

Systemic Oxidative Stress in Subacute Stroke Patients Undergoing Rehabilitation Treatment

 , ,
, ,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Biochemical Analyses
2.2.1. Oxidative Stress Analysis
2.2.2. Hematochemical Analysis
2.3. Rehabilitation Treatment
2.4. Activity of Daily Living, Endurance and Strength Assessment
2.5. Statistical Analysis
3. Results
3.1. Participants and Baseline Characteristics
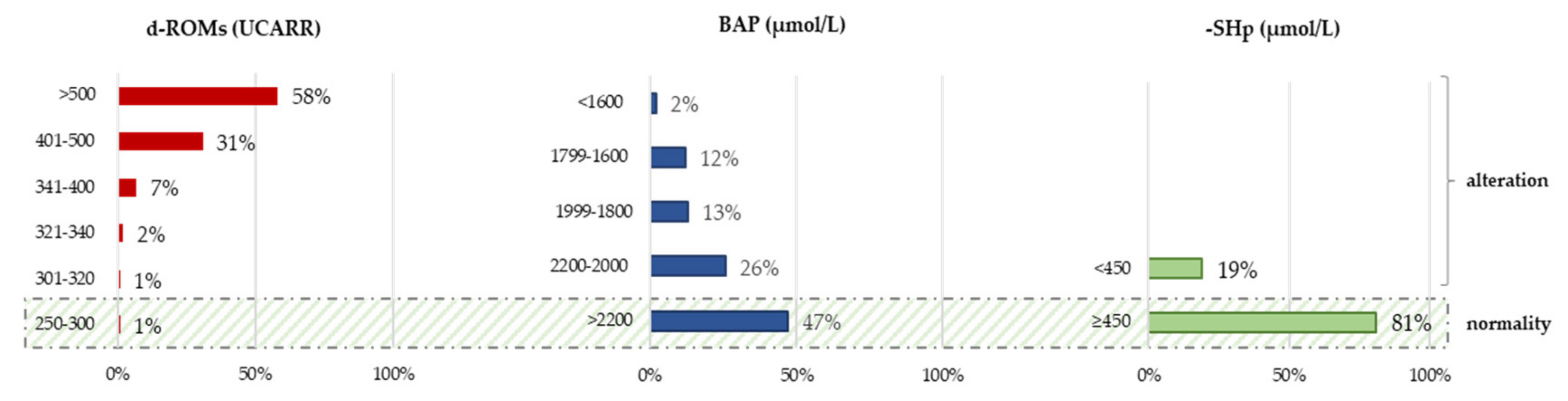
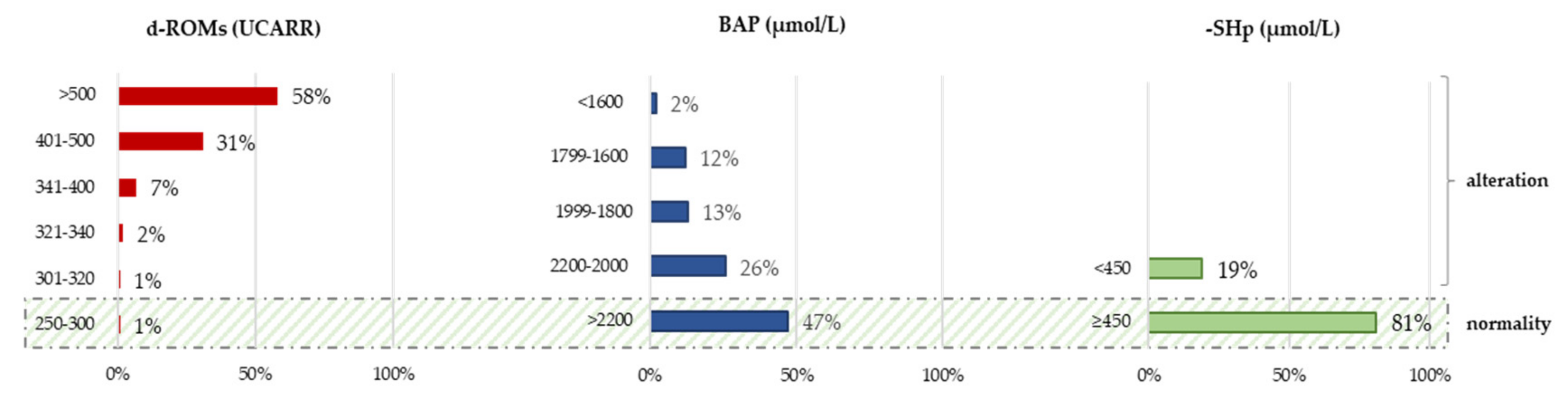
3.2. Oxidative Stress Parameters at Baseline
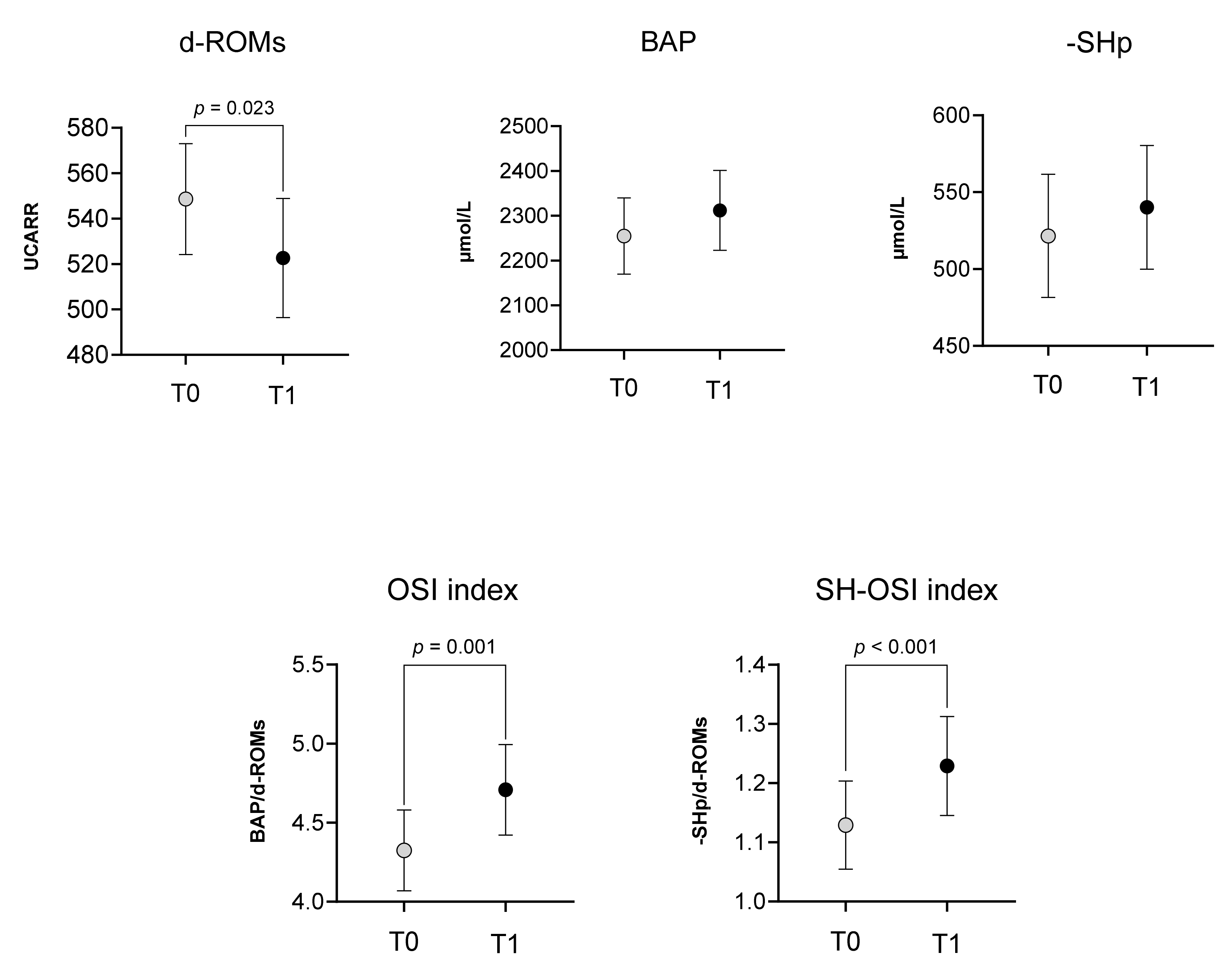
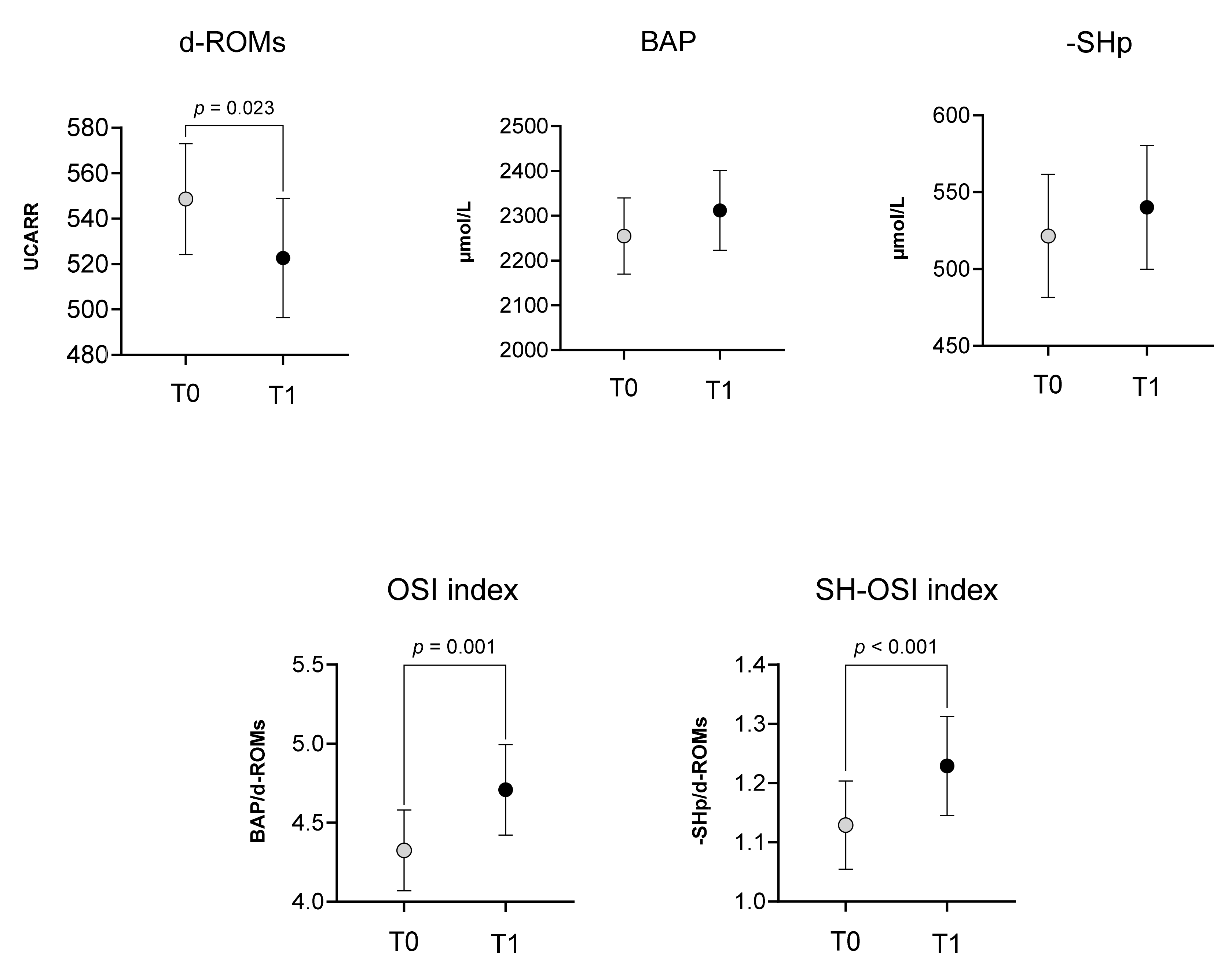
3.3. Rehabilitation Effect
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, J.; Thayabaranathan, T.; Donnan, G.A.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.; Norrving, B.; Owolabi, M.; Pandian, J.; et al. Global Stroke Statistics 2019. Int. J. Stroke 2020, 15, 819–838. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Executive Summary: Heart Disease and Stroke Statistics—2014 Update: A Report from the American Heart Association. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef]
- GBD 2019 Stroke Collaborators Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [CrossRef]
- Prabhakaran, S.; Zarahn, E.; Riley, C.; Speizer, A.; Chong, J.Y.; Lazar, R.M.; Marshall, R.S.; Krakauer, J.W. Inter-Individual Variability in the Capacity for Motor Recovery after Ischemic Stroke. J. Neurol. Rehabil. 2008, 22, 64–71. [Google Scholar] [CrossRef]
- Alexandrova, M.L.; Bochev, P.G. Oxidative Stress during the Chronic Phase after Stroke. Free Radic. Biol. Med. 2005, 39, 297–316. [Google Scholar] [CrossRef]
- Polidori, M.C.; Frei, B.; Cherubini, A.; Nelles, G.; Rordorf, G.; Keaney, J.F.; Schwamm, L.; Mecocci, P.; Koroshetz, W.J.; Beal, M.F. Increased Plasma Levels of Lipid Hydroperoxides in Patients with Ischemic Stroke. Free Radic. Biol. Med. 1998, 25, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Patel, M. Targeting Oxidative Stress in Central Nervous System Disorders. Trends Pharmacol. Sci. 2016, 37, 768–778. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef] [PubMed]
- Lakhan, S.E.; Kirchgessner, A.; Hofer, M. Inflammatory Mechanisms in Ischemic Stroke: Therapeutic Approaches. J. Transl. Med. 2009, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative Stress and Antioxidant Defense. World Allergy Organ. J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.L.; Bayraktutan, U. Oxidative Stress and Its Role in the Pathogenesis of Ischaemic Stroke. Int. J. Stroke 2009, 4, 461–470. [Google Scholar] [CrossRef]
- Shirley, R.; Ord, E.N.J.; Work, L.M. Oxidative Stress and the Use of Antioxidants in Stroke. Antioxidants 2014, 3, 472–501. [Google Scholar] [CrossRef] [PubMed]
- Jelinek, M.; Jurajda, M.; Duris, K. Oxidative Stress in the Brain: Basic Concepts and Treatment Strategies in Stroke. Antioxidants 2021, 10, 1886. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.A.; Shad, K.F.; Saleem, T.; Javed, F.; Khan, M.U. Some New Prospects in the Understanding of the Molecular Basis of the Pathogenesis of Stroke. Exp. Brain Res. 2007, 182, 1–10. [Google Scholar] [CrossRef]
- Ciancarelli, I.; Morone, G.; Iosa, M.; Cerasa, A.; Calabrò, R.S.; Iolascon, G.; Gimigliano, F.; Tonin, P.; Tozzi Ciancarelli, M.G. Influence of Oxidative Stress and Inflammation on Nutritional Status and Neural Plasticity: New Perspectives on Post-Stroke Neurorehabilitative Outcome. Nutrients 2023, 15, 108. [Google Scholar] [CrossRef] [PubMed]
- Salim, S. Oxidative Stress and the Central Nervous System. J. Pharmacol. Exp. Ther. 2017, 360, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, W.; Sun, X.; Li, R.; Sun, Q.; Cai, J.; Kang, Z.; Lv, S.; Zhang, J.H.; Zhang, W. Hydrogen Saline Offers Neuroprotection by Reducing Oxidative Stress in a Focal Cerebral Ischemia-Reperfusion Rat Model. Med. Gas Res. 2011, 1, 15. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-Y.; Si, Y.-L.; Liao, J.; Yan, G.-T.; Deng, Z.-H.; Xue, H.; Wang, L.-H.; Zhang, K. Leptin Administration Alleviates Ischemic Brain Injury in Mice by Reducing Oxidative Stress and Subsequent Neuronal Apoptosis. J. Trauma. Acute Care Surg. 2012, 72, 982–991. [Google Scholar] [CrossRef]
- Awooda, H.A.; Lutfi, M.F.; Sharara, G.G.M.; Saeed, A.M. Oxidative/Nitrosative Stress in Rats Subjected to Focal Cerebral Ischemia/Reperfusion. Int. J. Health Sci. 2015, 9, 17–24. [Google Scholar] [CrossRef]
- Dogan, O.; Kisa, U.; Erdemoglu, A.K.; Kacmaz, M.; Caglayan, O.; Kurku, H. Oxidative and Nitrosative Stress in Patients with Ischemic Stroke. J. Lab. Med. 2018, 42, 195–200. [Google Scholar] [CrossRef]
- Menon, B.; Ramalingam, K.; Kumar, R. Evaluating the Role of Oxidative Stress in Acute Ischemic Stroke. J. Neurosci. Rural Pract. 2020, 11, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Shaafi, S.; Hadisi, F.; Mahmoudinezhad, M.; Razmi, H.; Nejadghaderi, S.A.; Khalili, M. The Significance of the Oxidative Stress Markers in the One-Year Prognosis of Patients with Acute Ischemic Stroke: A Case-Control Study. BMC Neurol. 2021, 21, 258. [Google Scholar] [CrossRef] [PubMed]
- Squitti, R.; Siotto, M.; Assenza, G.; Giannantoni, N.M.; Rongioletti, M.; Zappasodi, F.; Tecchio, F. Prognostic Value of Serum Copper for Post-Stroke Clinical Recovery: A Pilot Study. Front. Neurol. 2018, 9, 366531. [Google Scholar] [CrossRef] [PubMed]
- Siotto, M.; Germanotta, M.; Santoro, M.; Canali, R.; Pascali, S.; Insalaco, S.; Cipollini, V.; Papadopoulou, D.; Antonacci, E.; Aprile, I. Oxidative Stress Status in Post Stroke Patients: Sex Differences. Healthcare 2022, 10, 869. [Google Scholar] [CrossRef] [PubMed]
- Žitňanová, I.; Šiarnik, P.; Kollár, B.; Chomová, M.; Pazderová, P.; Andrezálová, L.; Ježovičová, M.; Koňariková, K.; Laubertová, L.; Krivošíková, Z.; et al. Oxidative Stress Markers and Their Dynamic Changes in Patients after Acute Ischemic Stroke. Oxidative Med. Cell. Longev. 2016, 2016, e9761697. [Google Scholar] [CrossRef] [PubMed]
- Kihoin, N.; Tanaka, K.; Okuno, M.; Okamoto, T.; Saura, R. Exercise Attenuates Oxidative Stress in Patients with Stroke. Neurol. Asia 2016, 21, 7. [Google Scholar]
- Alexandrova, M.L.; Bochev, P.G.; Markova, V.I.; Bechev, B.G.; Popova, M.A.; Danovska, M.P.; Simeonova, V.K. Oxidative Stress in the Chronic Phase after Stroke. Redox Rep. 2003, 8, 169–176. [Google Scholar] [CrossRef]
- Serra, M.C.; Hafer-Macko, C.E.; Robbins, R.; O’Connor, J.C.; Ryan, A.S. Randomization to Treadmill Training Improves Physical and Metabolic Health in Association With Declines in Oxidative Stress in Stroke. Arch. Phys. Med. Rehabil. 2022, 103, 2077–2084. [Google Scholar] [CrossRef]
- Lee, K.H.; Cha, M.; Lee, B.H. Neuroprotective Effect of Antioxidants in the Brain. Int. J. Mol. Sci. 2020, 21, 7152. [Google Scholar] [CrossRef]
- Cherubini, A.; Polidori, M.C.; Bregnocchi, M.; Pezzuto, S.; Cecchetti, R.; Ingegni, T.; di Iorio, A.; Senin, U.; Mecocci, P. Antioxidant Profile and Early Outcome in Stroke Patients. Stroke 2000, 31, 2295–2300. [Google Scholar] [CrossRef]
- Baba, S.P.; Bhatnagar, A. Role of Thiols in Oxidative Stress. Curr. Opin. Toxicol. 2018, 7, 133–139. [Google Scholar] [CrossRef]
- Ulrich, K.; Jakob, U. The Role of Thiols in Antioxidant Systems. Free Radic. Biol. Med. 2019, 140, 14–27. [Google Scholar] [CrossRef]
- Bektas, H.; Vural, G.; Gumusyayla, S.; Deniz, O.; Alisik, M.; Erel, O. Dynamic Thiol–Disulfide Homeostasis in Acute Ischemic Stroke Patients. Acta Neurol. Belg. 2016, 116, 489–494. [Google Scholar] [CrossRef]
- Musumeci, M.; Sotgiu, S.; Persichilli, S.; Arru, G.; Angeletti, S.; Fois, M.L.; Minucci, A.; Musumeci, S. Role of SH Levels and Markers of Immune Response in the Stroke. Dis. Markers 2013, 35, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Ciancarelli, I.; De Amicis, D.; Di Massimo, C.; Carolei, A.; Ciancarelli, M.G.T. Oxidative Stress in Post-Acute Ischemic Stroke Patients after Intensive Neurorehabilitation. Curr. Neurovasc. Res. 2012, 9, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Manolescu, B.N.; Berteanu, M.; Oprea, E.; Chiriac, N.; Dumitru, L.; Vladoiu, S.; Popa, O.; Ianas, O. Dynamic of Oxidative and Nitrosative Stress Markers during the Convalescent Period of Stroke Patients Undergoing Rehabilitation. Ann. Clin. Biochem. 2011, 48, 338–343. [Google Scholar] [CrossRef]
- Yeh, T.-T.; Hsieh, Y.-W.; Wu, C.-Y.; Wang, J.-S.; Lin, K.-C.; Chen, C.-L. A Preliminary Investigation of the Association of Sleep With Inflammation and Oxidative Stress Biomarkers and Functional Outcomes After Stroke Rehabilitation. Sci. Rep. 2017, 7, 8634. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.W.; Lin, K.C.; Korivi, M.; Lee, T.H.; Wu, C.Y.; Wu, K.Y. The Reliability and Predictive Ability of a Biomarker of Oxidative DNA Damage on Functional Outcomes after Stroke Rehabilitation. Int. J. Mol. Sci. 2014, 15, 6504–6516. [Google Scholar] [CrossRef] [PubMed]
- Hudon, C.; Fortin, M.; Vanasse, A. Cumulative Illness Rating Scale Was a Reliable and Valid Index in a Family Practice Context. J. Clin. Epidemiol. 2005, 58, 603–608. [Google Scholar] [CrossRef]
- Cesarone, M.R.; Belcaro, G.; Carratelli, M.; Cornelli, U.; De Sanctis, M.T.; Incandela, L.; Barsotti, A.; Terranova, R.; Nicolaides, A. A Simple Test to Monitor Oxidative Stress. Int. Angiol. 1999, 18, 127–130. [Google Scholar]
- Ellman, G.L. Tissue Sulfhydryl Groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Westgard, J.O.; Poquette, M.A. Determination of Serum Albumin with the “SMA 12-60” by a Bromcresol Green Dye-Binding Method. Clin. Chem. 1972, 18, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Trinder, P. Oxidase Determination of Plasma Cholesterol as Cholest-4-En-3-One Using Iso-Octane Extraction. Ann. Clin. Biochem. 1981, 18, 64–70. [Google Scholar] [CrossRef]
- Izawa, S.; Okada, M.; Matsui, H.; Horita, Y. A New Direct Method for Measuring HDL-Cholesterol Which Does Not Produce Any Biased Values. J. Med. Pharm. Sci. 1997, 37, 1385–1388. [Google Scholar]
- McGowan, M.W.; Artiss, J.D.; Strandbergh, D.R.; Zak, B. A Peroxidase-Coupled Method for the Colorimetric Determination of Serum Triglycerides. Clin. Chem. 1983, 29, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Cruciani, A.; Germanotta, M.; Gower, V.; Pecchioli, C.; Cattaneo, D.; Vannetti, F.; Padua, L.; Gramatica, F. Upper Limb Robotics in Rehabilitation: An Approach to Select the Devices, Based on Rehabilitation Aims, and Their Evaluation in a Feasibility Study. Appl. Sci. 2019, 9, 3920. [Google Scholar] [CrossRef]
- Aprile, I.; Germanotta, M.; Cruciani, A.; Loreti, S.; Pecchioli, C.; Cecchi, F.; Montesano, A.; Galeri, S.; Diverio, M.; Falsini, C.; et al. Upper Limb Robotic Rehabilitation After Stroke: A Multicenter, Randomized Clinical Trial. J. Neurol. Phys. Ther. 2020, 44, 3–14. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the Sensitivity of the Barthel Index for Stroke Rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Enright, P.L. The Six-Minute Walk Test. Respir. Care 2003, 48, 783–785. [Google Scholar]
- Ozkul, A.; Akyol, A.; Yenisey, C.; Arpaci, E.; Kiylioglu, N.; Tataroglu, C. Oxidative Stress in Acute Ischemic Stroke. J. Clin. Neurosci. 2007, 14, 1062–1066. [Google Scholar] [CrossRef]
- Kihoin, N.; Tanaka, K.; Okuno, M.; Okamoto, T.; Saura, R. L’esercizio Fisico Attenua lo Stress Ossidativo nei Pazienti con Ictus. |Neurologia Asia |EBSCOhost. Available online: https://openurl.ebsco.com/contentitem/gcd:114243350?sid=ebsco:plink:crawler&id=ebsco:gcd:114243350 (accessed on 2 February 2024).
- Lochhead, J.J.; McCaffrey, G.; Quigley, C.E.; Finch, J.; DeMarco, K.M.; Nametz, N.; Davis, T.P. Oxidative Stress Increases Blood–Brain Barrier Permeability and Induces Alterations in Occludin during Hypoxia–Reoxygenation. J. Cereb. Blood Flow. Metab. 2010, 30, 1625–1636. [Google Scholar] [CrossRef]
- Pun, P.B.L.; Lu, J.; Moochhala, S. Involvement of ROS in BBB Dysfunction. Free Radic. Res. 2009, 43, 348–364. [Google Scholar] [CrossRef]
- Prakash, R.; Carmichael, S.T. Blood–Brain Barrier Breakdown and Neovascularization Processes after Stroke and Traumatic Brain Injury. Curr. Opin. Neurol. 2015, 28, 556–564. [Google Scholar] [CrossRef]
- Okada, T.; Suzuki, H.; Travis, Z.D.; Zhang, J.H. The Stroke-Induced Blood-Brain Barrier Disruption: Current Progress of Inspection Technique, Mechanism, and Therapeutic Target. Curr. Neuropharmacol. 2020, 18, 1187–1212. [Google Scholar] [CrossRef]
- Maldonado, E.; Morales-Pison, S.; Urbina, F.; Solari, A. Aging Hallmarks and the Role of Oxidative Stress. Antioxidants 2023, 12, 651. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Kornatowski, M.; Krzywińska, O.; Kędziora-Kornatowska, K. Changes in the Blood Antioxidant Defense of Advanced Age People. Clin. Interv. Aging 2019, 14, 763–771. [Google Scholar] [CrossRef]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Sacchetti, G.; Gonelli, A.; Neri, L.M. Oxidative Stress: Role of Physical Exercise and Antioxidant Nutraceuticals in Adulthood and Aging. Oncotarget 2018, 9, 17181–17198. [Google Scholar] [CrossRef]
- Bouzid, M.A.; Filaire, E.; Matran, R.; Robin, S.; Fabre, C. Lifelong Voluntary Exercise Modulates Age-Related Changes in Oxidative Stress. Int. J. Sports Med. 2018, 40, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Debold, E. Potential Molecular Mechanisms Underlying Muscle Fatigue Mediated by Reactive Oxygen and Nitrogen Species. Front. Physiol. 2015, 6, 153038. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, X.; Liu, Y.; Zhang, Z. Effects of Exercise-Induced ROS on the Pathophysiological Functions of Skeletal Muscle. Oxidative Med. Cell. Longev. 2021, 2021, e3846122. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.B. Free Radicals and Muscle Fatigue: Of ROS, Canaries, and the IOC. Free Radic. Biol. Med. 2008, 44, 169–179. [Google Scholar] [CrossRef]
- Ferreira, L.F.; Reid, M.B. Muscle-Derived ROS and Thiol Regulation in Muscle Fatigue. J. Appl. Physiol. 2008, 104, 853–860. [Google Scholar] [CrossRef]
- Matuszczak, Y.; Farid, M.; Jones, J.; Lansdowne, S.; Smith, M.A.; Taylor, A.A.; Reid, M.B. Effects of N-Acetylcysteine on Glutathione Oxidation and Fatigue during Handgrip Exercise. Muscle Nerve 2005, 32, 633–638. [Google Scholar] [CrossRef]
- Augestad, I.L.; Dekens, D.; Karampatsi, D.; Elabi, O.; Zabala, A.; Pintana, H.; Larsson, M.; Nyström, T.; Paul, G.; Darsalia, V.; et al. Normalisation of Glucose Metabolism by Exendin-4 in the Chronic Phase after Stroke Promotes Functional Recovery in Male Diabetic Mice. Br. J. Pharmacol. 2022, 179, 677–694. [Google Scholar] [CrossRef] [PubMed]
- Vergès, B.; Aboyans, V.; Angoulvant, D.; Boutouyrie, P.; Cariou, B.; Hyafil, F.; Mohammedi, K.; Amarenco, P. Protection against Stroke with Glucagon-like Peptide-1 Receptor Agonists: A Comprehensive Review of Potential Mechanisms. Cardiovasc. Diabetol. 2022, 21, 242. [Google Scholar] [CrossRef] [PubMed]
- Maskery, M.P.; Holscher, C.; Jones, S.P.; Price, C.I.; Strain, W.D.; Watkins, C.L.; Werring, D.J.; Emsley, H.C. Glucagon-like Peptide-1 Receptor Agonists as Neuroprotective Agents for Ischemic Stroke: A Systematic Scoping Review. J. Cereb. Blood Flow Metab. 2021, 41, 14–30. [Google Scholar] [CrossRef]
- Pigazzani, F.; Gorni, D.; Dyar, K.A.; Pedrelli, M.; Kennedy, G.; Costantino, G.; Bruno, A.; Mackenzie, I.; MacDonald, T.M.; Tietge, U.J.F.; et al. The Prognostic Value of Derivatives-Reactive Oxygen Metabolites (d-ROMs) for Cardiovascular Disease Events and Mortality: A Review. Antioxidants 2022, 11, 1541. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Baik, H.W.; Yoon, Y.S.; Joung, H.J.; Park, J.S.; Park, S.J.; Jang, E.J.; Park, S.W.; Kim, S.J.; Kim, M.J.; et al. Measurement of Antioxidant Capacity Using the Biological Antioxidant Potential Test and Its Role as a Predictive Marker of Metabolic Syndrome. Korean J. Intern. Med. 2014, 29, 31–39. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Baseline Characteristics | Whole Group (n = 109) | Women (n = 51) | Men (n = 58) | p-Value |
|---|---|---|---|---|
| Age (years) | 69 ± 11 | 72 ± 9 | 67 ± 12 | 0.027 * |
| Anthropometric value | ||||
| Weight (kg) | 69 ± 17 | 62 ± 13 | 75 ± 18 | <0.001 *** |
| Height (m) | 1.7 ± 10.2 | 1.6 ± 6.7 | 1.7 ± 10.2 | <0.001 *** |
| BMI (kg/m2) | 24.9 ± 4.8 | 24.2 ± 5.1 | 25.5 ± 4.4 | 0.055 |
| Index stroke type | ||||
| Ischemic | 86 (79%) | 42 (82%) | 44 (76%) | 0.412 |
| Haemorrhagic | 23 (21%) | 9 (18%) | 14 (24%) | |
| Affected side | ||||
| Right | 58 (53%) | 27 (53%) | 31 (56%) | 0.961 |
| Left | 51 (47%) | 24 (47%) | 27 (47%) | |
| Smoking | 50 (46%) | 19 (37%) | 31 (53%) | 0.103 |
| Comorbidities | ||||
| Hypertension | 93 (85%) | 44 (86%) | 49 (84%) | 0.797 |
| Type 2 diabetes | 28 (26%) | 12 (24%) | 16 (28%) | 0.633 |
| Dyslipidaemia | 45 (41%) | 22 (43%) | 23 (40%) | 0.716 |
| Heart disease | 16 (17%) | 4 (9%) | 12 (23%) | 0.082 |
| Dysphagia | 29 (27%) | 16 (31%) | 13 (22%) | 0.451 |
| Cumulative Illness Rating Scale (CIRS) | ||||
| CIRS severity | 2.2 ± 0.4 | 2.2 ± 0.4 | 2.1 ± 0.4 | 0.066 |
| CIRS comorbidity | 5.1 ± 2.0 | 5.3 ± 1.9 | 4.9 ± 2.2 | 0.285 |
| Days from stroke onset to enrolment | 87 ± 57 | 97 ± 62 | 77 ± 52 | 0.079 |
| Activity of Daily Living (ADL) assessment | ||||
| Modified Barthel Index (mBI) | 42 ± 22 | 37 ± 19 | 46 ± 24 | 0.094 |
| Endurance motor assessment | (n = 17) | (n = 6) | (n = 11) | |
| 6 min walk test (6MWT, m/min) | 296 ± 122 | 249 ± 150 | 321 ± 102 | 0.313 |
| Strength of arms | ||||
| Hand Grip test of unaffected arm (kg) | 19.8 ± 11.6 | 15.1 ± 8.7 | 23.9 ± 12.4 | <0.001 *** |
| Hand Grip test of affected arm (kg) | 6.2 ± 8.1 | 3.9 ± 8.2 | 8.2 ± 9.6 | 0.015 * |
| Ematochemical analyses | ||||
| Glucose (mg/dL) | 111 ± 39 | 116 ± 45 | 105 ± 33 | 0.294 |
| Cholesterol (mg/dL) | 126 ± 37 | 133 ± 41 | 119 ± 31 | 0.207 |
| HDL cholesterol (mg/dL) | 53 ± 17 | 57 ± 15 | 49 ± 18 | 0.005 ** |
| Triglycerides (mg/dL) | 123 ± 58 | 120 ± 61 | 126 ± 56 | 0.372 |
| Oxidative Stress Parameters | Whole Group (n = 109) | Women (n = 51) | Men (n = 58) | p-Value |
|---|---|---|---|---|
| d-ROMs (UCARR) | 549 ± 126 | 562 ± 139 | 537 ± 113 | 0.498 |
| BAP (µmol/L) | 2255 ± 440 | 2267 ± 491 | 2244 ± 394 | 0.810 |
| -SHp (µmol/L) | 587 ± 146 | 580 ± 131 | 593 ± 158 | 0.987 |
| OSI index (BAP/d-ROMs) | 4.3 ± 1.3 | 4.3 ± 1.4 | 4.4 ± 1.3 | 0.585 |
| SH-OSI index (-SHp/d-ROMs) | 1.1 ± 0.4 | 1.1 ± 0.4 | 1.2 ± 0.4 | 0.598 |
| mBI | Hand Grip Test Unaffected Arm (kg) | Hand Grip Test Affected Arm (kg) | ||||
|---|---|---|---|---|---|---|
| Oxidative Stress | Spearman’s Rho | p | Spearman’s Rho | p | Spearman’s Rho | p |
| d-ROMs (UCARR) | −0.300 ** | 0.003 | −0.091 | 0.367 | −0.138 | 0.170 |
| BAP (µmol/L) | 0.013 | 0.898 | −7.839 × 10−4 | 0.994 | −0.045 | 0.657 |
| -SHp (µmol/L) | 0.244 * | 0.103 | 0.326 *** | <0.001 | 0.201 * | 0.044 |
| OSI index (BAP/d-ROMs) | 0.265 ** | 0.007 | 0.053 | 0.596 | 0.113 | 0.262 |
| SH-OSI index (SHp/d-ROMs) | 0.324 *** | <0.001 | 0.276 ** | 0.005 | 0.258 ** | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cocco, C.; Siotto, M.; Guerrini, A.; Germanotta, M.; Galluccio, C.; Cipollini, V.; Cortellini, L.; Pavan, A.; Lattanzi, S.; Insalaco, S.; et al. Systemic Oxidative Stress in Subacute Stroke Patients Undergoing Rehabilitation Treatment. Antioxidants 2024, 13, 354. https://doi.org/10.3390/antiox13030354
Cocco C, Siotto M, Guerrini A, Germanotta M, Galluccio C, Cipollini V, Cortellini L, Pavan A, Lattanzi S, Insalaco S, et al. Systemic Oxidative Stress in Subacute Stroke Patients Undergoing Rehabilitation Treatment. Antioxidants. 2024; 13(3):354. https://doi.org/10.3390/antiox13030354
Chicago/Turabian StyleCocco, Carola, Mariacristina Siotto, Alessandro Guerrini, Marco Germanotta, Caterina Galluccio, Valeria Cipollini, Laura Cortellini, Arianna Pavan, Stefania Lattanzi, Sabina Insalaco, and et al. 2024. "Systemic Oxidative Stress in Subacute Stroke Patients Undergoing Rehabilitation Treatment" Antioxidants 13, no. 3: 354. https://doi.org/10.3390/antiox13030354
APA StyleCocco, C., Siotto, M., Guerrini, A., Germanotta, M., Galluccio, C., Cipollini, V., Cortellini, L., Pavan, A., Lattanzi, S., Insalaco, S., Ruco, E., Mosca, R., Campana, B., & Aprile, I. (2024). Systemic Oxidative Stress in Subacute Stroke Patients Undergoing Rehabilitation Treatment. Antioxidants, 13(3), 354. https://doi.org/10.3390/antiox13030354