
Neuroradiological Evaluation of Anatomo-Morphometric Arcuate Fascicle Modifications According to Different Brain Tumor Histotypes: An Italian Multicentric Study

 ,
,  ,
,  , ,
, ,  ,
,  ,
,  , ,
, ,  ,
,  , , ,
, , ,  , , , ,
, , , ,  , add
Show full author list
, add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. MRI Acquisition and Tractography Analysis
2.3. Statistical Analysis
3. Results
- Regression analysis
3.1. Results
3.2. Results of the Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giampiccolo, D.; Parmigiani, S.; Basaldella, F.; Russo, S.; Pigorini, A.; Rosanova, M.; Cattaneo, L.; Sala, F. Recording Cortico-Cortical Evoked Potentials of the Human Arcuate Fasciculus under General Anaesthesia. Clin. Neurophysiol. 2021, 132, 1966–1973. [Google Scholar] [CrossRef] [PubMed]
- Dick, A.S.; Tremblay, P. Beyond the Arcuate Fasciculus: Consensus and Controversy in the Connectional Anatomy of Language. Brain 2012, 135, 3529–3550. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, R.; Yordanova, Y.N.; Duffau, H.; Herbet, G. Neuropsychological Evidence for the Crucial Role of the Right Arcuate Fasciculus in the Face-Based Mentalizing Network: A Disconnection Analysis. Neuropsychologia 2018, 115, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Altieri, R.; Certo, F.; Rocca, G.L.; Melcarne, A.; Garbossa, D.; Bianchi, A.; Crimi, S.; Pluchino, A.; Peschillo, S.; Barbagallo, G.M.V. Radiological Evaluation of Ex Novo High Grade Glioma: Velocity of Diametric Expansion and Acceleration Time Study. Radiol. Oncol. 2020, 55, 26–34. [Google Scholar] [CrossRef]
- Rauch, P.; Gmeiner, M.; Aichholzer, M.; Sterrer, M.; Wagner, H.; Katletz, S.; Serra, C.; Böhm, P.; Sonnberger, M.; Stroh, N.; et al. Low-Grade Gliomas Do Not Grow along White Matter Tracts: Evidence from Quantitative Imaging. Brain Commun. 2025, 7, fcaf157. [Google Scholar] [CrossRef]
- Shen, E.; Van Swearingen, A.E.D.; Price, M.J.; Bulsara, K.; Verhaak, R.G.W.; Baëta, C.; Painter, B.D.; Reitman, Z.J.; Salama, A.K.S.; Clarke, J.M.; et al. A Need for More Molecular Profiling in Brain Metastases. Front. Oncol. 2021, 11, 785064. [Google Scholar] [CrossRef]
- Altieri, R.; Corvino, S.; La Rocca, G.; Cofano, F.; Melcarne, A.; Garbossa, D.; Barbarisi, M. Clinical Implication of Brain Metastases En-Bloc Resection: Surgical Technique Description and Literature Review. J. Pers. Med. 2024, 14, 1110. [Google Scholar] [CrossRef]
- Corvino, S.; Altieri, R.; La Rocca, G.; Piazza, A.; Corazzelli, G.; Palmiero, C.; Mariniello, G.; Maiuri, F.; Elefante, A.; de Divitiis, O. Topographic Patterns of Intracranial Meningioma Recurrences-Systematic Review with Clinical Implication. Cancers 2024, 16, 2267. [Google Scholar] [CrossRef]
- Catani, M.; Thiebaut de Schotten, M. A Diffusion Tensor Imaging Tractography Atlas for Virtual in Vivo Dissections. Cortex 2008, 44, 1105–1132. [Google Scholar] [CrossRef]
- Forkel, S.J.; Thiebaut de Schotten, M.; Kawadler, J.M.; Dell’Acqua, F.; Danek, A.; Catani, M. The Anatomy of Fronto-Occipital Connections from Early Blunt Dissections to Contemporary Tractography. Cortex 2014, 56, 73–84. [Google Scholar] [CrossRef]
- Thiebaut de Schotten, M.; ffytche, D.H.; Bizzi, A.; Dell’Acqua, F.; Allin, M.; Walshe, M.; Murray, R.; Williams, S.C.; Murphy, D.G.M.; Catani, M. Atlasing Location, Asymmetry and Inter-Subject Variability of White Matter Tracts in the Human Brain with MR Diffusion Tractography. NeuroImage 2011, 54, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Catani, M.; Howard, R.J.; Pajevic, S.; Jones, D.K. Virtual in Vivo Interactive Dissection of White Matter Fasciculi in the Human Brain. NeuroImage 2002, 17, 77–94. [Google Scholar] [CrossRef]
- Mandonnet, E.; Sarubbo, S.; Duffau, H. Proposal of an Optimized Strategy for Intraoperative Testing of Speech and Language during Awake Mapping. Neurosurg. Rev. 2016, 40, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Mandonnet, E.; Delattre, J.Y.; Tanguy, M.L.; Swanson, K.R.; Carpentier, A.F.; Duffau, H.; Cornu, P.; Van Effenterre, R.; Alvord, E.C., Jr.; Capelle, L. Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann. Neurol. 2003, 53, 524–528. [Google Scholar] [CrossRef]
- Altieri, R.; Hirono, S.; Duffau, H.; Ducati, A.; Fontanella, M.; LA Rocca, G.; Melcarne, A.; Panciani, P.P.; Spena, G.; Garbossa, D. Natural History of de Novo High Grade Glioma: First Description of Growth Parabola. J. Neurosurg. Sci. 2017, 64, 399–403. [Google Scholar] [CrossRef]
- Pallud, J.; Taillandier, L.; Capelle, L.; Fontaine, D.; Peyre, M.; Ducray, F.; Duffau, H.; Mandonnet, E. Quantitative Morphological Magnetic Resonance Imaging Follow-up of Low-Grade Glioma: A Plea for Systematic Measurement of Growth Rates. Neurosurgery 2012, 71, 729–739. [Google Scholar] [CrossRef]
- Eidel, O.; Burth, S.; Neumann, J.-O.; Kieslich, P.J.; Sahm, F.; Jungk, C.; Kickingereder, P.; Bickelhaupt, S.; Mundiyanapurath, S.; Bäumer, P.; et al. Tumor Infiltration in Enhancing and Non-Enhancing Parts of Glioblastoma: A Correlation with Histopathology. PLoS ONE 2017, 12, e0169292. [Google Scholar] [CrossRef]
- Altieri, R.; Certo, F.; Pacella, D.; Cammarata, G.; Garozzo, M.; Broggi, G.; Caltabiano, R.; Magro, G.; Russo, G.; Cosentino, S.; et al. Metabolic Delineation of IDH1 Wild-Type Glioblastoma Surgical Anatomy: How to Plan the Tumor Extent of Resection. J. Neuro-Oncol. 2023, 162, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Zlatescu, M.C.; TehraniYazdi, A.R.; Sasaki, H.; Megyesi, J.F.; Betensky, R.A.; Louis, D.N.; Cairncross, J.G. Tumor Location and Growth Pattern Correlate with Genetic Signature in Oligodendroglial Neoplasms. Cancer Res. 2001, 61, 6713–6715. [Google Scholar]
- Sun, Y.; Wang, X.; Zhang, D.Y.; Zhang, Z.; Bhattarai, J.P.; Wang, Y.; Park, K.H.; Dong, W.; Hung, Y.-F.; Yang, Q.; et al. Brain-Wide Neuronal Circuit Connectome of Human Glioblastoma. Nature 2025, 641, 222–231. [Google Scholar] [CrossRef]
- Wei, Y.; Li, C.; Cui, Z.; Mayrand, R.C.; Zou, J.; Wong, A.L.K.C.; Sinha, R.; Matys, T.; Schönlieb, C.-B.; Price, S.J. Structural Connectome Quantifies Tumour Invasion and Predicts Survival in Glioblastoma Patients. Brain 2023, 146, 1714–1727. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Hong, C.P.; Kwon, Y.H.; Hwang, Y.T.; Kim, J.H.; Park, J.W. Curvature Range Measurements of the Arcuate Fasciculus Using Diffusion Tensor Tractography. Neural Regen. Res. 2013, 8, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Diffuse Low-Grade Gliomas and Neuroplasticity. Diagn. Interv. Imaging 2014, 95, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Ius, T.; Angelini, E.; Thiebaut de Schotten, M.; Mandonnet, E.; Duffau, H. Evidence for Potentials and Limitations of Brain Plasticity Using an Atlas of Functional Resectability of WHO Grade II Gliomas: Towards a “Minimal Common Brain”. NeuroImage 2011, 56, 992–1000. [Google Scholar] [CrossRef]
- Duffau, H. Hodotopy, Neuroplasticity and Diffuse Gliomas. Neurochirurgie 2017, 63, 259–265. [Google Scholar] [CrossRef]
- Altieri, R.; Melcarne, A.; Junemann, C.; Zeppa, P.; Zenga, F.; Garbossa, D.; Certo, F.; Barbagallo, G. Inferior Fronto-Occipital Fascicle Anatomy in Brain Tumor Surgeries: From Anatomy Lab to Surgical Theater. J. Clin. Neurosci. 2019, 68, 290–294. [Google Scholar] [CrossRef]
- Sarubbo, S.; De Benedictis, A.; Merler, S.; Mandonnet, E.; Barbareschi, M.; Dallabona, M.; Chioffi, F.; Duffau, H. Structural and Functional Integration between Dorsal and Ventral Language Streams as Revealed by Blunt Dissection and Direct Electrical Stimulation. Human. Brain Mapp. 2016, 37, 3858–3872. [Google Scholar] [CrossRef]
- Guerrini, F.; Roca, E.; Spena, G. Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic. Brain Sci. 2022, 12, 652. [Google Scholar] [CrossRef]
- Aabedi, A.A.; Young, J.S.; Chang, E.F.; Berger, M.S.; Hervey-Jumper, S.L. Involvement of White Matter Language Tracts in Glioma: Clinical Implications, Operative Management, and Functional Recovery After Injury. Front. Neurosci. 2022, 16, 932478. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Morshed, R.A.; Berger, M.S. FLAIRectomy: Resecting beyond the Contrast Margin for Glioblastoma. Brain Sci. 2022, 12, 544. [Google Scholar] [CrossRef]
- Altieri, R.; Cammarata, G.; Grasso, E.; Certo, F.; Barbagallo, G. Circumferential or Sulcus-Guided Resection of Rolandic IDH1 Wildtype Glioblastoma: How I Do It: 2-Dimensional Operative Video. Oper. Neurosurg. 2023, 25, e49. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.; Virtuoso, A.; Papa, M.; Certo, F.; Barbagallo, G.M.V.; Altieri, R. Regional Development of Glioblastoma: The Anatomical Conundrum of Cancer Biology and Its Surgical Implication. Cells 2022, 11, 1349. [Google Scholar] [CrossRef] [PubMed]
- Altieri, R.; Raimondo, S.; Tiddia, C.; Sammarco, D.; Cofano, F.; Zeppa, P.; Monticelli, M.; Melcarne, A.; Junemann, C.; Zenga, F.; et al. Glioma Surgery: From Preservation of Motor Skills to Conservation of Cognitive Functions. J. Clin. Neurosci. 2019, 70, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, A.-L.; Herbet, G.; Duffau, H.; Lafargue, G. Preserved Metacognitive Ability despite Unilateral or Bilateral Anterior Prefrontal Resection. Brain Cogn. 2018, 120, 48–57. [Google Scholar] [CrossRef]
- Nikolova Yordanova, Y.; Duffau, H.; Herbet, G. Neural Pathways Subserving Face-Based Mentalizing. Brain Struct. Funct. 2017, 222, 3087–3105. [Google Scholar] [CrossRef]
- Altieri, R.; Bianconi, A.; Caneva, S.; Cirillo, G.; Cofano, F.; Corvino, S.; de Divitiis, O.; Pepa, G.M.D.; De Luca, C.; Fiaschi, P.; et al. Quantitative Evaluation of Neuroradiological and Morphometric Alteration of Inferior Fronto-Occipital Fascicle across Different Brain Tumor Histotype: An Italian Multicentric Study. Acta Neurochir. 2025, 167, 71. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | N = 156 |
|---|---|
| Sex | |
| Female | 73 (47%) |
| Male | 83 (53%) |
| Age | 59 (13) |
| Diagnosis | |
| GBM | 98 (63%) |
| LGG | 26 (17%) |
| Meningioma | 14 (9.0%) |
| Met | 18 (12%) |
| Location | |
| Bilateral frontal | 1 (0.6%) |
| Clinoid | 1 (0.6%) |
| Frontal | 45 (29%) |
| Frontal insular | 2 (1.3%) |
| Fronto-parietal | 7 (4.5%) |
| Fronto-temporal | 4 (2.6%) |
| Fronto-temporo-insular | 6 (3.8%) |
| Insular | 1 (0.6%) |
| Occipital | 1 (0.6%) |
| Parasagittal | 1 (0.6%) |
| Parietal | 16 (10%) |
| Parieto-occipital | 8 (5.1%) |
| Parieto-temporal | 4 (2.6%) |
| Temporal | 44 (28%) |
| Temporal–parietal | 9 (5.8%) |
| Temporo-insular | 4 (2.6%) |
| Temporo-occipitale | 1 (0.6%) |
| Thalamic | 1 (0.6%) |
| Side | |
| Left | 109 (70%) |
| Right | 47 (30%) |
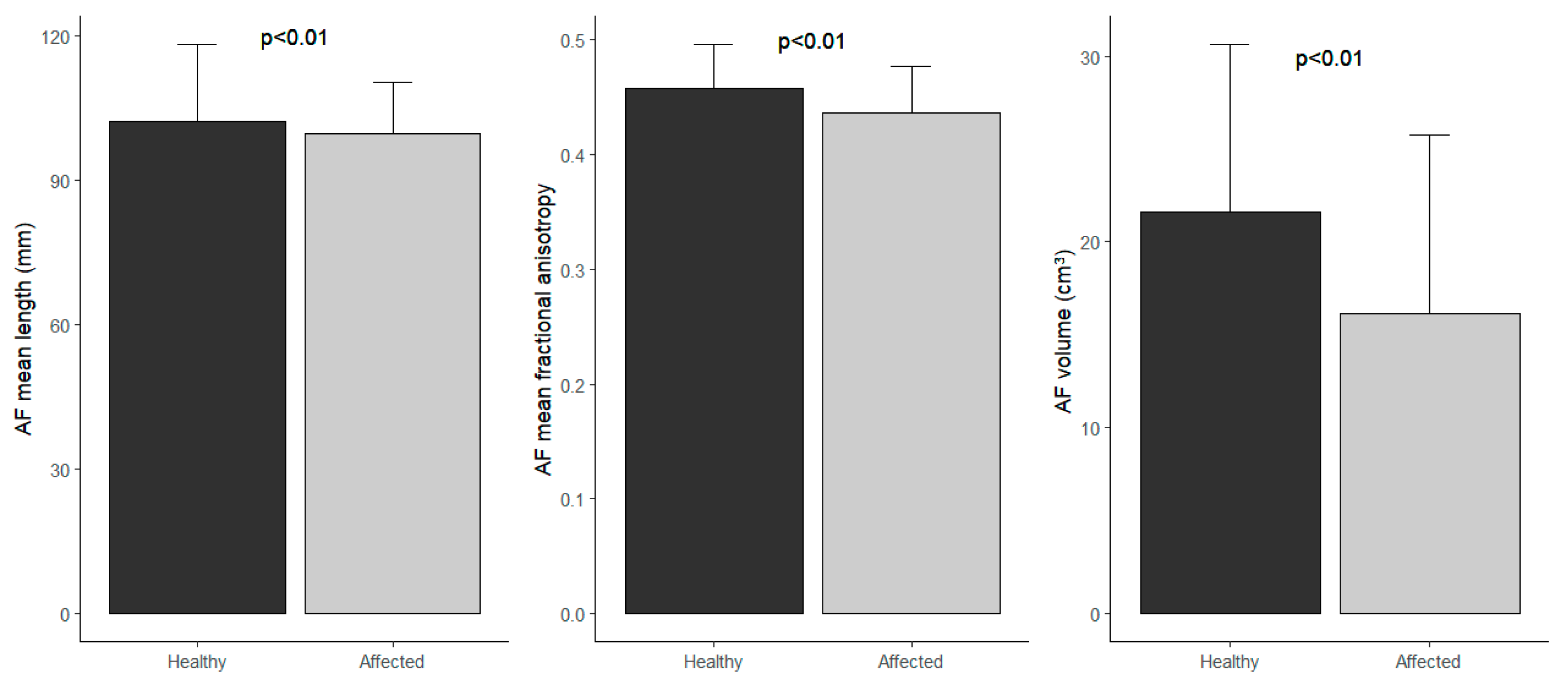
| Affected arcuate fascicle mean length mm | 100 (11) |
| Affected arcuate fascicle mean fractional anisotropy | 0.44 (0.04) |
| Affected arcuate fascicle volume cm3 | 16 (10) |
| Healthy arcuate fascicle mean length mm | 102 (16) |
| Healthy arcuate fascicle mean fractional anisotropy | 0.46 (0.04) |
| Healthy arcuate fascicle volume cm3 | 22 (9) |
| Tumor volume Enhancing Nodule | 25 (21) |
| Volume of FLAIR hyperintensity beyond EN | 49 (34) |
| Outcome: Arcuate Fascicle Mean Length (mm) | Outcome: Arcuate Fascicle Mean Fractional Anisotropy | Outcome: Arcuate Fascicle Volume cm3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Adjusted Beta | 95% CI | p-Value | Adjusted Beta | 95% CI | p-Value | Adjusted Beta | 95% CI | p-Value |
| Group | |||||||||
| Affected | — | — | — | — | — | — | |||
| Healthy | 2.5 | 0.62, 4.5 | 0.010 | 0.02 | 0.01, 0.03 | <0.001 | 5.4 | 3.9, 7.0 | <0.001 |
| Sex | |||||||||
| Female | — | — | — | — | — | — | |||
| Male | 2.7 | −0.51, 5.9 | 0.099 | 0.01 | 0.00, 0.02 | 0.013 | 3.1 | 0.67, 5.5 | 0.013 |
| Age | −0.14 | −0.30, 0.01 | 0.068 | 0.00 | 0.00, 0.00 | 0.059 | 0.00 | −0.12, 0.12 | 0.994 |
| Diagnosis | |||||||||
| GBM | — | — | — | — | — | — | |||
| LGG | −9.3 | −15, −3.1 | 0.003 | 0.01 | −0.01, 0.03 | 0.333 | 5.2 | 0.56, 9.8 | 0.028 |
| Meningioma | 19 | 14, 25 | <0.001 | 0.01 | −0.01, 0.03 | 0.166 | −5.9 | −10, −1.6 | 0.008 |
| Met | 4.0 | −1.2, 9.1 | 0.129 | 0.01 | −0.01, 0.03 | 0.273 | −2.1 | −6.0, 1.7 | 0.278 |
| Side | |||||||||
| Left | — | — | — | — | — | — | |||
| Right | 0.14 | −3.4, 3.7 | 0.936 | 0.00 | −0.01, 0.01 | 0.958 | −0.29 | −2.9, 2.4 | 0.827 |
| Tumor Volume Enhancing Nodule | −0.19 | −0.29, −0.08 | <0.001 | 0.00 | 0.00, 0.00 | 0.323 | 0.07 | −0.01, 0.14 | 0.097 |
| Volume of FLAIR Hyperintensity Beyond EN | 0.02 | −0.03, 0.08 | 0.434 | 0.00 | 0.00, 0.00 | 0.107 | −0.05 | −0.09, −0.01 | 0.026 |
| Outcome: Arcuate Fascicle Mean Fractional Anisotropy | Outcome: Arcuate Fascicle Volume (cm3) | |||||
|---|---|---|---|---|---|---|
| Characteristic | Adjusted Beta | 95% CI | p-Value | Adjusted Beta | 95% CI | p-Value |
| Group | ||||||
| Affected | — | — | — | — | ||
| Healthy | 0.02 | 0.02, 0.03 | <0.001 | 6.6 | 4.6, 8.6 | <0.001 |
| Sex | ||||||
| Female | — | — | — | — | ||
| Male | 0.00 | −0.01, 0.02 | 0.382 | 2.7 | −0.46, 5.8 | 0.094 |
| Age | 0.00 | 0.00, 0.00 | 0.299 | 0.00 | −0.16, 0.16 | 0.985 |
| Side | ||||||
| Left | — | — | — | — | ||
| Right | 0.00 | −0.01, 0.01 | 0.807 | −0.03 | −3.5, 3.4 | 0.985 |
| Tumor Volume Enhancing Nodule | 0.00 | 0.00, 0.00 | 0.743 | 0.08 | −0.02, 0.17 | 0.100 |
| Volume of FLAIR Hyperintensity Beyond EN | 0.0001 | 0.0000, 0.0001 | 0.012 | −0.04 | −0.09, 0.02 | 0.168 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, R.; Bianconi, A.; Caneva, S.; Cirillo, G.; Cofano, F.; Corvino, S.; de Divitiis, O.; Della Pepa, G.M.; De Luca, C.; Fiaschi, P.; et al. Neuroradiological Evaluation of Anatomo-Morphometric Arcuate Fascicle Modifications According to Different Brain Tumor Histotypes: An Italian Multicentric Study. Brain Sci. 2025, 15, 625. https://doi.org/10.3390/brainsci15060625
Altieri R, Bianconi A, Caneva S, Cirillo G, Cofano F, Corvino S, de Divitiis O, Della Pepa GM, De Luca C, Fiaschi P, et al. Neuroradiological Evaluation of Anatomo-Morphometric Arcuate Fascicle Modifications According to Different Brain Tumor Histotypes: An Italian Multicentric Study. Brain Sciences. 2025; 15(6):625. https://doi.org/10.3390/brainsci15060625
Chicago/Turabian StyleAltieri, Roberto, Andrea Bianconi, Stefano Caneva, Giovanni Cirillo, Fabio Cofano, Sergio Corvino, Oreste de Divitiis, Giuseppe Maria Della Pepa, Ciro De Luca, Pietro Fiaschi, and et al. 2025. "Neuroradiological Evaluation of Anatomo-Morphometric Arcuate Fascicle Modifications According to Different Brain Tumor Histotypes: An Italian Multicentric Study" Brain Sciences 15, no. 6: 625. https://doi.org/10.3390/brainsci15060625
APA StyleAltieri, R., Bianconi, A., Caneva, S., Cirillo, G., Cofano, F., Corvino, S., de Divitiis, O., Della Pepa, G. M., De Luca, C., Fiaschi, P., Galieri, G., Garbossa, D., La Rocca, G., Marino, S., Mazzucchi, E., Menna, G., Mezzogiorno, A., Morello, A., Olivi, A., ... Barbarisi, M. (2025). Neuroradiological Evaluation of Anatomo-Morphometric Arcuate Fascicle Modifications According to Different Brain Tumor Histotypes: An Italian Multicentric Study. Brain Sciences, 15(6), 625. https://doi.org/10.3390/brainsci15060625