Reading Deficits in Intellectual Disability Are still an Open Question: A Narrative Review

 ,
, 
Abstract
1. Introduction
2. Method
2.1. Study Design
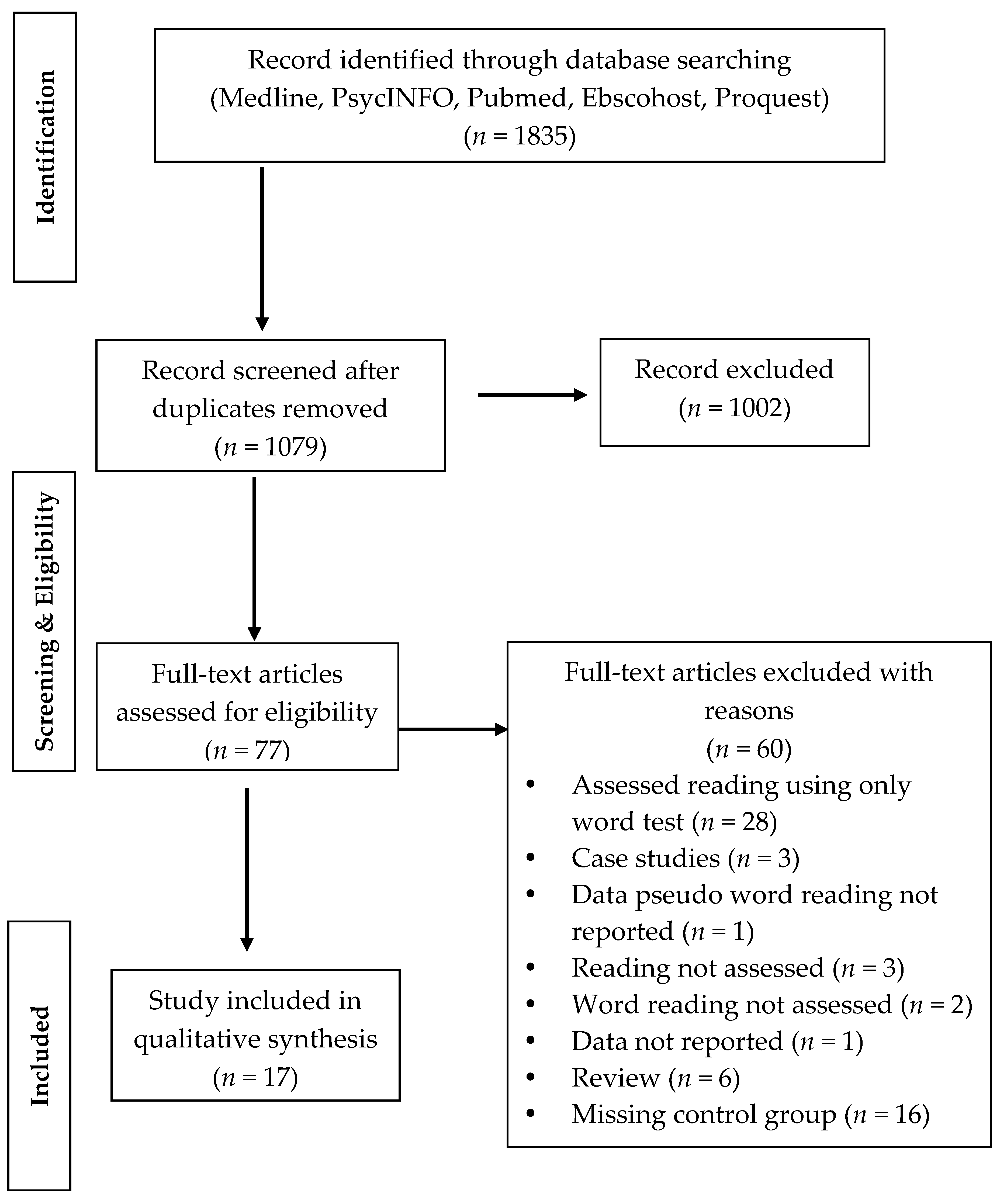
2.2. Search Strategy
2.3. Selection Criteria
2.4. Selection, Procedures, Screening and Data Elaboration
3. Data Synthesis
3.1. Methodological Considerations in Control Group Selection
4. Results
4.1. Studies Based on the Mental-Age Matching Design
4.2. Studies Based on the Reading-Level Design
4.3. Studies Based on Standard Zeta Scores or Chronological Match
5. Discussion
6. Implications for Clinical Practice and Research
7. Limitations
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). International Classification of Functioning, Disability and Health (ICF). Available online: http://www.who.int/en/ (accessed on 11 October 2017).
- WHO (World Health Organization). International Classification of Functioning, Disability and Health. Children &Youth (ICF-CY). Available online: http://www.who.int/en/ (accessed on 11 October 2017).
- Browder, D.M.; Wakeman, S.Y.; Spooner, F.; Ahlgrim-Delzell, L.; Algozzine, B. Research on reading instruction for students with significant cognitive disabilities. Except. Child. 2006, 72, 392–408. [Google Scholar] [CrossRef]
- Conners, F.A. Reading skills and cognitive abilities of individuals with mental retardation. In International Review of Research in Mental Retardation: Language and Communication in Mental Retardation; Abbeduto, L., Ed.; San Diego Academic Press: San Diego, CA, USA, 2003; Volume 27, pp. 191–229. ISBN 978-0-12-366227-9. [Google Scholar]
- National Reading Panel. Teaching Children to Read: An Evidence-Based Assessment of the Scientific Research Literature on Reading and Its Implications for Reading Instruction; US Department of Health and Human Services: Washington, DC, USA, 2000. Available online: https://www1.nichd.nih.gov/publications/pubs/nrp/Documents/report.pdf (accessed on 23 October 2017).
- Samuels, S.J.; Ediger, K.A.; Fautch-Patridge, T. The importance of fluent reading. N. Engl. Read. Assoc. J. 2005, 41, 1–8. [Google Scholar]
- Coltheart, M.; Rastle, K.; Perry, C.; Langdon, R.; Ziegler, J.C. DRC: A dual route cascaded model of visual word recognition and reading aloud. Psychol. Rev. 2001, 108, 204–256. [Google Scholar] [CrossRef] [PubMed]
- Saunders, K.J. Word-attack skills in individuals with mental retardation. Dev. Dis. Res. Rev. 2007, 13, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Næss, K.-A.B.; Melby-Lervåg, M.; Hulme, C.; HalaasLyster, S.-A. Reading skills in children with Down syndrome: A meta-analytic review. Res. Dev. Dis. 2001, 33, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Lemons, C.J.; Fuchs, D. Phonological awareness of children with Down syndrome: Its role in learning to read and the effectiveness of related interventions. Res. Dev. Disabil. 2010, 31, 316–330. [Google Scholar] [CrossRef] [PubMed]
- Joseph, L.M.; Seery, M.E. Where is the phonics? Are view of the literature on the use of phonetic analysis with students with mental retardation. Rem. Spec. Educ. 2004, 25, 88–94. [Google Scholar] [CrossRef]
- Hill, D.R. Phonics based reading interventions for students with intellectual disability: A systematic literature review. J. Educ. Train. Stud. 2016, 4, 205–214. [Google Scholar] [CrossRef]
- Mervis, C.B.; Klein-Tasman, P.B. Methodological Issues in Group-Matching Designs: α Levels for Control Variable Comparisons and Measurement Characteristics of Control and Target Variables. J. Autism Dev. Disord. 2004, 34, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, W.; Geudens, A. Old and new ways to study characteristics of reading disability: The case of the nonword-reading deficit. Cogn. Psychol. 2012, 65, 414–456. [Google Scholar] [CrossRef] [PubMed]
- Sitzmann, A.F.; Hagelstrom, R.T.; Tassone, F.; Hagerman, R.J.; Butler, M.G. Rare FMR1 gene mutations causing fragile X syndrome: A review. Am. J. Med. Genet. Part A 2018, 176A, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, R.J. Lessons from fragile X regarding neurobiology, autism, and neurodegeneration. J. Dev. Behav. Pediatr. 2006, 27, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.W.; Hessl, D.; Goodlin-Jones, B.; Ferranti, J.; Bacalman, S.; Barbato, I.; Tassone, F.; Hagerman, P.J.; Herman, H.; Hagerman, R.J. Autism profiles of males with fragile X syndrome. Am. J. Ment. Retard. 2008, 113, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, R.J.; Berry-Kravis, E.; Kaufmann, W.E.; Ono, M.Y.; Tartaglia, N.; Lachiewicz, A.; Kronk, R.; Delahunty, C.; Hessl, D.; Visootsak, J.; et al. Advances in the Treatment of Fragile X Syndrome. Pediatrics 2009, 123, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Bayes, M.; Magano, L.F.; Rivera, N.; Flores, R.; Perez Jurado, L.A. Mutational mechanisms of Williams–Beuren syndrome deletions. Am. J. Hum. Genet. 2003, 73, 131–151. [Google Scholar] [CrossRef] [PubMed]
- Donnai, D.; Karmiloff-Smith, A. Williams syndrome: From genotype through to the cognitive phenotype. Am. J. Med. Genet. 2000, 97, 164–171. [Google Scholar] [CrossRef]
- Mervis, C.B.; John, A.E. Cognitive and behavioral characteristics of children with Williams syndrome: Implications for intervention approaches. Am. J. Med. Genet. C Semin. Med. Genet. 2010, 154C, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Karmiloff-Smith, A. Perspectives on the dynamic development of cognitive capacities: Insights from Williams syndrome. Curr. Opin. Neurol. 2012, 25, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Järvinen-Pasley, A.; Bellugi, U.; Reilly, J.; Mills, D.L.; Galaburda, A.; Reiss, A.L.; Korenberg, J.R. Defining the social phenotype in Williams syndrome: A model for linking gene, the brain, and behavior. Dev. Psychopathol. 2008, 20, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, D.A.; Budarf, M.L.; Emanuel, B.S. A genetic etiology for Di George syndrome: Consistent deletions and microdeletions of 22q11. Am. J. Hum. Genet. 1992, 50, 924–933. [Google Scholar] [PubMed]
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K.; et al. The International 22q11.2 Deletion Syndrome Consortium. Practical guidelines for managing patients with 22q11.2 deletion syndrome. J. Pediatr. 2011, 159, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Shprintzen, R.J. Velo-cardio-facial syndrome: 30 Years of study. Dev. Disabil. Res. Rev. 2008, 14, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Debbané, M.; Bassett, A.S.; Chow, E.W.; Fung, W.L.; Van Den Bree, M.; Owen, M.; Murphy, K.C.; Niarchou, M.; Kates, W.R.; et al. Psychiatric disorders from childhood to adulthood in 22q11.2 deletion syndrome: Results from the international consortium on brain and behavior in 22q11.2 deletion syndrome. Am. J. Psychiatry 2014, 171, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Holm, V.A.; Cassidy, B.S.; Butler, M.G.; Hanchett, J.M.; Greenswag, L.R.; Whitman, B.Y.; Greenberg, F. Prader-Willi syndrome: Consensus diagnostic criteria. Pediatrics 1993, 91, 398–402. [Google Scholar] [PubMed]
- Swab, D. Prader-Willi syndrome and the hypothalamus. Acta Pediatr. 1997, 86, 50–54. [Google Scholar] [CrossRef]
- State, M.W.; Dykens, E.M. Genetic and clinical advances in Prader–Willi syndrome: Genes, brain and behaviour. J. Am. Acad. Child. Adolesc. Psychiatry 2000, 39, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Dykens, E.M.; Roof, E. Behavior in Prader-Willi syndrome: Relationship to genetic subtypes and age. J. Child. Psychol. Psychiatry 2008, 49, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Capone, G.T. Down syndrome: Advances in molecular biology and the neurosciences. J. Dev. Behav. Pediatr. 2001, 22, 40–59. [Google Scholar] [CrossRef] [PubMed]
- Chapman, R.S.; Hesketh, L.J. Behavioural phenotype of individuals with Down syndrome. Ment. Retard. Dev. Disabil. Res. Rev. 2000, 6, 84–95. [Google Scholar] [CrossRef]
- Silverman, W. Down syndrome: Cognitive phenotype. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Dykens, E.M.; Hodapp, R.M.; Finucane, B.M. Genetics and Mental Retardation Syndromes; Paul H Brookes: New York, NY, USA, 2000. [Google Scholar]
- Yang, Y.; Conners, F.A.; Merrill, E.C. Visuo-spatial ability in individuals with Down syndrome: Is it really a strength? Res. Dev. Disabil. 2014, 35, 1473–1500. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Glemberg, M.C. Fragile X syndrome: Neural network models of sequencing and memory. Cogn. Syst. Res. 2008, 9, 274–292. [Google Scholar] [CrossRef] [PubMed]
- Klusek, J.; Hunt, A.W.; Mirrett, P.L.; Hatton, D.D.; Hooper, S.R.; Roberts, J.E.; Bailey, D.B., Jr. Reading and phonological skills in boys with fragile X syndrome. J. Autism Dev. Disord. 2015, 45, 1699–1711. [Google Scholar] [CrossRef] [PubMed]
- Laing, E.; Hulme, C.; Grant, J.; Karmiloff-Smith, A. Learning to read in Williams syndrome: Looking beneath the surface of atypical reading development. J. Child. Psychol. Psychiatry 2001, 42, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Menghini, D.; Verucci, L.; Vicari, S. Reading and phonological awareness in Williams syndrome. Neuropsychology 2004, 18, 29–37. [Google Scholar] [CrossRef] [PubMed]
- GarayzabalHeize, E.; Cuetos Vega, F. Aprendizaje de la Lectura en los Niños con Syndrome de Williams. Psicothema 2008, 20, 672–677. Available online: http://2011.www.redalyc.org/articulo.oa?id=72720425 (accessed on 17 October 2017).
- Swillen, A.; Vandeputte, L.; Cracco, J.; Maes, B.; Ghesquière, P.; Devriendt, K.; Fryns, J.P. Neuropsychological, Learning and Psychosocial Profile of Primary School Aged Children with the Velo-Cardio-Facial Syndrome (22q11 Deletion): Evidence for a Nonverbal Learning Disability? Child. Neuropsychol. 1999, 5, 230–241. [Google Scholar] [PubMed]
- Lewandowski, K.E.; Shashi, V.; Berry, P.M.; Kwapil, T.R. Schizophrenic-Like Neurocognitive Deficits in Children and Adolescents with 22q11 Deletion Syndrome. Am. J. Med. Genet. Part B 2007, 144B, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Cossu, G.; Rossini, F.; Marshall, J.C. When reading is acquired but phonemic awareness is not: A study of literacy in Down’s syndrome. Cognition 1993, 49, 129–138. [Google Scholar] [CrossRef]
- Gombert, J.E. Children with Down syndrome use phonological knowledge in reading. Read. Writ. 2002, 15, 455–469. [Google Scholar] [CrossRef]
- Snowling, M.J.; Hulme, C.; Mercer, R.C. A deficit in rime awareness in children with Down syndrome. Read. Writ. 2002, 15, 471–495. [Google Scholar] [CrossRef]
- Verucci, L.; Menghini, D.; Vicari, S. Reading skills and phonological awareness acquisition in Down syndrome. J. Intellect. Disabil. Res. 2006, 50, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Kay-Raining Bird, E.; Cleave, P.L.; With, D.; Pike, H.; Helmkay, A. Written and oral narratives of children and adolescents with Down syndrome. J. Speech Lang. Hear. Res. 2008, 51, 436–450. [Google Scholar] [CrossRef]
- Roch, M.; Jarrold, C. A comparison between word and nonword reading in Down syndrome: The role of phonological awareness. J. Commun. Disord. 2008, 41, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Nash, H.; Heat, J. The role of vocabulary, working memory and inference making ability in reading comprehension in Down syndrome. Res. Dev. Disabil. 2011, 32, 1782–1791. [Google Scholar] [CrossRef] [PubMed]
- Hulme, C.; Goetz, K.; Brigstcke, S.; Nash, H.M.; Lervag, A.; Snowling, M.J. The growth of reading skills in children with Down syndrome. Dev. Sci. 2012, 15, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Mengoni, S.E.; Nash, H.M.; Hulme, C. Learning to read new words in individuals with Down syndrome: Testing the role of phonological knowledge. Res. Dev. Disabil. 2014, 35, 1098–1109. [Google Scholar] [CrossRef] [PubMed]
- Lovell, S.J.; Conners, F.A. Reading skills in Down syndrome: An examination of orthographic knowledge. Am. J. Intellect. Dev. Disabil. 2016, 121, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Backman, J.E.; Mamen, M.; Ferguson, H. Reading-level design: Conceptual and methodological issues in reading research. Psychol. Bull. 1984, 96, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Bryant, P.E.; Goswami, U. Strengths and weaknesses of the reading level design: A comment on Backman, Mamen, and Ferguson. Psychol. Bull. 1986, 100, 101–103. [Google Scholar] [CrossRef]
- Jackson, N.E.; Butterfield, E.C. Reading-level-matched designs: Myths and realities. J. Read. Behav. 1989, 21, 387–412. [Google Scholar] [CrossRef]
- Mervis, C.B.; Robinson, B.F. Designing measures for profiling and genotype/phenotype studies of individual with genetic syndrome or developmental language disorders. Appl. Psycholinguist. 2005, 26, 41–64. [Google Scholar] [CrossRef]
- Zoccolotti, P.; De Luca, M.; Di Filippo, G.; Judica, A.; Martelli, M. Reading development in an orthographically regular language: Effects of length, frequency, lexicality and global processing ability. Read. Writ. 2009, 22, 1053–1079. [Google Scholar] [CrossRef]
- Rack, J.P.; Snowling, M.J.; Olson, R.K. The nonword reading deficit in developmental dyslexia: A review. Read. Res. Q. 1992, 27, 28–53. [Google Scholar] [CrossRef]
- Van Ijzendoorn, M.H.; Bus, A.G. Meta-analytic confirmation of the nonword reading deficit in developmental dyslexia. Read. Res. Q. 1994, 29, 266–275. [Google Scholar] [CrossRef]
- Herrmann, J.A.; Matyas, T.; Pratt, C. Meta-analysis of the nonword reading deficit in specific reading disorder. Dyslexia 2006, 12, 195–221. [Google Scholar] [CrossRef] [PubMed]
- Bamber, D. State-trace analysis: A method of testing simple theories of causation. J. Math. Psychol. 1979, 19, 137–181. [Google Scholar] [CrossRef]
- De Smedt, B.; Swillen, A.; Verschaffel, L.; Ghesquiere, P. Mathematical learning disabilities in children with 22q11.2 deletion syndrome: A review. Dev. Disabil. Res. Rev. 2009, 15, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Cossu, G.; Marshall, J.C. Are cognitive skills a prerequisite for learning to read and write? Cogn. Neuropsychol. 1990, 7, 21–40. [Google Scholar] [CrossRef]
- Groen, M.A.; Laws, G.; Nation, K.; Bishop, D.V.M. A case of exceptional reading accuracy in a child with Down syndrome: Underlying skills and the relation to reading comprehension. Cogn. Neuropsychol. 2006, 23, 1190–1214. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | n | Age at Assessment M (SD) Years | IQ | Decoding Skill Measures | Group-Matching Design | Decoding Skills: Findings | |
|---|---|---|---|---|---|---|---|
| FXS | Johnson-Glenberg (2008) [37] | n = 15 males with FXS n = 22 TD males n = 13 TD males | Mean age = 20.6 (range 11.5–38.1) Mean age = 5.5 (range 3.11–8.3) Mean age = 7.6 (range 5.4–8.3) | Mean mental age = 5.30 (SD = 1.26) (Stanford-Binet) | Accuracy: word identification (WRMT-R) word attack (WRMT-R) | Mental-age Word reading-age | FXS > TD mental age group on word identification TD age word reading group > FXS on word attack |
| FXS | Klusek et al. (2015) [38] | n = 51 males with FXS n = 35 TD males | Mean age = 10 (range 7.9–13.2) Mean age = 5.1 (range 3.3–7.4) | IQ = 56 (36–74) mean mental age = 5.4 (SD = 0.6) (range 4.1–6.7) (Leiter-r) | Accuracy: letter-word identification (WJ-R) word attack (WJ-R) | Mental-age | FXS > TD on letter-word identification FXS-TD = NS on word attack |
| WS | Laing et al. (2001) [39] | n = 15 males with WS n = 15 TD males | Mean age = 15.1 (range 9–27.7) Mean age = 6.9 (range 5–9.2) | General Cognitive Ability = 43.8 (SD = 5.12) (range 39 to 54) (BAS) | Accuracy: single word reading (WORD); nonword reading (GNRT) | Mental-age | WS > TD on word reading WS-TD = NS on nonword reading |
| WS | Menghini et al. (2004) [40] | n = 16; 10 males, 6 females with WS n = 16; 10 TD males, 6 TD females | Mean age = 17.7 (range 10.9–30.2) Chronological age range 6.2–8.6 | Mental age = 7 (range 5.2–10.2) (Stanford-Binet) | Accuracy: word reading nonword reading Speed: word reading nonword reading (DDE) | Mental-age | TD > WS on accuracy nonword; WS-TD = NS on word accuracy and on word and nonword speed |
| WS | Garayzabal-Heize et al. (2008) [41] | n = 12; 5 males, 7 females with WS n = 12; 6 TD males, 6 TD females | Mean age = 12.4 (range 8–15) Mean age = 7.9 (range 6–9) | Mean IQ = 50.6 (WISC) Mean agemental verbal = 7.8 (PPVT) | Accuracy: word reading nonword reading Speed: word reading nonword reading (PROLEC-R) | Mental-age | TD > WS on accuracy and speed word; TD-WS = NS on accuracy and speed nonword; |
| VCFS | Swillen et al. (1999) [42] | n = 9; 4 males, 5 females with VCFS | Mean age = 10.5 (range 6.10–12.10 years) | Mean FSIQ = 74 (SD = 3.70) (WISC-R) | Accuracy and speed: word decoding (Brus-EMT) Accuracy and speed: Klepel-Pseudoword-test | Raw scores obtained on each of the tests were standardized using published age-based norms (z-scores) | Mean z-scores word and pseudoword decoding = age-based norms. |
| VCFS | Lewandowski et al. (2007) [43] | n = 26, 16 males, 10 females with VCFS n = 25, 13 males, 12 females TD | Mean age = 9.3 (SD = 2.6) (range 7–16 years) Mean age = 9.7 (SD = 2.4) (range 7–16 years) | Mean FSIQ = 70.7 (SD = 12.4) (WISC-III) | Accuracy and automaticity: word reading (WIAT-II) Accuracy: pseudoword decoding (WIAT-II) | Chronological age and gender | TD > VCFS on word reading VCFS-TD = NS on pseudoword decoding |
| DS | Cossu et al. (1993) [44] | n = 10 DS n = 10 TD | Mean age = 11.4 (range 8–15.8 years) Mean age = 7.3 (range 6.9–7.9 years) | IQ = 44 (range 40–56) (WISC) | Accuracy: word reading nonword reading | Reading-level | TD-DS = NS on nonword reading |
| DS | Gombert (2002) [45] | n = 11 DS n = 11 TD | Mean age = 13.9 (range 10.5–20.0 years) Mean age = 7.1 (range 6.6–8.1 years) | IQ = 47 (range 44–50) (WISC) | Accuracy: word reading irregular word reading; nonword reading; (neighbor and non-neighbor) | Reading-level | TD-DS = NS on accuracy word and irregular reading TD-DS = NS on neighbor and non-neighbor nonword reading |
| DS | Snowling et al. (2002) [46] | n = 29 DS n = 31 TD | Mean age = 13.2 (range 6.11–17.6 years) Mean age = 5.3 (range 4.6–6.5 years) | Vocabulary: age equivalent in months = 4.1 (range 1.09–8.07) (BPVS) | Accuracy: single word reading (BAS) nonword reading (GNRT) | Reading-level | TD-DS = NSon nonword reading |
| DS | Verucci et al. (2006) [47] | n = 17 DS n = 17 TD | Mean age = 16.5 (range 7.7–28.5 years) Mean age = 7 (range 6.2–8.6 years) | Mental age = 6.2 (range 5.2–7.8) | Accuracy: word reading nonword reading Speed: word reading nonword reading (DDE) | Reading-level | TD > DS: on accuracy nonword reading TD-DS = NS on speed nonword reading |
| DS | Kay-Raining Bird et al. (2008) [48] | n = 20 DS n = 17 TD children | Mean age = 171.7 months (range 8.6–19.10 years) Mean age = 81.2 months (range 4.9–10.9 years) | Vocabulary age equivalent in months = 71.9 (SD = 23.1), (range 28–126) (PPVT-R) | Accuracy: word identification; word attack; (WRMT) | Reading-level | TD > DS: on nonword reading |
| DS | Roch et al. (2008) [49] | n = 12 DS n = 14 TD children | Mean age = 18 years 11 months (range 10.5–26.7) Mean age = 7 years 3 months (range 6.10–7.3) | Vocabulary: age equivalent in months = 97.17 (SD = 27.93) (BPVS-II) | Accuracy: word reading; nonword reading; Speed: word reading; nonword reading; | Reading-level | TD-DS = NS on speed nonword reading TD > DS: on accuracy nonword reading |
| DS | Nash et al. (2011) [50] | n = 13; 1 male, 12 females with DS n = 13 TD-reading ability, 2 males, 11 females n = 13 TD-comprehension ability, 6 males, 7 females n = 13 TD-poor comprehenders, 4 males, 9 females | Mean age (months) = 185.92 (range 11.4–19.3 years) Mean age (months) = 109.92 Mean age (months) = 103.23 Mean age (months) = 114.00 | Vocabulary knowledge = 83.92 (SD = 14.63) (BPVS-II) | Accuracy: single word reading (BAS-II) nonword reading (GNRT) | Reading-level | TD > DS: on nonword reading |
| DS | Hulme et al. (2012) [51] | n = 49 DS, 22 males, 27 females n = 61 TD, 31 males, 30 girls | Mean age = 13.8 (range 8–17 years) Mean age = 6.1 (range 5–7 years) | Non-verbal ability; naming vocabulary; (BAS-II) (BPVS-II) | Accuracy: word reading (EWRT; BAS-II) nonword reading | Reading-level | TD > DS: on accuracy word reading TD > DS: on nonword reading |
| DS | Mengoni et al. (2014) [52] | n = 16; 5 males, 11 females with DS n = 16 TD males | Mean age = 13.8 (range 8–17 years) Mean age = 6.1 (range 5–7 years) | Matrices age-equivalent = 5 (SD = 1.03) (range 4–7.03) (WPPSI-III) | Accuracy: word reading (YARC) nonword reading (GNRT) | Reading-level | DS > TD = on word reading DS-TD = NS on nonword reading |
| DS | Lovell et al. (2016) [53] | n = 20 DS, 8 males, 12 females; n = 20 TD, 12 males, 8 females | Mean age = 16.16 (range 11–20 years) Mean age = 7.33 (range 5–9 years) | IQ = 47.75 (SD = 8.73) (KBIT-2) | Accuracy: word identification (WRMT-III) word attack (WRMT-III) | Reading-level | TD > DS: on nonword reading |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Blasi, F.D.; Buono, S.; Città, S.; Costanzo, A.A.; Zoccolotti, P. Reading Deficits in Intellectual Disability Are still an Open Question: A Narrative Review. Brain Sci. 2018, 8, 146. https://doi.org/10.3390/brainsci8080146
Di Blasi FD, Buono S, Città S, Costanzo AA, Zoccolotti P. Reading Deficits in Intellectual Disability Are still an Open Question: A Narrative Review. Brain Sciences. 2018; 8(8):146. https://doi.org/10.3390/brainsci8080146
Chicago/Turabian StyleDi Blasi, Francesco Domenico, Serafino Buono, Santina Città, Angela Antonia Costanzo, and Pierluigi Zoccolotti. 2018. "Reading Deficits in Intellectual Disability Are still an Open Question: A Narrative Review" Brain Sciences 8, no. 8: 146. https://doi.org/10.3390/brainsci8080146
APA StyleDi Blasi, F. D., Buono, S., Città, S., Costanzo, A. A., & Zoccolotti, P. (2018). Reading Deficits in Intellectual Disability Are still an Open Question: A Narrative Review. Brain Sciences, 8(8), 146. https://doi.org/10.3390/brainsci8080146