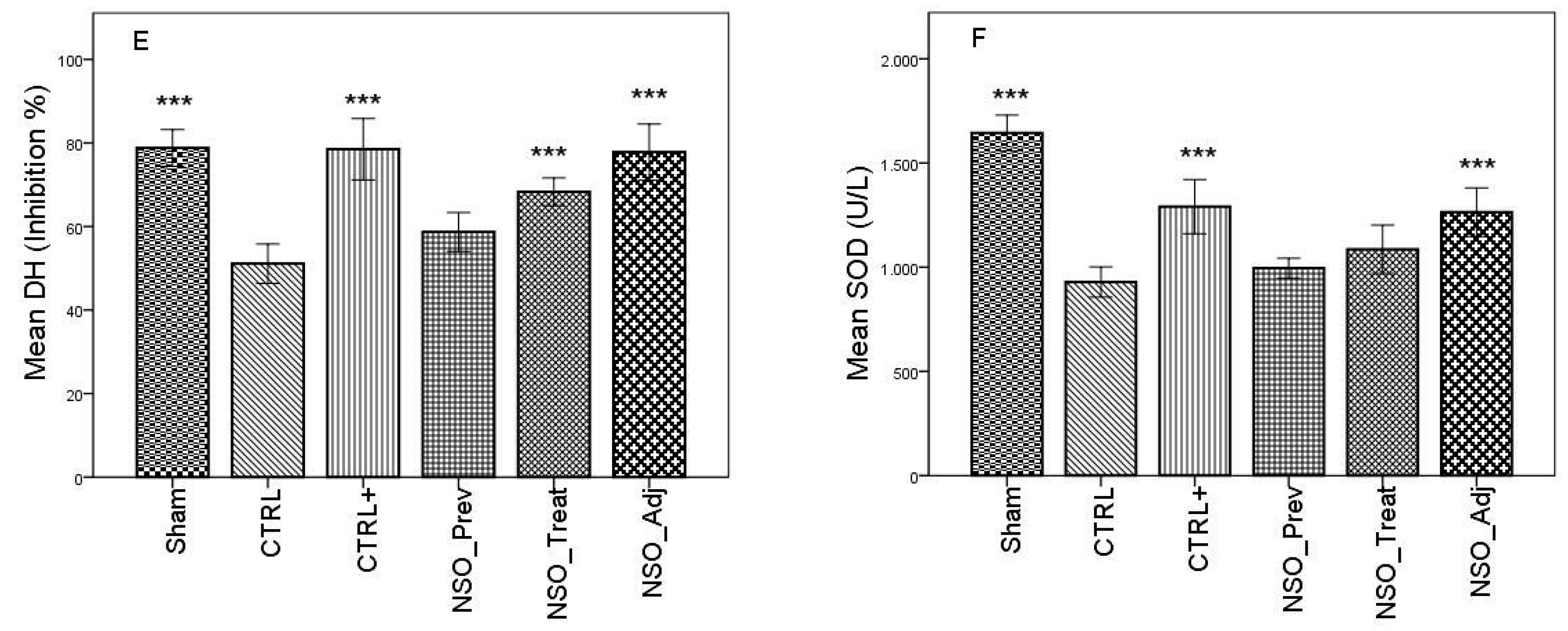
3.7. Effect of NSO on Oxidative Stress in Sub-Acute Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pise, H.N.; Padwal, S.L. Evaluation of anti-inflammatory activity of Nigella sativa: An experimental study. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7, 1. [Google Scholar] [CrossRef]
- Hunter, P. The inflammation theory of disease. The growing realization that chronic inflammation is crucial in many diseases opens new avenues for treatment. EMBO Rep. 2012, 13, 968–970. [Google Scholar] [CrossRef] [PubMed]
- Hossen, M.J.; Yang, W.S.; Kim, D.; Aravinthan, A.; Kim, J.-H.; Cho, J.Y. Thymoquinone: An IRAK1 inhibitor with in vivo and in vitro anti-inflammatory activities. Sci. Rep. 2017, 7, 42995. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Park, S. Role of vascular smooth muscle cell in the inflammation of atherosclerosis. BMB Rep. 2014, 47, 1–7. [Google Scholar] [CrossRef]
- Shin, K.; Lee, S.-H. Interplay between inflammatory responses and lymphatic vessels. Immune Netw. 2014, 14, 182–186. [Google Scholar] [CrossRef]
- Vishal, V.; Ganesh, S.; Mukesh, G.; Ranjan, B. A review on some plants having anti-inflammatory activity. J. Phytopharm. 2014, 3, 214–221. [Google Scholar]
- Salzano, S.; Checconi, P.; Hanschmann, E.-M.; Lillig, C.H.; Bowler, L.D.; Chan, P.; Vaudry, D.; Mengozzi, M.; Coppo, L.; Sacre, S.; et al. Linkage of inflammation and oxidative stress via release of glutathionylated peroxiredoxin-2, which acts as a danger signal. Proc. Natl. Acad. Sci. USA 2014, 111, 12157–12162. [Google Scholar] [CrossRef]
- Biswas, S.K. Does the interdependence between oxidative stress and inflammation explain the antioxidant paradox? Oxidative Med. Cell. Longev. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Kooti, W.; Hasanzadeh-Noohi, Z.; Sharafi-Ahvazi, N.; Asadi-Samani, M.; Ashtary-Larky, D. Phytochemistry, pharmacology, and therapeutic uses of black seed (Nigella sativa). Chin. J. Nat. Med. 2016, 14, 732–745. [Google Scholar] [CrossRef]
- Tiruppur Venkatachallam, S.K.; Pattekhan, H.; Divakar, S.; Kadimi, U.S. Chemical composition of Nigella sativa L. seed extracts obtained by supercritical carbon dioxide. J. Food Sci. Technol. 2010, 47, 598–605. [Google Scholar] [CrossRef]
- Gharby, S.; Harhar, H.; Guillaume, D.; Roudani, A.; Boulbaroud, S.; Ibrahimi, M.; Ahmad, M.; Sultana, S.; Ben Hadda, T.; Chafchaouni-Moussaoui, I.; et al. Chemical investigation of Nigella sativa L. seed oil produced in Morocco. J. Saudi Soc. Agric. Sci. 2015, 14, 172–177. [Google Scholar] [CrossRef]
- Bourgou, S.; Ksouri, R.; Bellila, A.; Skandrani, I.; Falleh, H.; Marzouk, B. Phenolic composition and biological activities of Tunisian Nigella sativa L. shoots and roots. Comptes Rendus Biol. 2008, 331, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Afzal, M. Chemical composition of Nigella sativa Linn: Part 2 Recent advances. Inflammopharmacology 2016, 24, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Gurumurthy, K.T.; Chandan, N.; Aamir, J.; Ashwini, L.S.; Khan, M.N.; Shaheen, S.; Baranwal, A. Synergistic antibacterial effect of essential oils of Nigella sativa and Salvadora persica on human pathogens. IJABR 2013, 3, 567–571. [Google Scholar]
- Altan, M.F.; Kanter, M.; Donmez, S.; Kartal, M.E.; Buyukbas, S. Combination therapy of Nigella sativa and human parathyroid hormone on bone mass, biomechanical behavior and structure in streptozotocin-induced diabetic rats. Acta Histochem. 2007, 109, 304–314. [Google Scholar] [CrossRef]
- Tavakkoli, A.; Mahdian, V.; Razavi, B.M.; Hosseinzadeh, H. Review on clinical trials of Black Seed (Nigella sativa) and its active constituent, Thymoquinone. J. Pharmacopunct. 2017, 20, 179–193. [Google Scholar] [CrossRef]
- Najmi, A.; Haque, S.; Naseeruddin, M.; Khan, R. Effect of Nigella Sativa oil on various clinical and biochemical parameters of metabolic syndrome. Int. J. Diabetes Metab. 2008, 16, 85–87. [Google Scholar]
- Asgary, S.; Sahebkar, A.; Goli-malekabadi, N. Ameliorative effects of Nigella sativa on dyslipidemia. J. Endocrinol. Investig. 2015, 38, 1039–1046. [Google Scholar] [CrossRef]
- Gali-Muhtasib, H.; El-Najjar, N.; Schneider-Stock, R. The medicinal potential of black seed (Nigella sativa) and its components. In Advances in Phytomedicine, Volume 2; Khan, M.T.H., Ather, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2006; pp. 133–153. [Google Scholar]
- Pop, R.M.; Trifa, A.P.; Popolo, A.; Chedea, V.S.; Militaru, C.; Bocsan, I.C.; Buzoianu, A.D. Nigella sativa: Valuable perspective in the management of chronic diseases. Iran. J. Basic Med. Sci. 2020, 23, 1–15. [Google Scholar]
- The Pherobase: Database of Pheromones and Semiochemicals. Available online: https://www.pherobase.com/ (accessed on September 2019).
- Flavornet: A Database of Aroma Compounds Based on Odor. Available online: https://www.flavornet.org (accessed on September 2019).
- Hasani, A.; Soljakova, M.; Jakupi, M.; Ustalar-Ozgen, S. Preemptive analgesic effects of midazolam and diclofenac in rat model. Bosn. J. Basic Med. Sci. 2011, 11, 113–118. [Google Scholar] [CrossRef]
- Szabo, A.; Bocsan, I.; Suciu, S.; Buzoianu, A. Comparative animal study of the antinociceptive efficacy of lamotrigine and gabapentin for the management of pain. Acta Physiol. Hung. 2015, 102, 363–371. [Google Scholar] [CrossRef]
- Conti, M.; Morand, P.C.; Levillain, P.; Lemonnier, A. Improved fluorometric determination of malonaldehyde. Clin. Chem. 1991, 37, 1273–1275. [Google Scholar] [CrossRef] [PubMed]
- Hu, M. Measurement of protein thiol groups and glutathione in plasma. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1994; pp. 380–384. [Google Scholar]
- Vats, P.; Singh, V.K.; Singh, S.N.; Singh, S.B. Glutathione metabolism under high-altitude stress and effect of antioxidant supplementation. Aviat. Space Environ. Med. 2008, 79, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Janaszewska, A.; Bartosz, G. Assay of total antioxidant capacity: Comparison of four methods as applied to human blood plasma. Scand. J. Clin. Lab. Investig. 2002, 62, 231–236. [Google Scholar] [CrossRef]
- Flohé, L.; Otting, F. Superoxide dismutase assays. Methods Enzymol. 1984, 105, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Ghahramanloo, K.H.; Kamalidehghan, B.; Javar, H.A.; Widodo, R.T.; Majidzadeh, K.; Noordin, M.I. Comparative analysis of essential oil composition of Iranian and Indian Nigella sativa L. extracted using supercritical fluid extraction and solvent extraction. Drug Des. Dev. Ther. 2017, 11, 2221–2226. [Google Scholar] [CrossRef]
- Kalidasu, G.; Reddy, G.S.; Kumari, S.S.; Kumari, A.L.; Sivasankar, A. Secondary volatiles and metabolites from Nigella sativa L. seed. Indian J. Nat. Prod. Resour. 2017, 8, 151–158. [Google Scholar]
- Patil, K.R.; Mahajan, U.B.; Unger, B.S.; Goyal, S.N.; Belemkar, S.; Surana, S.J.; Ojha, S.; Patil, C.R. Animal models of inflammation for screening of anti-inflammatory drugs: Implications for the discovery and development of phytopharmaceuticals. Int. J. Mol. Sci. 2019, 20, 4367. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdi, M.S. The anti-inflammatory, analgesic and antipyretic activity of Nigella sativa. J. Ethnopharmacol. 2001, 76, 45–48. [Google Scholar] [CrossRef]
- Nasuti, C.; Fedeli, D.; Bordoni, L.; Piangerelli, M.; Servili, M.; Selvaggini, R.; Gabbianelli, R. Anti-inflammatory, anti-arthritic and anti-nociceptive activities of Nigella sativa oil in a rat model of arthritis. Antioxidants 2019, 8, 342. [Google Scholar] [CrossRef]
- Kidd, B.L.; Urban, L.A. Mechanisms of inflammatory pain. Br. J. Anaesth. 2001, 87, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Deuis, J.R.; Dvorakova, L.S.; Vetter, I. Methods Used to Evaluate Pain Behaviors in Rodents. Front. Mol. Neurosci. 2017, 10, 284. [Google Scholar] [CrossRef] [PubMed]
- Ghannadi, A.; Hajhashemi, V.; Jafarabadi, H. An investigation of the analgesic and anti-inflammatory effects of Nigella sativa seed polyphenols. J. Med. Food 2005, 8, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Hajhashemi, V.; Ghannadi, A.; Jafarabadi, H. Black cumin seed essential oil, as a potent analgesic and antiinflammatory drug. Phyther. Res. 2004, 18, 195–199. [Google Scholar] [CrossRef]
- Abdelgalil, A.A.; El-Tahir, K.E.H.; Haseeb, A.M. Analgesic effect of melanin from (Nigella sativa L.) in the hotplate test in mice (possible opioid receptor involvement). Int. J. Pharmacol. 2016, 12, 567–571. [Google Scholar] [CrossRef]
- Houghton, P.; Zarka, R.; de las Heras, B.; Hoult, J. Fixed oil of Nigella sativa and derived Thymoquinone inhibit eicosanoid generation in leukocytes and membrane lipid peroxidation. Planta Med. 1995, 61, 33–36. [Google Scholar] [CrossRef]
- Hadi, V.; Kheirouri, S.; Alizadeh, M.; Khabbazi, A.; Hosseini, H. Effects of Nigella sativa oil extract on inflammatory cytokine response and oxidative stress status in patients with rheumatoid arthritis: A randomized, double-blind, placebo-controlled clinical trial. Avicenna J. Phytomed. 2016, 6, 34–43. [Google Scholar] [CrossRef]
- Tomin, T.; Schittmayer, M.; Birner-Gruenberger, R. Addressing Glutathione Redox Status in Clinical Samples by Two-Step Alkylation with N-ethylmaleimide Isotopologues. Metabolites 2020, 10, 71. [Google Scholar] [CrossRef]
- Sultan, M.T.; Butt, M.S.; Karim, R.; Ahmed, W.; Kaka, U.; Ahmad, S.; Dewanjee, S.; Jaafar, H.Z.; Zia-Ul-Haq, M. Nigella sativa fixed and essential oil modulates glutathione redox enzymes in potassium bromate induced oxidative stress. BMC Complement. Altern. Med. 2015, 15, 330. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Groups/Abbrev. | Administrated Substances/Dose | Route |
|---|---|---|
| Group I—control group (CTRL) | Normal saline solution | p.o. |
| Group II—positive control group (CTRL+) | Diclofenac sodium (5 mg/kg BW) | i.p. |
| Group III—(NSO_1) | NSO (1 mL/ kg BW) | p.o. |
| Group IV—(NSO_2) | NSO (2 mL/ kg BW) | p.o. |
| Group V—(NSO_4) | NSO (4 mL/ kg BW) | p.o. |
| Groups/Abbrev. | Administrated Substances/Dose/Time | Route |
|---|---|---|
| Group I—control group (CTRL) | Normal saline solution | p.o. |
| Group II—positive control group (CTRL+) | Diclofenac sodium (5 mg/kg BW) | i.p |
| Group III—(NSO_Prev) | NSO (4 mL/ kg BW)/ 7 days before FA | p.o. |
| Group IV—(NSO_Treat) | NSO (4 mL/ kg BW)/ 7 days after FA | p.o. |
| Group V—(NSO_Adj) | NSO (4 mL/ kg BW) + diclofenac sodium (5 mg/kg -BW) / 7 days after FA | p.o./ i.p |
| Compounds | RT (min) | Concentration (% from Total Peaks Area) |
|---|---|---|
| α-Thujene | 7.7 | 12.02 |
| α-Pinene | 7.948 | 2.49 |
| 4(10)-Thujene (Sabinene) | 9.325 | 1.02 |
| β-Pinene | 9.501 | 2.39 |
| (+)-4-Carene | 10.949 | 0.76 |
| p-Cymene | 11.236 | 39.72 |
| D-Limonene | 11.407 | 1.61 |
| Sabinene hydrate | 14.837 | 3.72 |
| 1-Terpinen-4-ol | 17.236 | 0.35 |
| Thymoquinone | 19.806 | 29.85 |
| Thymol | 21.562 | 2.35 |
| α-Longipinene | 23.46 | 0.66 |
| D-longifolene (Junipene) | 25.549 | 3.05 |
| Time Point | Paw Volume (ml) Mean ± SD and Inhibition Percentage (%) | ||||
|---|---|---|---|---|---|
| CTRL | CTRL+ | NSO_1 | NSO_2 | NSO_4 | |
| 0 min | 2.12 ± 0.31 | 2.47 ± 0.18 | 2.42 ± 0.27 | 2.59 ± 0.3 | 2.54 ± 0.18 |
| 90 min | 3.67 ± 0.26 | 2.65 ± 0.26 *** (27.35%) | 3.29 ± 0.31 * (9.95%) | 3.03 ± 0.35 *** (17.11%) | 2.90 ± 0.26 *** (20.78%) |
| 180 min | 4.04 ± 0.35 | 2.68 ± 0.41 *** (32.99%) | 3.46 ± 0.32 * (13.86%) | 3.43 ± 0.58 * (15.22%) | 3.36 ± 0.43 ** (16.27%) |
| 270 min | 4.12 ± 0.20 | 2.97 ± 0.38 *** (27.67%) | 3.83 ± 0.81 (7.26%) | 3.43 ± 0.46* (16.76%) | 3.42 ± 0.39 * (17.12%) |
| 360 min | 4.00 ± 0.28 | 3.36 ± 0.47 * (15.99%) | 3.64 ± 0.46 (8.44%) | 3.26 ± 0.39 ** (18.25%) | 3.05 ± 0.28 *** (23.41%) |
| Analgesy-Meter (g)/Time | CTRL | CTRL+ | NSO_1 | NSO_2 | NSO_4 |
|---|---|---|---|---|---|
| 0 min | 7.1 ± 1.47 | 8.1 ± 1.68 | 7.4 ± 3.4 | 6.1 ± 2.64 | 6.3 ± 2.00 |
| 90 min | 6.1 ± 1.35 | 10.2 ± 2.93 *** | 5.9 ± 0.99 | 5.9 ± 1.91 | 6.5 ± 2.22 |
| 180 min | 5.4 ± 1.50 | 8.6 ± 0.90 ** | 5.1 ± 2.07 | 3.8 ± 2.04 | 5.1 ± 2.46 |
| 270 min | 6.2 ± 1.51 | 8.1 ± 1.47 * | 5.3 ± 1.70 | 4.3 ± 2.05 * | 4.6 ± 0.96 |
| 360 min | 5.7 ± 1.39 | 8.5 ± 1.25 ** | 3.9 ± 1.85 | 3.3 ± 1.41 * | 4.4 ± 2.54 |
| Time (h) | Paw Volume (ml) Mean ± SD and Inhibition Percentage (%) | ||||
|---|---|---|---|---|---|
| CTRL | CTRL+ | NSO_Prev | NSO_Treat | NSO_Adj | |
| 0 h | 3.5 ± 0.30 | 3.9 ± 0.44 | 3.3 ± 0.64 | 3.5 ± 0.43 | 3.4 ± 0.54 |
| 24 h | 7.4 ± 1.07 | 6.1 ± 0.99 * (17.1%) | 6.3 ± 1.05 (16.7%) | 6.5 ± 1.08 (9.7%) | 6.6 ± 0.84 (10.8%) |
| 72 h | 6.3 ± 0.94 | 5.4 ± 0.84 (15.7%) | 6.5 ± 0.70 - | 7.4 ± 1.34 - | 5.1 ± 0.56 * (20.1%) |
| 168 h | 5.8 ± 1.03 | 4.7 ± 0.67 * (16.7%) | 5.3 ± 1.05 (3.7%) | 5.9 ± 1.19 - | 4.5 ± 0.52 * (19.2%) |
| Analgesy-Meter (g)/Time | CTRL | CTRL+ | NSO_Prev | NSO_Treat | NSO_Adj |
|---|---|---|---|---|---|
| 1 h | 6.9 ± 2.84 | 7.2 ± 2.69 | 4.7 ± 1.05 | 4.8 ± 0.78 | 5.50 ± 0.84 |
| 24 h | 4.4 ± 0.96 | 6.4 ± 1.57 | 5.7 ± 2.21 | 5.1 ± 2.33 | 8.3 ± 2.00 *** |
| 72 h | 6.6 ± 0.84 | 8.5 ± 1.58 | 5.6 ± 2.98 | 6.3 ± 2.00 | 10.0 ± 1.69 *** |
| 168 h | 4.8 ± 0.78 | 8.5 ± 1.43 *** | 7.4 ± 1.95 ** | 6.2 ± 1.98 *** | 10.6 ± 1.34 *** |
| Reaction Time Hot Plate (sec)/Time | CTRL | CTRL+ | NSO_Prev | NSO_Treat | NSO_Adj |
|---|---|---|---|---|---|
| 1 h | 4.4 ± 0.69 | 6.1 ± 1.66 | 8.8 ± 4.26 ** | 5.4 ± 0.84 | 7.3 ± 1.70 * |
| 24 h | 5.2 ± 1.54 | 8.3 ± 2.05 * | 7.9 ± 3.17 | 7.8 ± 2.04 | 7.6 ± 2.22 |
| 72 h | 6.0 ± 1.05 | 7.7 ± 1.94 | 6.4 ± 1.42 | 6.8 ± 1.47 | 8.3 ± 2.40 * |
| 168 h | 3.2 ± 1.13 | 8.1 ± 1.85 *** | 4.5 ± 0.97 | 4.4 ± 1.07 | 8.9 ± 2.60 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, R.M.; Sabin, O.; Suciu, Ș.; Vesa, S.C.; Socaci, S.A.; Chedea, V.S.; Bocsan, I.C.; Buzoianu, A.D. Nigella Sativa’s Anti-Inflammatory and Antioxidative Effects in Experimental Inflammation. Antioxidants 2020, 9, 921. https://doi.org/10.3390/antiox9100921
Pop RM, Sabin O, Suciu Ș, Vesa SC, Socaci SA, Chedea VS, Bocsan IC, Buzoianu AD. Nigella Sativa’s Anti-Inflammatory and Antioxidative Effects in Experimental Inflammation. Antioxidants. 2020; 9(10):921. https://doi.org/10.3390/antiox9100921
Chicago/Turabian StylePop, Raluca Maria, Octavia Sabin, Șoimița Suciu, Stefan Cristian Vesa, Sonia Ancuța Socaci, Veronica Sanda Chedea, Ioana Corina Bocsan, and Anca Dana Buzoianu. 2020. "Nigella Sativa’s Anti-Inflammatory and Antioxidative Effects in Experimental Inflammation" Antioxidants 9, no. 10: 921. https://doi.org/10.3390/antiox9100921
APA StylePop, R. M., Sabin, O., Suciu, Ș., Vesa, S. C., Socaci, S. A., Chedea, V. S., Bocsan, I. C., & Buzoianu, A. D. (2020). Nigella Sativa’s Anti-Inflammatory and Antioxidative Effects in Experimental Inflammation. Antioxidants, 9(10), 921. https://doi.org/10.3390/antiox9100921