
The Efficacy and Safety of GF101 and Its Antioxidant Effect on In Vitro Fertilization Outcomes: A Double-Blind, Non-Inferiority, Randomized, Controlled Trial with Coenzyme Q10

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design and Participants
2.2. Experimental Procedures
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographic Characteristics
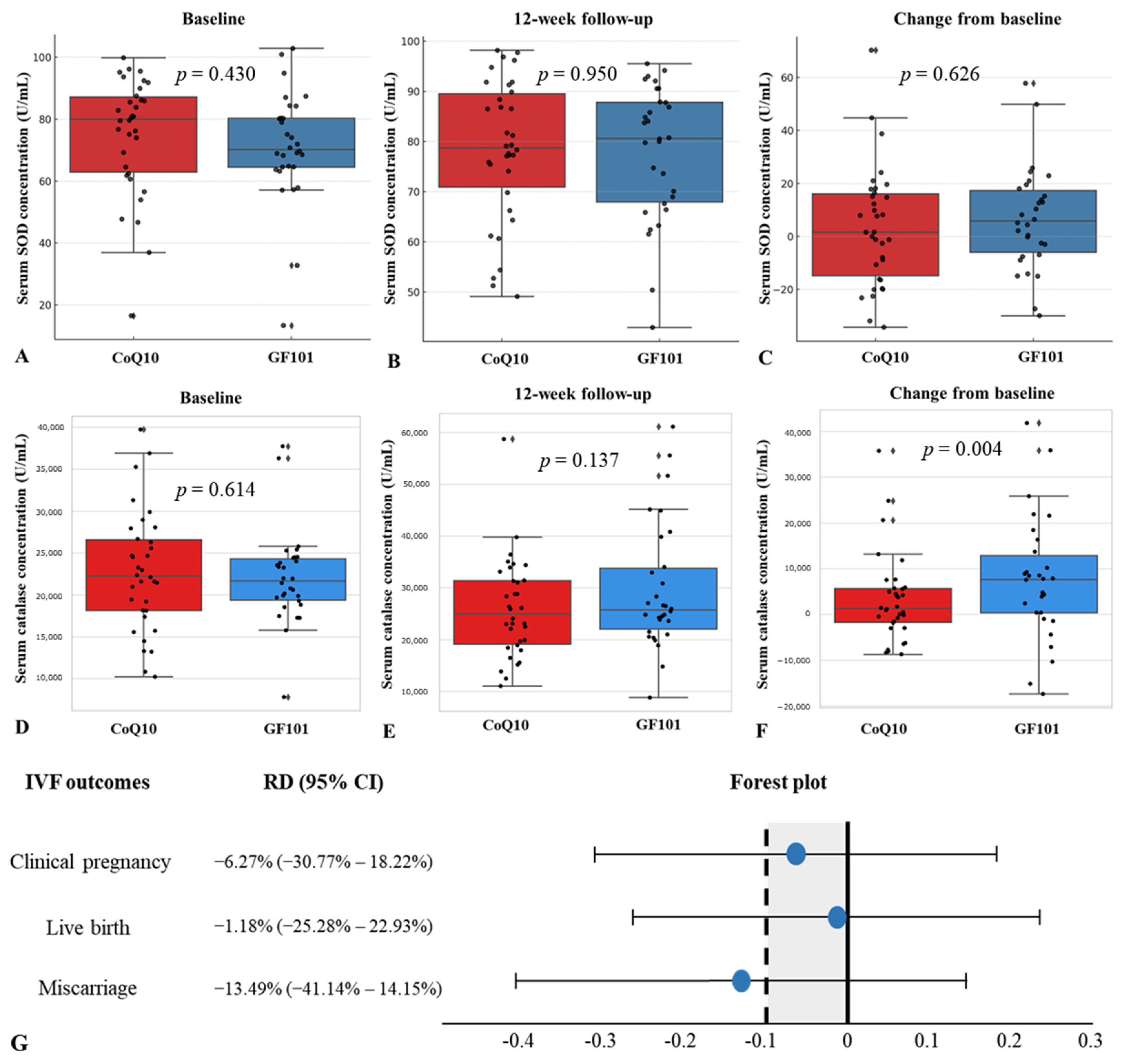
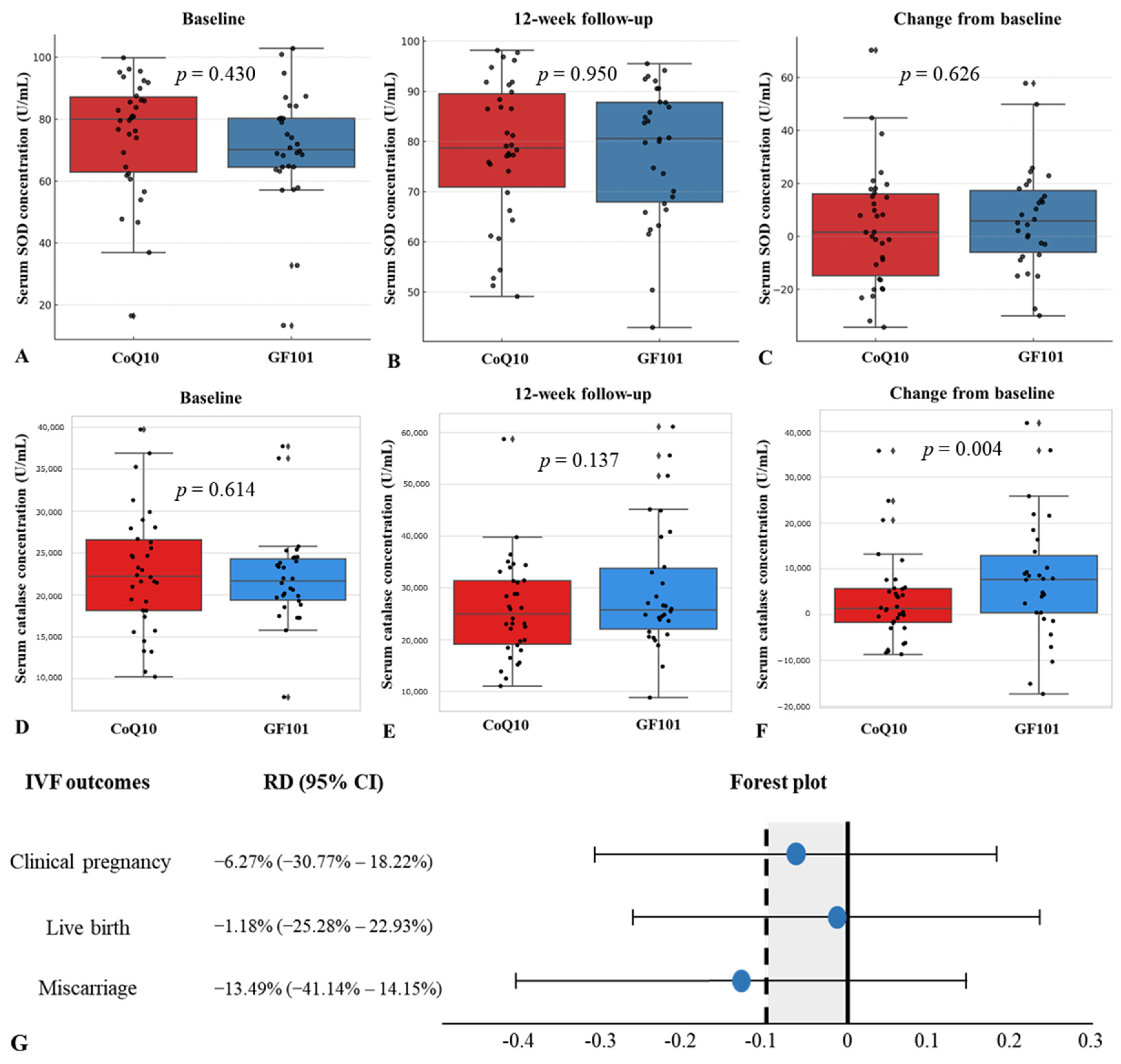
3.2. Serum Oxidative Stress Markers and IVF Outcomes
3.3. FF Oxidative Stress Markers, Oocyte Maturation, and Lipid Profiles
3.4. Safety Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodríguez-Varela, C.; Labarta, E. Does Coenzyme Q10 Supplementation Improve Human Oocyte Quality? Int. J. Mol. Sci. 2021, 22, 9541. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Lu, Y.; Zhang, M.; Miao, Y.; Zhou, C.; Cui, Z.; Xiong, B. Melatonin improves the fertilization ability of post-ovulatory aged mouse oocytes by stabilizing ovastacin and Juno to promote sperm binding and fusion. Hum. Reprod. 2017, 32, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, M.L.; Stein, P.; Carvacho, I.; Krapp, C.; Ardestani, G.; Mehregan, A.; Umbach, D.M.; Bartolomei, M.S.; Fissore, R.A.; Williams, C.J. TRPM7 and CaV3.2 channels mediate Ca2+ influx required for egg activation at fertilization. Proc. Natl. Acad. Sci. USA 2018, 115, E10370–E10378. [Google Scholar] [CrossRef] [PubMed]
- Perkins, A.T.; Das, T.M.; Panzera, L.C.; Bickel, S.E. Oxidative stress in oocytes during midprophase induces premature loss of cohesion and chromosome segregation errors. Proc. Natl. Acad. Sci. USA 2016, 113, E6823–E6830. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tang, J.; Wang, L.; Tan, F.; Song, H.; Zhou, J.; Li, F. Oxidative stress in oocyte aging and female reproduction. J. Cell. Physiol. 2021, 236, 7966–7983. [Google Scholar] [CrossRef]
- Saxena, P.; Selvaraj, K.; Khare, S.K.; Chaudhary, N. Superoxide dismutase as multipotent therapeutic antioxidant enzyme: Role in human diseases. Biotechnol. Lett. 2022, 44, 1–22. [Google Scholar] [CrossRef]
- Broeyer, F.J.; van Aken, B.E.; Suzuki, J.; Kemme, M.J.; Schoemaker, H.C.; Cohen, A.F.; Mizushima, Y.; Burggraaf, J. The pharmacokinetics and effects of a long-acting preparation of superoxide dismutase (PC-SOD) in man. Br. J. Clin. Pharmacol. 2008, 65, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Zelko, I.N.; Mariani, T.J.; Folz, R.J. Superoxide dismutase multigene family: A comparison of the CuZn-SOD (SOD1), Mn-SOD (SOD2), and EC-SOD (SOD3) gene structures, evolution, and expression. Free Radic. Biol. Med. 2002, 33, 337–349. [Google Scholar] [CrossRef]
- Najafi, A.; Asadi, E.; Benson, J.D. Ovarian tissue cryopreservation and transplantation: A review on reactive oxygen species generation and antioxidant therapy. Cell Tissue Res. 2023, 393, 401–423. [Google Scholar] [CrossRef]
- Stefanov, R.; Angelova, M.; Stefanova, T.; Subev, M.; Dolashka, P.; Voelter, W.; Zachariev, Z. Cu/Zn-superoxide dismutase from the fungal strain Humicola lutea 103 improves ram spermatozoa functions in vitro. Andrologia 2004, 36, 51–56. [Google Scholar] [CrossRef]
- Nonogaki, T.; Noda, Y.; Narimoto, K.; Umaoka, Y.; Mori, T. Effects of superoxide dismutase on mouse in vitro fertilization and embryo culture system. J. Assist. Reprod. Genet. 1992, 9, 274–280. [Google Scholar] [CrossRef]
- Rosa, A.C.; Corsi, D.; Cavi, N.; Bruni, N.; Dosio, F. Superoxide Dismutase Administration: A Review of Proposed Human Uses. Molecules 2021, 26, 1844. [Google Scholar] [CrossRef] [PubMed]
- Cocchia, N.; Corteggio, A.; Altamura, G.; Tafuri, S.; Rea, S.; Rosapane, I.; Sica, A.; Landolfi, F.; Ciani, F. The effects of superoxide dismutase addition to the transport medium on cumulus-oocyte complex apoptosis and IVF outcome in cats (Felis catus). Reprod. Biol. 2015, 15, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ochota, M.; Pasieka, A.; Niżański, W. Superoxide dismutase and taurine supplementation improves in vitro blastocyst yield from poor-quality feline oocytes. Theriogenology 2016, 85, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.H.; Tran, G.B.; Nguyen, C.T. Anti-oxidative effects of superoxide dismutase 3 on inflammatory diseases. J. Mol. Med. 2020, 98, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, Y.; Zhang, Y.; Zhang, Y.; Wang, W.; Han, H.; Yang, C.; Dong, X. Superoxide dismutase ameliorates oxidative stress and regulates liver transcriptomics to provide therapeutic benefits in hepatic inflammation. PeerJ 2023, 11, e15829. [Google Scholar] [CrossRef]
- Shuvaev, V.V.; Kiseleva, R.Y.; Arguiri, E.; Villa, C.H.; Muro, S.; Christofidou-Solomidou, M.; Stan, R.V.; Muzykantov, V.R. Targeting superoxide dismutase to endothelial caveolae profoundly alleviates inflammation caused by endotoxin. J. Control. Release 2018, 272, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Younus, H. Therapeutic potentials of superoxide dismutase. Int. J. Health Sci. 2018, 12, 88–93. [Google Scholar]
- Coudriet, G.M.; Delmastro-Greenwood, M.M.; Previte, D.M.; Marre, M.L.; O’Connor, E.C.; Novak, E.A.; Vincent, G.; Mollen, K.P.; Lee, S.; Dong, H.H.; et al. Treatment with a Catalytic Superoxide Dismutase (SOD) Mimetic Improves Liver Steatosis, Insulin Sensitivity, and Inflammation in Obesity-Induced Type 2 Diabetes. Antioxidants 2017, 6, 85. [Google Scholar] [CrossRef]
- Zheng, M.; Liu, Y.; Zhang, G.; Yang, Z.; Xu, W.; Chen, Q. The Applications and Mechanisms of Superoxide Dismutase in Medicine, Food, and Cosmetics. Antioxidants 2023, 12, 1675. [Google Scholar] [CrossRef]
- Bonetta, R. Potential Therapeutic Applications of MnSODs and SOD-Mimetics. Chemistry 2018, 24, 5032–5041. [Google Scholar] [CrossRef]
- Weisiger, R.A.; Fridovich, I. Superoxide dismutase. Organelle specificity. J. Biol. Chem. 1973, 248, 3582–3592. [Google Scholar] [CrossRef] [PubMed]
- Ben-Meir, A.; Burstein, E.; Borrego-Alvarez, A.; Chong, J.; Wong, E.; Yavorska, T.; Naranian, T.; Chi, M.; Wang, Y.; Bentov, Y.; et al. Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell 2015, 14, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Hornos Carneiro, M.F.; Colaiácovo, M.P. Beneficial antioxidant effects of Coenzyme Q10 on reproduction. Vitam. Horm. 2023, 121, 143–167. [Google Scholar] [CrossRef] [PubMed]
- Romao, S. Therapeutic value of oral supplementation with melon superoxide dismutase and wheat gliadin combination. Nutrition 2015, 31, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Bizoń, A.; Chojdak-Łukasiewicz, J.; Budrewicz, S.; Pokryszko-Dragan, A.; Piwowar, A. Exploring the Relationship between Antioxidant Enzymes, Oxidative Stress Markers, and Clinical Profile in Relapsing-Remitting Multiple Sclerosis. Antioxidants 2023, 12, 1638. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Jin, J.; Jeon, S.; Moon, S.H.; Park, M.Y.; Yum, D.Y.; Kim, J.H.; Kang, J.E.; Park, M.H.; Kim, E.J.; et al. SOD1 suppresses pro-inflammatory immune responses by protecting against oxidative stress in colitis. Redox Biol. 2020, 37, 101760. [Google Scholar] [CrossRef]
- Hannan, P.A.; Khan, J.A.; Ullah, I.; Ullah, S. Synergistic combinatorial antihyperlipidemic study of selected natural antioxidants; modulatory effects on lipid profile and endogenous antioxidants. Lipids Health Dis. 2016, 15, 151. [Google Scholar] [CrossRef]
- Lü, J.M.; Lin, P.H.; Yao, Q.; Chen, C. Chemical and molecular mechanisms of antioxidants: Experimental approaches and model systems. J. Cell. Mol. Med. 2010, 14, 840–860. [Google Scholar] [CrossRef]
- Ngestiningsih, D.; Rahayu, R.A.; Batubara, L. Effect of Superoxide Dismutase (SOD) Supplementation on Plasma Levels of Malondialdehyde (MDA), Total Cholesterol and LDL Cholesterol in the Elderly. J. Biomed. Transl. Res. 2019, 5, 29–33. [Google Scholar] [CrossRef]
- Wiener-Megnazi, Z.; Vardi, L.; Lissak, A.; Shnizer, S.; Reznick, A.Z.; Ishai, D.; Lahav-Baratz, S.; Shiloh, H.; Koifman, M.; Dirnfeld, M. Oxidative stress indices in follicular fluid as measured by the thermochemiluminescence assay correlate with outcome parameters in in vitro fertilization. Fertil. Steril. 2004, 82 (Suppl. S3), 1171–1176. [Google Scholar] [CrossRef]
- Huang, J.; Okuka, M.; McLean, M.; Keefe, D.L.; Liu, L. Telomere susceptibility to cigarette smoke-induced oxidative damage and chromosomal instability of mouse embryos in vitro. Free Radic. Biol. Med. 2010, 48, 1663–1676. [Google Scholar] [CrossRef]
- Appasamy, M.; Jauniaux, E.; Serhal, P.; Al-Qahtani, A.; Groome, N.P.; Muttukrishna, S. Evaluation of the relationship between follicular fluid oxidative stress, ovarian hormones, and response to gonadotropin stimulation. Fertil. Steril. 2008, 89, 912–921. [Google Scholar] [CrossRef]
- Becatti, M.; Fucci, R.; Mannucci, A.; Barygina, V.; Mugnaini, M.; Criscuoli, L.; Giachini, C.; Bertocci, F.; Picone, R.; Emmi, G.; et al. A Biochemical Approach to Detect Oxidative Stress in Infertile Women Undergoing Assisted Reproductive Technology Procedures. Int. J. Mol. Sci. 2018, 19, 592. [Google Scholar] [CrossRef]
- Barcelos, I.P.; Haas, R.H. CoQ10 and Aging. Biology 2019, 8, 28. [Google Scholar] [CrossRef]
- Bentov, Y.; Hannam, T.; Jurisicova, A.; Esfandiari, N.; Casper, R.F. Coenzyme Q10 Supplementation and Oocyte Aneuploidy in Women Undergoing IVF-ICSI Treatment. Clin. Med. Insights Reprod. Health 2014, 8, 31–36. [Google Scholar] [CrossRef]
- Xu, Y.; Nisenblat, V.; Lu, C.; Li, R.; Qiao, J.; Zhen, X.; Wang, S. Pretreatment with coenzyme Q10 improves ovarian response and embryo quality in low-prognosis young women with decreased ovarian reserve: A randomized controlled trial. Reprod. Biol. Endocrinol. 2018, 16, 29. [Google Scholar] [CrossRef]
- Showell, M.G.; Mackenzie-Proctor, R.; Jordan, V.; Hart, R.J. Antioxidants for female subfertility. Cochrane Database Syst. Rev. 2020, 8, CD007807. [Google Scholar] [CrossRef]
- Kim, N.H.; Kim, H.Y.; Lee, J.H.; Chang, I.; Heo, S.H.; Kim, J.; Kim, J.H.; Kang, J.H.; Lee, S.W. Superoxide dismutase secreting Bacillus amyloliquefaciens spores attenuate pulmonary fibrosis. Biomed. Pharmacother. 2023, 168, 115647. [Google Scholar] [CrossRef]
- Matos, L.; Stevenson, D.; Gomes, F.; Silva-Carvalho, J.L.; Almeida, H. Superoxide dismutase expression in human cumulus oophorus cells. Mol. Hum. Reprod. 2009, 15, 411–419. [Google Scholar] [CrossRef]
- Perkins, A.T.; Greig, M.M.; Sontakke, A.A.; Peloquin, A.S.; McPeek, M.A.; Bickel, S.E. Increased levels of superoxide dismutase suppress meiotic segregation errors in aging oocytes. Chromosoma 2019, 128, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Fridovich, I. Superoxide radical and superoxide dismutases. Annu. Rev. Biochem. 1995, 64, 97–112. [Google Scholar] [CrossRef]
- Natarajan, G.; Perriotte-Olson, C.; Bhinderwala, F.; Powers, R.; Desouza, C.V.; Talmon, G.A.; Yuhang, J.; Zimmerman, M.C.; Kabanov, A.V.; Saraswathi, V. Nanoformulated copper/zinc superoxide dismutase exerts differential effects on glucose vs lipid homeostasis depending on the diet composition possibly via altered AMPK signaling. Transl. Res. 2017, 188, 10–26. [Google Scholar] [CrossRef]
- Mohan, A.; Haider, R.; Fakhor, H.; Hina, F.; Kumar, V.; Jawed, A.; Majumder, K.; Ayaz, A.; Lal, P.M.; Tejwaney, U.; et al. Vitamin D and polycystic ovary syndrome (PCOS): A review. Ann. Med. Surg. 2023, 85, 3506–3511. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | GF101 (n = 30) | CoQ10 (n = 34) | p-Value |
|---|---|---|---|
| Age, mean ± S.D. (years) | 36.30 ± 4.25 | 35.38 ± 3.46 | 0.345 |
| Age, range (years) | 29–49 | 29–42 | |
| BMI, mean ± S.D. (kg/m2) | 24.57 ± 3.37 | 22.79 ± 3.52 | 0.044 |
| BMI, range (kg/m2) | 17.20–29.90 | 19.00–29.80 | |
| Infertility factor, n (%) | 0.19 | ||
| Male | 3 (10.71%) | 6 (19.35%) | |
| BTO | 4 (14.29%) | 3 (9.68%) | |
| DOR | 0 (0%) | 4 (12.90%) | |
| Unexplained | 6 (21.43%) | 8 (25.81%) | |
| Others | 15 (53.57%) | 10 (32.26%) | |
| Alcohol history, n (%) | 0.679 | ||
| Yes | 13 (43.33%) | 13 (38.24%) | |
| No | 17 (56.67%) | 21 (61.76%) | |
| Smoking history, n (%) | 1.000 | ||
| Yes | 4 (13.33%) | 4 (11.76%) | |
| No | 26 (86.67%) | 30 (88.24%) | |
| Past medical history, n (%) | 0.542 | ||
| Yes | 24 (80.00%) | 25 (73.53%) | |
| No | 6 (20.00%) | 9 (26.47%) | |
| Medication history, n (%) | 0.736 | ||
| Yes | 20 (66.67%) | 24 (70.59%) | |
| No | 10 (33.33%) | 10 (29.41%) |
| Variables | GF101 Group | CoQ10 Group | p-Value |
|---|---|---|---|
| Oxidative stress markers in FF | |||
| FF SOD at 2 weeks, mean ± S.D. (U/mL) | 1.03 ± 2.02 | 0.54 ± 0.12 | 0.519 |
| FF catalase at 2 weeks, mean ± S.D. (U/mL) | 9.22 ± 7.05 | 10.68 ± 8.42 | 0.490 |
| Lipid profiles | |||
| Total cholesterol, mean ± S.D. (mg/dL) | |||
| Baseline | 204.80 ± 40.46 | 192.15 ± 34.80 | 0.184 |
| 12-week follow-up | 189.87 ± 27.82 | 182.88 ± 34.54 | 0.381 |
| Change from baseline | −14.93 ± 27.51 | −9.26 ± 38.48 | 0.323 |
| p-value for paired | 0.006 | 0.170 | |
| HDL, mean ± S.D. (mg/dL) | |||
| Baseline | 57.82 ± 11.09 | 64.40 ± 11.95 | 0.028 |
| 12-week follow-up | 55.72 ± 12.20 | 63.70 ± 12.95 | 0.014 |
| Change from baseline | −2.10 ± 8.96 | −0.39 ± 9.37 | 0.464 |
| p-value for paired | 0.210 | 0.811 | |
| LDL, mean ± S.D. (mg/dL) | |||
| Baseline | 128.30 ± 35.20 | 115.03 ± 31.86 | 0.119 |
| 12-week follow-up | 114.20 ± 32.19 | 107.74 ± 30.14 | 0.492 |
| Change from baseline | −14.10 ± 27.50 | −7.29 ± 33.95 | 0.336 |
| p-value for paired | 0.009 | 0.219 | |
| TG, mean ± S.D. (mg/dL) | |||
| Baseline | 118.40 ± 77.79 | 111.85 ± 116.53 | 0.253 |
| 12-week follow-up | 145.03 ± 106.51 | 96.41 ± 49.94 | 0.046 |
| Change from baseline | 26.63 ± 90.51 | −14.39 ± 122.50 | 0.573 |
| p-value for paired | 0.118 | 0.505 | |
| Inflammation markers | |||
| TNF-α, mean ± S.D. (pg/mL) | |||
| Baseline | 0.55 ± 0.22 | 0.64 ± 0.41 | 0.443 |
| 12-week follow-up | 0.53 ± 0.19 | 0.54 ± 0.27 | 0.821 |
| Change from baseline | −0.02 ± 0.14 | −0.10 ± 0.33 | 0.672 |
| p-value for paired | 0.387 | 0.093 | |
| IL-1β, mean ± S.D. (U/mL) | |||
| Baseline | 0.08 ± 0.04 | 0.08 ± 0.05 | 0.576 |
| 12-week follow-up | 0.08 ± 0.04 | 0.08 ± 0.06 | 0.626 |
| Change from baseline | 0.00 ± 0.04 | 0.01 ± 0.07 | 0.778 |
| p-value for paired | 0.668 | 0.549 | |
| IL-6, mean ± S.D. (U/mL) | |||
| Baseline | 1.75 ± 1.20 | 1.65 ± 0.93 | 0.989 |
| 12-week follow-up | 2.30 ± 1.57 | 1.79 ± 0.98 | 0.12 |
| Change from baseline | 0.55 ± 1.63 | 0.14 ± 1.00 | 0.439 |
| p-value for paired | 0.074 | 0.427 | |
| hs-CRP, mean ± S.D. (U/mL) | |||
| Baseline | 0.19 ± 0.18 | 0.13 ± 0.13 | 0.107 |
| 12-week follow-up | 0.38 ± 0.54 | 0.14 ± 0.13 | 0.021 |
| Change from baseline | 0.19 ± 0.55 | 0.01 ± 0.15 | 0.636 |
| p-value for paired | 0.067 | 0.576 | |
| Immune cell activity | |||
| NK cell activity (U/mL) | |||
| Baseline | 2588.77 ± 2968.26 | 2378.86 ± 3392.39 | 0.687 |
| 12-week follow-up | 1899.59 ± 3344.97 | 1784.31 ± 6589.66 | 0.931 |
| Change from baseline | −689.17 ± 4095.96 | −594.54 ± 7686.04 | 0.431 |
| p-value for paired | 0.364 | 0.655 |
| Variables | GF101 Group | CoQ10 Group | p-Value |
|---|---|---|---|
| Oocytes at 2 weeks | |||
| Number of retrieved oocytes, mean ± S.D. (n) | 8.07 ± 4.23 | 7.94 ± 3.82 | 0.933 |
| Number of MII retrieved oocytes, mean ± S.D. (n) | 7.90 ± 4.26 | 7.79 ± 3.75 | 0.854 |
| Clinical outcomes of IVF | |||
| MII/total retrieved oocyte rate (%) | 60.11% (226/376) | 54.30% (246/453) | 0.093 |
| Fertilization rate (%) | 76.36% (239/313) | 71.86% (263/366) | 0.183 |
| Good-quality embryo rate (%) | 81.71% (67/82) | 89.11% (90/101) | 0.154 |
| Total pregnancy rate (%) | 60.71% (17/28) | 67.74% (21/31) | 0.598 |
| Implantation rate (%) | 38.10% (16/42) | 51.28% (20/39) | 0.268 |
| Clinical pregnancy rate (%) | 46.67% (14/30) | 52.94% (18/34) | 0.803 |
| Live birth rate (%) | 40.00% (12/30) | 41.18% (14/34) | 0.924 |
| Miscarriage rate (%) | 14.29% (2/14) | 27.78% (5/18) | 0.426 |
| Variables | GF101 Group (n = 42) | CoQ10 Group (n = 44) | p-Value |
|---|---|---|---|
| AEs | |||
| Total number | 48 | 34 | |
| Experienced patients’ number | 23 (54.76%) | 24 (54.55%) | 0.984 |
| AEs number per patient | |||
| Mild | 1.84 (35/19) | 1.20 (26/20) | |
| Moderate | 1.57 (11/7) | 1.14 (8/7) | |
| Severe | 1.00 (2/2) | 0 (0/0) | |
| Serious AEs | |||
| Experienced patients’ number | 1 (2.38%) | 0 (0%) | 0.488 |
| Causal relationship, number (events/patients) | |||
| Definite related | 0/0 | 0/0 | |
| Probably related | 0/0 | 1/1 | |
| Possibly related | 1/1 | 0/0 | |
| Probably not related | 1/1 | 0/0 | |
| Definitely not related | 40/22 | 33/23 | |
| Unknown | 6/1 | 0/0 | |
| AEs that cannot be ruled out in relation to target drugs, number (events/patients) | 7/2 | 1/1 | |
| Gastrointestinal disorders | 3/2 | 1/1 | |
| Abdominal pain | 1/1 | 0/0 | |
| Upper abdominal pain | 0/0 | 1/1 | |
| Diarrhea | 1/1 | 0/0 | |
| Nausea | 1/1 | 0/0 | |
| Abnormal laboratory findings | 2/1 | 0/0 | |
| ALT increased | 1/1 | 0/0 | |
| Blood cholesterol increased | 1/1 | 0/0 | |
| Metabolism and nutritional disorders | 2/1 | 0/0 | |
| Hypertriglyceridemia | 2/1 | 0/0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.Y.; Yoon, H.K.; Kim, J.H.; Kim, J.H.; Park, C.; Choi, D.H.; Yu, Y.D.; Shin, J.E.; Kwon, H. The Efficacy and Safety of GF101 and Its Antioxidant Effect on In Vitro Fertilization Outcomes: A Double-Blind, Non-Inferiority, Randomized, Controlled Trial with Coenzyme Q10. Antioxidants 2024, 13, 321. https://doi.org/10.3390/antiox13030321
Shin SY, Yoon HK, Kim JH, Kim JH, Park C, Choi DH, Yu YD, Shin JE, Kwon H. The Efficacy and Safety of GF101 and Its Antioxidant Effect on In Vitro Fertilization Outcomes: A Double-Blind, Non-Inferiority, Randomized, Controlled Trial with Coenzyme Q10. Antioxidants. 2024; 13(3):321. https://doi.org/10.3390/antiox13030321
Chicago/Turabian StyleShin, So Yeon, Hye Kyung Yoon, Jee Hyun Kim, Ji Hyang Kim, Chan Park, Dong Hee Choi, Young Dong Yu, Ji Eun Shin, and Hwang Kwon. 2024. "The Efficacy and Safety of GF101 and Its Antioxidant Effect on In Vitro Fertilization Outcomes: A Double-Blind, Non-Inferiority, Randomized, Controlled Trial with Coenzyme Q10" Antioxidants 13, no. 3: 321. https://doi.org/10.3390/antiox13030321
APA StyleShin, S. Y., Yoon, H. K., Kim, J. H., Kim, J. H., Park, C., Choi, D. H., Yu, Y. D., Shin, J. E., & Kwon, H. (2024). The Efficacy and Safety of GF101 and Its Antioxidant Effect on In Vitro Fertilization Outcomes: A Double-Blind, Non-Inferiority, Randomized, Controlled Trial with Coenzyme Q10. Antioxidants, 13(3), 321. https://doi.org/10.3390/antiox13030321