
White Matter Hyperintensities Mediate the Negative Impact of HbA1c Levels on Cognitive Function

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Cognitive Testing and Blood Draw
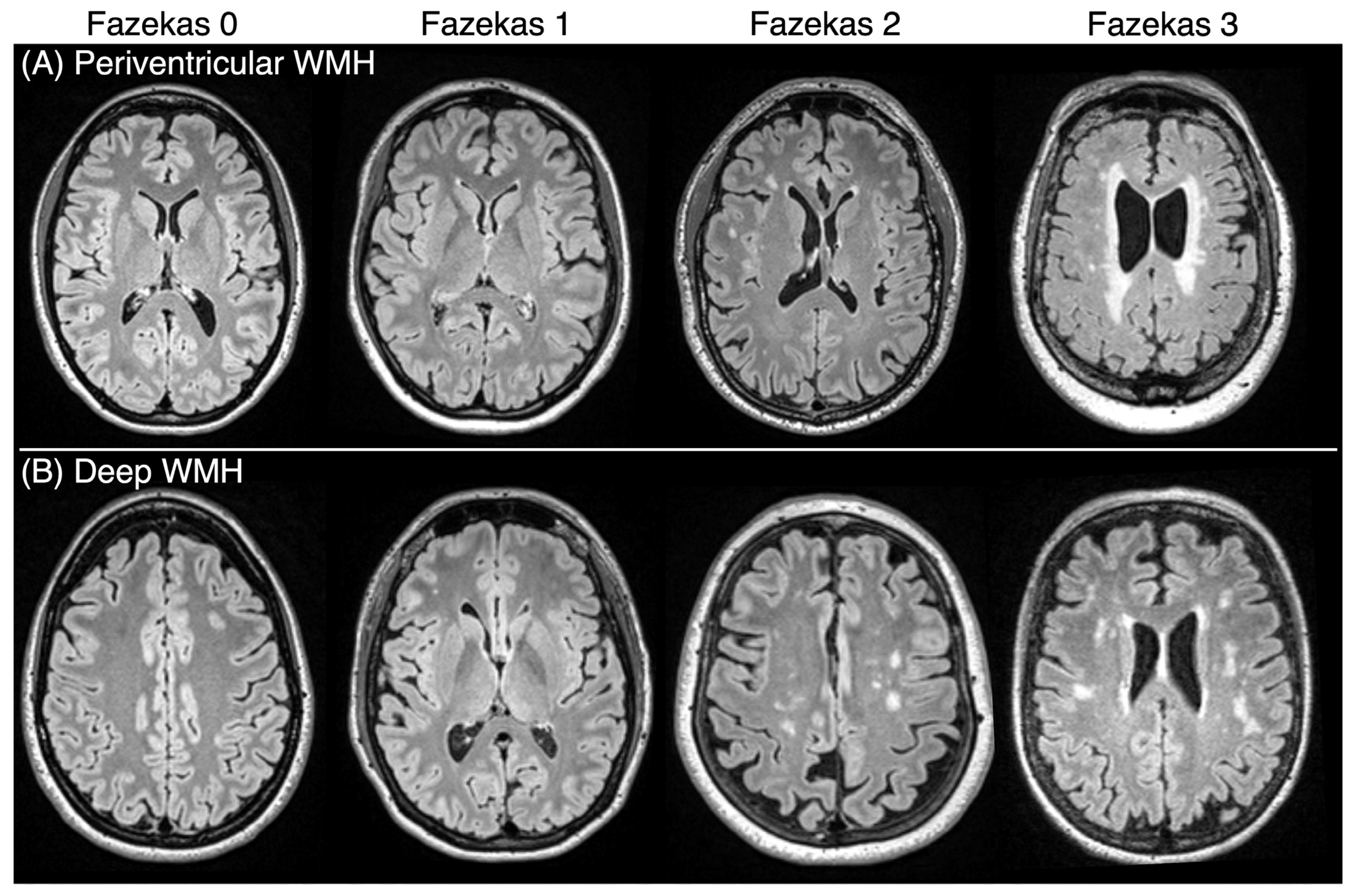
2.3. Neuroimaging/Quantifying WMHs
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Associations Between Hba1c, WMHs, and Cognition
3.3. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HbA1c | Hemoglobin A1c |
| MoCA | Montreal Cognitive Assessment |
| WMHs | White matter hyperintensities |
References
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, BMI.S38440. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, M.J.; Khan, S.K.; Pappachan, J.M.; Jeeyavudeen, M.S. Diabetes and cognitive function: An evidence-based current perspective. World J. Diabetes 2023, 14, 92–109. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Yan, L.; Yang, Z.; Zhong, B.; Xie, W. HbA1c, diabetes and cognitive decline: The English Longitudinal Study of Ageing. Diabetologia 2018, 61, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.J.; Al-Mamun, M.; Islam, M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused. Health Sci Rep. Health Sci Rep. 2024, 7, e2004. [Google Scholar] [CrossRef]
- Feinkohl, I.; Price, J.F.; Strachan, M.W.; Frier, B.M. The impact of diabetes on cognitive decline: Potential vascular, metabolic, and psychosocial risk factors. Alzheimer’s Res. Ther. 2015, 7, 46. [Google Scholar] [CrossRef]
- Milstein, J.L.; Ferris, H.A. The brain as an insulin-sensitive metabolic organ. Mol. Metab. 2021, 52, 101234. [Google Scholar] [CrossRef]
- Huang, C.-J.; Zhou, X.; Yuan, X.; Zhang, W.; Li, M.-X.; You, M.-Z.; Zhu, X.-Q.; Sun, Z.-W. Contribution of Inflammation and Hypoperfusion to White Matter Hyperintensities-Related Cognitive Impairment. Front. Neurol. 2022, 12, 786840. [Google Scholar] [CrossRef]
- Haller, S.; Kövari, E.; Herrmann, F.R.; Cuvinciuc, V.; Tomm, A.-M.; Zulian, G.B.; Lovblad, K.-O.; Giannakopoulos, P.; Bouras, C. Do brain T2/FLAIR white matter hyperintensities correspond to myelin loss in normal aging? A radiologic-neuropathologic correlation study. Acta Neuropathol. Commun. 2013, 1, 14. [Google Scholar] [CrossRef]
- Gupta, M.; Pandey, S.; Rumman, M.; Singh, B.; Mahdi, A.A. Molecular mechanisms underlying hyperglycemia associated cognitive decline. IBRO Neurosci. Rep. 2023, 14, 57–63. [Google Scholar] [CrossRef]
- Sun, J.; Xu, B.; Zhang, X.; He, Z.; Liu, Z.; Liu, R.; Nan, G. The Mechanisms of Type 2 Diabetes-Related White Matter Intensities: A Review. Front. Public Health 2020, 8, 498056. [Google Scholar] [CrossRef]
- van Sloten, T.T.; Sedaghat, S.; Carnethon, M.R.; Launer, L.J.; A Stehouwer, C.D. Cerebral microvascular complications of type 2 diabetes: Stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol. 2020, 8, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Grosu, S.; Lorbeer, R.; Hartmann, F.; Rospleszcz, S.; Bamberg, F.; Schlett, C.L.; Galie, F.; Selder, S.; Auweter, S.; Heier, M.; et al. White matter hyperintensity volume in pre-diabetes, diabetes and normoglycemia. BMJ Open Diabetes Res. Care 2021, 9, e002050. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.-Q.; Wang, L.; Wei, M.-M.; Xia, X.-S.; Tian, X.-L.; Cui, X.-H.; Li, X. Relationship Between Type 2 Diabetes and White Matter Hyperintensity: A Systematic Review. Front. Endocrinol. 2020, 11, 595962. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, N.; Son, S.J.; Aizenstein, H.; Yang, S.; Iordanova, B.; Hong, C.H.; Rho, H.W.; Cho, Y.H.; Park, B.; Kim, N.-R.; et al. Higher HbA1c Is Associated with Greater 2-Year Progression of White Matter Hyperintensities. Diabetes 2024, 73, 604–610. [Google Scholar] [CrossRef]
- Tamura, Y.; Kimbara, Y.; Yamaoka, T.; Sato, K.; Tsuboi, Y.; Kodera, R.; Chiba, Y.; Mori, S.; Fujiwara, Y.; Tokumaru, A.M.; et al. White Matter Hyperintensity in Elderly Patients with Diabetes Mellitus Is Associated with Cognitive Impairment, Functional Disability, and a High Glycoalbumin/Glycohemoglobin Ratio. Front. Aging Neurosci. 2017, 9, 220. [Google Scholar] [CrossRef]
- Moroni, F.; Ammirati, E.; Rocca, M.A.; Filippi, M.; Magnoni, M.; Camici, P.G. Cardiovascular disease and brain health: Focus on white matter hyperintensities. IJC Heart Vasc. 2018, 19, 63–69. [Google Scholar] [CrossRef]
- Hu, H.-Y.; Ou, Y.-N.; Shen, X.-N.; Qu, Y.; Ma, Y.-H.; Wang, Z.-T.; Dong, Q.; Tan, L.; Yu, J.-T. White matter hyperintensities and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 36 prospective studies. Neurosci. Biobehav. Rev. 2021, 120, 16–27. [Google Scholar] [CrossRef]
- Rijnhart, J.J.M.; Lamp, S.J.; Valente, M.J.; MacKinnon, D.P.; Twisk, J.W.R.; Heymans, M.W. Mediation analysis methods used in observational research: A scoping review and recommendations. BMC Med. Res. Methodol. 2021, 21, 226. [Google Scholar] [CrossRef]
- Newman-Norlund, R.D.; Newman-Norlund, S.E.; Sayers, S.; Nemati, S.; Riccardi, N.; Rorden, C.; Fridriksson, J. The Aging Brain Cohort (ABC) repository: The University of South Carolina’s multimodal lifespan database for studying the relationship between the brain, cognition, genetics and behavior in healthy aging. Neuroimage Rep. 2021, 1, 100008. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Lim, W.-Y.; Ma, S.; Heng, D.; Tai, E.S.; Khoo, C.M.; Loh, T.P. Screening for diabetes with HbA1c: Test performance of HbA1c compared to fasting plasma glucose among Chinese, Malay and Indian community residents in Singapore. Sci. Rep. 2018, 8, 12419. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Dohm-Hansen, S.; English, J.A.; Lavelle, A.; Fitzsimons, C.P.; Lucassen, P.J.; Nolan, Y.M. The ‘middle-aging’ brain. Trends Neurosci. 2024, 47, 259–272. [Google Scholar] [CrossRef]
- Zilliox, L.A.; Chadrasekaran, K.; Kwan, J.Y.; Russell, J.W. Diabetes and Cognitive Impairment. Curr. Diabetes Rep. 2016, 16, 87. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics (N = 205) | Mean (SD) or Percentage |
|---|---|
| Age (years) | 46.8 (19.9) |
| Sex (females:males) | 73.7%:25.9% |
| Race (percentage) | |
| Asian | 4.46% |
| African American | 11.88% |
| White | 83.66% |
| Hypertension (%) Highest Level of Education (percentage) | 18.54% |
| Completed High School | 9.27% |
| Completed at least one year of college or specialized training | 9.27% |
| Completed College/University | 41.95% |
| Completed Graduate School | 37.56% |
| Other | 0.98% |
| Socioeconomic Status | |
| High | 33.16% |
| Middle | 43.52% |
| Low | 23.32% |
| HbA1c (%) | 5.50 (0.62) |
| MoCA Total Score | 27.24 (2.56) |
| Fazekas Score Total | 2.55 (1.63) |
| Fazekas Score Deep | 1.08 (1.07) |
| Fazekas Score Periventricular | 1.47 (0.76) |
| Estimate | Standard Error | t Value | p Value | |
|---|---|---|---|---|
| Model 1. Dependent variable: MoCA score | ||||
| Model (R2 = 0.197, adjusted R2 = 0.185, p <0.001) | ||||
| Intercept | 35.243 | 1.584 | 22.254 | <0.001 |
| HbA1c | −1.441 | 0.292 | −4.936 | <0.001 |
| Hypertension | −0.372 | 0.467 | −0.797 | 0.427 |
| Model 2. Dependent variable: Fazekas score | ||||
| Model (R2 = 0.136, adjusted R2 = 0.127, p <0.001) | ||||
| Intercept | −0.736 | 1.011 | −0.728 | 0.468 |
| HbA1c | 0.565 | 0.186 | 3.029 | 0.003 |
| Hypertension | 0.939 | 0.298 | 3.147 | 0.002 |
| Model 3. Dependent variable: MoCA score | ||||
| Model (R2 = 0.197, R2 = 0.189, p < 0.001) | ||||
| Intercept | 34.951 | 1.538 | 22.728 | <0.001 |
| Fazekas Score | −0.397 | 0.107 | −3.713 | <0.001 |
| HbA1c | −1.217 | 0.290 | −4.204 | <0.001 |
| Hypertension | 0.0003 | 0.464 | 0.001 | 0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnstone, R.; Rangus, I.; Busby, N.; Wilmskoetter, J.; Riccardi, N.; Newman-Norlund, S.; Newman-Norlund, R.; Rorden, C.; Fridriksson, J.; Bonilha, L. White Matter Hyperintensities Mediate the Negative Impact of HbA1c Levels on Cognitive Function. Brain Sci. 2025, 15, 692. https://doi.org/10.3390/brainsci15070692
Johnstone R, Rangus I, Busby N, Wilmskoetter J, Riccardi N, Newman-Norlund S, Newman-Norlund R, Rorden C, Fridriksson J, Bonilha L. White Matter Hyperintensities Mediate the Negative Impact of HbA1c Levels on Cognitive Function. Brain Sciences. 2025; 15(7):692. https://doi.org/10.3390/brainsci15070692
Chicago/Turabian StyleJohnstone, Rudolph, Ida Rangus, Natalie Busby, Janina Wilmskoetter, Nicholas Riccardi, Sarah Newman-Norlund, Roger Newman-Norlund, Chris Rorden, Julius Fridriksson, and Leonardo Bonilha. 2025. "White Matter Hyperintensities Mediate the Negative Impact of HbA1c Levels on Cognitive Function" Brain Sciences 15, no. 7: 692. https://doi.org/10.3390/brainsci15070692
APA StyleJohnstone, R., Rangus, I., Busby, N., Wilmskoetter, J., Riccardi, N., Newman-Norlund, S., Newman-Norlund, R., Rorden, C., Fridriksson, J., & Bonilha, L. (2025). White Matter Hyperintensities Mediate the Negative Impact of HbA1c Levels on Cognitive Function. Brain Sciences, 15(7), 692. https://doi.org/10.3390/brainsci15070692