
Lyme Disease: A Role for Coenzyme Q10 Supplementation?


{kind=link}
Abstract
1. Introduction
2. Coenzyme Q10
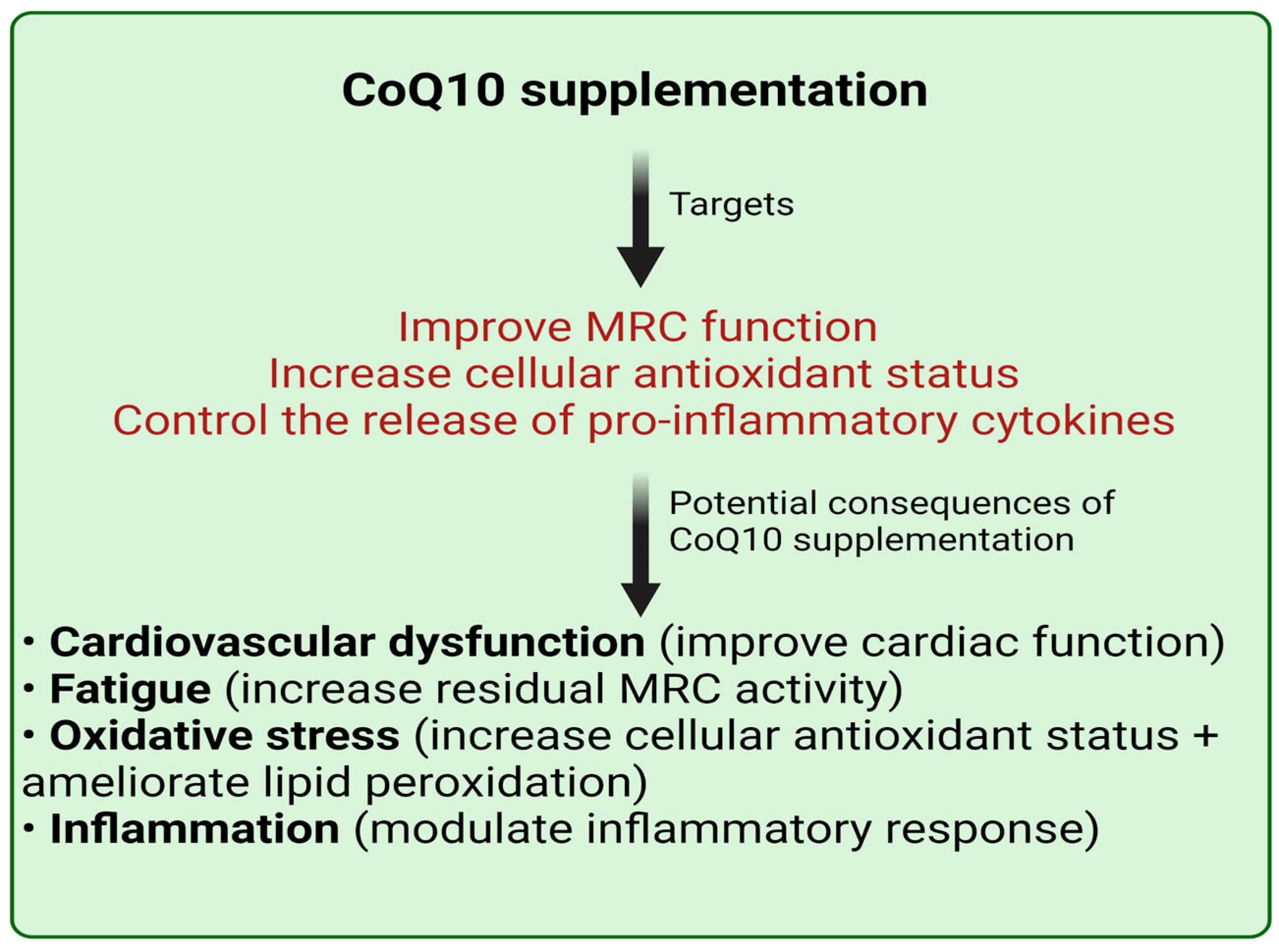
3. Lyme Disease, Fatigue, and CoQ10
4. Lyme Disease, Inflammation, and CoQ10
5. Lyme Disease, Oxidative Stress, and CoQ10
6. Lyme Disease, Cardiovascular Dysfunction, and CoQ10
7. CoQ10 Supplementation: Safety and Importance of Formulation Type
8. Monitoring of CoQ10 Status in Lyme Disease Patients
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barbour, A.G.; Benach, J.L. Discovery of the Lyme disease agent. mBio 2019, 10, e02166-19. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, O.; De Buck, E.; Van Wijngaerden, E. Lyme disease in Western Europe: An emerging problem? A systematic review. Acta Clin. Belg. 2021, 76, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Cairns, V.; Wallenhorst, C.; Rietbrock, S.; Martinez, C. Incidence of Lyme disease in the UK: A population-based cohort study. BMJ Open 2019, 9, e025916. [Google Scholar] [CrossRef] [PubMed]
- Schoen, R.T. Lyme disease: Diagnosis and treatment. Curr. Opin. Rheumatol. 2020, 32, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Radolf, J.D.; Strle, K.; Lemieux, J.E.; Strle, F. Lyme disease in humans. Curr. Issues Mol. Biol. 2021, 42, 333–384. [Google Scholar]
- Rupprecht, T.A.; Koedel, U.; Fingerle, V.; Pfister, H.W. The pathogenesis of Lyme neuroborreliosis: From infection to inflammation. Mol. Med. 2008, 14, 205–212. [Google Scholar] [CrossRef]
- Skare, J.T.; Garcia, B.L. Complement evasion by Lyme disease spirochetes. Trends Microbiol. 2020, 28, 889–899. [Google Scholar] [CrossRef]
- Coburn, J.; Garcia, B.; Hu, L.T.; Jewett, M.W.; Kraiczy, P.; Norris, S.J.; Skare, J. Lyme disease pathogenesis. Curr. Issues Mol. Biol. 2021, 42, 473–518. [Google Scholar]
- Crane, F.L. Biochemical functions of coenzyme Q10. J. Am. Coll. Nutr. 2001, 20, 591–598. [Google Scholar] [CrossRef]
- Heaton, R.A.; Heales, S.; Rahman, K.; Sexton, D.W.; Hargreaves, I. The effect of cellular CoQ10 deficiency on lysosomal acidification. J. Clin. Med. 2020, 9, 1923. [Google Scholar] [CrossRef]
- Schmelzer, C.; Lindner, I.; Rimbach, G.; Niklowitz, P.; Menke, T.; Döring, F. Functions of coenzyme Q10 in inflammation and gene expression. Biofactors 2008, 32, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Bysted, A.; Hłlmer, G. The CoQ10 content of the average Danish diet. Int. J. Vitam. Nutr. Res. 1997, 67, 123–129. [Google Scholar] [PubMed]
- Rebman, A.W.; Aucott, J.N. Post-treatment Lyme disease as a model for persistent symptoms in Lyme disease. Front. Med. (Lausanne) 2020, 7, 57. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, E.A.; Coyle, P.K.; Krupp, L.B. Post-Lyme syndrome and chronic fatigue syndrome. Neuropsychiatric similarities and differences. Arch. Neurol. 1997, 54, 1372–1376. [Google Scholar] [CrossRef]
- Dinerman, H.; Steere, A.C. Lyme disease associated with fibromyalgia. Ann. Intern. Med. 1992, 117, 281–285. [Google Scholar] [CrossRef]
- Fitzgerald, B.L.; Molins, C.R.; Islam, M.N.; Graham, B.; Hove, P.R.; Wormser, G.P.; Hu, L.; Ashton, L.V.; Belisle, J.T. Host metabolic response in early Lyme disease. J. Proteome Res. 2020, 19, 610–623. [Google Scholar] [CrossRef]
- Myhill, S.; Booth, N.E.; Howard, J. Chronic fatigue syndrome and mitochondrial and mitochondrial dysfunction. Int. J. Clin. Exp. Med. 2009, 2, 1–16. [Google Scholar]
- Cordero, M.D.; de Miguel, M.; Moreno-Fernández, A.M. Mitochondrial dysfunction in fibromyalgia and its implication in the pathogenesis of disease. Med. Clin. 2011, 136, 252–256. [Google Scholar] [CrossRef]
- Cordero, M.D.; Alcocer-Gómez, E.; de Miguel, M.; Culic, O.; Carrión, A.M.; Alvarez-Suarez, J.M.; Bullón, P.; Battino, M.; Fernández-Rodríguez, A.; Sánchez-Alcazar, J.A. Can CoQ10 improve clinical and molecular parameters in fibromyalgia? Antioxid. Redox Signal. 2013, 19, 1356–1361. [Google Scholar] [CrossRef]
- Castro-Marrero, J.; Cordero, M.D.; Segundo, M.J.; Sáez-Francàs, N.; Calvo, N.; Román-Malo, L.; Aliste, L.; Fernández de Sevilla, T.; Alegre, J. Effect of coenzyme Q10 plus nicotinamide adenine dinucleotide supplementation on maximum heart rate after exercise testing in chronic fatigue syndrome—A randomized, controlled, double-blind trial. Antioxid. Redox Signal. 2015, 35, 679–685. [Google Scholar] [CrossRef]
- Mehrabani, S.; Askari, G.; Miraghajani, M.; Tavakoly, R.; Arab, A. Effect of coenzyme Q10 supplementation on fatigue: A systematic review of interventional studies. Complement. Ther. Med. 2019, 43, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.; Settineri, R.; Ellithorpe, R. Glycophospholipid Formulation with NADH and CoQ10 Significantly Reduces Intractable Fatigue in Western Blot-Positive ‘Chronic Lyme Disease’ Patients: Preliminary Report. Funct. Foods Health Dis. 2012, 2, 35–47. [Google Scholar] [CrossRef]
- Sigal, L.H. Immunologic mechanisms in Lyme neuroborreliosis: The potential role of autoimmunity and molecular mimicry. Semin. Neurol. 1997, 17, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Koh, T.J.; DiPietro, L.A. Inflammation and wound healing: The role of the macrophage. Expert Rev. Mol. Med. 2011, 13, e23. [Google Scholar] [CrossRef]
- Mantle, D.; Heaton, R.A.; Hargreaves, I.P. Coenzyme Q10 and Immune Function: An Overview. Antioxidants 2021, 10, 759. [Google Scholar] [CrossRef]
- Lee, B.J.; Huang, Y.C.; Chen, S.J.; Lin, P.T. Coenzyme Q10 supplementation reduces oxidative stress and increases antioxidant enzyme activity in patients with coronary artery disease. Nutrition 2012, 28, 250–255. [Google Scholar] [CrossRef]
- Farsi, F.; Mohammadshahi, M.; Alavinejad, P.; Rezazadeh, A.; Zarei, M.; Engali, K.A. Functions of Coenzyme Q10 Supplementation on Liver Enzymes, Markers of Systemic Inflammation, and Adipokines in Patients Affected by Nonalcoholic Fatty Liver Disease: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial. J. Am. Coll. Nutr. 2016, 35, 346–353. [Google Scholar] [CrossRef]
- Rahmani, E.; Jamilian, M.; Samimi, M.; Zarezade Mehrizi, M.; Aghadavod, E.; Akbari, E.; Tamtaji, O.R.; Asemi, Z. The effects of coenzyme Q10 supplementation on gene expression related to insulin, lipid and inflammation in patients with polycystic ovary syndrome. Gynecol. Endocrinol. 2018, 34, 217–222. [Google Scholar] [CrossRef]
- Peacock, B.N.; Gherezghiher, T.B.; Hilario, J.D.; Kellermann, G.H. New insights into Lyme disease. Redox Biol. 2015, 5, 66–70. [Google Scholar] [CrossRef]
- Łuczaj, W.; Moniuszko, A.; Rusak, M.; Pancewicz, S.; Zajkowska, J.; Skrzydlewska, E. Lipid peroxidation products as potential bioindicators of Lyme arthritis. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 415–422. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Łuczaj, W.; Jarocka-Karpowicz, I.; Pancewicz, S.; Zajkowska, J.; Andrisic, L.; Zarkovic, N.; Skrzydlewska, E. Lipid peroxidation in the pathogenesis of neuroborreliosis. Free Radic. Biol. Med. 2016, 96, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Joyner, G.P. Host Derived Markers of Lyme Disease and Other Spirochaetal Infections: Their Discovery and Diagnostic Potential. Ph.D. Thesis, University of Liverpool, Liverpool, UK, 2020. [Google Scholar]
- Ligor, M.; Olszowy, P.; Buszewski, B. Aplication of medical and analytical methods in lyme borreliosis monitoring. Anal. Bioanal. Chem. 2012, 402, 2233–2248. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, B.J.; Tseng, Y.F.; Yen, C.H.; Lin, P.T. Effects of coenzyme Q10 supplementation (300 mg/day) on antioxidation and anti-inflammation in coronary artery disease patients during statins therapy: A randomized, placebo-controlled trial. Nutr. J. 2013, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Sanoobar, M.; Eghtesadi, S.; Azimi, A.; Khalili, M.; Jazayeri, S.; Reza Gohari, M. Coenzyme Q10 supplementation reduces oxidative stress and increases antioxidant enzyme activity in patients with relapsing-remitting multiple sclerosis. Int. J. Neurosci. 2013, 123, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Farhangi, M.A.; Alipour, B.; Jafarvand, E.; Khoshbaten, M. Oral coenzyme Q10 supplementation in patients with nonalcoholic fatty liver disease: Effects on serum vaspin, chemerin, pentraxin 3, insulin resistance and oxidative stress. Arch. Med. Res. 2014, 45, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Moazen, M.; Mazloom, Z.; Ahmadi, A.; Dabbaghmanesh, M.H.; Roosta, S. Effect of coenzyme Q10 on glycaemic control, oxidative stress and adiponectin in type 2 diabetes. J. Pak. Med. Assoc. 2015, 65, 404–408. [Google Scholar]
- Nagi, K.S.; Joshi, R.; Thakur, R.K. Cardiac manifestations of Lyme disease: A review. Can. J. Cardiol. 1996, 12, 503–506. [Google Scholar]
- Mortensen, S.A.; Rosenfeldt, F.; Kumar, A.; Dolliner, P.; Filipiak, K.J.; Pella, D.; Alehagen, U.; Steurer, G.; Littarru, G.P.; Q-SYMBIO Study Investigators. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: Results from Q-SYMBIO: A randomized double-blind trial. JACC Heart Fail. 2014, 2, 641–649. [Google Scholar] [CrossRef]
- Hidaka, T.; Fujii, K.; Funahashi, I.; Fukutomi, N.; Hosoe, K. Safety assessment of CoQ10. Biofactors 2008, 32, 199–208. [Google Scholar] [CrossRef]
- López-Lluch, G.; Del Pozo-Cruz, J.; Sánchez-Cuesta, A.; Cortés-Rodríguez, A.B.; Navas, P. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition 2019, 57, 133–140. [Google Scholar] [CrossRef]
- Molyneux, S.L.; Young, J.M.; Florkowski, C.M.; Lever, M.; George, P.M. Coenzyme Q10: Is there a clinical role and a case for measurement? Clin. Biochem. Rev. 2008, 29, 71. [Google Scholar] [PubMed]
- Yubero, D.; Montero, R.; Artuch, R.; Land, J.M.; Heales, S.J.; Hargreaves, I.P. Biochemical diagnosis of coenzyme Q10 deficiency. Mol. Syndromol. 2014, 5, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Duberley, K.; Heales, S.; Abramov, A.; Chalasani, A.; Land, J.; Rahman, S.; Hargreaves, I. Effect of Coenzyme Q10 supplementation on mitochondrial electron transport chain activity and mitochondrial oxidative stress in Coenzyme Q10 deficient human neuronal cells. Int. J. Biochem. Cell. Biol. 2014, 50, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Shult, C.W.; Oakes, D.; Kieburtz, K.; Beal, M.F.; Haas, R.; Plumb, S.; Juncos, J.L.; Nutt, J.; Shoulson, I.; Carter, J. Effects of coenzyme Q10 in early Parkinson disease: Evidence of slowing of the functional decline. Arch. Neurol. 2002, 59, 1541–1550. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantle, D.; Turton, N.; Hargreaves, I.P. Lyme Disease: A Role for Coenzyme Q10 Supplementation? Antioxidants 2022, 11, 667. https://doi.org/10.3390/antiox11040667
Mantle D, Turton N, Hargreaves IP. Lyme Disease: A Role for Coenzyme Q10 Supplementation? Antioxidants. 2022; 11(4):667. https://doi.org/10.3390/antiox11040667
Chicago/Turabian StyleMantle, David, Nadia Turton, and Iain P. Hargreaves. 2022. "Lyme Disease: A Role for Coenzyme Q10 Supplementation?" Antioxidants 11, no. 4: 667. https://doi.org/10.3390/antiox11040667
APA StyleMantle, D., Turton, N., & Hargreaves, I. P. (2022). Lyme Disease: A Role for Coenzyme Q10 Supplementation? Antioxidants, 11(4), 667. https://doi.org/10.3390/antiox11040667