Clinical and Electrophysiological Differences between Subjects with Dysphonetic Dyslexia and Non-Specific Reading Delay

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects (Entire Sample)
Composition of the Subsample
2.2. Clinical Protocol
Exclusion Criteria
2.3. The Direct Test Reading and Spelling (DTRS)
The Complexity Index
2.4. Neurophysiologic Assessment
2.4.1. EEG Data Acquisition
2.4.2. QEEG at the Scalp
2.4.3. QEEG Source Analysis (QEEGT)
2.4.4. Stability Based Biomarkers Identification
2.5. Statistical Analyses
3. Results
3.1. Results of the DTRS
3.2. Results of the QEEG
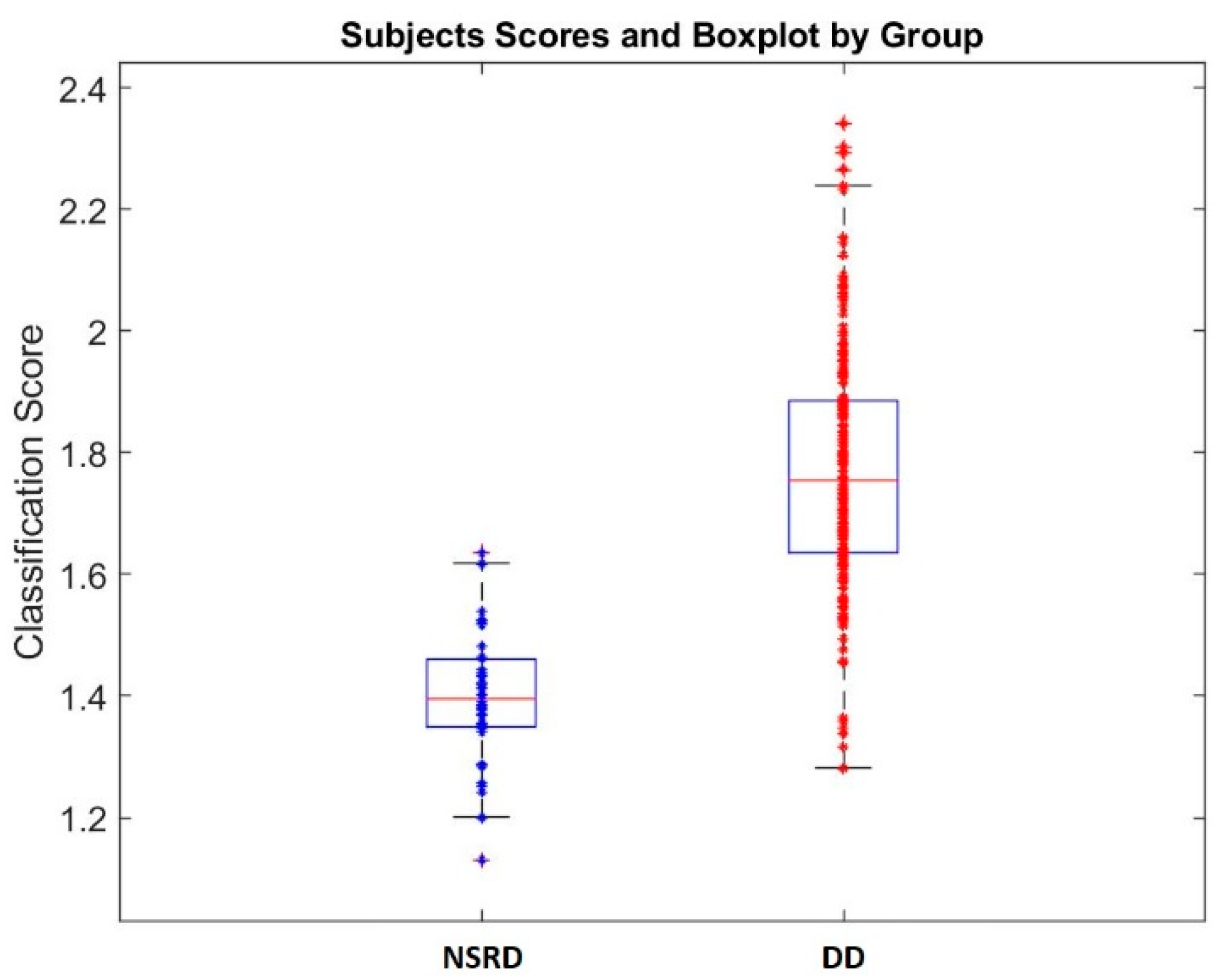
3.3. Biomarkers Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A1. Classification of Errors of the Reading Test
- -
- Wild guesses: the word read doesn’t have any correspondence with the word presented;
- -
- Gestalt substitution: the visual structure of the word is clearly recognizable; the elements that recall the words presented are: the length of the words, the presence of the initial and final syllables, or the central syllables; sometimes the central syllables could be omitted in plurisyllabic words
- -
- Semantic substitution: words closely related conceptually but not phonetically;
- -
- mismatch of similar homologous grapheme or inexact grapheme;
- -
- insertion/omission of letters of known words,
- -
- Non-words: the word read have phonological inaccuracies, accentuation errors, or sequencing errors.
- -
- Confusion of visually similar graphemes;
- -
- Initial fragment: words read only with the initial syllables;
- -
- Visuo-spatial reversal of letters and syllables;
- -
- Non-words: the word read have phonological inaccuracies, visuo-spatial reversal of letters and/or syllables.
Appendix A2. Classification Errors of the Spelling Test
- -
- Missing Lack of double letters;
- -
- Lack of accent
- -
- Insertion/omission of letters
- -
- mismatch of similar graphemes;
- -
- Good phonetic equivalent.
- -
- Dyseidetic errors:
- -
- Visuo-spatial reversal of syllables or letters;
References
- Boder, E. Developmental Dyslexia: A diagnostic approach based on three typical reading-spelling patterns. Dev. Med. Child Neurol. 1973, 15, 663–687. [Google Scholar] [CrossRef] [PubMed]
- Boder, E.; Jarrico, S. The Boder Test of Reading-Spelling Patterns; Grune Stratton: New York, NY, USA, 1982. [Google Scholar]
- Chiarenza, G.A.; Bindelli, D. Il test diretto di lettura e scrittura (DTLS): Versione computerizzata e dati normativi. Giornale Neuropsichiatria dell’Età Evolutiva 2001, 21, 163–179. [Google Scholar]
- Luisi, A.; Ruggerini, C. Dislessia e Disagio Pedagogico, un Approccio Interdisciplinare per la Diagnosi e L’aiuto; Editrice TEMI: Bologna, Italy, 1997. [Google Scholar]
- Chiarenza, G.A.; Di Pietro, S.F. La dislessia e i suoi sottotipi. Modelli clinici e risvolti applicativi nel trattamento della dislessia evolutiva. In Dentro la Dislessia; Sidoti, E., Ed.; Junior Edizioni: Brescia, Italy, 2014; pp. 107–132. [Google Scholar]
- Ginn, R. An Analysis of Various Psychometric Typologies of Primary Reading Disability. Unpublished Ph.D. Thesis, University of Southern California, Los Angeles, CA, USA, 1979. [Google Scholar]
- Naiden, N. (Basic Skills Department of the Seattle Public Schools, Washington, UK); Winger, J. (Department of Early Childhood Education, Oslo and Akershus University College of Applied Sciences, Oslo, Norway). Personal communication, 1972.
- Nockleby, D.M.; Galbraith, G.C. Developmental dyslexia subtypes and the Boder test of reading spelling patterns. J. Psychoeduc. Assess. 1984, 2, 91–100. [Google Scholar] [CrossRef]
- Breznitz, Z.; Meyler, A. Speed of lower-level auditory and visual processing as a basic factor in dyslexia: Electrophysiological evidence. Brain Lang. 2003, 85, 166–184. [Google Scholar] [CrossRef]
- Žarić, G.; Fraga González, G.; Tijms, J.; Van der Molen, M.W.; Blomert, L.; Bonte, M. Cross-modal deficit in dyslexic children: Practice affects the neural timing of letter-speech sound integration. Front. Hum. Neurosci. 2015, 24, 9–369. [Google Scholar] [CrossRef]
- Chabot, R.J.; di Michele, F.; Prichep, L.; John, E.R. The Clinical Role of Computerized EEG in the evaluation and treatment of learning and attention disorders in children and adolescents. J. Neuropsychiatry Clin. Neurosci. 2001, 13, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R. Electroencephalographic and neurophysiological studies in dyslexia. In Dyslexia: An Appraisal of Current Knowledge; Benton, A., Peal, D., Eds.; Oxford University Press: New York, NY, USA, 1978; pp. 207–240. [Google Scholar]
- Byring, R.; Jarvilehto, T. Auditory and visual evoked potentials of schoolboys with spelling disabilities. Dev. Med. Child Neurol. 1985, 27, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Conners, C.K. Critical review of electroencephalographic and neurophysiologic studies in dyslexia. In Dyslexia: An Appraisal of Current Knowledge; Benton, A., Peal, D., Eds.; Oxford University Press: New York, NY, USA, 1978; pp. 251–261. [Google Scholar]
- Becker, J.; Velasco, M.; Harmony, T. Electroencephalographic characteristics of children with learning disabilities. Clin. Electroencephalogr. 1987, 18, 93–101. [Google Scholar] [PubMed]
- Alvarez, A.; Perez-Avalo, M.C.; Morenza, L. Neuropsychological assessment of learning-disorder children with paroxysmal EEG activity. New Issues Neurosci. 1992, 4, 40–50. [Google Scholar]
- Koyama, M.S.; Di Martino, A.; Zuo, X.N.; Kelly, C.; Mennes, M.; Jutagir, D.R.; Castellanos, F.X.; Milham, M.P. Resting-state functional connectivity indexes reading competence in children and adults. J. Neurosci. 2011, 31, 8617–8624. [Google Scholar] [CrossRef]
- Koyama, M.S.; Di Martino, A.; Kelly, C.; Jutagir, D.R.; Sunshine, J.; Schwartz, S.J.; Castellanos, F.X.; Milham, M.P. Cortical signatures of dyslexia and remediation: An intrinsic functional connectivity approach. PLoS ONE 2013, 8, e55454. [Google Scholar] [CrossRef]
- Zhang, M.; Li, J.; Chen, C.; Xue, G.; Lu, Z.; Mei, L.; Xue, H.; Xue, F.; He, Q.; Chen, C.; et al. Resting-state functional connectivity and reading abilities in first and second languages. NeuroImage 2014, 84, 546–553. [Google Scholar] [CrossRef]
- Hoeft, F.; McCandliss, B.D.; Black, J.M.; Gantman, A.; Zakerani, N.; Hulme, C.; Lyytinen, H.; Whitfield-Gabrieli, S.; Glover, G.H.; Reiss, A.L.; et al. Neural systems predicting long-term outcome in dyslexia. Proc. Natl. Acad. Sci. USA 2011, 108, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Niogi, S.N.; McCandliss, B.D. Left lateralized white matter microstructure accounts for individual differences in reading ability and disability. Neuropsychologia 2006, 44, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Vandermosten, M.; Boets, B.; Wouters, J.; Ghesquière, P. A qualitative and quantitative review of diffusion tensor imaging studies in reading and dyslexia. Neurosci. Biobehav. Rev. 2012, 36, 1532–1552. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Shi, L.; Chen, F.; Waye, M.M.; Lim, C.K.; Cheng, P.W.; Luk, S.S.; Mok, V.C.; Chu, W.C.; Wang, D. Altered topological organization of brain structural network in Chinese children with developmental dyslexia. Neurosci. Lett. 2015, 589, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Richards, T.L.; Grabowski, T.J.; Boord, P.; Yagle, K.; Askren, M.; Mestre, Z.; Robinson, P.; Welker, O.; Gulliford, D.; Nagy, W.; et al. Contrasting brain patterns of writing-related DTI parameters, fMRI connectivity, and DTI–fMRI connectivity correlations in children with and without dysgraphia or dyslexia. Neuroimage Clin. 2015, 8, 408–421. [Google Scholar] [CrossRef] [PubMed]
- Schurz, M.; Wimmer, H.; Richlan, F.; Ludersdorfer, P.; Klackl, J.; Kronbichler, M. Resting state and task-based functional brain connectivity in developmental dyslexia. Cereb. Cortex 2014, 25, 3502–3514. [Google Scholar] [CrossRef] [PubMed]
- Van der Mark, S.; Klaver, P.; Bucher, K.; Maurer, U.; Schulz, E.; Brem, S.; Martin, E.; Brandeis, D. The left occipitotemporal system in reading: Disruption of focal fMRI connectivity to left inferior frontal and inferior parietal language areas in children with dyslexia. Neuroimage 2011, 54, 2426–2436. [Google Scholar] [CrossRef] [PubMed]
- John, E.R.; Prichep, L.S.; Ahn, H.; Easton, P.; Fridman, J.; Kaye, H. Neurometric evaluation of cognitive dysfunctions and neurological disorders in children. Prog. Neurobiol. 1983, 21, 239–290. [Google Scholar] [CrossRef]
- Duffy, F.H.; Denckla, M.B.; Bartels, P.H.; Sandini, G.; Kiessling, L.S. Dyslexia: Automated diagnosis by computerized classification of brain electrical activity. Ann. Neurol. 1980, 7, 421–428. [Google Scholar] [CrossRef] [PubMed]
- John, E.R. Neurometric evaluation of brain function related to learning disorders. Acta Neurol. Scand. 1981, 64 (Suppl. S89), 87–100. [Google Scholar] [CrossRef]
- Marosi, E.; Harmony, T.; Sánchez, L.; Becker, J.; Bernal, J.; Reyes, A.; Díaz de Léon, A.E.; Rodríguez, M. Maturation of the coherence of EEG activity in normal and learning-disabled children. Electroencephalogr. Clin. Neurophysiol. 1992, 83, 350–357. [Google Scholar] [CrossRef]
- Marosi, E.; Harmony, T.; Reyes, A.; Bernal, J.; Fernández, T.; Guerrero, V.; Rodríguez, M.; Silva, J.; Yáñez, G.; Rodríguez, H. A follow-up study of EEG coherence in children with different pedagogical evaluations. Int. J. Psychophysiol. 1997, 25, 227–235. [Google Scholar] [CrossRef]
- John, E.R.; Prichep, L.S. Principles of neurometrics and neurometric analysis of EEG and evoked potentials. In EEG: Basic Principles, Clinical Applications and Related Fields; Niedermeyer, E., Lopes Da Silva, F., Eds.; Williams and Wilkins: Baltimore, MD, USA, 1993; pp. 989–1003. [Google Scholar]
- Harmony, T.; Hinojosa, G.; Marosi, E.; Becker, J.; Rodriguez, M.; Reyes, A.; Rocha, C. Correlation between EEG spectral parameters and an educational evaluation. Int. J. Neurosci. 1990, 54, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Bayard, J.; Galán-García, L.; Fernandez, T.; Biscay Lirio, R.; Roca-Stappung, M.; Ricardo-Garcell, J.; Harmony, T.; Valdes-Sosa, P. Stable sparse classifiers identify QEEG signatures that predict learning disabilities (NOS) severity. Front. Neurosci. 2018, 11, 749. [Google Scholar] [CrossRef] [PubMed]
- Roca-Stappung, M.; Fernandez, T.; Bosch-Bayard, J.; Harmony, T.; Ricardo-Garcell, J. Electroencephalographic characterization of subgroups of children with learning disorders. PLoS ONE 2017, 12, e0179556. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.; Deering, W. Subtypes of dyslexia: Investigation of Boder’s system using quantitative neurophysiology. Dev. Med. Child Neurol. 1989, 31, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.M.; Deering, W.; Goldstein, M.; Rahbar, M.H. Electrophysiological correlates of dyslexic subtypes. J. Learn. Disabil. 1992, 28, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Casarotto, S.; Ricciardi, E.; Sani, L.; Guazzelli, M.; Pietrini, P.; Chiarenza, G.A. Single-letter reading elicits a different spatio-temporal modulation of brain activity in dyslexic children as compared to healthy controls. Neuroimage 2007, 36 (Suppl. S1), 171. [Google Scholar]
- Chiarenza, G.A. Normal and abnormal reading processes in children. Neuropsychophysiological studies. In Handbook of Clinical QEEG and Neurotherapy; Thomas, F.C., John, A.F., Eds.; Routledg: New York, NY, USA, 2017; Volume 10017, pp. 235–249. [Google Scholar]
- Velikova, S.; Chiarenza, G.A. EEG correlates of clinical subtypes of developmental dyslexia: Independent Component Analysis study. Int. J. Psychophysiol. 2012, 3, 322. [Google Scholar] [CrossRef]
- De Sonneville, L.M. Handbook Amsterdam Neuropsychological Tasks; Boom Test Publisher: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013.
- Cornoldi, C.; Colpo, G. Prove di Lettura MT-2 per la Scuola Primaria; Organizzazioni Speciali: Firenze, Italy, 2011. [Google Scholar]
- Cornoldi, C.; Colpo, G. Nuove Prove di Lettura MT per la Scuola Secondaria di I Grado; Organizzazioni Speciali: Firenze, Italy, 2012. [Google Scholar]
- Sartori, G.; Job, R.; Tressoldi, P.E. Batteria per la Valutazione Della Dislessia e Disortografia Evolutiva. DDE-2; Organizzazioni Speciali: Firenze, Italy, 2007. [Google Scholar]
- Chiarenza, G.A. Test Diretto di Lettura e Scrittura, DTLS (Seconda edizione); Centro Internazionale Disturbi di Apprendimento, Attenzione, Iperattività (CIDAAI): Milano, Italy, 2010. [Google Scholar]
- Cornoldi, C.; Lucangeli, D.; Bellina, M. Test AC-MT 6-11: Test di Valutazione Delle Abilità di Calcolo; Erickson: Trento, Italy, 2002. [Google Scholar]
- Cornoldi, C.; Cazzola, C. AC-MT 11-14: Test di Valutazione Delle Abilità di Calcolo e Problem Solving Dagli 11 ai 14 Anni; Erickson: Trento, Italy, 2003. [Google Scholar]
- Biancardi, A.; Morioni, E.; Pieretti, E. BDE, Batteria per la Discalculia Evolutiva; Omega: Torino, Italy, 2004. [Google Scholar]
- Di Brina, C.; Rossini, G. BHK Scala Sintetica per la Valutazione Della Scrittura in Età Evolutiva; Erickson: Trento, Italy, 2011. [Google Scholar]
- Tressoldi, P.; Cornoldi, C.; Re, A.M. BVSCO-2: Batteria per la Valutazione della Scrittura e della Competenza Ortografica-2; Giunti OS: Firenze, Italy, 2012. [Google Scholar]
- Pascual-Marqui, R.D.; Valdes-Sosa, P.A.; Alvarez-Amador, A. A parametric model for multichannel EEG spectra. Int. J. Neurosci. 1998, 40, 89–99. [Google Scholar] [CrossRef]
- Szava, S.; Valdes, P.; Biscay, R.; Galan, L.; Bosch, J.; Clark, I.; Jimenez, J.C. High resolution quantitative EEG analysis. Brain Topogr. Spring 1993, 6, 211–219. [Google Scholar] [CrossRef]
- Valdes-Sosa, P.; Biscay-Lirio, R.; Galán-García, L.; Bosch-Bayard, J.; Szava, S.; Virues-Alba, T. High Resolution Spectral EEG norms for topography. Brain Topogr. 1990, 3, 281–282. [Google Scholar]
- John, E.R.; Ahn, H.; Prichep, L.S.; Trepetin, M.; Brown, D.; Kaye, H. Developmental equations for the electroencephalogram. Science 1980, 210, 1255–1258. [Google Scholar] [CrossRef] [PubMed]
- Gasser, T.; Bacher, P.; Mochs, J. Transformation towards the normal distribution of broadband spectral parameters of the EEG. EEG Clin. Neurophysiol. 1982, 53, 119–124. [Google Scholar] [CrossRef]
- John, E.R.; Prichep, L.S.; Friedman, J.; Easton, P. Neurometrics: Computer-assisted differential diagnosis of brain dysfunctions. Science 1988, 293, 162–169. [Google Scholar] [CrossRef]
- Kondacs, A.; Szabo, M. Long-term intra-individual variability of the background EEG in normals. Clin. Neurophysiol. 1999, 110, 1708–1716. [Google Scholar] [CrossRef]
- Bosch-Bayard, J.; Valdes-Sosa, P.; Virues-Alba, T.; Aubert-Vazquez, E.; John, E.R.; Harmony, T.; Riera-Diaz, J.; Trujillo-Barreto, N. 3D statistical parametric mapping of EEG source spectra by means of variable resolution electromagnetic tomography (VARETA). Clin. Electroencephalogr. 2001, 32, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Riera, J.J.; Fuentes, M.E. Electric lead field for a piecewise homogeneous volume conductor model of the head. IEEE Trans. Biomed. Eng. 1998, 45, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.C.; Collins, D.L.; Mills, S.R.; Brown, E.D.; Kelly, R.L.; Peters, T.M. 3D Statistical Neuroanatomical Models from 305 MRI Volumes. In Proceedings of the IEEE Nuclear Science Symposium and Medical Imaging Conference, San Francisco, CA, USA, 31 October–6 November 1993; Volume 95, pp. 1813–1817. [Google Scholar]
- Hernandez, J.L.; Biscay, R.; Virues, T.; Szava, S.; Bosch, J.; Riquenes, A.; Clark, I. A global scale factor in brain topography. Int. J. Neurosci. 1994, 76, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Mulert, C.; Pogarell, O.; Juckel, G.; Rujescu, D.; Giegling, I.; Rupp, D.; Mavrogiorgou, P.; Bussfeld, P.; Gallinat, J.; Möller, H.J.; et al. The neural basis of the P300 potential: Focus on the time-course of the underlying cortical generators. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Bolwig, T.G.; Hansen, E.S.; Hansen, A.; Merkin, H.; Prichep, L.S. Toward a better understanding of the pathophysiology of OCD SSRI responder: QEEG source localization. Acta Psychiatr. Scand. 2007, 115, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Zumsteg, D.; Wennberg, R.A.; Treyer, V.; Buck, A.; Wieser, H.G. H2(15)O or 13NH3 PET and electromagnetic tomography (LORETA) during partial status epilepticus. Neurology 2005, 65, 1657–1660. [Google Scholar] [CrossRef] [PubMed]
- Prichep, L.S.; John, E.R.; Tom, M.L. Localization of deep white matter lymphoma using VARETA—A case study. Clin. EEG 2001, 32, 62–66. [Google Scholar] [CrossRef]
- Corsi-Cabrera, M.; Figueredo-Rodríguez, P.; del Río-Portilla, Y.; Sánchez-Romero, J.; Galán, L.; Bosch-Bayard, J. Enhanced fronto-parietal synchronized activation during the wake-sleep transition in patients with primary insomnia. Sleep 2012, 35, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.C.; Collins, D.L.; Neelin, P.; MacDonald, D.; Kamber, M.; Marrett, T.S. Three-Dimensional correlative imaging: Applications in human brain mapping. In Functional Neuroimaging: Technical Foundations; Thatcher, R., Hallet, M., Zeffiro, T., John, E.R., Huerta, M., Eds.; Academic Press: New York, NY, USA, 1994; pp. 145–161. [Google Scholar]
- Worsley, K.J.; Marrett, S.; Neelin, P.; Evans, A.C. A unified statistical approach for determining significant signals in location and scale space images of cerebral activation. In Quantification of Brain Function Using PET; Myers, R., Cunningham, V.G., Bailey, D.L., Jones, T., Eds.; Academic Press: San Diego, CA USA, 1995; pp. 327–333. [Google Scholar]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 2008, 33, 1–22. [Google Scholar] [CrossRef]
- Reynolds, C.R. Clinical Acumen but Psychometric Naivete in Neuropsychological Assessment of Educational Disorders. Arch. Clin. Neupsychol. 1986, 1, 121–137. [Google Scholar] [CrossRef]
- Howes N., L.; Bigler, E.D.; Lawson, J.S.; Burlingame, G.M. Reading Disability Subtypes and the Test of Memory and Learning. Arch. Clin. Neuropsychol. 1999, 14, 317–339. [Google Scholar] [CrossRef] [PubMed]
- Chiarenza, G.A.; Coati, P.; Cucci, M. Development of gestalt-reading processes in children: Assessment using the Boder test. Acta Paedopsychiatr. 1994, 56, 193–197. [Google Scholar] [PubMed]
- Kinsbourne, M.; Warrington, E. Developmental factors in reading and writing backwardness. Br. J. Psychol. 1963, 54, 154–156. [Google Scholar] [CrossRef]
- Ingram, T.; Mason, A.; Blackburn, I. A retrospective study of 82 children with reading disability. Dev. Med. Child Neurol. 1970, 12, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Coltheart, M.; Curtis, B.; Atkins, P.; Haller, M. Models of reading aloud: Dual route and parallel-distributed-processing approaches. Psychol. Rev. 1993, 100, 589–608. [Google Scholar] [CrossRef]
- Rourke, B.P.; Finlayson, M.A. Neuropsychological significance of variations in patterns of academic performance: Verbal and visual-spatial abilities. J. Abnorm. Child Psychol. 1978, 6, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Seymour, P.H. Individual cognitive analysis of competent and impaired reading. Br. J. Psychol. 1987, 78, 483–506. [Google Scholar] [CrossRef] [PubMed]
- Bakker, D.J. Hemispheric differences and reading strategies: Two dyslexias? Bull. Orton Soc. 1979, 29, 84–100. [Google Scholar] [CrossRef]
- Bakker, D.J. Neuropsychological Treatment of Dyslexia; Oxford University Press: New York, NY, USA, 1990. [Google Scholar]
- Snowling, M.J. Dyslexia: A language learning impairment. J. Br. Acad. 2014, 2, 43–58. [Google Scholar] [CrossRef]
- Chiarenza, G.A.; Olgiati, P.; Trevisan, C.; De Marchi, I.; Casarotto, S. Reading aloud: A psychophysiological investigation in children. Neuropsychologia 2013, 51, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Jena, S.P.K. Learning Disability: Theory to Practice; SAGE Publishing: New Delhi, India, 2013. [Google Scholar]
- Penolazzi, B.; Spironelli, C.; Angrilli, A. Delta EEG activity as a marker of dysfunctional linguistic processing in developmental dyslexia. Psychophysiology 2008, 45, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Colon, E.J.; Notermas, S.L.; de Weerd, J.P.; Kap, J. The discriminating role of EEG power spectra in dyslexic children. J. Neurol. 1979, 221, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Fernández, T.; Harmony, T.; Fernández-Bouzas, A.; Silva, J.; Herrera, W.; Santiago-Rodríguez, E.; Sánchez, L. Sources of EEG activity in learning disabled children. Clin. Electroencephalogr. 2002, 33, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Jäncke, L.; Alahmadi, N. Resting State EEG in Children with Learning Disabilities: An Independent Component Analysis Approach. Clin. EEG Neurosci. 2016, 47, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Mechelse, K.; Gemund, J.J.; Nije, J.; Burg, L.; Laurs, J. Visual and quantitative analysis of EEGs of school children, children, and school children with specific reading disability. Electroencephalogr. Clin. Neurophysiol. 1975, 39, 106–108. [Google Scholar]
- Byring, R.; Salmi, T.K.; Sainio, K.O.; Orn, H.P. EEG in children with spelling disabilities. Electroencephalogr. Clin. Neurophysiol. 1991, 79, 247–255. [Google Scholar] [CrossRef]
- Fonseca, L.C.; Tedrus, G.M.; Chiodi, M.G.; Cerqueira, J.N.; Tonelotto, J.M. Quantitative EEG in children with learning disabilities: Analysis of band power. Arq. Neuropsiquiatr. 2006, 64, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Galaburda, A.M. The pathogenesis of childhood dyslexia. Res. Pub. Assoc. Res. Nerv. Ment. Dis. 1988, 66, 127–138. [Google Scholar]
- Galaburda, A.M. Neurology of developmental dyslexia. Curr. Opin. Neurol. Neurosurg. 1992, 5, 7176. [Google Scholar] [CrossRef]
- Galaburda, A.M. Neuroanatomic basis of developmental dyslexia. Neurol. Clin. N. Am. 1993, 11, 161–173. [Google Scholar] [CrossRef]
- Galaburda, A.M. Neurology of developmental dyslexia. Curr. Opin. Neurobiol. 1993, 3, 237–242. [Google Scholar] [CrossRef]
- Galaburda, A.M. The planum temporale (editorial). Arch. Neurol. 1993, 50, 457. [Google Scholar] [CrossRef] [PubMed]
- Galaburda, A.M. Developmental dyslexia and animal studies: At the interface between cognition and neurology. Cognition 1994, 50, 133–149. [Google Scholar] [CrossRef]
- Hunphreys, P.; Kaufmann, W.E.; Galaburda, A.M. Developmental dyslexia in women: Neuropathological findings in three patients. Ann. Neurol. 1990, 28, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Shaywitz, S.E.; Shaywitz, B.A.; Pugh, K.R.; Fulbright, R.K.; Constable, R.T.; Mencl, W.R.; Shankweiler, D.P.; Liberman, A.M.; Skudlarski, P.; Fletcher, J.M.; et al. Functional disruption in the organization of the brain for reading in dyslexia. Proc. Natl. Acad. Sci. USA 1998, 95, 2636–2641. [Google Scholar] [CrossRef] [PubMed]
- Filipek, P.A.; Pennington, B.F.; Simon, J.H.; Filley, C.M.; DeFries, J.C. Structural and functional neuroanatomy disorder. In Reading and Attention Disorders; Duane, D.D., Ed.; York Press Inc.: Baltimore, MD, USA, 1999; pp. 43–59. [Google Scholar]
- Wood, F.B.; Flowers, D.L. Functional neuroanatomy of dyslexic subtypes. In Reading and Attention Disorders. Neurobiological Correlates; Duane, D.D., Ed.; York Press Inc.: Baltimore, MD, USA, 1999; pp. 129–160. [Google Scholar]
- Wolff, P.H.; Melngailis, I.; Kotwica, K. Impaired motor timing control in specific reading retardation. Neuropsychologia 1984, 22, 587–600. [Google Scholar] [CrossRef]
- Wolff, P.H.; Michel, G.; Ovrut, M. The timing of syllables repetitions in developmental dyslexia. J. Speech Hear. Res. 1990, 33, 281. [Google Scholar] [CrossRef] [PubMed]
- Chiarenza, G.A.; Papakostopoulos, D.; Grioni, A.G.; Tengattini, M.B.; Mascellani, P.; Guareschi Cazzullo, A. Movement-related brain macropotentials during a motor perceptual task in dyslexic-dysgraphic children. In Cerebral Psychophysiology: Studies in Event-Related Potentials (EEG Suppl. 38); McCallum, W.C., Zappoli, R., Denoth, F., Eds.; Elsevier Science Publisher: Amsterdam, The Netherlands, 1986; pp. 489–491. [Google Scholar]
- Chiarenza, G.A.; Papakostopoulos, D.; Guareschi Cazzullo, A.; Giordana, F.; Giammari Aldè, G. Movement related brain macropotentials during skilled performance task in children with learning disabilities. In Clinical Application of Cerebral Evoked Potentials in Pediatric Medicine; Chiarenza, G.A., Papakostopoulos, D., Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1982; pp. 259–292. [Google Scholar]
- Chiarenza, G.A.; Papakostopoulos, D.; Guareschi Cazzullo, A.; Giordana, F.; Giammari Aldè, G. Movement related brain macropotentials (MRBMs) and their relationship with the accuracy of skilled performance in normal and learning disabled children. In Event Related Potentials in Children. Basic Concepts and Clinical Applications; Rothenberger, A., Ed.; Elsevier Biomedical Press: Amsterdam, The Netherlands, 1982; pp. 243–256. [Google Scholar]
- Chiarenza, G.A. Motor-perceptual function in children with developmental reading disorders: Neuropsychophysiological analysis. J. Learn. Disabil. 1990, 23, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Llinas, R. Is dyslexia a dyschronia? Ann. N. Y. Acad. Sci. 1993, 682, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Buzsáki, G. Rhythms of the Brain; Oxford University Press: New York, NY, USA, 2006; pp. 1–448. [Google Scholar]
- Casanova, R.; Whitlow, C.T.; Wagner, B.; Williamson, J.; Shumaker, S.A.; Maldjian, J.A.; Espeland, M.A. High Dimensional Classification of Structural MRI Alzheimer’s Disease Data Based on Large Scale Regularization. Front. Neuroinform. 2011, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Chiarenza, G.A.; Villa, S.; Galan, L.; Valdes-Sosa, P.; Bosch-Bayard, J. Junior temperament character inventory together with quantitative EEG discriminate children with attention deficit hyperactivity disorder combined subtype from children with attention deficit hyperactivity disorder combined subtype plus oppositional defiant disorder. Int. J. Psychophysiol. 2018, 130, 9–20. [Google Scholar] [PubMed]
- Hernandez-Gonzales, G.; Bringas-Vega, M.L.; Galán-Garcia, L.; Bosch-Bayard, J.; Lorenzo-Ceballos, Y.; Melie-Garcia, L.; Valdes-Urrutia, L.; Cobas-Ruiz, M.; Valdes-Sosa, P.A. Multimodal quantitative neuroimaging databases and methods: The Cuban Human Brain Mapping Project. Clin. EEG Neurosci. 2011, 42, 149–159. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, D.E.; Gridley, B.E. Differential ability scales: Profiles of learning-disabled subtypes. Psychol. Sch. 1993, 30, 11–24. [Google Scholar] [CrossRef]
- Swanson, H.L.; Cochran, K.F.; Ewers, C.A. Can learning disabilities be determined from working memory performance? J. Learn. Disabil. 1990, 23, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.; Willows, D.M. Information-processing patterns in specific reading disability. J. Learn. Disabil. 1995, 28, 216–231. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FSIQ | VIQ | PIQ | S.L.D. | Dysorth. | Dysgr. | Dyscal. | Com. | T.O.C. | S.T. | T.O.S.T. | S.T.D. | F.Q. | M.Q. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DD (N.S. = 169)—Means | 101.4 | 99.6 | 103.4 | 0.57 | 0.6 | 0.21 | 0.31 | 0.25 | 6.48 | 0.19 | 0.08 | 3.36 | 2.27 | 2.34 |
| NSRD (N.S. = 36)—Means | 105.5 | 103.9 | 106.6 | 0.58 | 0.49 | 0.22 | 0.27 | 0.44 | 6.5 | 0.04 | 0 | 0.31 | 2.38 | 2.22 |
| DD—SD | 10.9 | 11,7 | 12,1 | 0.61 | 0.49 | 0.41 | 0.46 | 0.43 | 1.66 | 0.39 | 0.5 | 9.04 | 2.39 | 2.36 |
| NSRD—SD | 9.2 | 12.1 | 10.0 | 0.54 | 0.51 | 0.42 | 0.45 | 0.5 | 0.61 | 0.21 | 0 | 1.47 | 2.26 | 2 |
| DD Vs. NSRD—P value | 0.02 | 0.03 | 0,1 | 0.93 | 0.18 | 0.88 | 0.59 | 0.008 | 0.95 | 0.01 | 0.29 | 0.025 | 0.79 | 0.75 |
| DD Vs. NSRD—t value | −2.3 | −2.19 | −1.64 | −0.08 | 1.32 | −0.14 | 0.53 | −2.7 | −0.06 | 2.4 | 1.04 | 2.25 | −0.26 | 0.31 |
| School | Age at DTRS | N.L.R. | RL | RA | RQ | RQM | RQC | |
|---|---|---|---|---|---|---|---|---|
| DD (N.S. = 169)—Means | 1.26 | 10.02 | 6.72 | 2.38 | 8.07 | 80.58 | 79.99 | 80.08 |
| NSRD (N.S. = 36)—Means | 1.47 | 10.84 | 6.87 | 2.27 | 8.12 | 75.23 | 71.64 | 73.26 |
| DD—SD | 0.46 | 1.92 | 2.49 | 1.38 | 1.79 | 9.63 | 9.82 | 8.64 |
| NSRD—SD | 0.59 | 2.17 | 2.3 | 1.5 | 1.82 | 10.04 | 9.98 | 9.52 |
| DD Vs. NSRD—P value | 0.011 | 0.013 | 0.72 | 0.66 | 0.88 | 0.001 | 7.8 × 10−7 | 6.1 × 10−6 |
| DD Vs. NSRD—t value | −2.56 | −2.51 | −0.36 | 0.43 | −0.15 | 3.31 | 5.08 | 4.64 |
| %KW | %UW | N.D.E.KW | D.E.IOL.KW | N.DY.E.KW | N.D.E.UW | D.E.MDL.UW | D.E.A.UW | D.E.GP.UW | D.E.IOL.UW | D.E.MGUW | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| DD (N.S. = 169)—Means | 71.81 | 47.65 | 1.9 | 1.06 | 1.2 | 5.1 | 1.35 | 0.28 | 1.51 | 1.21 | 0.56 |
| NSRD (N.S. = 36)—Means | 89.44 | 83.61 | 0.6 | 0.29 | 0.4 | 1.7 | 0.3 | 0.11 | 0.5 | 0.55 | 0.2 |
| DD—SD | 18.68 | 15.5 | 1.6 | 1.17 | 1.4 | 2.4 | 1.46 | 0.53 | 1.54 | 1.23 | 0.13 |
| NSRD—SD | 7.43 | 5.84 | 0.7 | 0.51 | 0.5 | 1 | 0.51 | 0.31 | 0.64 | 0.68 | 0.34 |
| DD Vs. NSRD P value | 2.8 × 10−10 | 1.4 × 10−33 | 3.2 × 10−7 | 2.4 × 10−5 | 1.0 × 10−10 | 1.5 × 10−17 | 4.8 × 10−6 | 0.012 | 1.2 × 10−5 | 0.001 | 0.008 |
| DD Vs. NSRD t value | −6.61 | −14.38 | 5.27 | 4.31 | 3.55 | 9.29 | 4.69 | 2.53 | 4.47 | 3.3 | 2.68 |
| FCOR | FINCOR | FHESIT | FSILL | UCOR | UINCOR | UGDIFF | NR | RTFCOR | RTFINCOR | RTFHESIT | RTFSILL | RTUCOR | RTUINCOR | RTUGDIFF | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DD (N.S. = 169)—Means | 15.1 | 2 | 1.8 | 0.2 | 2.7 | 0.2 | 0.3 | 0 | 1 | 2 | 2 | 1.26 | 1.6 | 1.7 | 3.3 |
| NSRD (N.S. = 36)—Means | 14.6 | 2 | 3 | 0.1 | 2.1 | 0 | 0.1 | 0 | 1 | 1,9 | 1.9 | 1.84 | 1.6 | 2 | 3.2 |
| DD—SD | 4.5 | 2.2 | 2.6 | 0.7 | 4 | 0.5 | 0.8 | 0.2 | 0.5 | 1.1 | 1 | 0.77 | 0.7 | 1.9 | 1.9 |
| NSRD—SD | 4.2 | 2.4 | 4 | 0.5 | 2.6 | 0.2 | 0.3 | 0 | 0.5 | 1.1 | 1 | 0.25 | 0.9 | 1.9 | 1.9 |
| DD Vs. NSRD—P value | 4.49 | 0.65 | 0.01 | 0.3 | 0.27 | 0.12 | 0.14 | 0.50 | 0.33 | 0.90 | 0.64 | 0.22 | 0.90 | 0.50 | 0.70 |
| DD Vs. NSRD—t value | 4.49 | 0.46 | −2.55 | 1.05 | 1.11 | 1.55 | 1.49 | 0.68 | 0.97 | 0.12 | 0.47 | −1.25 | 0.16 | −0.68 | 0.38 |
| 10 | 11 | 12 | 20 | 21 | 22 | 23 | 30 | 31 | 32 | 33 | 40 | 41 | 42 | 43 | 44 | 50 | 51 | 52 | 53 | 60 | 61 | 62 | 63 | 70 | 71 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 11 | 2.92 0.004 | |||||||||||||||||||||||||
| 15 | ||||||||||||||||||||||||||
| 21 | 2.21 0.028 | −2.38 0.019 | 2.64 0.025 | 2.41 0.024 | ||||||||||||||||||||||
| 22 | 9.35 0.003 | |||||||||||||||||||||||||
| 30 |
| Variables | Percent | Coeff. |
|---|---|---|
| Anamnestic and clinical data | ||
| Class | 100 | 0.031413 |
| Comorbidity | 100 | 0.029233 |
| Speech therapy | 96.36 | 0.053496 |
| Verbal Intelligent Quotient | 86.57 | 0.025448 |
| Age at DTRS | 83.56 | 0.029181 |
| School at DTRS | 80.85 | −0.00266 |
| Full Scale Intelligent Quotient | 78.57 | 0.005488 |
| DTRS: Writing Test: Dysphonetic errors in the known words list | ||
| Grapheme-phoneme correspondence | 77.59 | 0.049424 |
| Omission of letters | 76.67 | 0.005422 |
| Number of dysphonetic errors | 76 | 0.016698 |
| DTRS: Writing Test: Dyseidetic errors in the known words list | ||
| Errors of reversal of similar letters | 72.13 | −0.001226 |
| Number of dyseidetic errors | 70.49 | 0.010814 |
| DTRS: Writing Test: Dysphonetic errors in the unknown words list | ||
| Missing double letters | 67.86 | 0.000454 |
| Accent errors | 67.35 | 0.004261 |
| Grapheme-phoneme correspondence | 62.5 | 0.03555 |
| Omission of letters | 62 | 0.054781 |
| Grapheme mismatch | 60.38 | −0.034673 |
| Number of dysphonetic errors | 59.18 | 0.018046 |
| DTRS: Writing Test: Dyseidetic errors in the unknown words list | ||
| Total dyseidetic errors | 55.17 | −0.009407 |
| Total errors in the known and unknown words lists combined | ||
| Total dysphonetic errors | 54.39 | 0.021067 |
| Total dyseidetic errors | 52.54 | −0.005514 |
| DTRS: Reading Test: Dyseidetic errors in flash mode | ||
| Confusion of visually similar graphemes | 51.52 | −0.019377 |
| Dyseidetic non-words | 50.75 | 0.016049 |
| DTRS: Reading Test: Dyseidetic errors in untimed mode | ||
| Confusion of visually similar graphemes | 50.75 | −0.03763 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bosch-Bayard, J.; Peluso, V.; Galan, L.; Valdes Sosa, P.; Chiarenza, G.A. Clinical and Electrophysiological Differences between Subjects with Dysphonetic Dyslexia and Non-Specific Reading Delay. Brain Sci. 2018, 8, 172. https://doi.org/10.3390/brainsci8090172
Bosch-Bayard J, Peluso V, Galan L, Valdes Sosa P, Chiarenza GA. Clinical and Electrophysiological Differences between Subjects with Dysphonetic Dyslexia and Non-Specific Reading Delay. Brain Sciences. 2018; 8(9):172. https://doi.org/10.3390/brainsci8090172
Chicago/Turabian StyleBosch-Bayard, Jorge, Valeria Peluso, Lidice Galan, Pedro Valdes Sosa, and Giuseppe A. Chiarenza. 2018. "Clinical and Electrophysiological Differences between Subjects with Dysphonetic Dyslexia and Non-Specific Reading Delay" Brain Sciences 8, no. 9: 172. https://doi.org/10.3390/brainsci8090172
APA StyleBosch-Bayard, J., Peluso, V., Galan, L., Valdes Sosa, P., & Chiarenza, G. A. (2018). Clinical and Electrophysiological Differences between Subjects with Dysphonetic Dyslexia and Non-Specific Reading Delay. Brain Sciences, 8(9), 172. https://doi.org/10.3390/brainsci8090172