Abstract
Diabetes mellitus is recognized as the leading contributor to cardiovascular disease and associated mortality rates worldwide. Despite the use of pharmaceutical drugs to treat diabetes, its prevalence continues to rise alarmingly. Therefore, exploring remedies with a lower toxicity profile is crucial while remaining safe and effective in addressing this global public health crisis. Punica granatum Linn (pomegranate), known for its properties and safety profile, has been investigated in applied research and preclinical and clinical trials. However, conflicting reports still exist regarding its effects in diabetes. According to our knowledge, no systematic review has been conducted to critically analyze evidence from preclinical and clinical trials simultaneously, explicitly focusing on oxidative stress, inflammation, and endothelial function in diabetes. Therefore, in this systematic review, we searched for evidence on the impact of pomegranate in diabetes using databases such as PubMed, Scopus, and Google Scholar. Our inclusion criteria were limited to studies published in English. Of the 170 retrieved studies, 46 were deemed relevant and underwent critical analysis. The analyzed evidence suggests that pomegranate has the potential to alleviate oxidative stress, inflammation, and endothelial dysfunction in diabetes. Although a beneficial impact was noted in these markers, the endothelial function evidence still requires validation through further clinical trials with a powered sample size.
1. Introduction
Diabetes mellitus (DM) is a chronic metabolic condition characterized by hyperglycemia, which causes damage to the heart, blood vessels, eyes, kidneys, and nerves over time [1]. A report by the International Diabetes Federation (IDF) indicated that about 537 million people were living with DM in 2021, which is anticipated to reach 783 million by 2045 [2]. The IDF further revealed that about 90% of the DM population has type 2 diabetes globally (T2D) [2]. Some of the mechanisms implicated in the pathophysiology of T2D include oxidative stress, which disrupts insulin signaling, damages pancreatic β-cells, and induces inflammation, thus promoting endothelial dysfunction [3,4]. In oxidative stress, there is an imbalance between the rate of reactive oxygen species (ROS) production and the body’s ability to eliminate them [5]. This further predisposes the body to damage due to excessive ROS. Notably, endothelial dysfunction in T2D increases the risk of developing secondary complications and cardiovascular disease (CVD) (Figure 1).
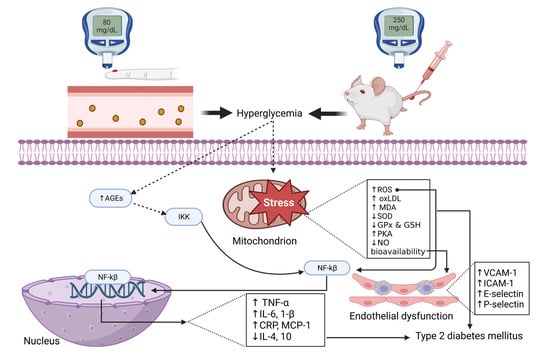
Figure 1.
An overview of the pathophysiology of endothelial dysfunction and type 2 diabetes. AGEs: advanced glycation end product; IKK: inhibitor of nuclear factor-κ; NF-κβ: nuclear factor kappa β; ROS: reactive oxygen species; oxLDL: oxidized lipoprotein; MDA: malondialdehydes; SOD: superoxide dismutase; GPx: glutathione peroxidase; GSH: glutathione; PKA: protein kinase; NO: nitric oxide; TNF-α: tumor necrosis factor-alpha; IL: interleukin; CRP: C-reactive protein; MCP-1: monocyte chemoattractant protein-1, VCAM-1: vascular adhesion molecules-1; ICAM-1: intercellular adhesion molecule-1.
The literature suggests that any therapeutic approach that can ameliorate oxidative stress may help control T2D and associated CVD. Several pharmaceutical drugs, including sodium-glucose cotransporter-2 (SGLT2) inhibitors, biguanides, glitazones, and α-glucosidase inhibitors, are widely used to control insulin sensitivity and reduce blood glucose in T2D patients [6,7]. However, such drugs are associated with various adverse effects and related complications, ranging from megaloblastic anemia and neuropathy associated with vitamin B12 deficiency, increased low-density lipoproteins (LDL), hypoglycemia, water retention, acidosis, bone fractures, heart failure, weight gain, and gastrointestinal reactions [6,7,8,9]. Due to all these secondary complications associated with pharmacological drugs, it would be ideal to evaluate the effect of functional foods and natural compounds with antioxidants on diabetes control and management. In fact, the World Health Organization (WHO) acknowledges the benefits of traditional, complementary, and alternative medicines (TCAMs), especially the use of plants that have been scientifically proven to be effective [10]. This has prompted more research into natural remedies for diabetes.
In South Africa, traditional medicine has existed for a long time, with practitioners providing care to the public, although some of these medicinal plants are not properly verified by botanists for use in diabetes [11]. More recently, Mokgalaboni et al. [12] reported a significant effect of Corchorus olitorius in animal models of diabetes on hyperglycemia, oxidative stress, and inflammation. Although the results showed potential benefits in diabetes, this was only conducted in preclinical models, thus calling for more research in clinical trials. Although there are limitations associated with the translation of preclinical studies into clinical trials, the evidence from these studies may provide the basis for developing new alternative therapies to treat DM and prevent secondary complications. Pomegranate is another fruit that has gained research attention due to its antioxidant properties and, more recently, has been suggested to be a functional food due to its multiple health-promoting properties [13,14]. This fruit is scientifically known as Punica granatum Linn and belongs to the Plantae kingdom and Punicaceae family [15]. Several studies have investigated the effects of pomegranate on oxidative stress in diabetes. The evidence from preclinical studies has demonstrated the potential effect of pomegranate as an anti-oxidative agent, as revealed by its ability to reduce the levels of ROS in rodent models of diabetes [16,17,18,19,20,21,22,23,24].
Interestingly, the same results seem to be observable in clinical studies, as revealed by reduced markers of oxidative stress in T2D patients following treatment with pomegranate [25,26,27,28,29,30]. However, there are still some inconsistencies in clinical trials on the impact of pomegranate, especially on different markers of oxidative stress and inflammation, and limited evidence on endothelial function in diabetes. More recently, a meta-analysis was conducted on pomegranate, and the researchers found no effect of pomegranate on oxidative stress and inflammation. One of the limitations is that their analysis focused on only total antioxidant capacity (TAC) and high-sensitive C-reactive protein (hs-CRP) as markers of oxidative stress and inflammation, respectively; hence, they might not independently be ideal predictors [27]. In contrast, another meta-analysis showed a significant decrease in hs-CRP, interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) without effects on CRP, soluble vascular cell adhesion molecule-1 (sVCAM-1), soluble intercellular cell adhesion molecule-1 (sICAM-1), and malonaldehyde (MDA) [31].
Additionally, a meta-analysis by Morvaridzadeh et al. [32] on pomegranate showed no effect on TAC, glutathione peroxidase (GPx), paraoxonase-1 (PON1), and MDA. Furthermore, the analyzed studies encompassed a wide range of conditions, making it difficult to interpret and make conclusive remarks and recommendations to a wider diabetic population. The current review highlights the potential benefits of pomegranate extracts, focusing on various oxidative, inflammation, and endothelial markers in diabetes while elucidating its mode of action.
2. Methodology
2.1. Search Strategy
Evidence was retrieved by independent investigators (KM and SD) through online databases, including Scopus and PubMed, on 20 May 2023 and updated on 20 July 2023, according to the updated guidelines of the preferred reporting items for systematic review and meta-analysis (PRISMA) [33]. The exact search strategy is presented in the Supplementary File (Tables S1–S6). The search comprised five key terms: “pomegranate”, “oxidative stress”, “inflammation”, “endothelial dysfunction”, and “diabetes mellitus”. This was performed in a separate search with the use of the Boolean operator “AND”. The search was restricted to evidence published in English, however, with no duration limitation. Additionally, two independent investigators verified the search before decisions could be made (WNP and PM).
2.2. Study Selection
Two independent researchers (KM and SD) selected the studies based on their title, abstract, keywords, and overall aims and findings. The third independent researcher read all of the studies that the prior researchers had disagreements on and made a conclusion. The studies that passed the initial screening were subjected to a full screening of their full text. All studies that passed the second phase of screening were included if they met the following criteria: (i) they used either pomegranate juice extract, powder, or its active compounds; (ii) they included a rodent model of diabetes or diabetic patients; and (iii) they reported any markers of oxidative stress, inflammation, or endothelial function. The exclusion criteria were (i) reviews, commentaries, book chapters, and letters to editors and (ii) in vitro studies.
2.3. Data Extraction
Two investigators (KM and SD) independently extracted data from all relevant studies. The data extracted from each clinical study included the first author’s surname; publication year; the country where the study was conducted; the study design; the number of participants in both groups; the number and proportion of males; the mean age in years; the body mass index (BMI) of the group on pomegranate in kg/m2; the duration of treatment with pomegranate; the dose; the form of pomegranate treatment; and the main findings. Similarly, for preclinical studies, the data extracted included the first author’s surname, the experimental model, the form of pomegranate and the duration of treatment, the main findings, and the statistical data for effect measures. In cases of disparities between the two investigators, WNP made a decision by re-evaluating the study and items in question.
3. Results
A total of 95 records were obtained from Scopus, while 57 were retrieved from PubMed. Additionally, Google Scholar was searched, and about 18 records were found relevant. Prior to the screening process, it was determined that 34 records were duplicates found in both databases through these separate searches, and thus, they were excluded. As a result, 136 records were subjected to initial screening by their title, abstract, keywords, and objectives. Fifty-one records were considered irrelevant and excluded due to their title, abstract, and aims being outside the scope of our review.
Consequently, a total of 85 records underwent a thorough screening process. Among these 85 records, 39 were excluded based on the following criteria: 17 were review articles, 9 did not report on outcomes of interest, 4 did not focus on pomegranate as an intervention, 1 was a commentary, 1 was a book chapter, 5 were not related to diabetes or models, 1 was a cell culture study, and 1 was a study protocol. Hence, a total of 46 records (33 preclinical and 13 clinical trials) were deemed relevant as they reported on the effect measures of interest in diabetic models or patients (Figure 2).
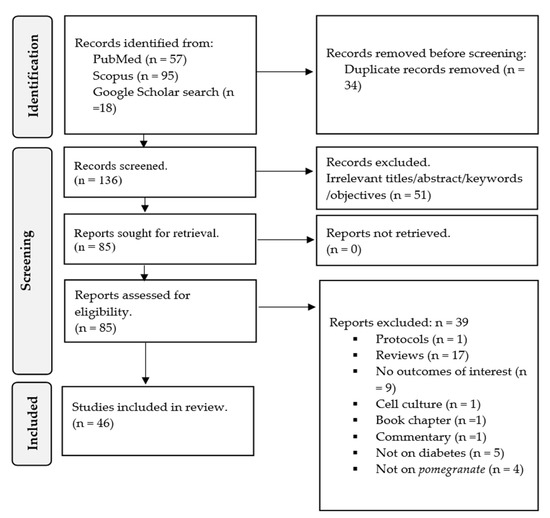
Figure 2.
PRISMA flow chart depicting the study selection, screening, and inclusion.
Characteristics of the included clinical and preclinical studies.
We identified 33 preclinical studies published in peer-reviewed journals from 2006 to 2023 relevant to our review. These studies were published in various countries, including China [22,34,35], Egypt [36,37,38,39,40,41,42,43,44], India [24,45,46,47,48], Iran [20,23,49,50], Indonesia [51], Israel [52], Iraq [53], Malaysia [16,54], Mexico [55], Saudi Arabia [56], Turkey [19,21,57,58], and United States of America [59]. Various methods were used to induce a diabetes model in these preclinical studies, such as the intraperitoneal injection of single streptozotocin (STZ), STZ combined with nicotinamide (NAD), STZ, and high-fat diet, and alloxan monohydrate. Different rodent models, including rats (Wistar, Sprague Dawley, and Swiss Albino) and mice (C57BL/6, Balb/C, and Kunming), were used in these studies (Table 1).

Table 1.
General overview of the effect of pomegranate extract and its active compounds on oxidative stress in rodent models of diabetes.
Additionally, we found thirteen relevant clinical studies that investigated the impact of pomegranate on oxidative stress, inflammation, and endothelial function in individuals with diabetes. These studies were published in peer-reviewed journals between 2000 and 2022, thus providing a comprehensive range of evidence on the effects of pomegranate in diabetes. The research was conducted in various countries, including three studies in Israel [28,29,60], eight in Iran [25,26,30,61,62,63,64,65], one in Turkey [66], and one in Bosnia and Herzegovina [67]. A total of 468 participants with diabetes, with a mean age of 54.48 ± 1.64, were included in these studies, alongside 120 healthy control individuals. The mean body mass index for the diabetic group receiving pomegranate was 29.70 ± 2.42 kg/m2, and 145 participants were male. The pomegranate was administered orally as juice or a capsule for 6 weeks to 3 months (Table 2). Different study designs were included, with at least four being quasi-experimental; this study aims to evaluate interventions but does not use randomization. One was a case–control study and eight were randomized controlled trials (Table 2).
Table 2.
Overview of the effect of pomegranate extract and its active compounds on oxidative stress and inflammation in diabetic patients.
An overview of pomegranate, its bioactive compounds, and its bioavailability.
Punica granatum L. (pomegranate) is a plant belonging to the Punicaceae family [15]. It is widely cultivated in regions such as the Middle East, the Caucasus, northern and tropical Africa, Iran, the Indian subcontinent, Central Asia, Southeast Asia (in drier parts), and the Mediterranean Basin [68]. Therefore, consuming fruits and vegetables containing these bioactive compounds has been associated with good health [69,70]. Some of these bioactive compounds found in pomegranate fruit include hydrolyzable tannins like gallotannins and ellagitannins, along with ellagic acid and its derivatives, gallic acid, anthocyanins, proanthocyanidins, flavonoids, vitamins, sterols, lignans, saccharides, fatty acids, organic acids, terpenes, and terpenoids (Figure 3). The term “bioavailability” refers to the extent to which a chemical or medicine becomes available to its intended target tissue [71]. In the case of pomegranate, ellagitannins are metabolized into ellagic acid and glucose in the small intestine [72], while gallotannins are metabolized into gallic acid and glucose [73,74,75]. The predominant hydrolyzable tannin in pomegranate is punicalagin [76], in pomegranate juice [77,78,79]. The primary phenolic compounds in pomegranate seed include flavol-3-ols, flavonoid glycosides, phenolic acids, and hydrolyzable tannins [80,81]. Pomegranate peel is abundant in gallic acid and is known for its high phenolic content, and it is also rich in flavonoids, including kaempferol-3-O-glucoside [69]. A fresh pomegranate fruit peel contains at least flavonoids (51.52 ± 8.14 mg of rutin), total phenolic compounds (85.60 ± 4.87 mg of gallic acid), anthocyanins (102.2 ± 16.4 mg of cyanidin-3-glucoside), and hydrolyzable tannins (139.63 ± 4.25 mg of tannic acid) [81].
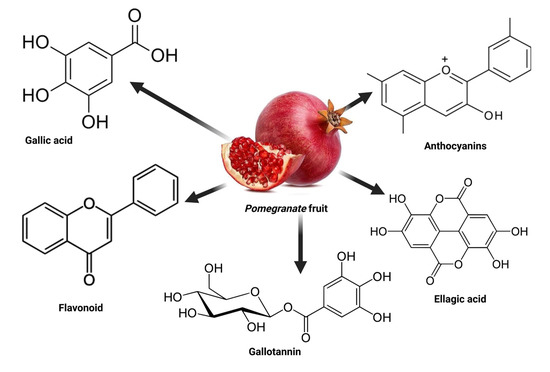
Figure 3.
The active compounds found in pomegranate.
The effect of pomegranate and its derivatives on markers of inflammation in animal models of diabetes.
Evidence from preclinical studies has revealed, to some extent, the potential of pomegranate as an anti-inflammatory remedy. For instance, El-Deeb et al. [41] used Sprague Dawley STZ-NAD-induced diabetic rats to explore the benefits of 200 mg/kg of ethanolic extract of pomegranate for four weeks. This study demonstrated a significantly lower level of TNF-α (43.2 ± 1.51 pg/mL) compared to untreated diabetic rats (73.0 ± 0.87 pg/mL), p < 0.05. The same researcher further reported significantly decreased IL-6 (46.1 ± 1.31 pg/mL) compared to the untreated group (66.9 ± 0.99 pg/mL), p < 0.05. Moreover, these findings were confirmed by a previous study that used the same model [54] with a dose of 1 mL of PJ or 100 mg of pomegranate seed powder for 21 days. Interestingly, they reported a significant decrease in markers of inflammation, including TNF-α, IL-6, and NF-κβ. For instance, the mean of TNF-α was 2944.02 pg/mL, p > 0.05, and 2844.92 pg/mL, p < 0.05, at 1 mL of PJ and 100 mg of PS, respectively, compared to the untreated group, with 3074.37 pg/mL. Additionally, there was a decrease in the levels of IL-6 in the respective dosages: 296.42 pg/mL, p < 0.01, and 316.51 pg/mL, p < 0.01, compared to 355.86 pg/mL. Furthermore, the same study showed reduced NF-κβ in PJ, 2228.89 pg/mL, p < 0.05, and 2138.68 pg/mL in the PS group compared to the untreated group, with 2337.14 pg/mL, p < 0.01. Similar results are partly corroborated by Shaker et al. [44], who also used the same model of diabetes and a slightly higher dosage (300 mg/kg) of pomegranate seed extract for four weeks. Consistently, they demonstrated a significant decrease in the pancreatic expression of NF-κβ, mean, SD, 765.6 ± 9.9 pg/gm, compared to the untreated group, with 992.5 ± 8.46 pg/gm, p < 0.01. Furthermore, transforming growth factor beta (TGF-β) was significantly decreased in the treated group, 477.5 ± 4.24 pg/gm, compared to the untreated group, 879.16 ± 6.91 pg/gm, p < 0.01. In another investigation, diabetic Sprague Dawley rats induced by STZ were subjected to an oral pomegranate regimen of 150 mg/kg daily for 18 days [56]. In this experiment, the researchers made notable observations, specifically a substantial reduction in embryonic IL-1β, 2.78 ± 0.48 pg/mL, compared to 4.12 ± 0.57 pg/mL and IL-6, 1.30 ± 0.15 pg/mL compared to the untreated group, 2.18 ± 0.29 pg/mL. Moreover, in the diabetic mother rats, the same results were shown. For instance, there was a decrease in IL-6: 3.74 ± 1.08 pg/mL and IL-1β, 5.12 ± 1.24 pg/mL compared to the untreated diabetic groups: IL-6, 6.44 ± 1.98 pg/mL, p < 0.05 and IL-1β, 7.99 ± 1.23 pg/mL, p < 0.05. These results are further supported by Abo-Saif et al. [43], who demonstrated a significant decrease in IL-1β following eight weeks of PPE at a 150 mg/kg dose in diabetic Wistar rats. El-Missiry et al. [42] used the same model with an intraperitoneal punicalagin dose of 1 mg/kg for 15 days. Consistently, the treatment resulted in a significant decrease in IL-6 (45.9 ± 2.27 pg/mL compared to 72.7 ± 1.98 pg/mL, p < 0.001); TNF-α, (37.3 ± 0.42 pg/mL compared to 63.8 ± 2.75 pg/mL, p < 0.001); and IL-1β (75.7 ± 2.09 pg/mL compared to 124.9 ± 4.44 pg/mL, p < 0.001). In the most recent study by Abdulhadi et al. [53], STZ-induced diabetic Wistar rats were intraperitoneally injected with punicalagin at a dose of 1 mg/kg for 15 days; interestingly, this was associated with a significant decrease in CRP (p < 0.001) and MCP-1 (p < 0.001) levels compared to the untreated diabetic group. On the contrary, a different study found no significant effect of pomegranate oil on CRP (p < 0.05) in HFD-fed mice [59].
The effects of pomegranate and its derivatives on markers of endothelial function in rodent models of diabetes.
Endothelial dysfunction in diabetes increases the risk of developing CVD complications such as atherosclerosis due to the formation of foam cells in the blood vessels [82]. Thus, to curb these secondary complications in diabetes, it is important to control endothelial dysfunction in diabetes. Therefore, pomegranate may improve endothelial function due to its antioxidant potential, especially in diabetes. For example, in Sprague Dawley rats with STZ-NAD-induced diabetes, a four-week administration of 200 mg/kg of ethanolic extract of pomegranate demonstrated a significant decrease in NO bioavailability: 34.4 ± 0.60 µmol/L, p < 0.05 compared to 56.3 ± 1.30 µmol/L [41]. A study by Çukurova et al. [58], also using the same animal model, revealed that 2.5 mL of PJ treatment significantly decreased endothelial nitric oxide synthase (eNOS) expression (p < 0.05). Additionally, in Wistar rats with STZ-NAD-induced diabetes, lower levels of NADPH oxidase (NOx) were observed following oral administration of PAJ at 100 (13 ± 1.5 µmol/g) or 300 mg (11.6 ± 1.0 5 µmol/g) compared to 31.7 ± 1.45 µmol/g, p < 0.001 [36]. However, Onal et al. [19], after using 100 mg/kg pomegranate for ten weeks in Sprague Dawley STZ-induced diabetic rats, observed no significant difference in iNOS (p > 0.05) and eNOS (p > 0.05) protein levels. Most recently, Abdulhadi et al. [53] investigated 1 mg/kg intraperitoneal injection of punicalagin in STZ-induced diabetic Wistar rats for 15 days. Interestingly, this study reported significantly lower levels of ICAM-1 (p < 0.001), VCAM-1 (p < 0.001), E-selectin (p < 0.001), and endothelin-1 (ET-1) (p < 0.001) compared to the untreated diabetic group. The aforementioned results were corroborated by El-Mansi et al. [56], who used the same model coupled with an oral methanolic extract of pomegranate at a 150 mg/kg dose for 18 days. This study demonstrated a significant decrease in the level of ET-1 in both the embryo (3.59 ± 0.27 pg/mL) and its mother (6.87 ± 0.41 pg/mL) compared to the untreated diabetic embryo (5.16 ± 0.37 pg/mL) and its mother (8.87 ± 0.68 pg/mL). Increased ET-1 stimulates the production of ROS [83,84]. Its reduction in diabetes following pomegranate treatment shows its potential to ameliorate endothelial dysfunction and associated CVD complications.
The effect of pomegranate and its derivatives on markers of oxidative stress in a rodent model of diabetes.
For instance, in Wistar rats with STZ-induced diabetes, treatment with pomegranate seed oil at doses of 0.4 and 0.8 mg/kg for 28 days increased total thiol content and decreased MDA levels in the heart (p < 0.01) and kidneys (p < 0.001) [23]. Similarly, in an STZ-NAD-induced diabetic model, high doses of pomegranate aril juice (100 or 300 mg/kg) administered for six weeks significantly reduced MDA levels (12.03 ± 0.37 nmol/g) at 100 mg/kg and 6.67 ± 0.22 nmol/g at 300 mg/kg compared to untreated diabetic group (13.81 ± 0.44 nmol/g). Consistently, this study reported increased activity of GPx (44.2 ± 7.9 U/g at 100 mg/kg) and (67.1 ± 3.7 U/g, p < 0.001 at 300 mg/kg) compared to 26.1 ± 1.7 U/g, p < 0.001, glutathione (GSH) (1.54 ± 0.26 mmol/g at 100 mg/kg and 2.34 ± 0.31 mmol/g, p < 0.001 at 300 mg/kg versus 1.02 ± 0.06 mmol/g. Concomitantly, the levels of superoxide dismutase (SOD) showed a significant increase at both 100 mg/kg (557.6 ± 10.1 U/g, p < 0.001) and 300 mg/kg (611.8 ± 12.4 U/g, p < 0.001) compared to the baseline (510.0 ± 6.3 U/g). Similarly, catalase (CAT) levels also exhibited a noticeable increase at 100 mg/kg (1.88 ± 0.03 U/g) and 300 mg/kg (1.83 ± 0.04 U/g) compared to untreated diabetic 1.42 ± 0.12 U/g [36]. Another study using the same model reported that different doses decrease pancreatic thiobarbituric acid reactive substances (TBARS) and MDA levels. For instance, MDA was reduced (0.427 ± 0.034 nmol/mg at 250 mg/kg and 0.325 ± 0.012 nmol/mg at 500 mg/kg) compared to untreated diabetic rats (0.686 ± 0.035 nmol/mg, p < 0.001. Interestingly, this was accompanied by increased activities of GPx (p < 0.05), GSH (7.31 ± 0.109 nmol/g at 250 mg/kg and 11.36 ± 0.099 nmol/g at 500 mg/kg) compared to 2.68 ± 0.87 nmol/g, CAT (p < 0.05), SOD (p < 0.05), and glutathione reductase (GR) (p < 0.05) [47]. Consistently, in a Sprague Dawley diabetic rat induced by STZ-NAD, treatment with an ethanolic extract of pomegranate at a dose of 200 mg/kg for four weeks led to a decrease in MDA levels (14.9 ± 0.43 nmol/mL compared to untreated group, 21.7 ± 0.97 nmol/mL). This was coupled with an increase in markers of antioxidant capacity such as TAC (0.57 ± 0.02 mmol/L compared to 0.29 ± 0.01 mmol/L, p < 0.05) and GSH (38.7 ± 0.96 mg/dL compared to 26.0 ± 0.79 mg/dL, p < 0.05) [41]. Furthermore, in STZ-induced diabetic Wistar rats, administration of PSO at doses of 0.4 and 0.8 mL/kg for three weeks significantly increased the activity of CAT (p < 0.001), SOD (p < 0.001), and GPx (p < 0.001) in the tissue and mitochondria while decreasing oxidative stress index (OSI) values [49]. These findings are also supported by an experimental study in Wistar diabetic rats that were treated with pomegranate peel extract (PSE) at a dose of 300 mg/kg for four weeks, as they also reported a significant increase in pancreatic GSH levels (46.78 ± 1.5 pg/gm compared to 46.78 ± 1.5 pg/gm) [44]. The administration of pomegranate as either leaf extracts (100 and 200 mg/kg) increased SOD (2.03 ± 0.28 Umin/mg at 100 mg/kg and 2.47 ± 0.31 Umin/mg at 200 mg/kg) compared to 1.85 ± 0.15 Umin/mg. Likewise, the 100 or 200 mg/kg of fruit peel extract also significantly increased SOD (2.32 ± 0.35 Umin/mg at 100 mg/kg and 2.82 ± 0.29 Umin/mg at 200 mg/kg all compared to 1.85 ± 0.15 Umin/mg) and CAT (60.23 ± 5.26 Umin/mg at 100 mg/kg and 70.23 ± 5.13 Umin/mg at 200 mg/kg both compared to 40.02 ± 4.51 Umin/mg). Furthermore, the same study reported a decrease in TBARS in (2.33 ± 0.62 mmol/g and 1.65 ± 0.28 mmol/g at 100 LEP and PEP, respectively, compared to untreated diabetic rats, with 2.75 ± 0.78 mmol/g, p < 0.05) Wistar diabetic rats [48]. According to Tugcu et al. [21], PJ at a dose of 100 μL significantly increased GSH (21.58 ± 1.65 nmol/mg compared to 16.15 ± 2.63 nmol/mg, p = 0.010) and GPx (187.95 ± 26.62 nmol/mg compared to 148.09 ± 26.61 nmol/mg, p = 0.042) in Sprague Dawley diabetic rats. In addition, the same scholar reported a significant decrease in MDA (0.92 ± 0.09 nmol/mg compared to 1.28 ± 0.11 nmol/mg, p < 0.001) without changes in SOD (21.87 ± 3.54 U/mg compared to 20.58 ± 5.34 U/mg, p = 0.938). Interestingly, evidence from Wistar diabetic rats treated with PGE at doses of 100, 200, and 350 mg/kg for 21 days revealed a significant reduction in the generation of ROS (p < 0.001) [50]. Bagheri et al. [20] also demonstrated a significant increase in GSH (p < 0.05), GPx (p < 0.05), and SOD (p < 0.05), concomitant with decreased CAT (p < 0.05) and MDA (p < 0.05) when diabetic Wistar rats were treated with ethanolic pomegranate extract. Similarly, the recent findings of Abo-Saif et al. [43] showed that the use of pomegranate peel extract (PPE) at a dose of 150 mg/kg for eight weeks significantly decreased lipid peroxidation and MDA.
Consistently, El-Missiry et al. [42] showed that intraperitoneal administration of punicalagin at a dose of 1 mg/kg for 15 days in Wistar rats resulted in a significant increase in GSH (p < 0.001), CAT (p < 0.001), and SOD (p < 0.001) activity while decreasing MDA (p < 0.001) and hydrogen peroxide levels (p < 0.001). Similarly, treatment with pomegranate juice or seed extract at a dose of 500 mg/kg for four weeks significantly increased CAT (39.5± 2.27 U/mL, p < 0.05, with PJ and 38.20 ± 3.08 U/mL compared to 21.7 ± 2.83 U/mL, p < 0.05) activity and decreased MDA (16.37 ± 2.77 µmol/L, p < 0.05, and 14.1 ± 2.54 µmol/L, p < 0.05, compared to 23.73 ± 3.29 µmol/L, p < 0.05) levels in albino rats with alloxan-induced diabetes [37]. Most importantly, three different doses of pomegranate hexane extract (25, 50, and 75 mg/kg) given to STZ-induced diabetic Wistar rats for eight weeks significantly decreased MDA levels (142 ± 32 µmol/mg, 133 ± 25 µmol/mg, and 121 ± 25 µmol/mg, respectively, compared to 188 ± 37 µmol/mg, p < 0.05). The same study reported increased GSH (259 ± 50 µg /mg, 128 ± 16.4 µg /mg, and 128 ± 16.4 µg /mg, with all values compared to 123.6 ± 19.3 µg/mg, p < 0.05). In addition, this study demonstrated increased CAT activity at 25, 50, and 75 mg/kg (843 ± 134 U/mg, 987 ± 56 U/mg, and 1112 ± 86 U/mg, respectively, in comparison with 358± 65 U/mg, p < 0.05). Furthermore, these researchers demonstrated a significant increase in SOD according to these dosages (1021 ± 163 U/mg, 836 ± 53 U/mg, and 1233 ± 153 U/mg, respectively, compared to 760 ± 78 U/mg, p < 0.05) [38]. When Wistar rats were treated with STZ to induce diabetes and further fed with a ground pomegranate flower pellet mixture (300, 400, and 500 mg/kg), decreased levels of lipid peroxidation (LPO) (3.41 ± 0.24, 3.21 ± 0.24, and 2.91 ± 0.38, respectively, compared to 5.54 ± 0.25) were found. The same study reported improved GSH activity (162.9 ± 3.7 µg/g, 172.8 ± 4.0 µg/g, and 179.8 ± 3.3 µg/g in the respective doses compared to 156.1 ± 3.3 µg/g, p < 0.05) [57]. Although a study that used 2.5 mL of diluted pomegranate juice in STZ-indued diabetic Sprague Dawley rats showed a significant increase in SOD activity (11.28 (9.71–12.85) U/mg) compared to (8.72 (8.07–10)U/mg, p < 0.001)), this was associated with no significant changes in GSH (2.28 (1.89–2.69) nmol/mg) compared to the untreated diabetic rats (1.96 (1.64–2.16), p > 0.05)) [58]. Another study focused on Wistar rats with STZ-induced diabetes when treated with a pomegranate flavonoid fraction at doses of 50 mg/kg, 100 mg/kg, and 200 mg/kg for 28 days [46]. The results showed a significant decrease in MDA levels (289.31 ± 4.70 nmol/mg, 268.55 ± 5.65 nmol/mg, and 229.58 ± 4.03 nmol/mg, all compared to 389.87 ± 6.58 nmol/mg, p < 0.01) which was more pronounced at 200 mg/kg. Additionally, the same report showed an increase in GSH (3.97 ± 0.06 U/mg, 4.14 ± 0.04 U/mg, and 4.53 ± 0.06 U/mg, respectively, compared to 2.73 ± 0.06 U/mg, p < 0.01) SOD activity [46]. Interestingly, CAT was reportedly increased (42.59 ± 0.74 U/mg, 46.21 ± 0.65 U/mg, and 52.48 ± 0.64 U/mg in the respective dosages compared to the untreated group, 36.64 ± 1.54 U/mg, p < 0.001). Lastly, the same study showed an increase in the activities of SOD in all doses as compared to the untreated group (5.03 ± 0.05 U/mg, 5.71 ± 0.13 U/mg, and 6.11 ± 0.12 U/mg, respectively, compared to 3.35 ± 0.16 U/mg, p < 0.001).
Similar findings were observed in diabetic rats given oral administration of pomegranate leaves ethanolic extract at doses of 50, 100, and 200 mg/kg for 28 days [45]. This led to significantly decreased MDA in all doses (343.38 ± 5.95 nmol/mg, 274.22 ± 6.17 nmol/mg, and 242.69 ± 6.28 nmol/mg, respectively, compared to 448.91 ± 12.12 nmol/mg, p < 0.01), with a pronounced reduction observed at 200 mg/kg [45]. Moreover, there was increased activity of GSH (25.92 ± 1.12 U/mg, 32.28 ± 0.92 U/mg, and 36.99 ± 1.09 U/mg, respectively, compared to 13.62 ± 1.07 U/mg, p < 0.01), CAT (51.21 ± 0.54 U/mg, 57.52 ± 0.58 U/mg and 66.59 ± 0.57 U/mg, respectively, compared to 43.68 ± 1.41 U/mg, p < 0.01), and SOD (11.22 ± 0.69 U/mg, 10.66 ± 0.62 U/mg, and 11.84 ± 0.47 U/mg, respectively, compared to 5.16 ± 0.79 U/mg, p < 0.01) [45]. Regarding STZ-induced IDDM in Swiss Albino rats, pomegranate at 200 mg/kg for 20 days significantly increased SOD (182.8 ± 11.68 U/mL versus the untreated group 50.06 ± 3.56 U/mL, p < 0.001) and TAC (1.40 ± 0.06 mM/L compared to 0.604 ± 0.18 U/mg, p < 0.001) [39]. Interestingly, this was accompanied by a reduction in the level of MDA (4.48 ± 1.14 nmol/L compared to 9.84 ± 1.21 nmol/L, p < 0.001) [39]. Onal et al. [19] also demonstrated a significant decrease in MDA levels (p < 0.05) following the administration of pomegranate at a dose of 100 mg/kg for ten weeks in Sprague Dawley STZ-induced diabetic rats. According to El-Mansi et al. [56], the administration of 150 mg/kg pomegranate for 18 days to diabetic mothers significantly reduced MDA (p < 0.05) and GPx (p < 0.05) activity and remarkably increased the activity of CAT (p < 0.05) and SOD (p < 0.05) enzymes in diabetic Wistar rats. In a study involving STZ-NAD-induced Sprague-Dawley rats, the combination of pomegranate juice and seeds (1 mL of PJ + 100 mg of PS) for 21 days significantly increased the levels of enzymatic antioxidants, including CAT, SOD (25.1 ± 0.42 U/mL, 20.8 ± 0.61 U/mL, and 28.9 ± 0.8 U/mL compared to 17.2 ± 0.51 U/mL, p < 0.05), and total antioxidant status (TAS) (0.91 ± 0.01 mmol/L, 0.73 ± 0.11 mmol/L, and 1.03 ± 0.03 mmol/L compared to 0.69 ± 0.03 mmol/L, p < 0.05), and decreased MDA (p < 0.05) in the plasma [16]. Treating STZ-induced diabetic Wistar rats with pomegranate juice at doses of 100 mg/kg and 300 mg/kg for four weeks resulted in increased GSH (56.25 ± 1.90 nM/mg and 66.51 ± 1.82 nM/mg compared to 34.67 ± 2.76 nM/mg, p < 0.05), CAT (47.14 ± 1.65 U/mg and 66.36 ± 1.99 U/mg compared to 16.47 ± 0.79 U/mg, p < 0.05), and SOD levels (165.3 ± 3.25 U/mg, 237.9 ± 19.72 U/mg compared to 45.62 ± 6.10 U/mg, p < 0.05) and decreased levels of TBARS (1.247 ± 0.02 μM/mg and 0.80 ± 0.02 μM/mg in respective dosage compared to untreated group 2.23 ± 0.04 µM/mg, p < 0.05) [24]. Some contrasting findings were dose-dependent as Praseytastuti et al. [51] revealed that STZ-induced diabetic Sprague Dawley rats for four weeks of pomegranate juice only 2 mL/200 g of PJ could significantly decrease MDA levels while 1 and 4 mL/200 g showed no difference in MDA levels (post-treatment, 0.69 ± 0.22 µmol/L compared to baseline 2.02 ± 1.68 µmol/L, p > 0.05 at 1 mL/200g). Moreover, at 2 mL/200 g (0.68 ± 0.38 µmol/L compared to 2.02 ± 1.68 µmol/L, p < 0.05 at 2 mL/200 g) and 0.85 ± 0.12 µmol/L compared to 3.16 ± 2.09 µmol/L at a dose of 4 mL/200 g. This is partially supported by more recent evidence, as a study by Abdulhadi et al. [53] showed that intraperitoneal injection of punicalagin at 1 mg/kg for 15 days in STZ-induced diabetic Wistar rats showed a significant decrease in MDA formation in the pancreas (p < 0.001). The same study revealed a significant increase in GSH (p < 0.001) and the activity of GPx (p < 0.001), GR (p < 0.001), SOD (p < 0.001), CAT (p < 0.001), and PON1 (p < 0.001) in the pancreas concomitant with decreased protein oxidation and lipid peroxidation. Some of the findings were observed in mice models of diabetes. For instance, oral administration of 0.35 mmol of pomegranate for four months significantly increased PON1 gene expression (p < 0.05) and its activity in STZ-induced diabetes in mice fed an HFD [55]. A different mice strain (Kunming) with diabetes induced by STZ demonstrated a significant increase in AOC (p < 0.01), GSH (p < 0.01), and T-AOC (p < 0.01) when treated with a 400 mg/kg pomegranate dose for four weeks [22]. Interestingly, Balb/C mice with STZ-induced diabetes, when treated with pomegranate, revealed a significant decrease in macrophage peroxides (p < 0.05) concomitant with increased macrophagic GSH (p < 0.05) [52]. More recently, in HFD-STZ-induced diabetic C57BL/6 mice, administration of 20 mg/kg of punicalagin for eight weeks significantly decreased MDA (p < 0.01) and free fatty acid (FFA) levels (1147.2 ± 89.3 µmol/L compared to 1351.8 ± 91.6 µmol/L, p < 0.05) concomitant with increased total-superoxide dismutase (T-SOD) activity in the liver (p < 0.01). Surprisingly, this study showed no significant changes in serum T-SOD activity (p > 0.05) [34]. These findings collectively demonstrate the potential of pomegranate and its derivatives in reducing oxidative stress in rodent models of diabetes.
The effect of pomegranate on markers of endothelial function in diabetic patients.
Endothelial dysfunction contributes to the development of CVD. This study focused on sICAM-1 and sVCAM-1 from clinical trials. Our evidence in clinical trials showed conflicting findings on endothelial function following treatment with 250 mL of pomegranate oil in diabetes [65]. For instance, we observed a significant decrease in sICAM-1 levels from baseline (151 ± 17 ng/mL) to post treatment (138 ± 12 ng/mL, p < 0.001) and a decrease in sE-selectin levels from 19 ± 7 ng/mL to 13 ± 6 ng/mL post treatment (p < 0.001). However, there was no significant difference in sVCAM-1 levels: 27 ± 11 ng/mL compared to 31 ± 19 ng/mL (p > 0.05).
The effect of pomegranate and its derivatives on markers of inflammation in diabetic patients.
Inflammation is implicated in the development and progression of diabetes, especially T2D. Diabetes and inflammation have a complex relationship that involves several cellular and molecular pathways. Some implicated mechanisms include inflammatory pathways such as the activation of nuclear factor-kappa-beta (NF-κβ) [85]. Various inflammatory markers, such as TNF-α, IL-6, CRP, and NF-κβ, are evaluated to assess inflammation and serve as targets for potential therapies [85,86]. In the current review, evidence from clinical studies showed a significant decrease in the circulating levels of CRP (p < 0.05), IL-6 (p < 0.01), and TNF-α (p < 0.01) in diabetic patients on 8-week treatment with 500 mg of pomegranate peel extract [67]. Similar results were reported by a study conducted in Iran, where 12 weeks of 250 mL of PJ significantly decreased plasma hs-CRP (baseline: 3243 ± 2935 ng/mL compared to post treatment: 1791 ± 1657 ng/mL, p < 0.05) and IL-6 (10.9 ± 4.4 ng/L compared to 7.1 ± 5.6 ng/L, p < 0.05) [62]. Furthermore, this study showed a significant decrease in TNF-α between the baseline (37.0 ± 19.3 ng/L) and post-treatment (30.4 ± 17.5 ng/L) levels, p < 0.01. Consistently, PSO at a dose of 3g for eight weeks significantly reduced IL-6 (before treatment: 5.2 ± 2.2 pmol/mL compared to after treatment: 4.5 ± 1.9 pmol/mL, p = 0003) and TNF-α (before treatment: 9.2 ± 4.1 pmol/mL compared to after: 7.7 ± 2.4 pmol/mL, p = 0.028) in T2D patients. However, no significant differences were observed in the serum levels of hs-CRP (before: 1.4 ± 1.8 pg/mL compared to after: 0.9 ± 0.6 pg/mL, p = 0.11) [63]. Similar findings were acknowledged in a quasi-experimental design [61] that used concentrated PJ (50 g) for four weeks and observed a significant decrease in IL-6 levels from baseline (31.12 ± 3.12 pg/mL) to post treatment (23.40 ± 2.27 pg/mL, p = 0.04). Surprisingly, no statistically significant differences were observed in the levels of TNF-α (baseline: 18.72 ± 0.95 pg/mL compared to post treatment: 17.66 ± 1.41 pg/mL, p = 0.42) and CRP (2.37 ± 0.24 ng/ML compared to 2.44 ± 0.23 ng/ML, p = 0.74). Likewise, administering 250 mL of PJ for 12 weeks in diabetic patients showed no significant effect on NF-κβ [65]. Although these findings revealed some contradictory reports, the gathered evidence suggests that pomegranate and its derivatives may have the potential to modulate inflammation by reducing markers associated with inflammation in diabetic patients.
The effect of pomegranate and its derivatives on markers of oxidative stress in diabetic patients.
Oxidative stress plays an important role in the development and progression of both T1D and T2D due to the accumulation of ROS [5]. The accumulation of ROS results in cell, tissue, and organ damage, thus predisposing them to oxidative stress [5]. Several treatment strategies aim to target oxidative stress to minimize associated complications. In this review, we focused on the effect of pomegranate on various markers of oxidative stress, including MDA, SOD, CAT, and AOC, as presented in Table 2. The overall evidence gathered from clinical studies revealed that pomegranate exerts an antioxidant effect in patients with diabetes (Table 2). For instance, a study by Rosenblat et al. [29] showed that 50 mL of pomegranate juice administered for three months significantly decreased serum oxidative stress. Consistently, this was associated with lower lipid peroxide (p < 0.01) and TBARS levels (p < 0.05) and an increase in PON1 arylesterase (p < 0.05) activity. Furthermore, the study reported an increase in GSH levels (p < 0.05), concomitant with a decrease in ox-LDL uptake (p < 0.05), following pomegranate juice treatment.
Interestingly these findings were supported by Sohrab et al. [25], who reported a significant decrease in ox-LDL, increased serum TAC, and higher arylesterase activity of PON1. Partial confirmation of these results was also observed by [28], who reported increased PON1 arylesterase activity (p < 0.05). Similarly, administering 500 mg of pomegranate for three months significantly decreased MDA levels (−0.57 ± 0.55 µmol/L compared to 0.37 ± 0.48 µmol/L, p < 0.001) and improved antioxidant defense by increasing total plasma GSH (761.86 ± 652.71 µmol/L compared to 202.11 ± 390.76 µmol/L, p < 0.001) and AOC (0.45 ± 0.62 mmol/L compared to −0.09 ± 0.28 mmol/L, p < 0.001) [66]. These results are supported by a quasi-experimental study, as 200 mL of PJ in T2D for six weeks significantly increased PON1 (135.02 ± 104.14 μmol/L compared to 225.18 ± 149.52 μmol/L, p < 0.001) and arylesterase activity (165.02 ± 56.63 μmol/L compared 246.36 ± 49.26 μmol/L, p < 0.001), concomitant with decreasing the levels of MDA (0.073 ± 0.046 μmol/L compared to 0.029 ± 0.021 μmol/L, p < 0.001) [30]. More recently, Grabez et al. [67] demonstrated that 500 mg of pomegranate peel extract daily for eight weeks significantly ameliorated oxidative stress by reducing TBARS (baseline: 1.60 ± 0.29 µmol/mL compared to post treatment: 0.38 ± 0.15 µmol/mL, p < 0.001), nitrites (NO2−) (14.04 ± 2.17 nmol/mL versus 6.95 ± 1.94 nmol/mL, p < 0.001), and superoxide anion radical (O2−) (5.81 ± 1.09 nmol/mL compared to 3.19 ± 1.40 nmol/mL, p < 0.001). Moreover, the same trial showed a significant increase in TAC within the group, indicating improved antioxidant status (baseline: 149.93 ± 69.00 µmol/L versus post treatment: 230.81 ± 84.72 µmol/L, p < 0.05). Consistent findings were observed when 50 mL of PJ was administered for 12 weeks, as it was associated with a significant increase in TAC (22.89 ± 6.4 U/mL compared to 27.49 ± 6.8 U/mL, p < 0.001) and a decrease in MDA (7.69 ± 1.9 µmol/L compared to 5.79 ± 2.1 µmol/L, p < 0.0001) levels [26]. In addition, 150 mL of pomegranate extract for six weeks in T2D significantly increased the levels of GPx (414.78 ± 71.10 U/mL compared to 746.88 ± 90.24 U/L), SOD (176.50 ± 28.72 U/mL compared to 218.13 ± 22.02 U/mL), plasma GSH (5.88 ± 3.13 µmole/L compared to 10.63 ± 2.26 µmole/L), and TAC (498.75 ± 118.61 µmole/L compared to 664.37 ± 125.62 µmole/L) [64]. A quasi-experimental report also showed that administering 50 g of concentrated PJ for six weeks could increase TAC significantly (baseline: 381.88 ± 20.54 µm/L compared to post treatment: 1501 ± 146.90 µm/L, p < 0.001) [61]. Finally, Rock et al. [60] reported that 50 mL/day of pomegranate juice significantly decreased TBARS levels (p < 0.05), while 5 mL/day of pomegranate polyphenol extract for six weeks increased thiol level (p < 0.05), representing the serum’s AOC.
The gathered evidence suggests the potential effects of pomegranate and its derivatives in reducing oxidative stress in diabetic patients. These effects include reduced lipid peroxidation, increased antioxidant enzyme activity, improved glutathione levels, and enhanced TAC. To completely understand the underlying mechanisms and identify the ideal dosage and duration of pomegranate supplementation for efficient therapy for the management of oxidative stress, further research is required.
4. Discussion
Our systematic review is composed of 33 preclinical and 13 clinical studies. Indeed, more evidence supports using pomegranate as an antioxidant and anti-inflammatory agent, showing the benefits of improving endothelial function. Although there was no uniform evaluation of the same markers for all these parameters, the evidence gathered in this study suggests that pomegranate can ameliorate oxidative stress, inflammation, and endothelial dysfunction in diabetes. However, its mechanisms of action are still not well documented. When significant focus was placed on the effect of pomegranate on oxidative stress in rodent models of diabetes, a few markers that were considered included MDA, SOD, CAT, TBARS, GSH, GPx, TAC/AOC, ROS, PON1, FFA, and lipid peroxidation. Due to a physiological imbalance or condition, a decline in the activity of antioxidant enzymes such as GSH, SOD, CAT, and GPx enhances the vulnerability to oxidative stress.
In our review, extensive evidence from preclinical studies suggests that pomegranate extracts and their derivatives are good sources of antioxidant activity. This has been revealed by multiple rodent studies. These studies demonstrated a significant increase in the activity of antioxidant enzymes such as GSH [22,24,36,38,41,44,46,47,52,53,57], GPx [20,36,47,49,53], CAT [16,24,36,37,38,42,45,46,47,48,49,56], SOD [16,20,24,34,38,39,42,45,46,47,48,49,53,56,58], PON1 [53,55], and TAC [16,22,38,39,41]. Likewise, clinical evidence in diabetic patients who were treated with pomegranate revealed an increase in the activity of antioxidant enzymes, including GSH [29,64,66], GPx [64], PON1 [25,28,29,30], and TAC [25,26,60,61,64,66,67]. The improved activity of antioxidant enzymes supports pomegranate as an antioxidant in diabetes. The overall evidence indicates that pomegranate treatment leads to an elevation in PON1 levels in diabetes, further supporting the potential of pomegranate as an anti-oxidative agent. These effects are attributed to its high anthocyanin, ellagic acid, and PU content, which help counteract excessive ROS levels [60]. Therefore, this high content of secondary active compounds promotes the beneficial impact of pomegranate in diabetes in relation to oxidative stress. It is noteworthy that PON1 contributes to the prevention of secondary complications in diabetes, such as atherosclerosis, by hydrolyzing ox-LDL and fatty acids in the blood [87]. While such evidence is acknowledged, a contrasting report by El-Mansi et al. [56] observed a significant decrease in the activity of an antioxidant, GPx, following pomegranate treatment in diabetic rat embryos and their mothers. However, this might be due to the status of these animal models. On the other hand, Çukurova et al. [58] showed no effect of 2.5 mL of pomegranate on GSH in diabetic Sprague Dawley rats.
MDA levels were reduced in several preclinical studies [16,19,20,23,34,36,37,38,39,41,42,43,45,46,47,51,56]. Interestingly, similar findings were observed in clinical studies, as shown by a decrease in MDA levels [26,30,53,66]. Another biomarker of oxidative stress that was evaluated included TBARS. This takes into account the level of LPO degradation products in cells and tissues. In fact, diabetes is associated with increased TBARS, thus indicating increased LPO and further oxidative stress [88]. Therefore, it is imperative that LPO be inhibited in diabetes in order to alleviate oxidative stress. In the current review, TBARS levels were decreased in preclinical and clinical studies following pomegranate treatment in diabetes [24,29,47,48,60,67]. This shows the potential of pomegranate as an anti-oxidative agent in the state of diabetes.
Moreover, pomegranate treatment has been shown to alleviate oxidative stress by neutralizing ROS [21] and preventing LPO [43,53]. This beneficial effect can be explained, at least in part, by the high content of anthocyanins and ellagic acid in pomegranate (Figure 4). Likewise, pomegranate inhibits LPO, thus reducing MDA production and mitigating oxidative damage [21].
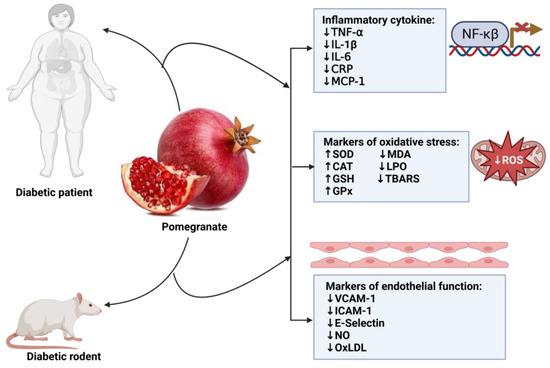
Figure 4.
Overview of the impact of pomegranate on inflammation, oxidative stress, and endothelial function in diabetes. TNF-α: tumor necrosis factor-alpha; IL-1β: interleukin-1 beta; IL-6: interleukin-6; CRP: C-reactive protein; MCP-1: monocyte chemoattractant protein-1; SOD: superoxide dismutase; CAT: catalase; GSH: glutathione; GPx: glutathione peroxide; MDA: malondialdehyde; LPO: lipid peroxidation; TBARS: thiobarbituric acid reactive substances; VCAM-1 vascular cell adhesion molecule-1; ICAM-1: intercellular adhesion molecule-1; NO: nitric oxide; oxLDL: oxidized low-density lipoprotein.
All of these findings support the use of pomegranate as an anti-oxidative agent, as evidenced by its ameliorative effect on the various markers of oxidative stress. The antioxidant compounds in pomegranate include anthocyanins and ellagic acid [89,90,91], which ameliorate oxidative stress in diabetes. A few studies suggest that anthocyanins, ellagic acid, and PU mediate pomegranate’s anti-oxidative stress effects by degrading and scavenging free radicals [42,92,93,94,95,96].
We found that in rodent models of diabetes, various markers of inflammation were assessed. After treatment with pomegranate, these markers were remarkably decreased. Some of these markers included TNF-α [35,41,42,54], IL-6 [41,42,56], IL-1β [35,42,43,54,56], NF-κβ [44,54], MCP-1 [35], and CRP [53]. Similarly, in clinical studies, we found that the administration of pomegranate decreased TNF-α [62,63,67], IL-6 [61,62,63,67], and CRP [62,67]. Although the results from preclinical have been replicated in clinical trials, there are still some inconsistencies in inflammation, as reported by other researchers. For instance, no significant effect of pomegranate was observed on TNF-α [61,62], CRP [61], hsCRP [63], and NF-κβ [65] in clinical studies. This points out the limitation of this fruit as an anti-inflammatory agent; however, some reasons may be due to the preparation of the plant extract, part of fruit used, dosage, and the stage of diabetes. Some of the modes of action of pomegranate in the amelioration of inflammation are mediated by anthocyanins, which inhibit the cyclooxygenase (COX), NF-κβ activity, and phosphorylation of mitogen-activated protein kinase (MAPK) proteins while inducing nitric oxide (NO) expression [97,98,99]. Regarding endothelial function, a few preclinical studies have shown reduced levels of the following endothelial markers: VCAM-1 [53], ICAM-1 [53], E-selectin [53], ET-1 [56], eNOS [58], and NO bioavailability [36,39,41]. Similarly, sICAM-1 and sE-selectin were also reduced without any effect on sVCAM-1 [65]. Reduced markers of endothelial function following pomegranate treatment in diabetes support its use as an agent to improve endothelial function in diabetes. One mechanism by which pomegranates enhance endothelial function is by reducing oxLDL levels [25].
This is partly because the accumulation of ox-LDL is associated with endothelial dysfunction and the development of atherosclerosis [100]. Therefore, our results show that pomegranate may preserve healthy endothelial function by preventing LDL oxidation. In clinical studies, there have been contradictory findings on oxLDL following pomegranate treatment. On the other hand, in a study, pomegranate showed no effect on eitheriNOS and eNOS [19]. For example, a report by Rosenblat [29] indicated an increase in oxLDL, whereas Sohrab [25] reported a decrease in oxLDL. Oxidized LDL impairs endothelial function and vascular health, forming foam cells and atherosclerotic plaques. This in turn may lead individuals to develop secondary complications. Due to these controversies, further research is required to better understand the effects of pomegranate treatment in diabetes on endothelial functions.
Although the current review has shown some of the potential benefits of pomegranate in diabetes, it is important to consider some of the following limitations. Firstly, most of the included studies were conducted in Asia, which comprises countries known to be major pomegranate-producing countries. Secondly, the diabetic rodent models presented in this study were induced through the administration of STZ or alloxan, causing T1D, unlike T2D observed in humans (as shown in Table 2). As a result, the physiological pathways leading to oxidative stress, endothelial function, and inflammation may differ between the two conditions, affecting how pomegranate regulates them. Additionally, the method of administration of pomegranate, especially in rodents, varied from different studies, with some using powder in their diet, such as pomegranate juice, while others prepared extracts from fruit peel and seeds. These differences in administration could contribute to conflicting findings across the studies.
Moreover, the human studies also employed different methods and doses, which led to contradicting results. For instance, some studies used pomegranate juice, while others used powdered pomegranate at varying doses. These variations in the approaches used further complicate the interpretation of the results. Amongst the strengths of the current review is the inclusion of evidence from preclinical studies and clinical trials. Evaluation of various treatment regimens also allows us to find a possible effective and safe dose. The stringent eligibility criteria, selection, and multiple database searches strengthened our review.
5. Conclusions
Based on a thorough examination of the various studies in this review, a comprehensive body of research consisting of 33 preclinical and 13 clinical studies involving 468 patients with T2D suggests that pomegranate shows promising results as a potential agent for improving oxidative stress, inflammation, and endothelial dysfunction in diabetes. Although these benefits have been acknowledged in both preclinical and clinical studies, there is limited evidence regarding endothelial function, particularly in clinical studies, which necessitates further investigation, particularly in diabetes. Additionally, it is worth noting that the clinical evidence presented in this study was based on small sample sizes ranging from 10 to 60 T2D patients, indicating that these trials may have been insufficiently powered. Therefore, based on this observation, we recommend conducting future clinical trials with larger sample sizes to gain a better understanding of the underlying mechanisms through which pomegranate exerts its effects and to determine the optimal dosage and duration of pomegranate treatment that can be used to achieve optimal anti-inflammatory and anti-oxidative benefits.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/antiox12081566/s1. Table S1: Search on Scopus for oxidative stress; Table S2: Search on Scopus for endothelial function; Table S3: Search on Scopus for inflammation; Table S4: Search on PubMed for oxidative stress; Table S5: Seach on PubMed for inflammation; Table S6: Search on PubMed for endothelial function.
Author Contributions
Conceptualization, K.M. and S.L.L.; methodology, K.M., S.D., W.N.P. and P.M; software, K.M.; validation, K.M., S.D., W.N.P., P.M. and S.L.L.; formal analysis, K.M.; investigation, K.M.; resources, K.M. and S.L.L.; data curation, K.M., S.D. and W.N.P.; funding, K.M.; writing—original draft preparation, K.M.; writing—review and editing, K.M., S.D., W.N.P., S.L.L. and P.M.; supervision, S.L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by Research Development Grants for nGAP Scholars (reference number NGAP23022780506) and the Research Excellence Award for Next Generation Researchers: NONF230515106418. The content herein is the sole responsibility of the authors and does not necessarily represent the official views of the National Research Foundation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
All figures were generated by KM using Biorender. W.N.P is currently funded by the University of South Africa Women in Research (WiR of 2023), which forms part of wider research funding under “the use and functional properties of African indigenous fruits and vegetables in alleviating household food and nutrition insecurity for local communities”. The content herein is the sole responsibility of the authors and does not necessarily represent the official views of the funders.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
DM: diabetes mellitus; T2D: type 2 diabetes; STZ: streptozotocin; NAD: nicotinamide; TNF-α: tumor necrosis factor-alpha; IL-1β: interleukin-1 beta; IL-6: interleukin-6; CVD: cardiovascular disease; ROS: reactive oxygen species; PON1: paraoxonase-1; FFA: free fatty acid; LDL: low density lipoprotein; CRP: C-reactive protein; MCP-1: monocyte chemoattractant protein-1; SOD: superoxide dismutase; CAT: catalase; GSH: glutathione; GPx: glutathione peroxide; MDA: malondialdehyde; LPO: lipid peroxidation; TBARS: thiobarbituric acid reactive substances; VCAM-1: vascular cell adhesion molecule-1; sVCAM-1: soluble vascular cell adhesion molecules-1; ICAM-1: intercellular adhesion molecule-1; sICAM-1: soluble intercellular adhesion molecule-1; NOx: NADPH oxidase; NO: nitric oxide; oxLDL: oxidized low-density lipoprotein; COX: cyclooxygenase; AGEs: advanced glycation end product; IKK: inhibitor of nuclear factor-κ; NF-κβ: nuclear factor kappa β; ROS: reactive oxygen species; oxLDL: oxidized lipoprotein; PKA: protein kinase; PSE: pomegranate peel extract; TAC: total antioxidant capacity; PJ: pomegranate juice; MAPK: mitogen-activated protein kinase; ET-1: endothelin-1; eNOS: endothelial nitric oxide synthase; iNOS: inducible nitric oxide synthase; PoPEx: pomegranate peel extract; PSO: pomegranate seed oil; NO2−: nitrites; WPOMx1: Wonderful variety of pomegranate polyphenol extract; PPE: pomegranate peel extract; PHE: pomegranate hexane extracts; PAJ: pomegranate aril juice; PU: punicalagin; IDDM: insulin-dependent diabetes mellitus; SGLT2: sodium-glucose cotransporter-2; WHO: world health organization; TCAM: traditional, complementary, and alternative medicines; IDF: International Diabetes Federation.
References
- World Health Organisation. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 29 April 2023).
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Oguntibeju, O.O. Type 2 Diabetes Mellitus, Oxidative Stress and Inflammation: Examining the Links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar] [PubMed]
- Baig, S.; Shabeer, M.; Parvaresh Rizi, E.; Agarwal, M.; Lee, M.H.; Ooi, D.S.Q.; Chia, C.; Aung, N.; Ng, G.; Teo, Y.; et al. Heredity of Type 2 Diabetes Confers Increased Susceptibility to Oxidative Stress and Inflammation. BMJ Open Diabetes Res. Care 2020, 8, e000945. [Google Scholar] [CrossRef] [PubMed]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Chaudhury, A.; Duvoor, C.; Reddy Dendi, V.S.; Kraleti, S.; Chada, A.; Ravilla, R.; Marco, A.; Shekhawat, N.S.; Montales, M.T.; Kuriakose, K.; et al. Clinical Review of Antidiabetic Drugs: Implications for Type 2 Diabetes Mellitus Management. Front. Endocrinol. 2017, 8, 6. [Google Scholar] [CrossRef]
- Padhi, S.; Nayak, A.K.; Behera, A. Type II Diabetes Mellitus: A Review on Recent Drug Based Therapeutics. Biomed. Pharmacother. 2020, 131, 110708. [Google Scholar] [CrossRef]
- Stumvoll, M.; Häring, H.U. Glitazones: Clinical Effects and Molecular Mechanisms. Ann. Med. 2002, 34, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Lebovitz, H.E. Thiazolidinediones: The Forgotten Diabetes Medications. Curr. Diabetes Rep. 2019, 19, 151. [Google Scholar] [CrossRef]
- WHO. Supports Scientifically-Proven Traditional Medicine. Available online: https://www.afro.who.int/news/who-supports-scientifically-proven-traditional-medicine (accessed on 3 April 2023).
- Cock, I.E.; Ndlovu, N.; Van Vuuren, S.F. The Use of South African Botanical Species for the Control of Blood Sugar. J. Ethnopharmacol. 2021, 264, 113234. [Google Scholar] [CrossRef] [PubMed]
- Mokgalaboni, K.; Phoswa, W.N. Corchorus Olitorius Extract Exhibit Anti-Hyperglycemic and Anti-Inflammatory Properties in Rodent Models of Obesity and Diabetes Mellitus. Front. Nutr. 2023, 10, 1099880. [Google Scholar] [CrossRef]
- Fahmy, H.; Hegazi, N.; El-Shamy, S.; Farag, M.A. Pomegranate Juice as a Functional Food: A Comprehensive Review of Its Polyphenols, Therapeutic Merits, and Recent Patents. Food Funct. 2020, 11, 5768–5781. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Barman, S. Antidiabetic and Antihyperlipidemic Effects of Ethanolic Extract of Leaves of Punica granatum in Alloxan-Induced Non-Insulin-Dependent Diabetes Mellitus Albino Rats. Indian J. Pharmacol. 2012, 42, 219–224. [Google Scholar] [CrossRef]
- Venkitasamy, C.; Zhao, L.; Zhang, R.; Pan, Z. Pomegranate. In Integrated Processing Technologies for Food and Agricultural By-Products; Elsevier: Amsterdam, The Netherlands, 2019; pp. 181–216. ISBN 9780128141397. [Google Scholar]
- Aboonabi, A.; Rahmat, A.; Othman, F. Antioxidant Effect of Pomegranate against Streptozotocin-Nicotinamide Generated Oxidative Stress Induced Diabetic Rats. Toxicol. Rep. 2014, 1, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Amri, Z.; Ben Khedher, M.R.; Zaibi, M.S.; Kharroubi, W.; Turki, M.; Ayadi, F.; Hammami, M. Anti-Diabetic Effects of Pomegranate Extracts in Long-Term High Fructose-Fat Fed Rats. Clin. Phytoscience 2020, 6, 55. [Google Scholar] [CrossRef]
- Sun, W.; Yan, C.; Frost, B.; Wang, X.; Hou, C.; Zeng, M.; Gao, H.; Kang, Y.; Liu, J. Pomegranate Extract Decreases Oxidative Stress and Alleviates Mitochondrial Impairment by Activating AMPK-Nrf2 in Hypothalamic Paraventricular Nucleus of Spontaneously Hypertensive Rats. Sci. Rep. 2016, 6, srep34246. [Google Scholar] [CrossRef]
- Onal, E.; Yilmaz, D.; Kaya, E.; Bastaskin, T.; Bayatli, N.; Gur, S. Pomegranate Juice Causes a Partial Improvement through Lowering Oxidative Stress for Erectile Dysfunction in Streptozotocin-Diabetic Rat. Int. J. Impot. Res. 2016, 28, 234–240. [Google Scholar] [CrossRef]
- Bagheri, S.; Khorramabadi, R.M.; Assadollahi, V.; Khosravi, P.; Cheraghi Venol, A.; Veiskerami, S.; Ahmadvand, H. The Effects of Pomegranate Peel Extract on the Gene Expressions of Antioxidant Enzymes in a Rat Model of Alloxan-Induced Diabetes. Arch. Physiol. Biochem. 2021, 129, 870–878. [Google Scholar] [CrossRef]
- Tugcu, B.; Nacaroglu, S.A.; Gedikbasi, A.; Uhri, M.; Acar, N.; Ozdemir, H. Protective Effect of Pomegranate Juice on Retinal Oxidative Stress in Streptozotocin-Induced Diabetic Rats. Int. J. Ophthalmol. 2017, 10, 1662–1668. [Google Scholar] [CrossRef]
- Wang, J.Y.; Zhu, C.; Qian, T.W.; Guo, H.; Wang, D.D.; Zhang, F.; Yin, X. Extracts of Black Bean Peel and Pomegranate Peel Ameliorate Oxidative Stress-Induced Hyperglycemia in Mice. Exp. Ther. Med. 2015, 9, 43–48. [Google Scholar] [CrossRef]
- Mollazadeh, H.; Sadeghnia, H.R.; Hoseini, A.; Farzadnia, M.; Boroushaki, M.T. Effects of Pomegranate Seed Oil on Oxidative Stress Markers, Serum Biochemical Parameters and Pathological Findings in Kidney and Heart of Streptozotocin-Induced Diabetic Rats. Ren. Fail. 2016, 38, 1256–1266. [Google Scholar] [CrossRef]
- Mohan, M.; Waghulde, H.; Kasture, S. Effect of Pomegranate Juice on Angiotensin II-Induced Hypertension in Diabetic Wistar Rats. Phytother. Res. 2010, 24, S196–S203. [Google Scholar] [CrossRef]
- Sohrab, G.; Ebrahimof, S.; Sotoudeh, G.; Neyestani, T.R.; Angoorani, P.; Hedayati, M.; Siasi, F. Effects of Pomegranate Juice Consumption on Oxidative Stress in Patients with Type 2 Diabetes: A Single-Blind, Randomized Clinical Trial. Int. J. Food Sci. Nutr. 2017, 68, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Sohrab, G.; Angoorani, P.; Tohidi, M.; Tabibi, H.; Kimiagar, M.; Nasrollahzadeh, J. Pomegranate (Punicagranatum) Juice Decreases Lipid Peroxidation, but Has No Effect on Plasma Advanced Glycated End-Products in Adults with Type 2 Diabetes: A Randomized Double-Blind Clinical Trial. Food Nutr. Res. 2015, 59, 28551. [Google Scholar] [CrossRef] [PubMed]
- Jandari, S.; Hatami, E.; Ziaei, R.; Ghavami, A.; Yamchi, A.M. The Effect of Pomegranate (Punica granatum) Supplementation on Metabolic Status in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2020, 52, 102478. [Google Scholar] [CrossRef]
- Fuhrman, B.; Volkova, N.; Aviram, M. Pomegranate Juice Polyphenols Increase Recombinant Paraoxonase-1 Binding to High-Density Lipoprotein: Studies in Vitro and in Diabetic Patients. Nutrition 2010, 26, 359–366. [Google Scholar] [CrossRef]
- Rosenblat, M.; Hayek, T.; Aviram, M. Anti-Oxidative Effects of Pomegranate Juice (PJ) Consumption by Diabetic Patients on Serum and on Macrophages. Atherosclerosis 2006, 187, 363–371. [Google Scholar] [CrossRef]
- Parsaeyan, N.; Mozaffari-Khosravi, H.; Mozayan, M.R. Effect of Pomegranate Juice on Paraoxonase Enzyme Activity in Patients with Type 2 Diabetes. J. Diabetes Metab. Disord. 2012, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Q.; Hou, H.; Liu, Z.; Wang, L.; Rasekhmagham, R.; Kord-Varkaneh, H.; Santos, H.O.; Yao, G. The Effects of Pomegranate Supplementation on Biomarkers of Inflammation and Endothelial Dysfunction: A Meta-Analysis and Systematic Review. Complement. Ther. Med. 2020, 49, 102358. [Google Scholar] [CrossRef]
- Morvaridzadeh, M.; Sepidarkish, M.; Daneshzad, E.; Akbari, A.; Mobini, G.R.; Heshmati, J. The Effect of Pomegranate on Oxidative Stress Parameters: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2020, 48, 102252. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, X.; Cao, Y.; An, X.; Chen, J.; Yang, L. Punicalagin Protects against Diabetic Liver Injury by Upregulating Mitophagy and Antioxidant Enzyme Activities. Nutrients 2022, 14, 2782. [Google Scholar] [CrossRef] [PubMed]
- Jin, D.; Zhang, B.; Li, Q.; Tu, J.; Zhou, B. Effect of Punicalagin on Multiple Targets in Streptozotocin/High-Fat Diet-Induced Diabetic Mice. Food Funct. 2020, 11, 10617–10634. [Google Scholar] [CrossRef]
- El-Beih, N.M.; Ramadan, G.; El-Husseiny, E.A.; Hussein, A.M. Effects of Pomegranate Aril Juice and Its Punicalagin on Some Key Regulators of Insulin Resistance and Oxidative Liver Injury in Streptozotocin-Nicotinamide Type 2 Diabetic Rats. Mol. Biol. Rep. 2019, 46, 3701–3711. [Google Scholar] [CrossRef] [PubMed]
- Mabrouk Gabr, N. Effects of Pomegranate (Punica granatum L.) Fresh Juice and Peel Extract on Diabetic Male Albino Rats. Al-Azhar Med. J. 2017, 46, 965–980. [Google Scholar] [CrossRef]
- Mosaoa, R.M.; Yaghmoor, S.S.; Moselhy, S.S. Oxygen Scavenging, Anti-Inflammatory, and Antiglycation Activity of Pomegranate Flavonoids (Punica granum) against Streptozotocin Toxicity Induced Diabetic Nephropathy in Rats. Environ. Sci. Pollut. Res. 2023, 30, 16687–16693. [Google Scholar] [CrossRef] [PubMed]
- Saad, E.A.; Hassanien, M.; Elhagrasy, M.; Saad, E.A.; Hassanien, M.M.; El-Hagrasy, M.A.; Radwan, K.H. Antidiabetic, Hypolipidemic and Antioxidant Activities and Protective Effects of Punica granatum Peels Powder against Pancreatic and Hepatic Tissues Injuries in Streptozotocin Induced IDDM in Rats. Int. J. Pharm. Pharm. Sci. 2015, 7, 397–402. [Google Scholar]
- Osman, H.F.; Eshak, M.G.; El-Sherbiny, M.; Bayoumi, M.M.; Hala; Osman, F. Biochemical and Genetical Evaluation of Pomegranate Impact on Diabetes Mellitus Induced by Alloxan in Female Rats Genetical Evaluation of Pomegranate Impact on Diabetes Mellitus Induced by Alloxan in Female Rats. Life Sci. J. 2012, 9, 1543–1553. [Google Scholar]
- El Deeb, K.S.; Eid, H.H.; Ali, Z.Y.; Shams, M.M.; Elfiky, A.M. Bioassay-Guided Fractionation and Identification of Antidiabetic Compounds from the Rind of Punica granatum Var. Nana. Nat. Prod. Res. 2021, 35, 2103–2106. [Google Scholar] [CrossRef]
- El-Missiry, M.A.; Amer, M.A.; Hemieda, F.A.E.; Othman, A.I.; Sakr, D.A.; Abdulhadi, H.L. Cardioameliorative Effect of Punicalagin against Streptozotocin-Induced Apoptosis, Redox Imbalance, Metabolic Changes and Inflammation. Egypt. J. Basic Appl. Sci. 2015, 2, 247–260. [Google Scholar] [CrossRef]
- Abo-Saif, M.A.; Ragab, A.E.; Ibrahim, A.O.; Abdelzaher, O.F.; Mehanyd, A.B.M.; Saber-Ayad, M.; El-Feky, O.A. Pomegranate Peel Extract Protects against the Development of Diabetic Cardiomyopathy in Rats by Inhibiting Pyroptosis and Downregulating LncRNA-MALAT1. Front. Pharmacol. 2023, 14, 1166653. [Google Scholar] [CrossRef]
- Shaker, O.G.; Sourour, D.A. Protective Effects of Pomegranate Seed Extract on Streptozotocin-Induced β-Cell Damage in Rats: Inhibition of Pancreatic Nuclear Factor Kappa Beta, Transforming Growth Factor Beta and Matrix Metalloproteinase-2 Genes Expression. Int. J. Adv. Res. 2013, 1, 88–102. [Google Scholar]
- Patel, A.N.; Bandawane, D.D.; Mhetre, N.K. Pomegranate (Punica granatum Linn.) Leaves Attenuate Disturbed Glucose Homeostasis and Hyperglycemia Mediated Hyperlipidemia and Oxidative Stress in Streptozotocin Induced Diabetic Rats. Eur. J. Integr. Med. 2014, 6, 307–321. [Google Scholar] [CrossRef]
- Ankita, P.; Deepti, B.; Nilam, M. Flavonoid Rich Fraction of Punica granatum Improves Early Diabetic Nephropathy by Ameliorating Proteinuria and Disturbed Glucose Homeostasis in Experimental Animals. Pharm. Biol. 2015, 53, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Bagri, P.; Ali, M.; Aeri, V.; Bhowmik, M.; Sultana, S. Antidiabetic Effect of Punica granatum Flowers: Effect on Hyperlipidemia, Pancreatic Cells Lipid Peroxidation and Antioxidant Enzymes in Experimental Diabetes. Food Chem. Toxicol. 2009, 47, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Salwe, K.J.; Sachdev, D.O.; Bahurupi, Y.; Kumarappan, M. Evaluation of Antidiabetic, Hypolipedimic and Antioxidant Activity of Hydroalcoholic Extract of Leaves and Fruit Peel of Punica granatum in Male Wistar Albino Rats. J. Nat. Sci. Biol. Med. 2015, 6, 56–62. [Google Scholar] [CrossRef]
- Mollazadeh, H.; Boroushaki, M.T.; Soukhtanloo, M.; Afshari, A.R.; Vahedi, M.M. Effects of Pomegranate Seed Oil on Oxidant/Antioxidant Balance in Heart and Kidney Homogenates and Mitochondria of Diabetic Rats and High Glucose-Treated H9c2 Cell Line. AJP 2017, 7, 317–333. [Google Scholar]
- Gharib, E.; Kouhsari, S.M.; Izad, M. Punica granatum L. Fruit Aqueous Extract Suppresses Reactive Oxygen Species-Mediated P53/P65/MiR-145 Expressions Followed by Elevated Levels of Irs-1 in Alloxan-Diabetic Rats. Cell J. 2018, 19, 520–527. [Google Scholar] [CrossRef]
- Prasetyastuti; Anthony, M.W.P.; Rahman, N.A.; Ngadikun; Sunarti. Hypoglycemic and Antioxidative Effects of Pomegranate (Punica granatum L.) Juice in Streptozotocin Induced Diabetic Rats. Pak. J. Nutr. 2014, 13, 567–572. [Google Scholar] [CrossRef]
- Rozenberg, O.; Howell, A.; Aviram, M. Pomegranate Juice Sugar Fraction Reduces Macrophage Oxidative State, Whereas White Grape Juice Sugar Fraction Increases It. Atherosclerosis 2006, 188, 68–76. [Google Scholar] [CrossRef]
- Abdulhadi, H.L.; Dabdoub, B.R.; Ali, L.H.; Othman, A.I.; Amer, M.E.; El-Missiry, M.A. Punicalagin Protects against the Development of Pancreatic Injury and Insulitis in Rats with Induced T1DM by Reducing Inflammation and Oxidative Stress. Mol. Cell Biochem. 2022, 477, 2817–2828. [Google Scholar] [CrossRef]
- Rouhi, S.Z.T.; Sarker, M.M.R.; Rahmat, A.; Alkahtani, S.A.; Othman, F. The Effect of Pomegranate Fresh Juice versus Pomegranate Seed Powder on Metabolic Indices, Lipid Profile, Inflammatory Biomarkers, and the Histopathology of Pancreatic Islets of Langerhans in Streptozotocin-Nicotinamide Induced Type 2 Diabetic Sprague-Dawley Rats. BMC Complement. Altern. Med. 2017, 17, 156. [Google Scholar] [CrossRef]
- Betanzos-Cabrera, G.; Guerrero-Solano, J.A.; Martínez-Pérez, M.M.; Calderón-Ramos, Z.G.; Belefant-Miller, H.; Cancino-Diaz, J.C. Pomegranate Juice Increases Levels of Paraoxonase1 (PON1) Expression and Enzymatic Activity in Streptozotocin-Induced Diabetic Mice Fed with a High-Fat Diet. Food Res. Int. 2011, 44, 1381–1385. [Google Scholar] [CrossRef]
- El-Mansi, A.A.; Al-Kahtani, M.A. Calcitriol and Punica granatum Extract Concomitantly Attenuate Cardiomyopathy of Diabetic Mother Rats and Their Neonates via Activation of Raf/MEK/ERK Signalling and Mitigation of Apoptotic Pathways. Folia Biol. 2019, 65, 70–87. [Google Scholar]
- Cambay, Z.; Baydas, G.; Tuzcu, M.; Bal, R. Pomegranate (Punica granatum L.) Flower Improves Learning and Memory Performances Impaired by Diabetes Mellitus in Rats. Acta Physiol. Hung. 2011, 98, 409–420. [Google Scholar] [CrossRef]
- Çukurova, Z.; Hergünsel, O.; Eren, G.; Gedikbaşi, A.; Uhri, M.; Demir, G.; Tekdöş, Y. The Effect of Pomegranate Juice on Diabetes-Related Oxidative Stress in Rat Lung. Turk. Klin. J. Med. Sci. 2012, 32, 444–452. [Google Scholar] [CrossRef]
- McFarlin, B.K.; Strohacker, K.A.; Kueht, M.L. Pomegranate Seed Oil Consumption during a Period of High-Fat Feeding Reduces Weight Gain and Reduces Type 2 Diabetes Risk in CD-1 Mice. Br. J. Nutr. 2009, 102, 54–59. [Google Scholar] [CrossRef]
- Rock, W.; Rosenblat, M.; Miller-Lotan, R.; Levy, A.P.; Elias, M.; Aviram, M. Consumption of Wonderful Variety Pomegranate Juice and Extract by Diabetic Patients Increases Paraoxonase 1 Association with High-Density Lipoprotein and Stimulates Its Catalytic Activities. J. Agric. Food Chem. 2008, 56, 8704–8713. [Google Scholar] [CrossRef]
- Shishehbor, F.; Shahi, M.M.; Zarei, M.; Saki, A.; Zakerkish, M.; Shirani, F.; Zare, M. Effects of Concentrated Pomegranate Juice on Subclinical Inflammation and Cardiometabolic Risk Factors for Type 2 Diabetes: A Quasi-Experimental Study. Int. J. Endocrinol. Metab. 2016, 14, e33835. [Google Scholar] [CrossRef]
- Sohrab, G.; Nasrollahzadeh, J.; Zand, H.; Amiri, Z.; Tohidi, M.; Kimiagar, M. Effects of Pomegranate Juice Consumption on Inflammatory Markers in Patients with Type 2 Diabetes: A Randomized, Placebo-Controlled Trial. J. Res. Med. Sci. 2014, 19, 215–220. [Google Scholar]
- Khajebishak, Y.; Payahoo, L.; Hamishehkar, H.; Alivand, M.; Alipour, M.; Solhi, M.; Alipour, B. Effect of Pomegranate Seed Oil on the Expression of PPAR-γ and pro-Inflammatory Biomarkers in Obese Type 2 Diabetic Patients. Nutr. Food Sci. 2019, 49, 854–865. [Google Scholar] [CrossRef]
- Yarmohammadi, M.; Mahjoub, S. Effects of Aerobic Exercise and Pomegranate Extract on Antioxidant Markers in Women Postmenopausal with Type 2 Diabetes. Hormozgan Med. J. 2017, 21, 129–137. [Google Scholar] [CrossRef]
- Sohrab, G.; Nasrollahzadeh, J.; Tohidi, M.; Zand, H.; Nikpayam, O. Pomegranate Juice Increases Sirtuin1 Protein in Peripheral Blood Mononuclear Cell from Patients with Type 2 Diabetes: A Randomized Placebo Controlled Clinical Trial. Metab. Syndr. Relat. Disord. 2018, 16, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Kutan Fenercioglu, A.; Saler, T.; Genc, E.; Sabuncu, H.; Altuntas, Y. The Effects of Polyphenol-Containing Antioxidants on Oxidative Stress and Lipid Peroxidation in Type 2 Diabetes Mellitus without Complications. J. Endocrinol. Investig. 2010, 33, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Grabež, M.; Škrbić, R.; Stojiljković, M.P.; Vučić, V.; Grujić, V.R.; Jakovljević, V.; Djuric, D.M.; Suručić, R.; Šavikin, K.; Bigović, D.; et al. A Prospective, Randomized, Double-Blind, Placebo-Controlled Trial of Polyphenols on the Outcomes of Inflammatory Factors and Oxidative Stress in Patients with Type 2 Diabetes Mellitus. Rev. Cardiovasc. Med. 2022, 23, 57. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.F.; Dowling, C.F. Pomegranate. Available online: https://www.worldcat.org/title/Fruits-of-warm-climates/oclc/16947184 (accessed on 28 May 2023).
- Mphahlele, R.R.; Fawole, O.A.; Mokwena, L.M.; Opara, U.L. Effect of Extraction Method on Chemical, Volatile Composition and Antioxidant Properties of Pomegranate Juice. South Afr. J. Bot. 2016, 103, 135–144. [Google Scholar] [CrossRef]
- Maphetu, N.; Unuofin, J.O.; Masuku, N.P.; Olisah, C.; Lebelo, S.L. Medicinal Uses, Pharmacological Activities, Phytochemistry, and the Molecular Mechanisms of Punica granatum L. (Pomegranate) Plant Extracts: A Review. Biomed. Pharmacother. 2022, 153, 113256. [Google Scholar] [CrossRef]
- Bhosle, V.K.; Altit, G.; Autmizguine, J.; Chemtob, S. Drugs That Cause Significant Displacement of Bilirubin from Albumin in Vitro. In Fetal and Neonatal Physiology, 2-Volume Set; Elsevier: Amsterdam, The Netherlands, 2017; pp. 187–201.e3. ISBN 9780323352147. [Google Scholar]
- Lipińska, L.; Klewicka, E.; Sójka, M. Structure, Occurrence and Biological Activity of Ellagitannins: A General Review. Acta Sci. Pol. Technol. Aliment. 2014, 13, 289–299. [Google Scholar] [CrossRef]
- Rippin; Beniwal, V.; Sharma, A.; Singh, B.J.; Ramniwas, S.; Sak, K.; Kumar, S.; Sharma, A.K. Ginnalin A and Hamamelitannin: The Unique Gallotannins with Promising Anti-Carcinogenic Potential. Explor. Target. Antitumor Ther. 2023, 4, 208–216. [Google Scholar] [CrossRef]
- Falcão, L.; Araújo, M.E.M. Tannins Characterisation in New and Historic Vegetable Tanned Leathers Fibres by Spot Tests. J. Cult. Herit. 2011, 12, 149–156. [Google Scholar] [CrossRef]
- He, H.F. Recognition of Gallotannins and the Physiological Activities: From Chemical View. Front. Nutr. 2022, 9, 888892. [Google Scholar] [CrossRef]
- Rozadi, N.; Oktavia, S.; Fauziah, F. Pharmacological Activities of Punicalagin: A Review. J. Drug Deliv. Ther. 2022, 12, 148–155. [Google Scholar] [CrossRef]
- Esposto, S.; Veneziani, G.; Taticchi, A.; Urbani, S.; Selvaggini, R.; Sordini, B.; Daidone, L.; Gironi, G.; Servili, M. Chemical Composition, Antioxidant Activity, and Sensory Characterization of Commercial Pomegranate Juices. Antioxidants 2021, 10, 1381. [Google Scholar] [CrossRef] [PubMed]
- Benchagra, L.; Berrougui, H.; Islam, M.O.; Ramchoun, M.; Boulbaroud, S.; Hajjaji, A.; Fulop, T.; Ferretti, G.; Khalil, A. Antioxidant Effect of Moroccan Pomegranate (Punica granatum L. Sefri Variety) Extracts Rich in Punicalagin against the Oxidative Stress Process. Foods 2021, 10, 2219. [Google Scholar] [CrossRef] [PubMed]
- Akhavan, H.; Barzegar, M.; Weidlich, H.; Zimmermann, B.F. Phenolic Compounds and Antioxidant Activity of Juices from Ten Iranian Pomegranate Cultivars Depend on Extraction. J. Chem. 2015, 2015, 907101. [Google Scholar] [CrossRef]
- Peng, Y. Comparative Analysis of the Biological Components of Pomegranate Seed from Different Cultivars. Int. J. Food Prop. 2019, 22, 784–794. [Google Scholar] [CrossRef]
- Elfalleh, W. Total Phenolic Contents and Antioxidant Activities of Pomegranate Peel, Seed, Leaf and Flower. J. Med. Plants Res. 2012, 6, 4724–4730. [Google Scholar] [CrossRef]
- Takeda, Y.; Matoba, K.; Sekiguchi, K.; Nagai, Y.; Yokota, T.; Utsunomiya, K.; Nishimura, R. Endothelial Dysfunction in Diabetes. Biomedicines 2020, 8, 182. [Google Scholar] [CrossRef]
- Du Plooy, C.S.; Martha Cornelia Mels, C.; Huisman, H.W.; Kruger, R. The Association of Endothelin-1 with Markers of Oxidative Stress in a Biethnic South African Cohort: The SABPA Study. Hypertens. Res. 2017, 40, 189–195. [Google Scholar] [CrossRef]
- Gopal, N.; Maithilikarpagaselvi, N.; Rajendiran, A.; Srinivasan, A.R.; Gowda, P.; Subramanyam, V. Association of Endothelin-1 with Oxidative Stress and Inflammatory Response in Pre-Hypertensives. Cor Vasa 2019, 6, 562–566. [Google Scholar] [CrossRef]
- Wang, X.; Bao, W.; Liu, J.; Ouyang, Y.Y.; Wang, D.; Rong, S.; Xiao, X.; Shan, Z.L.; Zhang, Y.; Yao, P.; et al. Inflammatory Markers and Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetes Care 2013, 36, 166–175. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-Reactive Protein, Interleukin 6, and Risk of Developing Type 2 Diabetes Mellitus. JAMA 2002, 286, 327–334. [Google Scholar] [CrossRef]
- Moya, C.; Máñez, S. Paraoxonases: Metabolic Role and Pharmacological Projection. Naunyn Schmiedebergs Arch. Pharmacol. 2018, 391, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Turk, H.M.; Sevinc, A.; Camci, C.; Cigli, A.; Buyukberber, S.; Savli, H.; Bayraktar, N. Plasma Lipid Peroxidation Products and Antioxidant Enzyme Activities in patients with Type 2 Diabetes Mellitus. Acta Diabetol. 2002, 39, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Saparbekova, A.A.; Kantureyeva, G.O.; Kudasova, D.E.; Konarbayeva, Z.K.; Latif, A.S. Potential of Phenolic Compounds from Pomegranate (Punica granatum L.) by-Product with Significant Antioxidant and Therapeutic Effects: A Narrative Review. Saudi J. Biol. Sci. 2023, 30, 103553. [Google Scholar] [CrossRef]
- Melgarejo-Sánchez, P.; Núñez-Gómez, D.; Martínez-Nicolás, J.J.; Hernández, F.; Legua, P.; Melgarejo, P. Pomegranate Variety and Pomegranate Plant Part, Relevance from Bioactive Point of View: A Review. Bioresour. Bioprocess. 2021, 8, 2. [Google Scholar] [CrossRef]
- Gumienna, M.; Szwengiel, A.; Górna, B. Bioactive Components of Pomegranate Fruit and Their Transformation by Fermentation Processes. Eur. Food Res. Technol. 2016, 242, 631–640. [Google Scholar] [CrossRef]
- Harakeh, S.; Qari, M.; Rajeh, N.; Ali, S.; El-Shitany, N.; Hassan, S.; Abd-Allah, E.A.; Tashkandi, H.; Malik, M.F.A.; Aljabri, F.K.; et al. Ellagic Acid Nanoparticles Attenuate Oxidative Stress and Testicular Damage in High Fat Diet/Streptozotocin-Induced Diabetic Rats. J. King Saud Univ. Sci. 2022, 34, 101720. [Google Scholar] [CrossRef]
- Rao, F.; Tian, H.; Li, W.; Hung, H.; Sun, F. Potential Role of Punicalagin against Oxidative Stress Induced Testicular Damage. Asian J. Androl. 2016, 18, 627–632. [Google Scholar] [CrossRef]
- Xu, J.; Cao, K.; Liu, X.; Zhao, L.; Feng, Z.; Liu, J. Punicalagin Regulates Signaling Pathways in Inflammation-Associated Chronic Diseases. Antioxidants 2022, 11, 29. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, M.; Yang, X.; Yang, Z.; Li, L.; Mei, J. Supplementing Punicalagin Reduces Oxidative Stress Markers and Restores Angiogenic Balance in a Rat Model of Pregnancy-Induced Hypertension. Korean J. Physiol. Pharmacol. 2018, 22, 409–417. [Google Scholar] [CrossRef]
- Martins, I.C.V.S.; Maciel, M.G.; do Nascimento, J.L.M.; Mafra, D.; Santos, A.F.; Padilha, C.S. Anthocyanins-Rich Interventions on Oxidative Stress, Inflammation and Lipid Profile in Patients Undergoing Hemodialysis: Meta-Analysis and Meta-Regression. Eur. J. Clin. Nutr. 2023, 77, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Speer, H.; D’Cunha, N.M.; Alexopoulos, N.I.; McKune, A.J.; Naumovski, N. Anthocyanins and Human Health—A Focus on Oxidative Stress, Inflammation and Disease. Antioxidants 2020, 9, 366. [Google Scholar] [CrossRef]
- Kostka, T.; Ostberg-Potthoff, J.J.; Briviba, K.; Matsugo, S.; Winterhalter, P.; Esatbeyoglu, T. Pomegranate (Punica granatum L.) Extract and Its Anthocyanin and Copigment Fractions—Free Radical Scavenging Activity and Influence on Cellular Oxidative Stress. Foods 2020, 9, 1617. [Google Scholar] [CrossRef] [PubMed]
- Hou, D.X.; Yanagita, T.; Uto, T.; Masuzaki, S.; Fujii, M. Anthocyanidins Inhibit Cyclooxygenase-2 Expression in LPS-Evoked Macrophages: Structure-Activity Relationship and Molecular Mechanisms Involved. Biochem. Pharmacol. 2005, 70, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Nikiforov, N.G.; Markin, A.M.; Kashirskikh, D.A.; Myasoedova, V.A.; Gerasimova, E.V.; Orekhov, A.N. Overview of OxLDL and Its Impact on Cardiovascular Health: Focus on Atherosclerosis. Front. Pharmacol. 2021, 11, 613780. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).