
Acute Ischemic Stroke Treatment in Germany (2015–2023): Nationwide Trends in Thrombolysis and Thrombectomy by Age and Sex

Abstract
1. Introduction
2. Methods
2.1. Database
2.2. Study Population
2.3. Statistical Analyses
3. Results
3.1. AIS Incidence over Time
3.2. Intravenous Thrombolysis (IVT) Trends
3.3. Mechanical Thrombectomy (MT) Trends
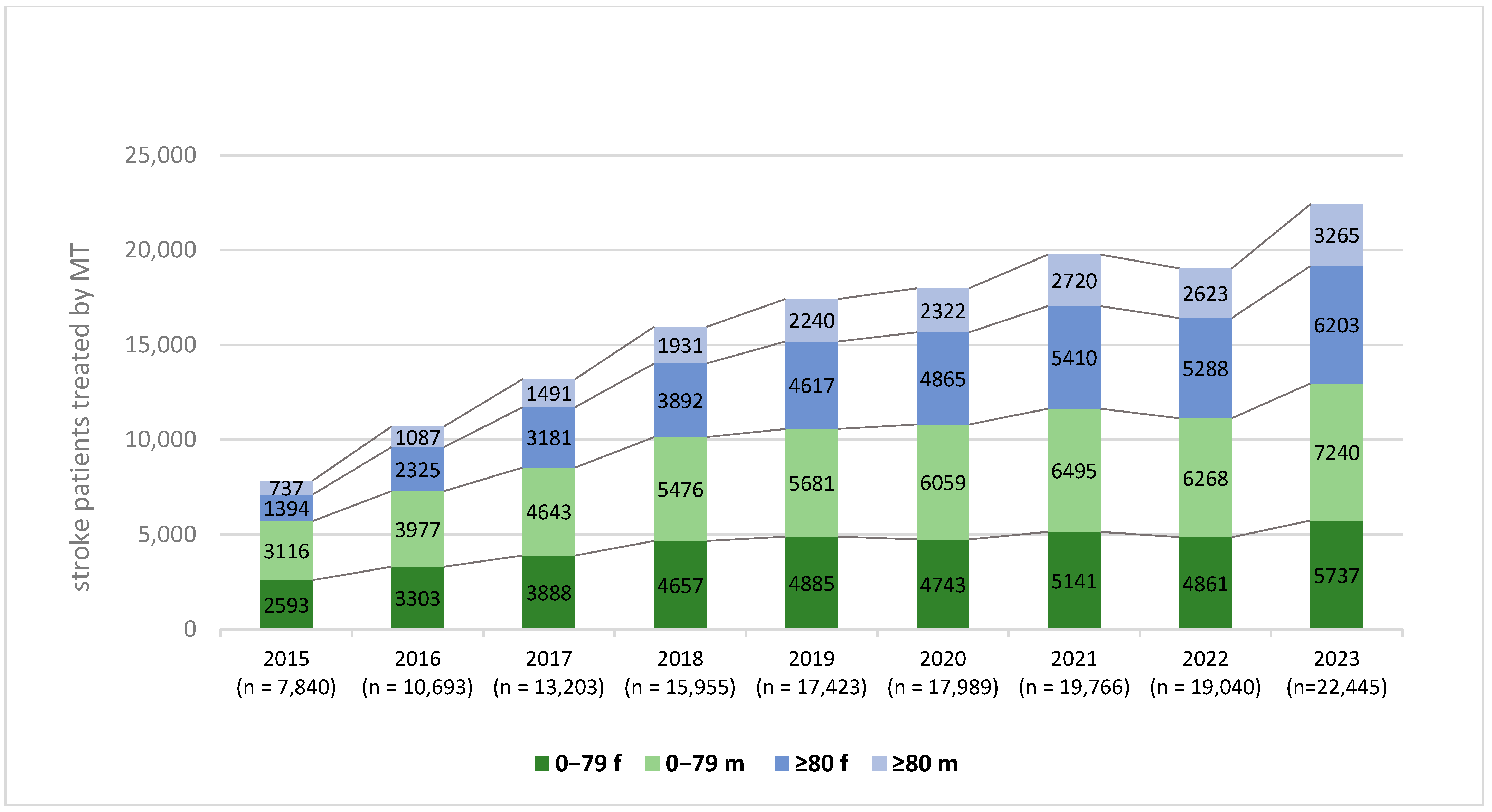
3.4. Age- and Sex-Specific Trends in MT
4. Discussion
4.1. Overview of Findings
4.2. Stroke Incidence During the COVID-19 Pandemic
4.3. Resilience of Acute Stroke Care Pathways
4.4. Demographic Shifts in Treatment Patterns
4.5. Expanded Indications and Evolving Clinical Practice
4.6. International Comparison and Potential for Further Growth
4.7. Implications for Health System Planning
4.8. Limitations
4.9. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Full Term |
| AIS | Acute Ischemic Stroke |
| IVT | Intravenous Thrombolysis |
| MT | Mechanical Thrombectomy |
| DRGs | Diagnosis-Related Groups |
| OPS | Operation and Procedure Codes |
| ICD-10 | International Classification of Diseases, 10th Revision |
| SU | Stroke Unit |
| TIA | Transient Ischemic Attack |
| SD | Standard Deviation |
| ICH | Intracerebral Hemorrhage |
| DAWN | Diffusion-weighted imaging or computerized tomography perfusion Assessment with clinical mismatch in the triage of Wake up and late-presenting strokes undergoing neurointervention (DAWN) trial |
| MDK | Medizinischer Dienst der Krankenversicherung (Medical Review Board of Health Insurers) |
References
- Fiehler, J.; Gerloff, C. Mechanical Thrombectomy in Stroke. Dtsch. Arztebl. Int. 2015, 112, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Weber, R.; Eyding, J.; Bartig, D.; Misselwitz, B.; Grau, A.; Hacke, W.; Krogias, C. Acute ischemic stroke care in Germany—Further progress from 2016 to 2019. Neurol. Res. Pract. 2021, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Berg, L.A.V.D.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Hammed, A.; Al-Qiami, A.; Alzawahreh, A.; Rosenbauer, J.; Nada, E.A.; Otmani, Z.; Hamam, N.G.; Alnajjar, A.Z.; Hammad, E.M.; Hamamreh, R.; et al. Comparative Effectiveness of Intravenous Thrombolysis plus Mechanical Thrombectomy versus Mechanical Thrombectomy Alone in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2024, 603–616. [Google Scholar] [CrossRef] [PubMed]
- Schroeter, M.; Klein, J.; Erbguth, F.; Kiefer, R.; Neumann-Haefelin, T.; Redecker, C.; Reese, H.; Schilling, M.; Steinmetz, H.; Fink, G.R. Ergebnisse der 14. Erhebung der Deutschen Gesellschaft für Neurologie zur Struktur der Neurologischen Kliniken mit Akutversorgungsauftrag in Deutschland [Results of the 14th survey conducted by the German Neurological Society on the structure of neurology centers with a mandate for acute care in Germany]. DGNeurologie 2021, 4, 332–344. [Google Scholar] [CrossRef]
- Eyding, J.; Misselwitz, B.; Weber, R.; Neumann-Haefelin, T.; Bartig, D.; Krogias, C. Vergleichbarkeit unterschiedlicher Datenquellen zur Schlaganfallversorgung in Deutschland [Comparability of different data sources on stroke care in Germany]. Der Nervenarzt 2020, 91, 877–890. [Google Scholar] [CrossRef] [PubMed]
- Kreis, K.; Neubauer, S.; Klora, M.; Lange, A.; Zeidler, J. Status and perspectives of claims data analyses in Germany-A systematic review. Health Policy 2016, 120, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt (Destatis). Diagnosedaten der Patienten und Patientinnen in Krankenhäusern (einschl. Sterbe- und Stundenfälle)—Fachserie 12 Reihe 6.2.1-2016; Wiesbaden: Statistisches Bundesamt, Germany, 2017; Available online: https://www.destatis.de (accessed on 20 November 2017).
- Statistisches Bundesamt (Destatis). Statistischer Bericht—Diagnosen der Krankenhauspatienten-2023; Wiesbaden: Statistisches Bundesamt, Germany, 2024; Available online: https://www-genesis.destatis.de/genesis/online?operation=abruftabelleBearbeiten&levelindex=1&levelid=1688134387037&auswahloperation=abruftabelleAuspraegungAuswaehlen&auswahlverzeichnis=ordnungsstruktur&auswahlziel=werteabruf&code=231310001&auswahltext=&nummer=3&variable=3&name=GES025&werteabruf=Werteabruf#abreadcrumb (accessed on 14 November 2024).
- Rizvi, R.F.; Craig, K.J.T.; Hekmat, R.; Reyes, F.; South, B.; Rosario, B.; Kassler, W.J.; Jackson, G.P. Effectiveness of non-pharmaceutical interventions related to social distancing on respiratory viral infectious disease outcomes: A rapid evidence-based review and meta-analysis. SAGE Open Med. 2021, 9, 20503121211022973. [Google Scholar] [CrossRef] [PubMed]
- Kucharski, A.J.; Klepac, P.; Conlan, A.J.K.; Kissler, S.M.; Tang, M.L.; Fry, H.; Gog, J.R.; Edmunds, W.J.; Emery, J.C.; Medley, G.; et al. Effectiveness of isolation, testing, contact tracing, and physical distancing on reducing transmission of SARS-CoV-2 in different settings: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Niemöller, U.; Tanislav, C.; Kostev, K. Incidences for Fractures 2017–2021: What Do We Learn from the COVID-19 Pandemic? Healthcare 2023, 11, 2804. [Google Scholar] [CrossRef] [PubMed]
- Tanislav, C.; Jacob, L.; Kostev, K. Consultations Decline for Stroke, Transient Ischemic Attack, and Myocardial Infarction during the COVID-19 Pandemic in Germany. Neuroepidemiology 2021, 55, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Tanislav, C.; Kostev, K. Fewer non-COVID-19 respiratory tract infections and gastrointestinal infections during the COVID-19 pandemic. J. Med. Virol. 2022, 94, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, V.; Mahfoud, F.; Lauder, L.; Reith, W.; Behnke, S.; Smola, S.; Rissland, J.; Pfuhl, T.; Scheller, B.; Böhm, M.; et al. Decline of emergency admissions for cardiovascular and cerebrovascular events after the outbreak of COVID-19. Clin. Res. Cardiol. 2020, 109, 1500–1506. [Google Scholar] [CrossRef] [PubMed]
- Hautz, W.E.; Sauter, T.C.; Exadakytlos, A.K.; Krummrey, G.; Schauber, S.; Müller, M. Barriers to seeking emergency care during the COVID-19 pandemic may lead to higher morbidity and mortality—a retrospective study from a Swiss university hospital. Swiss Med. Wkly. 2020, 150, w20331. [Google Scholar] [CrossRef] [PubMed]
- Gdovinová, Z.; Vitková, M.; Baráková, A.; Cvopová, A. The impact of the COVID-19 outbreak on acute stroke care in Slovakia: Data from across the country. Eur. J. Neurol. 2021, 28, 3263–3266. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Krishnamurthi, R.V.; Parmar, P.; Norrving, B.; Mensah, G.A.; Bennett, D.A.; Barker-Collo, S.; Moran, A.E.; Sacco, R.L.; Truelsen, T.; et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990–2013: The GBD 2013 Study. Neuroepidemiology 2015, 45, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Marzà-Florensa, A.; Kiss, P.; Youssef, D.M.; Jalali-Farahani, S.; Lanas, F.; Di Cesare, M.; Juanatey, J.R.G.; Taylor, S.; Uijl, A.; Grobbee, D.E.; et al. Sex Differences in Acute Coronary Syndromes: A Scoping Review Across the Care Continuum. Glob. Heart. 2025, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|---|---|---|---|
| Annual absolute frequency | 250,802 | 258,480 | 259,594 | 257,472 | 256,965 | 245,944 | 247,176 | 242,492 | 248,107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirsch, S.; Kostev, K.; Tanislav, C.; Hammed, A. Acute Ischemic Stroke Treatment in Germany (2015–2023): Nationwide Trends in Thrombolysis and Thrombectomy by Age and Sex. Brain Sci. 2025, 15, 832. https://doi.org/10.3390/brainsci15080832
Hirsch S, Kostev K, Tanislav C, Hammed A. Acute Ischemic Stroke Treatment in Germany (2015–2023): Nationwide Trends in Thrombolysis and Thrombectomy by Age and Sex. Brain Sciences. 2025; 15(8):832. https://doi.org/10.3390/brainsci15080832
Chicago/Turabian StyleHirsch, Sara, Karel Kostev, Christian Tanislav, and Ali Hammed. 2025. "Acute Ischemic Stroke Treatment in Germany (2015–2023): Nationwide Trends in Thrombolysis and Thrombectomy by Age and Sex" Brain Sciences 15, no. 8: 832. https://doi.org/10.3390/brainsci15080832
APA StyleHirsch, S., Kostev, K., Tanislav, C., & Hammed, A. (2025). Acute Ischemic Stroke Treatment in Germany (2015–2023): Nationwide Trends in Thrombolysis and Thrombectomy by Age and Sex. Brain Sciences, 15(8), 832. https://doi.org/10.3390/brainsci15080832