
Enhancing the Bioavailability and Bioactivity of Curcumin for Disease Prevention and Treatment

 , , ,
, , , 
Abstract
1. Introduction
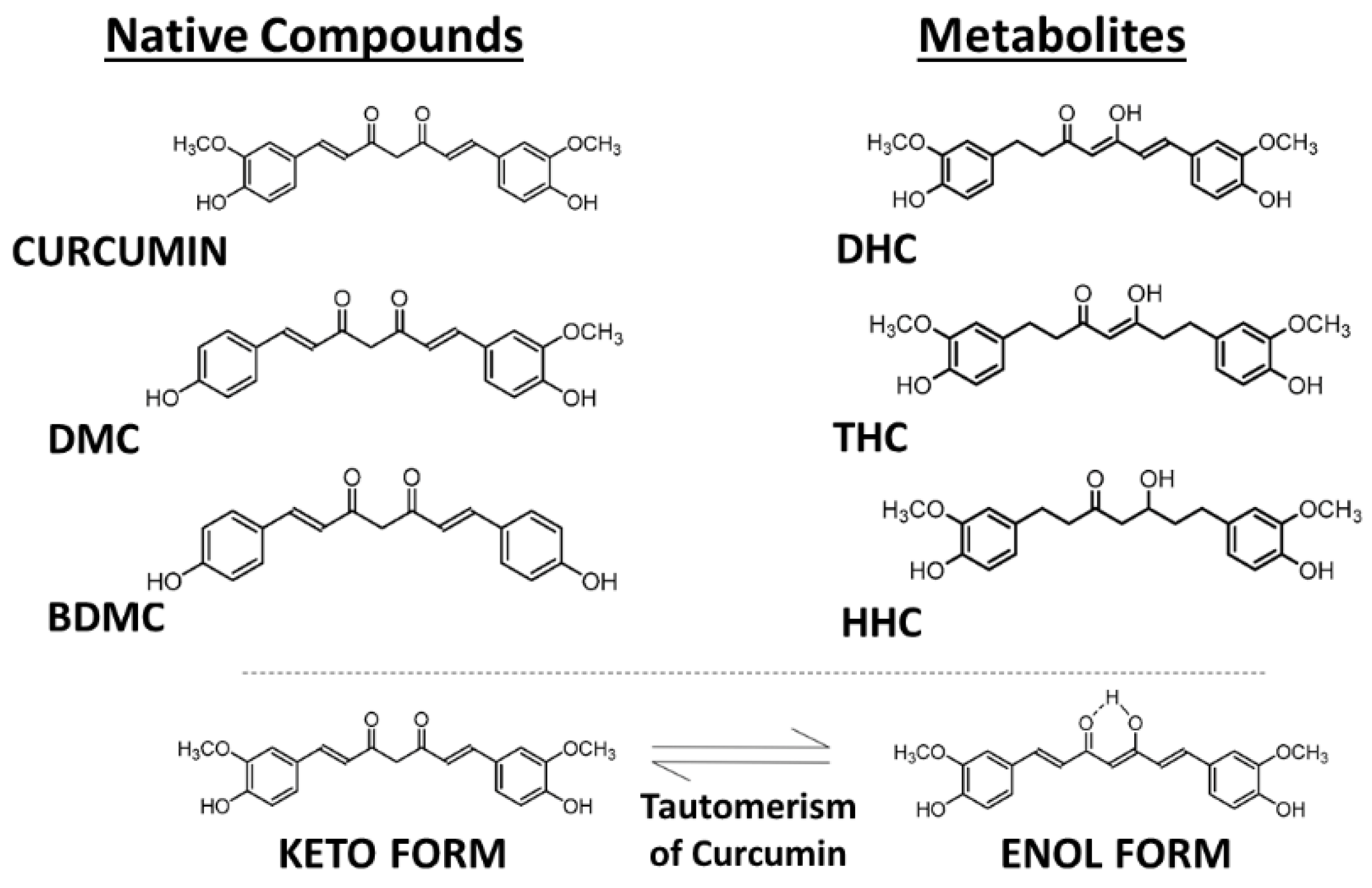
2. Curcumin and Curcuminoids
2.1. Comparative Analysis of Curcumin Levels in the Body versus Cell Culture
2.1.1. Curcumin Levels in Serum and Plasma
2.1.2. Curcumin Levels in the Intestine
2.1.3. Curcumin Levels in Cultured Cells
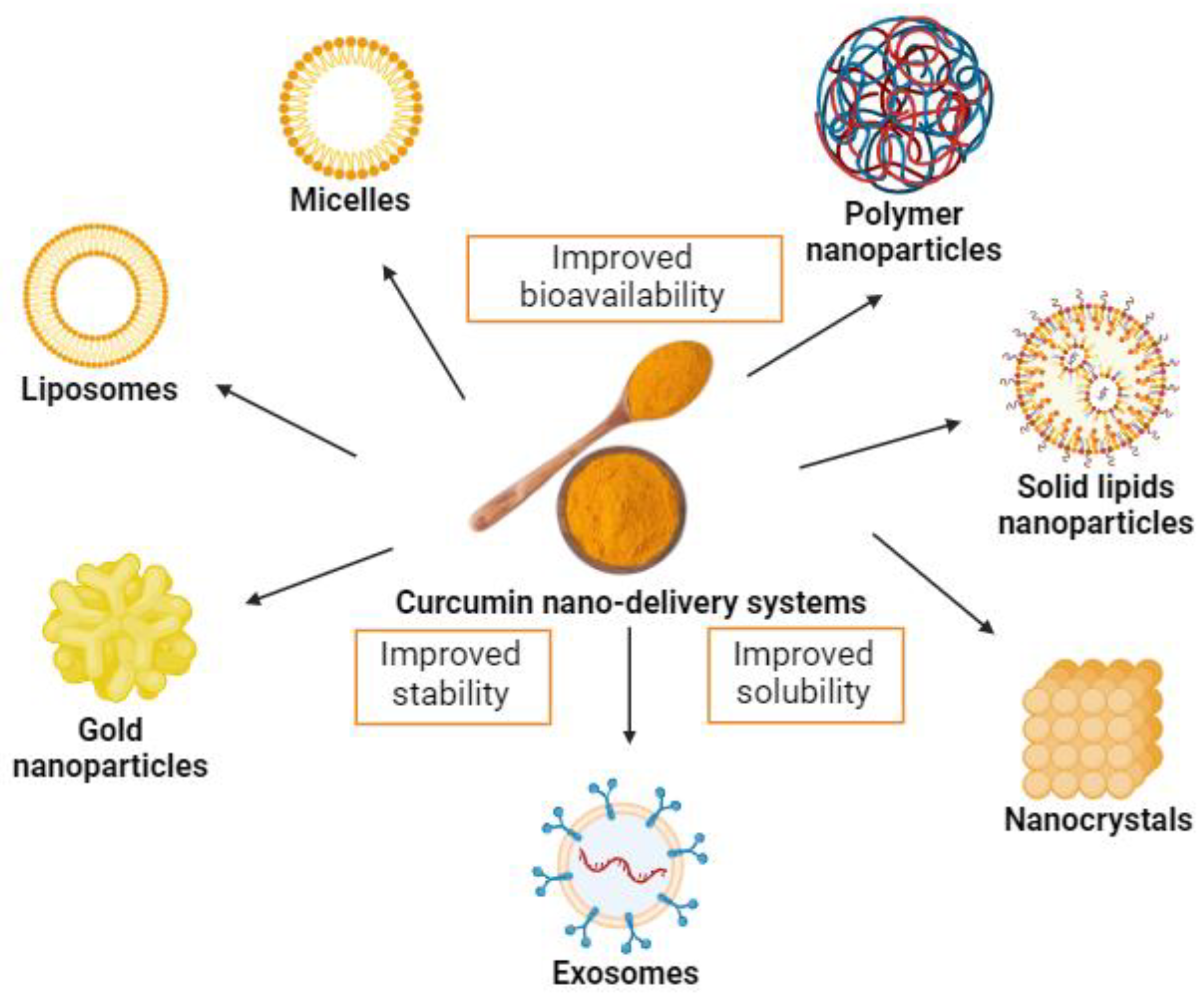
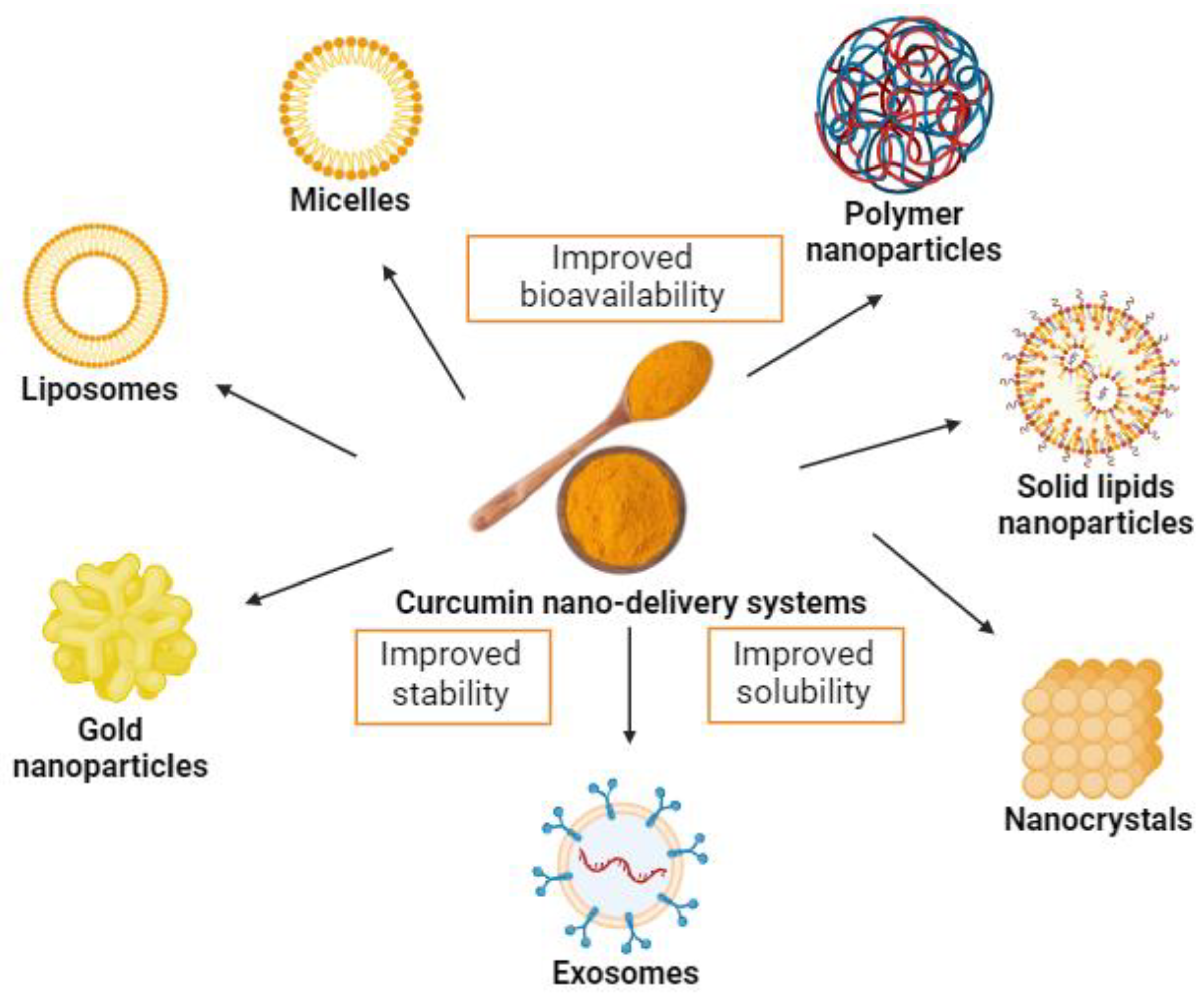
2.2. Increasing the Bioavailability of Curcumin with Nanoformulations

{kind=link}
{kind=link}
{kind=link}
| Formulation | Composition | Bioavailability Increase | Reference |
|---|---|---|---|
| Micronized curcumin with turmeric essential oils (BCM-95CG) (Biocurcumax) | Combination of curcuminoids with volatile oils of turmeric rhizome, which are usually eliminated during preparation. | 7-fold, compared to 6.4-fold with curcumin−lecithin−piperine. | [67] |
| Curcumin as solid lipid particles (LONGVIDA, M3C-X) | Solid lipid curcumin particles (SLCPs) with soy lecithin containing purified phospholipids, docosahexaenoic acid (DHA), and/or vegetable stearic acid, ascorbyl (vitamin C) esters, and inert ingredients. | Plasma concentrations of 22.43 ng/mL after 2.4 h, compared to undetectable levels without formulation. | [68] |
| Colloidal nanoparticles dispersed with a high-pressure homogenizer (THERACURMIN) | Nanoparticle colloidal dispersion, prepared with gum ghatti and glycerine, consisting of 10 w/w% of curcumin, 2% of other curcuminoids such as demethoxycurcumin and bisdemethoxycurcumin, 46% of glycerin, 4% of gum ghatti, and 38% of water. | Tmax and AUC0–6 h values for total curcumin: 27.6-fold increased stability, water-solubility, stable preparation, and enhanced gastrointestinal absorption. | [69] |
| A 95% soybean-based phospholipid−curcumin formulation (Meriva) | Lipophilic matrix composed of curcumin/soybean lecithin/microcrystalline cellulose (1:2:2), 43 mg per capsule: curcumin (33 mg), demethoxycurcumin (8 mg), and bisdemethoxycurcumin (1 mg)— total curcuminoids 42 mg. | Increased absorption of curcumin and total curcuminoids by 19- and 32-fold, respectively. Increased absorption of DMC by 68-fold and of BDMC by 57-fold; hydrolytic stabilization of curcumin at intestinal pH may increase the curcumin load for the gut microbiota. | [70] |
| Encapsulated curcumin | Inner coating material of microcapsules was constituted by cellulose derivative (Ethocel 100) as a first layer and hydrogenated vegetable oil (HVO) as an external layer. | Curcuminoid microencapsulation increased bioavailability from enriched bread, probably preventing biotransformation. | [71] |
| Micronized curcumin powder | Micronized powder and particularly liquid micellar formulation of curcumin. | Oral bioavailability with AUC values in plasma for total curcumin 9- and 185-fold, respectively. Higher concentrations of DMC and BDMC were also observed. | [72] |
| Comparison of formulations of curcumin: CHC (cellulosic derivatives with antioxidants) CC (cellulosic derivatives with γ- cyclodextrin) CP (phytosome formulation) CTR (formulation with volatile oils of turmeric rhizome) | Combinations of a hydrophilic carrier. | The total concentration of curcuminoids in the new formulations was higher (45.9-fold in CHC and 37.4-fold in CC) than in CP (7.9- to 8.4-fold) and CTR (1.2- to 1.3-fold). | [73,74] |
| Curcumin solid dispersion (C-SD) | Large particle sizes of C-SDs were pulverized using zirconia beads. | Particle size determined the uptake, with an increased uptake of small particles orally, and an increased uptake of large particles intravenously in rats. | [54] |
2.3. Antimicrobial Action of Curcumin and Curcumin Nanoformulations
2.4. Regulatory Effects of Curcumin and Curcumin Nanoformulations in Different Tissues
2.4.1. Regulatory Effects of Curcumin in the Intestine and on the Microbiome
2.4.2. Regulatory Effects of Curcumin in the Liver and Adipose Tissue
2.4.3. Regulatory Effects of Curcumin in Heart and Vessels
2.4.4. Regulatory Effects of Curcumin in Brain and Cognitive Disorders
2.5. Potential Safe Concentration Range and Toxicity of Curcumin
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Strimpakos, A.S.; Sharma, R.A. Curcumin: Preventive and Therapeutic Properties in Laboratory Studies and Clinical Trials. Antioxid. Redox Signal. 2008, 10, 511–545. [Google Scholar] [CrossRef]
- Aggarwal, B.B. Targeting Inflammation-Induced Obesity and Metabolic Diseases by Curcumin and Other Nutraceuticals. Annu. Rev. Nutr. 2010, 30, 173–199. [Google Scholar] [CrossRef]
- Epstein, J.; Sanderson, I.R.; Macdonald, T.T. Curcumin as a Therapeutic Agent: The Evidence from in Vitro, Animal and Human Studies. Br. J. Nutr. 2010, 103, 1545–1557. [Google Scholar] [CrossRef]
- Shehzad, A.; Ha, T.; Subhan, F.; Lee, Y.S. New Mechanisms and the Anti-Inflammatory Role of Curcumin in Obesity and Obesity-Related Metabolic Diseases. Eur. J. Nutr. 2011, 50, 151–161. [Google Scholar] [CrossRef]
- Gupta, S.C.; Patchva, S.; Koh, W.; Aggarwal, B.B. Discovery of Curcumin, a Component of Golden Spice, and Its Miraculous Biological Activities. Clin. Exp. Pharmacol. Physiol. 2012, 39, 283–299. [Google Scholar] [CrossRef]
- Gupta, S.C.; Patchva, S.; Aggarwal, B.B. Therapeutic Roles of Curcumin: Lessons Learned from Clinical Trials. AAPS J. 2013, 15, 195–218. [Google Scholar] [CrossRef] [PubMed]
- Itaya, M.; Miyazawa, T.; Zingg, J.-M.; Eitsuka, T.; Azzi, A.; Meydani, M.; Miyazawa, T.; Nakagawa, K. The Differential Cellular Uptake of Curcuminoids in Vitro Depends Dominantly on Albumin Interaction. Phytomedicine 2019, 59, 152902. [Google Scholar] [CrossRef]
- Priyadarsini, K.I. The Chemistry of Curcumin: From Extraction to Therapeutic Agent. Molecules 2014, 19, 20091–20112. [Google Scholar] [CrossRef] [PubMed]
- Carlson, S. GRAS-Notice-GRN-822-Agency-Response-Letter; U.S. Food and Drug Administration, Center for Food Safety & Applied Nutrition: College Park, MD, USA, 2019; pp. 1–5.
- Asai, A.; Miyazawa, T. Dietary Curcuminoids Prevent High-Fat Diet-Induced Lipid Accumulation in Rat Liver and Epididymal Adipose Tissue. J. Nutr. 2001, 131, 2932–2935. [Google Scholar] [CrossRef] [PubMed]
- Shoji, M.; Nakagawa, K.; Watanabe, A.; Tsuduki, T.; Yamada, T.; Kuwahara, S.; Kimura, F.; Miyazawa, T. Comparison of the Effects of Curcumin and Curcumin Glucuronide in Human Hepatocellular Carcinoma HepG2 Cells. Food Chem. 2014, 151, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.H.; Huang, T.M.; Lin, J.K. Biotransformation of Curcumin through Reduction and Glucuronidation in Mice. Drug Metab. Dispos. 1999, 27, 486–494. [Google Scholar]
- Ryu, E.K.; Choe, Y.S.; Lee, K.-H.; Choi, Y.; Kim, B.-T. Curcumin and Dehydrozingerone Derivatives: Synthesis, Radiolabeling, and Evaluation for Beta-Amyloid Plaque Imaging. J. Med. Chem. 2006, 49, 6111–6119. [Google Scholar] [CrossRef]
- Girardon, M.; Parant, S.; Monari, A.; Dehez, F.; Chipot, C.; Rogalska, E.; Canilho, N.; Pasc, A. Triggering Tautomerization of Curcumin by Confinement into Liposomes. ChemPhotoChem 2019, 3, 1034–1041. [Google Scholar] [CrossRef]
- Chowdhury, R.; Nimmanapalli, R.; Graham, T.; Reddy, G. Curcumin Attenuation of Lipopolysaccharide Induced Cardiac Hypertrophy in Rodents. ISRN Inflamm. 2013, 2013, 539305. [Google Scholar] [CrossRef]
- Marczylo, T.H.; Steward, W.P.; Gescher, A.J. Rapid Analysis of Curcumin and Curcumin Metabolites in Rat Biomatrices Using a Novel Ultraperformance Liquid Chromatography (UPLC) Method. J. Agric. Food Chem. 2009, 57, 797–803. [Google Scholar] [CrossRef]
- Shoba, G.; Joy, D.; Joseph, T.; Majeed, M.; Rajendran, R.; Srinivas, P.S. Influence of Piperine on the Pharmacokinetics of Curcumin in Animals and Human Volunteers. Planta Med. 1998, 64, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, N.; Aggarwal, B.B.; Newman, R.A.; Wolff, R.A.; Kunnumakkara, A.B.; Abbruzzese, J.L.; Ng, C.S.; Badmaev, V.; Kurzrock, R. Phase II Trial of Curcumin in Patients with Advanced Pancreatic Cancer. Clin. Cancer Res. an Off. J. Am. Assoc. Cancer Res. 2008, 14, 4491–4499. [Google Scholar] [CrossRef]
- Lao, C.D.; Ruffin, M.T., 4th; Normolle, D.; Heath, D.D.; Murray, S.I.; Bailey, J.M.; Boggs, M.E.; Crowell, J.; Rock, C.L.; Brenner, D.E. Dose Escalation of a Curcuminoid Formulation. BMC Complement. Altern. Med. 2006, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.A.; Ireson, C.R.; Verschoyle, R.D.; Hill, K.A.; Williams, M.L.; Leuratti, C.; Manson, M.M.; Marnett, L.J.; Steward, W.P.; Gescher, A. Effects of Dietary Curcumin on Glutathione S-Transferase and Malondialdehyde-DNA Adducts in Rat Liver and Colon Mucosa: Relationship with Drug Levels. Clin. Cancer Res. An Off. J. Am. Assoc. Cancer Res. 2001, 7, 1452–1458. [Google Scholar]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I Clinical Trial of Curcumin, a Chemopreventive Agent, in Patients with High-Risk or Pre-Malignant Lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar] [PubMed]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M.; et al. Phase I Clinical Trial of Oral Curcumin: Biomarkers of Systemic Activity and Compliance. Clin. Cancer Res. An Off. J. Am. Assoc. Cancer Res. 2004, 10, 6847–6854. [Google Scholar] [CrossRef]
- Feng, W.; Wang, H.; Zhang, P.; Gao, C.; Tao, J.; Ge, Z.; Zhu, D.; Bi, Y. Modulation of Gut Microbiota Contributes to Curcumin-Mediated Attenuation of Hepatic Steatosis in Rats. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B.; Kumar, A.; Bharti, A.C. Anticancer Potential of Curcumin: Preclinical and Clinical Studies. Anticancer Res. 2003, 23, 363–398. [Google Scholar] [PubMed]
- Wang, Y.J.; Pan, M.H.; Cheng, A.L.; Lin, L.I.; Ho, Y.S.; Hsieh, C.Y.; Lin, J.K. Stability of Curcumin in Buffer Solutions and Characterization of Its Degradation Products. J. Pharm. Biomed. Anal. 1997, 15, 1867–1876. [Google Scholar] [CrossRef] [PubMed]
- Perkins, S.; Verschoyle, R.D.; Hill, K.; Parveen, I.; Threadgill, M.D.; Sharma, R.A.; Williams, M.L.; Steward, W.P.; Gescher, A.J. Chemopreventive Efficacy and Pharmacokinetics of Curcumin in the Min/+ Mouse, a Model of Familial Adenomatous Polyposis. Cancer Epidemiol. Biomark. Prev. A Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2002, 11, 535–540. [Google Scholar]
- Garcea, G.; Berry, D.P.; Jones, D.J.L.; Singh, R.; Dennison, A.R.; Farmer, P.B.; Sharma, R.A.; Steward, W.P.; Gescher, A.J. Consumption of the Putative Chemopreventive Agent Curcumin by Cancer Patients: Assessment of Curcumin Levels in the Colorectum and Their Pharmacodynamic Consequences. Cancer Epidemiol. Biomark. Prev. A Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2005, 14, 120–125. [Google Scholar] [CrossRef]
- Irving, G.R.B.; Howells, L.M.; Sale, S.; Kralj-Hans, I.; Atkin, W.S.; Clark, S.K.; Britton, R.G.; Jones, D.J.L.; Scott, E.N.; Berry, D.P.; et al. Prolonged Biologically Active Colonic Tissue Levels of Curcumin Achieved after Oral Administration—A Clinical Pilot Study Including Assessment of Patient Acceptability. Cancer Prev. Res. 2013, 6, 119–128. [Google Scholar] [CrossRef]
- Muangnoi, C.; Ratnatilaka Na Bhuket, P.; Jithavech, P.; Supasena, W.; Paraoan, L.; Patumraj, S.; Rojsitthisak, P. Curcumin Diethyl Disuccinate, a Prodrug of Curcumin, Enhances Anti-Proliferative Effect of Curcumin against HepG2 Cells via Apoptosis Induction. Sci. Rep. 2019, 9, 11718. [Google Scholar] [CrossRef]
- Nakagawa, K.; Zingg, J.-M.; Kim, S.H.; Thomas, M.J.; Dolnikowski, G.G.; Azzi, A.; Miyazawa, T.; Meydani, M. Differential Cellular Uptake and Metabolism of Curcuminoids in Monocytes/Macrophages: Regulatory Effects on Lipid Accumulation. Br. J. Nutr. 2014, 112, 8–14. [Google Scholar] [CrossRef]
- Polia, F.; Pastor-Belda, M.; Martínez-Blázquez, A.; Horcajada, M.-N.; Tomás-Barberán, F.A.; García-Villalba, R. Technological and Biotechnological Processes To Enhance the Bioavailability of Dietary (Poly)Phenols in Humans. J. Agric. Food Chem. 2022, 70, 2092–2107. [Google Scholar] [CrossRef]
- Hettiarachchi, S.S.; Dunuweera, S.P.; Dunuweera, A.N.; Rajapakse, R.M.G. Synthesis of Curcumin Nanoparticles from Raw Turmeric Rhizome. ACS Omega 2021, 6, 8246–8252. [Google Scholar] [CrossRef]
- Hegde, M.; Girisa, S.; BharathwajChetty, B.; Vishwa, R.; Kunnumakkara, A.B. Curcumin Formulations for Better Bioavailability: What We Learned from Clinical Trials Thus Far? ACS Omega 2023, 8, 10713–10746. [Google Scholar] [CrossRef]
- Sun, H.; Zhan, M.; Mignani, S.; Shcharbin, D.; Majoral, J.-P.; Rodrigues, J.; Shi, X.; Shen, M. Modulation of Macrophages Using Nanoformulations with Curcumin to Treat Inflammatory Diseases: A Concise Review. Pharmaceutics 2022, 14, 2239. [Google Scholar] [CrossRef]
- Trigo-Gutierrez, J.K.; Vega-Chacón, Y.; Soares, A.B.; Mima, E.G. de O. Antimicrobial Activity of Curcumin in Nanoformulations: A Comprehensive Review. Int. J. Mol. Sci. 2021, 22, 7130. [Google Scholar] [CrossRef]
- Ansari, L.; Mashayekhi-Sardoo, H.; Baradaran Rahimi, V.; Yahyazadeh, R.; Ghayour-Mobarhan, M.; Askari, V.R. Curcumin-Based Nanoformulations Alleviate Wounds and Related Disorders: A Comprehensive Review. Biofactors 2023. [Google Scholar] [CrossRef]
- Ma, Z.; Wang, N.; He, H.; Tang, X. Pharmaceutical Strategies of Improving Oral Systemic Bioavailability of Curcumin for Clinical Application. J. Control. Release 2019, 316, 359–380. [Google Scholar] [CrossRef]
- Quispe, C.; Cruz-Martins, N.; Manca, M.L.; Manconi, M.; Sytar, O.; Hudz, N.; Shanaida, M.; Kumar, M.; Taheri, Y.; Martorell, M.; et al. Nano-Derived Therapeutic Formulations with Curcumin in Inflammation-Related Diseases. Oxid. Med. Cell. Longev. 2021, 2021, 3149223. [Google Scholar] [CrossRef]
- Laurindo, L.F.; de Carvalho, G.M.; de Oliveira Zanuso, B.; Figueira, M.E.; Direito, R.; de Alvares Goulart, R.; Buglio, D.S.; Barbalho, S.M. Curcumin-Based Nanomedicines in the Treatment of Inflammatory and Immunomodulated Diseases: An Evidence-Based Comprehensive Review. Pharmaceutics 2023, 15, 229. [Google Scholar] [CrossRef] [PubMed]
- Witika, B.A.; Makoni, P.A.; Matafwali, S.K.; Mweetwa, L.L.; Shandele, G.C.; Walker, R.B. Enhancement of Biological and Pharmacological Properties of an Encapsulated Polyphenol: Curcumin. Molecules 2021, 26, 4244. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, F.; Lavi Arab, F.; Jaafari, M.R.; Rastin, M.; Tabasi, N.; Hatamipour, M.; Nikkhah, K.; Mahmoudi, M. Immunoregulatory, Proliferative and Anti-Oxidant Effects of Nanocurcuminoids on Adipose-Derived Mesenchymal Stem Cells. EXCLI J. 2019, 18, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Pillai, S.C.; Borah, A.; Le, M.N.T.; Kawano, H.; Hasegawa, K.; Kumar, D.S. Co-Delivery of Curcumin and Bioperine via PLGA Nanoparticles to Prevent Atherosclerotic Foam Cell Formation. Pharmaceutics 2021, 13, 1420. [Google Scholar] [CrossRef]
- Ashtary-Larky, D.; Rezaei Kelishadi, M.; Bagheri, R.; Moosavian, S.P.; Wong, A.; Davoodi, S.H.; Khalili, P.; Dutheil, F.; Suzuki, K.; Asbaghi, O. The Effects of Nano-Curcumin Supplementation on Risk Factors for Cardiovascular Disease: A GRADE-Assessed Systematic Review and Meta-Analysis of Clinical Trials. Antioxidants 2021, 10, 1015. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.-M.; Chien, C.-F.; Lin, L.-C.; Tsai, T.-H. Curcumin and Its Nano-Formulation: The Kinetics of Tissue Distribution and Blood-Brain Barrier Penetration. Int. J. Pharm. 2011, 416, 331–338. [Google Scholar] [CrossRef]
- Shindikar, A.; Singh, A.; Nobre, M.; Kirolikar, S. Curcumin and Resveratrol as Promising Natural Remedies with Nanomedicine Approach for the Effective Treatment of Triple Negative Breast Cancer. J. Oncol. 2016, 2016, 9750785. [Google Scholar] [CrossRef]
- Silvestre, F.; Santos, C.; Silva, V.; Ombredane, A.; Pinheiro, W.; Andrade, L.; Garcia, M.; Pacheco, T.; Joanitti, G.; Luz, G.; et al. Pharmacokinetics of Curcumin Delivered by Nanoparticles and the Relationship with Antitumor Efficacy: A Systematic Review. Pharmaceuticals 2023, 16, 943. [Google Scholar] [CrossRef]
- Marrache, S.; Dhar, S. Engineering of Blended Nanoparticle Platform for Delivery of Mitochondria-Acting Therapeutics. Proc. Natl. Acad. Sci. USA 2012, 109, 16288–16293. [Google Scholar] [CrossRef]
- Amalraj, A.; Gopi, S.; Pius, A.; Gopi, S. Biological Activities of Curcuminoids, Other Biomolecules from Turmeric and Their Derivatives—A Review. J. Tradit. Complement. Med. 2017, 7, 205–233. [Google Scholar] [CrossRef] [PubMed]
- Fanali, G.; Fasano, M.; Ascenzi, P.; Zingg, J.-M.; Azzi, A. α-Tocopherol Binding to Human Serum Albumin. Biofactors 2013, 39, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Nakatomi, T.; Itaya-Takahashi, M.; Horikoshi, Y.; Shimizu, N.; Parida, I.S.; Jutanom, M.; Eitsuka, T.; Tanaka, Y.; Zingg, J.-M.; Matsura, T.; et al. The Difference in the Cellular Uptake of Tocopherol and Tocotrienol Is Influenced by Their Affinities to Albumin. Sci. Rep. 2023, 13, 7392. [Google Scholar] [CrossRef]
- Kou, M.-C.; Chiou, S.-Y.; Weng, C.-Y.; Wang, L.; Ho, C.-T.; Wu, M.-J. Curcuminoids Distinctly Exhibit Antioxidant Activities and Regulate Expression of Scavenger Receptors and Heme Oxygenase-1. Mol. Nutr. Food Res. 2013, 57, 1598–1610. [Google Scholar] [CrossRef]
- Jamwal, R. Bioavailable Curcumin Formulations: A Review of Pharmacokinetic Studies in Healthy Volunteers. J. Integr. Med. 2018, 16, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-S.; Cao, J.; Naeem, M.; Noh, J.; Hasan, N.; Choi, H.-K.; Yoo, J.-W. Size-Controlled Biodegradable Nanoparticles: Preparation and Size-Dependent Cellular Uptake and Tumor Cell Growth Inhibition. Colloids Surf. B. Biointerfaces 2014, 122, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Kato, C.; Itaya-Takahashi, M.; Miyazawa, T.; Ito, J.; Parida, I.S.; Yamada, H.; Abe, A.; Shibata, M.; Someya, K.; Nakagawa, K. Effects of Particle Size of Curcumin Solid Dispersions on Bioavailability and Anti-Inflammatory Activities. Antioxidants 2023, 12, 724. [Google Scholar] [CrossRef]
- Kunnumakkara, A.B.; Hegde, M.; Parama, D.; Girisa, S.; Kumar, A.; Daimary, U.D.; Garodia, P.; Yenisetti, S.C.; Oommen, O.V.; Aggarwal, B.B. Role of Turmeric and Curcumin in Prevention and Treatment of Chronic Diseases: Lessons Learned from Clinical Trials. ACS Pharmacol. Transl. Sci. 2023, 6, 447–518. [Google Scholar] [CrossRef] [PubMed]
- Yallapu, M.M.; Nagesh, P.K.B.; Jaggi, M.; Chauhan, S.C. Therapeutic Applications of Curcumin Nanoformulations. AAPS J. 2015, 17, 1341–1356. [Google Scholar] [CrossRef] [PubMed]
- Mahjoob, M.; Stochaj, U. Curcumin Nanoformulations to Combat Aging-Related Diseases. Ageing Res. Rev. 2021, 69, 101364. [Google Scholar] [CrossRef] [PubMed]
- Zingg, J.-M.; Hasan, S.T.; Meydani, M. Molecular Mechanisms of Hypolipidemic Effects of Curcumin. Biofactors 2013, 39, 101–121. [Google Scholar] [CrossRef]
- Panahi, Y.; Ahmadi, Y.; Teymouri, M.; Johnston, T.P.; Sahebkar, A. Curcumin as a Potential Candidate for Treating Hyperlipidemia: A Review of Cellular and Metabolic Mechanisms. J. Cell. Physiol. 2018, 233, 141–152. [Google Scholar] [CrossRef]
- Nasra, S.; Shah, T.; Bhatt, M.; Chaudhari, R.; Bhatia, D.; Kumar, A. Reprogramming M1-to-M2 Phenotype to Alleviate Inflammation: Using Liposomal Curcumin as a Tool to Redefine Macrophage Functionality. ACS Appl. Bio Mater. 2023, 6, 2886–2897. [Google Scholar] [CrossRef]
- Wang, Y.; Smith, W.; Hao, D.; He, B.; Kong, L. M1 and M2 Macrophage Polarization and Potentially Therapeutic Naturally Occurring Compounds. Int. Immunopharmacol. 2019, 70, 459–466. [Google Scholar] [CrossRef]
- Chen, J.-W.; Kong, Z.-L.; Tsai, M.-L.; Lo, C.-Y.; Ho, C.-T.; Lai, C.-S. Tetrahydrocurcumin Ameliorates Free Fatty Acid-Induced Hepatic Steatosis and Improves Insulin Resistance in HepG2 Cells. J. Food Drug Anal. 2018, 26, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Zingg, J.-M.; Hasan, S.T.; Nakagawa, K.; Canepa, E.; Ricciarelli, R.; Villacorta, L.; Azzi, A.; Meydani, M. Modulation of CAMP Levels by High-Fat Diet and Curcumin and Regulatory Effects on CD36/FAT Scavenger Receptor/Fatty Acids Transporter Gene Expression. Biofactors 2017, 43, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.T.; Zingg, J.M.; Kwan, P.; Noble, T.; Smith, D.; Meydani, M. Curcumin Modulation of High Fat Diet-Induced Atherosclerosis and Steatohepatosis in LDL Receptor Deficient Mice. Atherosclerosis 2014, 232, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, L.J.; Walker, M.; Pattabiraman, M.; Zhong, H.A.; Luedtke, B.; Chandra, S. Novel Curcumin Analog (Cis-Trans Curcumin) as Ligand to Adenosine Receptors A(2A) and A(2B): Potential for Therapeutics. Pharmacol. Res. 2021, 165, 105410. [Google Scholar] [CrossRef]
- Balstad, T.R.; Carlsen, H.; Myhrstad, M.C.W.; Kolberg, M.; Reiersen, H.; Gilen, L.; Ebihara, K.; Paur, I.; Blomhoff, R. Coffee, Broccoli and Spices Are Strong Inducers of Electrophile Response Element-Dependent Transcription in Vitro and in Vivo—Studies in Electrophile Response Element Transgenic Mice. Mol. Nutr. Food Res. 2011, 55, 185–197. [Google Scholar] [CrossRef]
- Antony, B.; Merina, B.; Iyer, V.S.; Judy, N.; Lennertz, K.; Joyal, S. A Pilot Cross-Over Study to Evaluate Human Oral Bioavailability of BCM-95CG (Biocurcumax), A Novel Bioenhanced Preparation of Curcumin. Indian J. Pharm. Sci. 2008, 70, 445–449. [Google Scholar] [CrossRef]
- Gota, V.S.; Maru, G.B.; Soni, T.G.; Gandhi, T.R.; Kochar, N.; Agarwal, M.G. Safety and Pharmacokinetics of a Solid Lipid Curcumin Particle Formulation in Osteosarcoma Patients and Healthy Volunteers. J. Agric. Food Chem. 2010, 58, 2095–2099. [Google Scholar] [CrossRef]
- Sasaki, H.; Sunagawa, Y.; Takahashi, K.; Imaizumi, A.; Fukuda, H.; Hashimoto, T.; Wada, H.; Katanasaka, Y.; Kakeya, H.; Fujita, M.; et al. Innovative Preparation of Curcumin for Improved Oral Bioavailability. Biol. Pharm. Bull. 2011, 34, 660–665. [Google Scholar] [CrossRef]
- Cuomo, J.; Appendino, G.; Dern, A.S.; Schneider, E.; McKinnon, T.P.; Brown, M.J.; Togni, S.; Dixon, B.M. Comparative Absorption of a Standardized Curcuminoid Mixture and Its Lecithin Formulation. J. Nat. Prod. 2011, 74, 664–669. [Google Scholar] [CrossRef]
- Vitaglione, P.; Barone Lumaga, R.; Ferracane, R.; Radetsky, I.; Mennella, I.; Schettino, R.; Koder, S.; Shimoni, E.; Fogliano, V. Curcumin Bioavailability from Enriched Bread: The Effect of Microencapsulated Ingredients. J. Agric. Food Chem. 2012, 60, 3357–3366. [Google Scholar] [CrossRef]
- Schiborr, C.; Kocher, A.; Behnam, D.; Jandasek, J.; Toelstede, S.; Frank, J. The Oral Bioavailability of Curcumin from Micronized Powder and Liquid Micelles Is Significantly Increased in Healthy Humans and Differs between Sexes. Mol. Nutr. Food Res. 2014, 58, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Lowery, R.P.; Calvanese, A.V.; Joy, J.M.; Purpura, M.; Wilson, J.M. Comparative Absorption of Curcumin Formulations. Nutr. J. 2014, 13, 11. [Google Scholar] [CrossRef]
- Purpura, M.; Lowery, R.P.; Wilson, J.M.; Mannan, H.; Münch, G.; Razmovski-Naumovski, V. Analysis of Different Innovative Formulations of Curcumin for Improved Relative Oral Bioavailability in Human Subjects. Eur. J. Nutr. 2018, 57, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Lin, J.; Li, H.; Shen, Z.; Wang, Y.; Velkov, T.; Shen, J. The Natural Product Curcumin as an Antibacterial Agent: Current Achievements and Problems. Antioxidants 2022, 11, 459. [Google Scholar] [CrossRef]
- Saini, K.; Modgill, N.; Singh, K.K.; Kakkar, V. Tetrahydrocurcumin Lipid Nanoparticle Based Gel Promotes Penetration into Deeper Skin Layers and Alleviates Atopic Dermatitis in 2,4-Dinitrochlorobenzene (DNCB) Mouse Model. Nanomaterials 2022, 12, 636. [Google Scholar] [CrossRef]
- Kakkar, V.; Kaur, I.P.; Kaur, A.P.; Saini, K.; Singh, K.K. Topical Delivery of Tetrahydrocurcumin Lipid Nanoparticles Effectively Inhibits Skin Inflammation: In Vitro and in Vivo Study. Drug Dev. Ind. Pharm. 2018, 44, 1701–1712. [Google Scholar] [CrossRef]
- Zheng, D.; Huang, C.; Huang, H.; Zhao, Y.; Khan, M.R.U.; Zhao, H.; Huang, L. Antibacterial Mechanism of Curcumin: A Review. Chem. Biodivers. 2020, 17, e2000171. [Google Scholar] [CrossRef] [PubMed]
- Lade, H.; Paul, D.; Kweon, J.H. Combined Effects of Curcumin and (-)-Epigallocatechin Gallate on Inhibition of N-Acylhomoserine Lactone-Mediated Biofilm Formation in Wastewater Bacteria from Membrane Bioreactor. J. Microbiol. Biotechnol. 2015, 25, 1908–1919. [Google Scholar] [CrossRef]
- Dai, C.; Ciccotosto, G.D.; Cappai, R.; Tang, S.; Li, D.; Xie, S.; Xiao, X.; Velkov, T. Curcumin Attenuates Colistin-Induced Neurotoxicity in N2a Cells via Anti-Inflammatory Activity, Suppression of Oxidative Stress, and Apoptosis. Mol. Neurobiol. 2018, 55, 421–434. [Google Scholar] [CrossRef]
- Marathe, S.A.; Balakrishnan, A.; Negi, V.D.; Sakorey, D.; Chandra, N.; Chakravortty, D. Curcumin Reduces the Motility of Salmonella Enterica Serovar Typhimurium by Binding to the Flagella, Thereby Leading to Flagellar Fragility and Shedding. J. Bacteriol. 2016, 198, 1798–1811. [Google Scholar] [CrossRef]
- Marathe, S.A.; Kumar, R.; Ajitkumar, P.; Nagaraja, V.; Chakravortty, D. Curcumin Reduces the Antimicrobial Activity of Ciprofloxacin against Salmonella Typhimurium and Salmonella Typhi. J. Antimicrob. Chemother. 2013, 68, 139–152. [Google Scholar] [CrossRef]
- Zhao, X.; Drlica, K. Reactive Oxygen Species and the Bacterial Response to Lethal Stress. Curr. Opin. Microbiol. 2014, 21, 1–6. [Google Scholar] [CrossRef]
- Hettiarachchi, S.S.; Perera, Y.; Dunuweera, S.P.; Dunuweera, A.N.; Rajapakse, S.; Rajapakse, R.M.G. Comparison of Antibacterial Activity of Nanocurcumin with Bulk Curcumin. ACS Omega 2022, 7, 46494–46500. [Google Scholar] [CrossRef]
- Kali, A.; Bhuvaneshwar, D.; Charles, P.M.V.; Seetha, K.S. Antibacterial Synergy of Curcumin with Antibiotics against Biofilm Producing Clinical Bacterial Isolates. J. Basic Clin. Pharm. 2016, 7, 93–96. [Google Scholar] [CrossRef]
- Jadaun, V.; Prateeksha; Singh, B.R.; Paliya, B.S.; Upreti, D.K.; Rao, C.V.; Rawat, A.K.S.; Singh, B.N. Honey Enhances the Anti-Quorum Sensing Activity and Anti-Biofilm Potential of Curcumin. RSC Adv. 2015, 5, 71060–71070. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Jaggi, M.; Chauhan, S.C. Curcumin Nanomedicine: A Road to Cancer Therapeutics. Curr. Pharm. Des. 2013, 19, 1994–2010. [Google Scholar] [CrossRef] [PubMed]
- Jahagirdar, P.S.; Gupta, P.K.; Kulkarni, S.P.; Devarajan, P.V. Polymeric Curcumin Nanoparticles by a Facile in Situ Method for Macrophage Targeted Delivery. Bioeng. Transl. Med. 2019, 4, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Enayati, A.; Soghi, A.; Butler, A.E.; Rizzo, M.; Sahebkar, A. The Effect of Curcumin on the Gut-Brain Axis: Therapeutic Implications. J. Neurogastroenterol. Motil. 2023, 29, 409–418. [Google Scholar] [CrossRef]
- Pluta, R.; Januszewski, S.; Ułamek-kozioł, M. Mutual Two-Way Interactions of Curcumin and Gut Microbiota. Int. J. Mol. Sci. 2020, 21, 1055. [Google Scholar] [CrossRef]
- Jabczyk, M.; Nowak, J.; Hudzik, B.; Zubelewicz-Szkodzińska, B. Curcumin and Its Potential Impact on Microbiota. Nutrients 2021, 13, 2004. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Deb, L.; Prasad, S. Curcumin Differs from Tetrahydrocurcumin for Molecular Targets, Signaling Pathways and Cellular Responses. Molecules 2014, 20, 185–205. [Google Scholar] [CrossRef]
- Hassaninasab, A.; Hashimoto, Y.; Tomita-Yokotani, K.; Kobayashi, M. Discovery of the Curcumin Metabolic Pathway Involving a Unique Enzyme in an Intestinal Microorganism. Proc. Natl. Acad. Sci. USA 2011, 108, 6615–6620. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, M.; Huang, N.; Guan, F.; Luo, H.; Chen, L.; Wei, G.; Li, M.; Lin, Z.; Su, Z.; et al. Curcumin Alleviates High-Fat Diet-Induced Nonalcoholic Steatohepatitis via Improving Hepatic Endothelial Function with Microbial Biotransformation in Rats. J. Agric. Food Chem. 2023, 71, 10338–10348. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Kong, L.; Han, Y.; Zhang, S. Gut Microbiota Enhances the Chemosensitivity of Hepatocellular Carcinoma to 5-Fluorouracil in Vivo by Increasing Curcumin Bioavailability. Phytother. Res. 2021, 35, 5823–5837. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhai, Y.; Heng, X.; Che, F.Y.; Chen, W.; Sun, D.; Zhai, G. Oral Bioavailability of Curcumin: Problems and Advancements. J. Drug Target. 2016, 24, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Ji, H.-F. Intestinal Microbiota and Metabolic Diseases: Pharmacological Implications. Trends Pharmacol. Sci. 2016, 37, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Scazzocchio, B.; Minghetti, L.; D’archivio, M. Interaction between Gut Microbiota and Curcumin: A New Key of Understanding for the Health Effects of Curcumin. Nutrients 2020, 12, 2499. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Smart, J.D.; Pannala, A.S. Recent Developments in Formulation Design for Improving Oral Bioavailability of Curcumin: A Review. J. Drug Deliv. Sci. Technol. 2020, 60, 102082. [Google Scholar] [CrossRef]
- Wong, K.E.; Ngai, S.C.; Chan, K.-G.; Lee, L.-H.; Goh, B.-H.; Chuah, L.-H. Curcumin Nanoformulations for Colorectal Cancer: A Review. Front. Pharmacol. 2019, 10, 152. [Google Scholar] [CrossRef]
- Ohno, M.; Nishida, A.; Sugitani, Y.; Nishino, K.; Inatomi, O.; Sugimoto, M.; Kawahara, M.; Andoh, A. Nanoparticle Curcumin Ameliorates Experimental Colitis via Modulation of Gut Microbiota and Induction of Regulatory T Cells. PLoS ONE 2017, 12, e0185999. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Chiu, W.-C.; Chiu, Y.-S.; Li, T.; Sung, H.-C.; Hsiao, C.-Y. Supplementation of Nano-Bubble Curcumin Extract Improves Gut Microbiota Composition and Exercise Performance in Mice. Food Funct. 2020, 11, 3574–3584. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Zhuang, X.; Xiang, X.; Liu, Y.; Zhang, S.; Liu, C.; Barnes, S.; Grizzle, W.; Miller, D.; Zhang, H.-G. A Novel Nanoparticle Drug Delivery System: The Anti-Inflammatory Activity of Curcumin Is Enhanced When Encapsulated in Exosomes. Mol. Ther. 2010, 18, 1606–1614. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Han, Z.; Wu, Y.; Lu, X.; Tang, X.; Xiao, J.; Li, N. Enhancing Stability and Anti-Inflammatory Properties of Curcumin in Ulcerative Colitis Therapy Using Liposomes Mediated Colon-Specific Drug Delivery System. Food Chem. Toxicol. An Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2021, 151, 112123. [Google Scholar] [CrossRef]
- Beloqui, A.; Memvanga, P.B.; Coco, R.; Reimondez-Troitiño, S.; Alhouayek, M.; Muccioli, G.G.; Alonso, M.J.; Csaba, N.; de la Fuente, M.; Préat, V. A Comparative Study of Curcumin-Loaded Lipid-Based Nanocarriers in the Treatment of Inflammatory Bowel Disease. Colloids Surf. B. Biointerfaces 2016, 143, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Pandelidou, M.; Dimas, K.; Georgopoulos, A.; Hatziantoniou, S.; Demetzos, C. Preparation and Characterization of Lyophilised Egg PC Liposomes Incorporating Curcumin and Evaluation of Its Activity against Colorectal Cancer Cell Lines. J. Nanosci. Nanotechnol. 2011, 11, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.J.; Kalman, D.S. Curcumin: A Review of Its Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, J.; Ankola, D.D.; Beniwal, V.; Singh, D.; Kumar, M.N.V.R. Nanoparticle Encapsulation Improves Oral Bioavailability of Curcumin by at Least 9-Fold When Compared to Curcumin Administered with Piperine as Absorption Enhancer. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2009, 37, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, C.; Krishnan, K.; Manavalan, R.; Kathiresan, K. Preparation and Characterization of Curcumin-Piperine Dual Drug Loaded Nanoparticles. Asian Pac. J. Trop. Biomed. 2012, 2, 841–848. [Google Scholar] [CrossRef]
- Ahmad, S.; Hafeez, A. Formulation and Development of Curcumin-Piperine-Loaded S-SNEDDS for the Treatment of Alzheimer’s Disease. Mol. Neurobiol. 2023, 60, 1067–1082. [Google Scholar] [CrossRef]
- Dei Cas, M.; Ghidoni, R. Dietary Curcumin: Correlation between Bioavailability and Health Potential. Nutrients 2019, 11, 2147. [Google Scholar] [CrossRef]
- Ferguson, J.J.A.; Abbott, K.A.; Garg, M.L. Anti-Inflammatory Effects of Oral Supplementation with Curcumin: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutr. Rev. 2021, 79, 1043–1066. [Google Scholar] [CrossRef]
- Zeng, X.; Cai, D.; Zeng, Q.; Chen, Z.; Zhong, G.; Zhuo, J.; Gan, H.; Huang, X.; Zhao, Z.; Yao, N.; et al. Selective Reduction in the Expression of UGTs and SULTs, a Novel Mechanism by Which Piperine Enhances the Bioavailability of Curcumin in Rat. Biopharm. Drug Dispos. 2017, 38, 3–19. [Google Scholar] [CrossRef]
- Shi, L.; Xun, W.; Peng, W.; Hu, H.; Cao, T.; Hou, G. Effect of the Single and Combined Use of Curcumin and Piperine on Growth Performance, Intestinal Barrier Function, and Antioxidant Capacity of Weaned Wuzhishan Piglets. Front. Vet. Sci. 2020, 7, 418. [Google Scholar] [CrossRef]
- Bolat, Z.B.; Islek, Z.; Demir, B.N.; Yilmaz, E.N.; Sahin, F.; Ucisik, M.H. Curcumin- and Piperine-Loaded Emulsomes as Combinational Treatment Approach Enhance the Anticancer Activity of Curcumin on HCT116 Colorectal Cancer Model. Front. Bioeng. Biotechnol. 2020, 8, 50. [Google Scholar] [CrossRef]
- Wu, X.; Koh, G.Y.; Huang, Y.; Crott, J.W.; Bronson, R.T.; Mason, J.B. The Combination of Curcumin and Salsalate Is Superior to Either Agent Alone in Suppressing Pro-Cancerous Molecular Pathways and Colorectal Tumorigenesis in Obese Mice. Mol. Nutr. Food Res. 2019, 63, e1801097. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Pfalzer, A.C.; Koh, G.Y.; Tang, S.; Crott, J.W.; Thomas, M.J.; Meydani, M.; Mason, J.B. Curcumin and Salsalate Suppresses Colonic Inflammation and Procarcinogenic Signaling in High-Fat-Fed, Azoxymethane-Treated Mice. J. Agric. Food Chem. 2017, 65, 7200–7209. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Ueland, P.M.; Roper, J.; Koh, G.Y.; Liang, X.; Crott, J.W.; Yilmaz, Ö.H.; Bronson, R.T.; Mason, J.B. Combined Supplementation with Vitamin B-6 and Curcumin Is Superior to Either Agent Alone in Suppressing Obesity-Promoted Colorectal Tumorigenesis in Mice. J. Nutr. 2021, 151, 3678–3688. [Google Scholar] [CrossRef] [PubMed]
- Holder, G.M.; Plummer, J.L.; Ryan, A.J. The Metabolism and Excretion of Curcumin (1,7-Bis-(4-Hydroxy-3-Methoxyphenyl)-1,6-Heptadiene-3,5-Dione) in the Rat. Xenobiotica 1978, 8, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of Curcumin: Problems and Promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef]
- Ireson, C.; Orr, S.; Jones, D.J.; Verschoyle, R.; Lim, C.K.; Luo, J.L.; Howells, L.; Plummer, S.; Jukes, R.; Williams, M.; et al. Characterization of Metabolites of the Chemopreventive Agent Curcumin in Human and Rat Hepatocytes and in the Rat in Vivo, and Evaluation of Their Ability to Inhibit Phorbol Ester-Induced Prostaglandin E2 Production. Cancer Res. 2001, 61, 1058–1064. [Google Scholar] [PubMed]
- Metzler, M.; Pfeiffer, E.; Schulz, S.I.; Dempe, J.S. Curcumin Uptake and Metabolism. Biofactors 2013, 39, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Correa, M.; Shoskes, D.A.; Sanchez, P.; Zhao, R.; Hylind, L.M.; Wexner, S.D.; Giardiello, F.M. Combination Treatment with Curcumin and Quercetin of Adenomas in Familial Adenomatous Polyposis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2006, 4, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.P.; Salamone, E.; Goldin, B. Curcumin and Genistein, Plant Natural Products, Show Synergistic Inhibitory Effects on the Growth of Human Breast Cancer MCF-7 Cells Induced by Estrogenic Pesticides. Biochem. Biophys. Res. Commun. 1997, 233, 692–696. [Google Scholar] [CrossRef]
- Lukita-Atmadja, W.; Ito, Y.; Baker, G.L.; McCuskey, R.S. Effect of Curcuminoids as Anti-Inflammatory Agents on the Hepatic Microvascular Response to Endotoxin. Shock 2002, 17, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Jazayeri-Tehrani, S.A.; Rezayat, S.M.; Mansouri, S.; Qorbani, M.; Alavian, S.M.; Daneshi-Maskooni, M.; Hosseinzadeh-Attar, M.-J. Nano-Curcumin Improves Glucose Indices, Lipids, Inflammation, and Nesfatin in Overweight and Obese Patients with Non-Alcoholic Fatty Liver Disease (NAFLD): A Double-Blind Randomized Placebo-Controlled Clinical Trial. Nutr. Metab. 2019, 16, 8. [Google Scholar] [CrossRef]
- Ejaz, A.; Wu, D.; Kwan, P.; Meydani, M. Curcumin Inhibits Adipogenesis in 3T3-L1 Adipocytes and Angiogenesis and Obesity in C57/BL Mice. J. Nutr. 2009, 139, 919–925. [Google Scholar] [CrossRef]
- Zhao, D.; Pan, Y.; Yu, N.; Bai, Y.; Ma, R.; Mo, F.; Zuo, J.; Chen, B.; Jia, Q.; Zhang, D.; et al. Curcumin Improves Adipocytes Browning and Mitochondrial Function in 3T3-L1 Cells and Obese Rodent Model. R. Soc. Open Sci. 2021, 8, 200974. [Google Scholar] [CrossRef]
- Miyazawa, T.; Nakagawa, K.; Kim, S.H.; Thomas, M.J.; Paul, L.; Zingg, J.-M.; Dolnikowski, G.G.; Roberts, S.B.; Kimura, F.; Miyazawa, T.; et al. Curcumin and Piperine Supplementation of Obese Mice under Caloric Restriction Modulates Body Fat and Interleukin-1β. Nutr. Metab. 2018, 15, 12. [Google Scholar] [CrossRef]
- Bertoncini-Silva, C.; Fassini, P.G.; Carlos, D.; de Paula, N.A.; Ramalho, L.N.Z.; Rodrigues Giuliani, M.; Pereira, Í.S.; Guimarães, J.B.; Suen, V.M.M. The Dose-Dependent Effect of Curcumin Supplementation on Inflammatory Response and Gut Microbiota Profile in High-Fat Fed C57BL/6 Mice. Mol. Nutr. Food Res. 2023, 67, e2300378. [Google Scholar] [CrossRef]
- Di Pierro, F.; Bressan, A.; Ranaldi, D.; Rapacioli, G.; Giacomelli, L.; Bertuccioli, A. Potential Role of Bioavailable Curcumin in Weight Loss and Omental Adipose Tissue Decrease: Preliminary Data of a Randomized, Controlled Trial in Overweight People with Metabolic Syndrome. Preliminary Study. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4195–4202. [Google Scholar]
- Surma, S.; Sahebkar, A.; Urbański, J.; Penson, P.E.; Banach, M. Curcumin—The Nutraceutical With Pleiotropic Effects? Which Cardiometabolic Subjects Might Benefit the Most? Front. Nutr. 2022, 9, 865497. [Google Scholar] [CrossRef] [PubMed]
- Keihanian, F.; Saeidinia, A.; Bagheri, R.K.; Johnston, T.P.; Sahebkar, A. Curcumin, Hemostasis, Thrombosis, and Coagulation. J. Cell. Physiol. 2018, 233, 4497–4511. [Google Scholar] [CrossRef] [PubMed]
- Singh, L.; Sharma, S.; Xu, S.; Tewari, D.; Fang, J. Curcumin as a Natural Remedy for Atherosclerosis: A Pharmacological Review. Molecules 2021, 26, 4036. [Google Scholar] [CrossRef] [PubMed]
- Li, K.-X.; Wang, Z.-C.; Machuki, J.O.; Li, M.-Z.; Wu, Y.-J.; Niu, M.-K.; Yu, K.-Y.; Lu, Q.-B.; Sun, H.-J. Benefits of Curcumin in the Vasculature: A Therapeutic Candidate for Vascular Remodeling in Arterial Hypertension and Pulmonary Arterial Hypertension? Front. Physiol. 2022, 13, 848867. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Jin, J.; Pu, F.; Bai, Y.; Chen, Y.; Li, Y.; Wang, X. Cardioprotective Effects of Curcumin against Myocardial I/R Injury: A Systematic Review and Meta-Analysis of Preclinical and Clinical Studies. Front. Pharmacol. 2023, 14, 1111459. [Google Scholar] [CrossRef]
- Zhang, H.A.; Kitts, D.D. Turmeric and Its Bioactive Constituents Trigger Cell Signaling Mechanisms That Protect against Diabetes and Cardiovascular Diseases. Mol. Cell. Biochem. 2021, 476, 3785–3814. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Rana, S.; Banerjee, D.; Mitra, A.; Datta, R.; Naskar, S.; Sarkar, S. Improved Bioavailability of Targeted Curcumin Delivery Efficiently Regressed Cardiac Hypertrophy by Modulating Apoptotic Load within Cardiac Microenvironment. Toxicol. Appl. Pharmacol. 2016, 290, 54–65. [Google Scholar] [CrossRef]
- Shome, S.; Talukdar, A.D.; Choudhury, M.D.; Bhattacharya, M.K.; Upadhyaya, H. Curcumin as Potential Therapeutic Natural Product: A Nanobiotechnological Perspective. J. Pharm. Pharmacol. 2016, 68, 1481–1500. [Google Scholar] [CrossRef]
- Czyzynska-Cichon, I.; Janik-Hazuka, M.; Szafraniec-Szczęsny, J.; Jasinski, K.; Węglarz, W.P.; Zapotoczny, S.; Chlopicki, S. Low Dose Curcumin Administered in Hyaluronic Acid-Based Nanocapsules Induces Hypotensive Effect in Hypertensive Rats. Int. J. Nanomedicine 2021, 16, 1377–1390. [Google Scholar] [CrossRef]
- Preez, R.D.; Pahl, J.; Arora, M.; Kumar, M.N.V.R.; Brown, L.; Panchal, S.K. Low-Dose Curcumin Nanoparticles Normalise Blood Pressure in Male Wistar Rats with Diet-Induced Metabolic Syndrome. Nutrients 2019, 11, 1542. [Google Scholar] [CrossRef]
- Rachmawati, H.; Soraya, I.S.; Kurniati, N.F.; Rahma, A. In Vitro Study on Antihypertensive and Antihypercholesterolemic Effects of a Curcumin Nanoemulsion. Sci. Pharm. 2016, 84, 131–140. [Google Scholar] [CrossRef]
- Martinez, K.; Smith, A.; Ye, D.; Zhou, W.; Tester, D.J.; Ackerman, M.J. Curcumin, a Dietary Natural Supplement, Prolongs the Action Potential Duration of KCNE1-D85N-Induced Pluripotent Stem Cell-Derived Cardiomyocytes. Hear. Rhythm 2023, 20, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Soltani, D.; Azizi, B.; Rahimi, R.; Talasaz, A.H.; Rezaeizadeh, H.; Vasheghani-Farahani, A. Mechanism-Based Targeting of Cardiac Arrhythmias by Phytochemicals and Medicinal Herbs: A Comprehensive Review of Preclinical and Clinical Evidence. Front. Cardiovasc. Med. 2022, 9, 990063. [Google Scholar] [CrossRef]
- Yue, H.; Zhao, X.; Liang, W.; Qin, X.; Bian, L.; He, K.; Wu, Z. Curcumin, Novel Application in Reversing Myocardial Fibrosis in the Treatment for Atrial Fibrillation from the Perspective of Transcriptomics in Rat Model. Biomed. Pharmacother. 2022, 146, 112522. [Google Scholar] [CrossRef]
- Hu, C.-W.; Sheng, Y.; Zhang, Q.; Liu, H.-B.; Xie, X.; Ma, W.-C.; Huo, R.; Dong, D.-L. Curcumin Inhibits HERG Potassium Channels in Vitro. Toxicol. Lett. 2012, 208, 192–196. [Google Scholar] [CrossRef]
- Barangi, S.; Hayes, A.W.; Karimi, G. The More Effective Treatment of Atrial Fibrillation Applying the Natural Compounds; as NADPH Oxidase and Ion Channel Inhibitors. Crit. Rev. Food Sci. Nutr. 2018, 58, 1230–1241. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, A.P.; Mukerjee, A.; Helson, L.; Vishwanatha, J.K. Mitigating Prolonged QT Interval in Cancer Nanodrug Development for Accelerated Clinical Translation. J. Nanobiotechnology 2013, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Nirmala, C.; Puvanakrishnan, R. Protective Role of Curcumin against Isoproterenol Induced Myocardial Infarction in Rats. Mol. Cell. Biochem. 1996, 159, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Nirmala, C.; Puvanakrishnan, R. Effect of Curcumin on Certain Lysosomal Hydrolases in Isoproterenol-Induced Myocardial Infarction in Rats. Biochem. Pharmacol. 1996, 51, 47–51. [Google Scholar] [CrossRef]
- Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Râjnoveanu, R.-M.; Bolboacă, S.D. Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules 2019, 24, 2802. [Google Scholar] [CrossRef]
- Nabofa, W.E.E.; Alashe, O.O.; Oyeyemi, O.T.; Attah, A.F.; Oyagbemi, A.A.; Omobowale, T.O.; Adedapo, A.A.; Alada, A.R.A. Cardioprotective Effects of Curcumin-Nisin Based Poly Lactic Acid Nanoparticle on Myocardial Infarction in Guinea Pigs. Sci. Rep. 2018, 8, 16649. [Google Scholar] [CrossRef] [PubMed]
- Brosková, Z.; Drábiková, K.; Sotníková, R.; Fialová, S.; Knezl, V. Effect of Plant Polyphenols on Ischemia-Reperfusion Injury of the Isolated Rat Heart and Vessels. Phytother. Res. 2013, 27, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Duan, W.; Lin, Y.; Yi, W.; Liang, Z.; Yan, J.; Wang, N.; Deng, C.; Zhang, S.; Li, Y.; et al. SIRT1 Activation by Curcumin Pretreatment Attenuates Mitochondrial Oxidative Damage Induced by Myocardial Ischemia Reperfusion Injury. Free Radic. Biol. Med. 2013, 65, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, C.; Becatti, M.; Pensalfini, A.; Cecchi, C.; Lanzilao, L.; Donzelli, G.; Nassi, N.; Giannini, L.; Borchi, E.; Nassi, P. Curcumin Protects Cardiac Cells against Ischemia-Reperfusion Injury: Effects on Oxidative Stress, NF-KappaB, and JNK Pathways. Free Radic. Biol. Med. 2008, 45, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.-P.; Wang, Z.-F.; Tootle, S.; Philip, T.; Zhao, Z.-Q. Curcumin Promotes Cardiac Repair and Ameliorates Cardiac Dysfunction Following Myocardial Infarction. Br. J. Pharmacol. 2012, 167, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Duan, W.; Yang, Y.; Yan, J.; Yu, S.; Liu, J.; Zhou, J.; Zhang, J.; Jin, Z.; Yi, D. The Effects of Curcumin Post-Treatment against Myocardial Ischemia and Reperfusion by Activation of the JAK2/STAT3 Signaling Pathway. Basic Res. Cardiol. 2012, 107, 263. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Ye, B.; Dai, Z.; Wu, X.; Lu, Z.; Shan, P.; Huang, W. Curcumin Inhibits Autophagy and Apoptosis in Hypoxia/Reoxygenation-Induced Myocytes. Mol. Med. Rep. 2015, 11, 4678–4684. [Google Scholar] [CrossRef]
- Hardy, N.; Viola, H.M.; Johnstone, V.P.A.; Clemons, T.D.; Cserne Szappanos, H.; Singh, R.; Smith, N.M.; Iyer, K.S.; Hool, L.C. Nanoparticle-Mediated Dual Delivery of an Antioxidant and a Peptide against the L-Type Ca2+ Channel Enables Simultaneous Reduction of Cardiac Ischemia-Reperfusion Injury. ACS Nano 2015, 9, 279–289. [Google Scholar] [CrossRef]
- Aslanabadi, N.; Entezari-Maleki, T.; Rezaee, H.; Jafarzadeh, H.R.; Vahedpour, R. Curcumin for the Prevention of Myocardial Injury Following Elective Percutaneous Coronary Intervention; a Pilot Randomized Clinical Trial. Eur. J. Pharmacol. 2019, 858, 172471. [Google Scholar] [CrossRef]
- Phrommintikul, A.; Chanchai, R.; Wongcharoen, W. Effects of Curcuminoids on Myocardial Injury After Percutaneous Coronary Intervention. J. Med. Food 2019, 22, 680–684. [Google Scholar] [CrossRef]
- Wongcharoen, W.; Jai-Aue, S.; Phrommintikul, A.; Nawarawong, W.; Woragidpoonpol, S.; Tepsuwan, T.; Sukonthasarn, A.; Apaijai, N.; Chattipakorn, N. Effects of Curcuminoids on Frequency of Acute Myocardial Infarction after Coronary Artery Bypass Grafting. Am. J. Cardiol. 2012, 110, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Helli, B.; Gerami, H.; Kavianpour, M.; Heybar, H.; Hosseini, S.K.; Haghighian, H.K. Curcumin Nanomicelle Improves Lipid Profile, Stress Oxidative Factors and Inflammatory Markers in Patients Undergoing Coronary Elective Angioplasty; A Randomized Clinical Trial. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 2090–2098. [Google Scholar] [CrossRef] [PubMed]
- Dastani, M.; Rahimi, H.R.; Askari, V.R.; Jaafari, M.R.; Jarahi, L.; Yadollahi, A.; Rahimi, V.B. Three Months of Combination Therapy with Nano-Curcumin Reduces the Inflammation and Lipoprotein (a) in Type 2 Diabetic Patients with Mild to Moderate Coronary Artery Disease: Evidence of a Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. Biofactors 2023, 49, 108–118. [Google Scholar] [CrossRef]
- Vafadar Afshar, G.; Rasmi, Y.; Yaghmaei, P.; Khadem-Ansari, M.-H.; Makhdomii, K.; Rasooli, J. The Effects of Nano-Curcumin Supplementation on Serum Level of Hs-CRP, Adhesion Molecules, and Lipid Profiles in Hemodialysis Patients, A Randomized Controlled Clinical Trial. Iran. J. Kidney Dis. 2020, 14, 52–61. [Google Scholar] [PubMed]
- Mirzabeigi, P.; Mohammadpour, A.H.; Salarifar, M.; Gholami, K.; Mojtahedzadeh, M.; Javadi, M.R. The Effect of Curcumin on Some of Traditional and Non-Traditional Cardiovascular Risk Factors: A Pilot Randomized, Double-Blind, Placebo-Controlled Trial. Iran. J. Pharm. Res. IJPR 2015, 14, 479–486. [Google Scholar] [PubMed]
- Kannan, R.G.; Abhilash, M.B.; Dinesh, K.; Syam, D.S.; Balu, M.; Sibi, I.; Krishnakumar, I.M. Brain Regional Pharmacokinetics Following the Oral Administration of Curcumagalactomannosides and Its Relation to Cognitive Function. Nutr. Neurosci. 2022, 25, 1928–1939. [Google Scholar] [CrossRef] [PubMed]
- Voulgaropoulou, S.D.; van Amelsvoort, T.A.M.J.; Prickaerts, J.; Vingerhoets, C. The Effect of Curcumin on Cognition in Alzheimer’s Disease and Healthy Aging: A Systematic Review of Pre-Clinical and Clinical Studies. Brain Res. 2019, 1725, 146476. [Google Scholar] [CrossRef]
- Yu, Y.; Shen, Q.; Lai, Y.; Park, S.Y.; Ou, X.; Lin, D.; Jin, M.; Zhang, W. Anti-Inflammatory Effects of Curcumin in Microglial Cells. Front. Pharmacol. 2018, 9, 386. [Google Scholar] [CrossRef]
- Khanna, A.; Das, S.S.; Kannan, R.; Swick, A.G.; Matthewman, C.; Maliakel, B.; Ittiyavirah, S.P.; Krishnakumar, I.M. The Effects of Oral Administration of Curcumin-Galactomannan Complex on Brain Waves Are Consistent with Brain Penetration: A Randomized, Double-Blinded, Placebo-Controlled Pilot Study. Nutr. Neurosci. 2022, 25, 1240–1249. [Google Scholar] [CrossRef]
- Pandaran Sudheeran, S.; Jacob, D.; Natinga Mulakal, J.; Gopinathan Nair, G.; Maliakel, A.; Maliakel, B.; Kuttan, R.; Im, K. Safety, Tolerance, and Enhanced Efficacy of a Bioavailable Formulation of Curcumin With Fenugreek Dietary Fiber on Occupational Stress: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J. Clin. Psychopharmacol. 2016, 36, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Xiang, X.; Grizzle, W.; Sun, D.; Zhang, S.; Axtell, R.C.; Ju, S.; Mu, J.; Zhang, L.; Steinman, L.; et al. Treatment of Brain Inflammatory Diseases by Delivering Exosome Encapsulated Anti-Inflammatory Drugs from the Nasal Region to the Brain. Mol. Ther. 2011, 19, 1769–1779. [Google Scholar] [CrossRef]
- He, R.; Jiang, Y.; Shi, Y.; Liang, J.; Zhao, L. Curcumin-Laden Exosomes Target Ischemic Brain Tissue and Alleviate Cerebral Ischemia-Reperfusion Injury by Inhibiting ROS-Mediated Mitochondrial Apoptosis. Mater. Sci. Eng. C. Mater. Biol. Appl. 2020, 117, 111314. [Google Scholar] [CrossRef]
- Sokolik, V. Effect of Curcumin Liposomal Form on Angiotensin Converting Activity, Cytokines And Cognitive Characteristics of The Rats With Alzheimer’s Disease Model. Biotechnol. Acta 2015, 8, 48–55. [Google Scholar] [CrossRef]
- Hardy, J.; Allsop, D. Amyloid Deposition as the Central Event in the Aetiology of Alzheimer’s Disease. Trends Pharmacol. Sci. 1991, 12, 383–388. [Google Scholar] [CrossRef]
- Di Martino, R.M.C.; De Simone, A.; Andrisano, V.; Bisignano, P.; Bisi, A.; Gobbi, S.; Rampa, A.; Fato, R.; Bergamini, C.; Perez, D.I.; et al. Versatility of the Curcumin Scaffold: Discovery of Potent and Balanced Dual BACE-1 and GSK-3β Inhibitors. J. Med. Chem. 2016, 59, 531–544. [Google Scholar] [CrossRef]
- Zheng, K.; Dai, X.; Xiao, N.; Wu, X.; Wei, Z.; Fang, W.; Zhu, Y.; Zhang, J.; Chen, X. Curcumin Ameliorates Memory Decline via Inhibiting BACE1 Expression and β-Amyloid Pathology in 5×FAD Transgenic Mice. Mol. Neurobiol. 2017, 54, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Z.; Hongmei, Z.; Lu, S.; Yu, L. Curcumin Mediates Presenilin-1 Activity to Reduce β-Amyloid Production in a Model of Alzheimer’s Disease. Pharmacol. Rep. 2011, 63, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Montalto, G.; Ricciarelli, R. Tau, Tau Kinases, and Tauopathies: An Updated Overview. Biofactors 2023, 49, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Zeng, Q.; Mitchell, E.S.; Xiu, J.; Duan, Y.; Li, C.; Tiwari, J.K.; Hu, Y.; Cao, X.; Zhao, Z. Curcumin Enhances Neurogenesis and Cognition in Aged Rats: Implications for Transcriptional Interactions Related to Growth and Synaptic Plasticity. PLoS ONE 2012, 7, e31211. [Google Scholar] [CrossRef]
- Conboy, L.; Foley, A.G.; O’Boyle, N.M.; Lawlor, M.; Gallagher, H.C.; Murphy, K.J.; Regan, C.M. Curcumin-Induced Degradation of PKC Delta Is Associated with Enhanced Dentate NCAM PSA Expression and Spatial Learning in Adult and Aged Wistar Rats. Biochem. Pharmacol. 2009, 77, 1254–1265. [Google Scholar] [CrossRef] [PubMed]
- Baum, L.; Lam, C.W.K.; Cheung, S.K.-K.; Kwok, T.; Lui, V.; Tsoh, J.; Lam, L.; Leung, V.; Hui, E.; Ng, C.; et al. Six-Month Randomized, Placebo-Controlled, Double-Blind, Pilot Clinical Trial of Curcumin in Patients with Alzheimer Disease. J. Clin. Psychopharmacol. 2008, 28, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Ringman, J.M.; Frautschy, S.A.; Teng, E.; Begum, A.N.; Bardens, J.; Beigi, M.; Gylys, K.H.; Badmaev, V.; Heath, D.D.; Apostolova, L.G.; et al. Oral Curcumin for Alzheimer’s Disease: Tolerability and Efficacy in a 24-Week Randomized, Double Blind, Placebo-Controlled Study. Alzheimers. Res. Ther. 2012, 4, 43. [Google Scholar] [CrossRef] [PubMed]
- Small, G.W.; Siddarth, P.; Li, Z.; Miller, K.J.; Ercoli, L.; Emerson, N.D.; Martinez, J.; Wong, K.-P.; Liu, J.; Merrill, D.A.; et al. Memory and Brain Amyloid and Tau Effects of a Bioavailable Form of Curcumin in Non-Demented Adults: A Double-Blind, Placebo-Controlled 18-Month Trial. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2018, 26, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Bengmark, S. Curcumin, an Atoxic Antioxidant and Natural NFkappaB, Cyclooxygenase-2, Lipooxygenase, and Inducible Nitric Oxide Synthase Inhibitor: A Shield against Acute and Chronic Diseases. JPEN. J. Parenter. Enteral Nutr. 2006, 30, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Chainani-Wu, N. Safety and Anti-Inflammatory Activity of Curcumin: A Component of Tumeric (Curcuma Longa). J. Altern. Complement. Med. 2003, 9, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Ombredane, A.S.; Silva, V.R.P.; Andrade, L.R.; Pinheiro, W.O.; Simonelly, M.; Oliveira, J.V.; Pinheiro, A.C.; Gonçalves, G.F.; Felice, G.J.; Garcia, M.P.; et al. In Vivo Efficacy and Toxicity of Curcumin Nanoparticles in Breast Cancer Treatment: A Systematic Review. Front. Oncol. 2021, 11, 612903. [Google Scholar] [CrossRef] [PubMed]
- Armandeh, M.; Bameri, B.; Samadi, M.; Heidari, S.; Foroumadi, R.; Abdollahi, M. A Systematic Review of Nonclinical Studies on the Effect of Curcumin in Chemotherapy- Induced Cardiotoxicity. Curr. Pharm. Des. 2022, 28, 1843–1853. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.J.; Cote, B.; Alani, A.W.; Rao, D.A. Polymeric Micellar Co-Delivery of Resveratrol and Curcumin to Mitigate in Vitro Doxorubicin-Induced Cardiotoxicity. J. Pharm. Sci. 2014, 103, 2315–2322. [Google Scholar] [CrossRef]
- Moutabian, H.; Ghahramani-Asl, R.; Mortezazadeh, T.; Laripour, R.; Narmani, A.; Zamani, H.; Ataei, G.; Bagheri, H.; Farhood, B.; Sathyapalan, T.; et al. The Cardioprotective Effects of Nano-Curcumin against Doxorubicin-Induced Cardiotoxicity: A Systematic Review. Biofactors 2022, 48, 597–610. [Google Scholar] [CrossRef]
- Mosa, I.F.; Abd, H.H.; Abuzreda, A.; Yousif, A.B.; Assaf, N. Chitosan and Curcumin Nanoformulations against Potential Cardiac Risks Associated with Hydroxyapatite Nanoparticles in Wistar Male Rats. Int. J. Biomater. 2021, 2021, 3394348. [Google Scholar] [CrossRef]
- Akbari, S.; Kariznavi, E.; Jannati, M.; Elyasi, S.; Tayarani-Najaran, Z. Curcumin as a preventive or therapeutic measure for chemotherapy and radiotherapy induced adverse reaction: A comprehensive review. Food Chem. Toxicol. 2020, 145, 111699. [Google Scholar] [CrossRef] [PubMed]

| Method of Administration | Dose | Time | Levels of Curcumin | Local | Model | Reference |
|---|---|---|---|---|---|---|
| Oral | 0.1 g/kg | 1 h later | 0.22 µg/mL | Plasma | Mice | [12] |
| Oral | 0.1 g/kg | 6 h later | 5 ng/mL | Plasma | Mice | |
| Oral | 340 mg/kg | 2 h later | 16.1 ng/mL | Plasma | Rat | [16] |
| Oral | 340 mg/kg | 2 h later | 1.4 mg/g | Intestinal mucosa | Rat | [16] |
| Oral | 1.2 g/kg | - | 0–12 nM | Plasma | Rat | [20] |
| Oral | 1.2 g/kg | - | 0.2–1.8 µmol/g | Colon mucosa | Rat | [20] |
| Oral | 2 g/kg | Within 0.83 h | 1.35 µg/mL | Serum | Rat | [17] |
| Oral | 2 g/kg | 1 h later | 1.00 µg/mL | Serum | Rat | [9,17] |
| Oral | 2 g/kg | 1 h later | 0.006 µg/mL | Serum | Human | [17] |
| Oral | 2.35 g/day | 40 h later | 127.8 nmol/g | Intestinal mucosa | Human | [28] |
| Oral | 3.6 g/day | 1 h later | 11.1 nmol/L | Plasma | Human | [22] |
| Oral | 3600 mg/day | 38 min later | 12.7 nmol/g | Colorectum | Human | [27] |
| Oral | 4 g/day | Within 12 h | 0.51 µM | Serum | Human | [21] |
| Oral | 6 g/day | Within 12 h | 0.63 µM | Serum | Human | [21] |
| Oral | 8 g/day | Within 12 h | 1.77 µM | Serum | Human | [21] |
| Oral | Up to 8 g/day | After 1, 2, or 4 h | Remained undetectable | Serum | Human | [18,19] |
| Oral | 10 g/day | After 1, 2, or 4 h | 50.5 ng/mL | Serum | Human | [18,19] |
| Oral | 12 g/day | After 1, 2, or 4 h | 51.2 ng/mL | Serum | Human | [18,19] |
| Intraperitoneal | 0.1 g/kg | 15 min later | 2.25 µg/mL | Plasma | Mice | [12] |
| Intraperitoneal | 0.1 g/kg | 1 h later | 177.04 µg/g | Intestine | Mice | [12] |
| Intraperitoneal | 100 mg/kg | 2 h later | 200 nmol/g | Intestinal mucosa | Mice | [26] |
| - | 5 µM | 15 min later | 0.013 µM | Caco-2 cells | In vitro | [29] |
| - | 5 µM | 60 min later | 0.055 µM | Caco-2 cells | In vitro | |
| - | 5 µM | 4 h later | 0.031 µM | Caco-2 cells | In vitro | |
| - | 10 µM | 10 min later | 1313 pmol/2.0 × 106 | THP-1 monocytes and macrophages | In vitro | [30] |
| 2 h later | 2029 pmol/2.0 × 106 | |||||
| 24 h later | 401 pmol/2.0 × 106 | |||||
| - | 25 µM | 1–9 h later | 1840–5650 pmol/2.5 × 106 | HepG2 cells | In vitro | [11] |
| Applications/Target Tissues | Curcumin Nanoformulations (Examples) |
|---|---|
| Antimicrobial activities (viruses, bacteria, fungi) | Colloidal (micelles, liposomes, nanoemulsions, cyclodextrins, chitosan, and polymeric nanoparticles) metallic and mesoporous particles, graphene, quantum dots, and hybrid nanosystems such as films and hydrogels [35]. |
| Wound healing | Nanofibers, nanoparticles, nanomicelles, nanofibers, films, composites, scaffolds, gels and hydrogels, sponges, and aerogels [36]. |
| Inflammatory and oxidative stress-related diseases | Liposomes, polymeric micelles, Metal organic frameworks (MOFs), inorganic nanocarriers, polymeric nanoparticles, proteins, and nanofibers [34,37,38]. |
| Gastrointestinal | Solid dispersions, nano/microparticles, polymeric micelles, nanosuspensions, lipid-based nanocarriers, cyclodextrins, conjugates, and polymorphs [37]. |
| Liver | Phosphatidylserine (PS)-modified nanostructured lipid carriers (mNLCs), Gold nanoparticles (AuNPs), Cur hyaluronic acid–polylactide nanoparticles (HPNPs), Silver nanoparticles (AgNPs), and simple nano curcumin (nanoCUR) [39,40]. |
| Adipose tissue | Curcuminoid nanomicelles for adipose-derived mesenchymal stem cells [41]. |
| Cardiovascular | Curumin-Bioperin PLGA NPs (type of nanoformulation), nano curcumin, nanoparticles, and lipososmes [39,42,43]. |
| Lung | Curcumin-loaded phospholipid vesicles, polymer glycerosomes, and liposomal formulations [38,40]. |
| Brain | Curcumin-loaded PLGA nanoparticles (C-NPs) [44]. |
| Cancer (e.g., breast) | Curcumin and resveratrol in liposomes, polymeric micelles and phospholipid complexes, polymeric nanoparticles, dendrimers, adjuvants, solid lipid nanoparticles, nanosponges, nanoemulsions, and nanogels [45,46]. |
| Mitochondria | Mitochondria-targeted polymeric nanoparticle (NP) system [47]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertoncini-Silva, C.; Vlad, A.; Ricciarelli, R.; Giacomo Fassini, P.; Suen, V.M.M.; Zingg, J.-M. Enhancing the Bioavailability and Bioactivity of Curcumin for Disease Prevention and Treatment. Antioxidants 2024, 13, 331. https://doi.org/10.3390/antiox13030331
Bertoncini-Silva C, Vlad A, Ricciarelli R, Giacomo Fassini P, Suen VMM, Zingg J-M. Enhancing the Bioavailability and Bioactivity of Curcumin for Disease Prevention and Treatment. Antioxidants. 2024; 13(3):331. https://doi.org/10.3390/antiox13030331
Chicago/Turabian StyleBertoncini-Silva, Caroline, Adelina Vlad, Roberta Ricciarelli, Priscila Giacomo Fassini, Vivian Marques Miguel Suen, and Jean-Marc Zingg. 2024. "Enhancing the Bioavailability and Bioactivity of Curcumin for Disease Prevention and Treatment" Antioxidants 13, no. 3: 331. https://doi.org/10.3390/antiox13030331
APA StyleBertoncini-Silva, C., Vlad, A., Ricciarelli, R., Giacomo Fassini, P., Suen, V. M. M., & Zingg, J.-M. (2024). Enhancing the Bioavailability and Bioactivity of Curcumin for Disease Prevention and Treatment. Antioxidants, 13(3), 331. https://doi.org/10.3390/antiox13030331