
Suicide, Psychoactive Substances, and Homelessness: A Scoping Review

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Risk Factors Related to Suicide in SUD
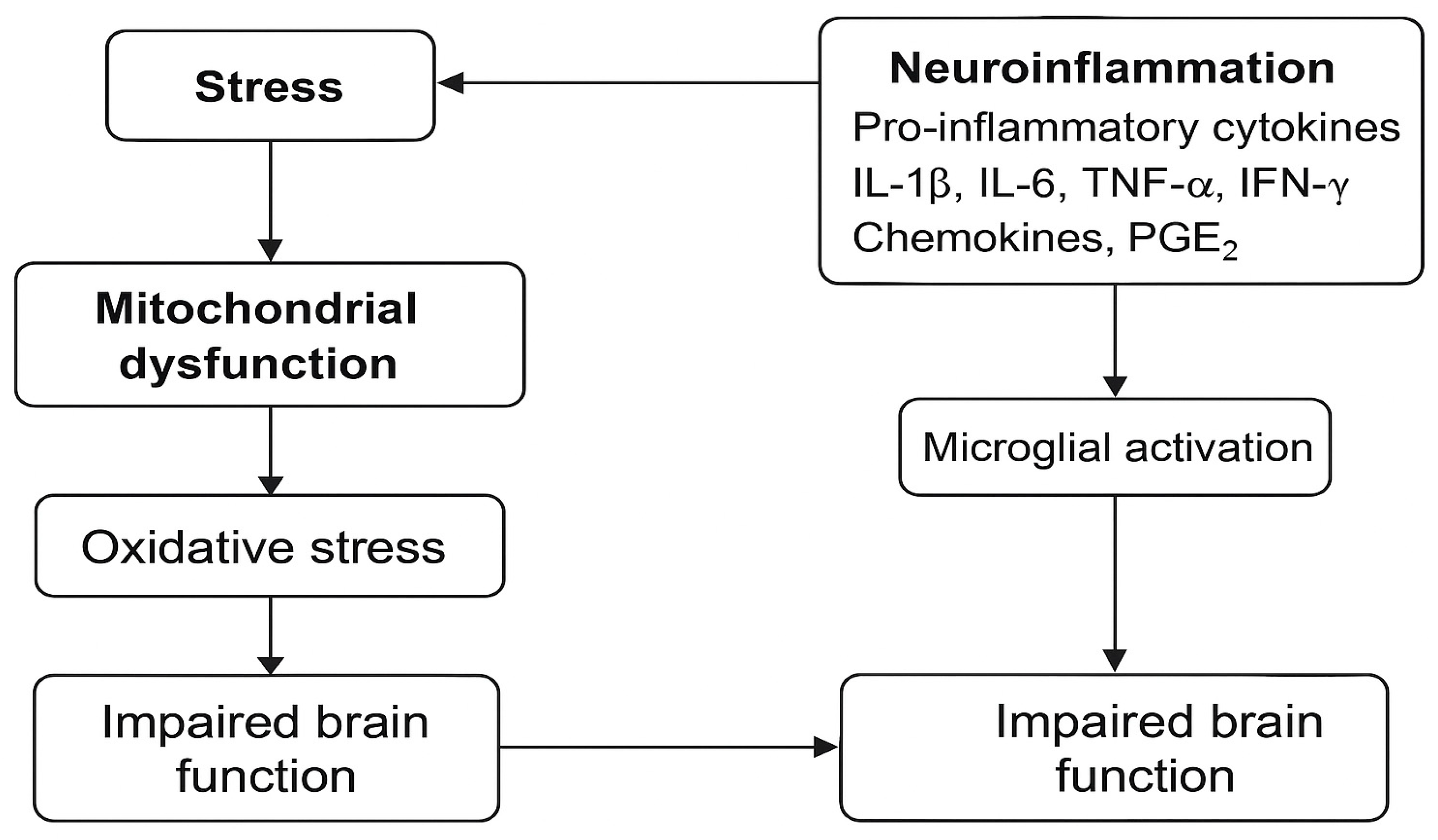
3.2. Neuroimmunological and Neuroinflammatory Aspects in the Context of Psychoactive Substance Use and Suicide in SUD
3.3. The Relationship Between Psychoactive Substance Use and Suicide in SUD
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Governo Federal. Política Nacional para Inclusão Social da População em Situação de Rua; Governo Federal: Brasília, Brazil, 2008.
- Silva, L.F.S. População em Situação de rua Supera 281,4 mil Pessoas no Brasil; Instituto de Pesquisa Econômica Aplicada (IPEA): Brasília, Brazil, 2022.
- Fundação de Amparo à Pesquisa do Estado de São Paulo. New Census and Housing Program for the Homeless Population. Revista Pesquisa FAPESP, 2023. Available online: https://revistapesquisa.fapesp.br/en/new-census-and-housing-program-for-the-homeless-population/ (accessed on 29 May 2025).
- Campos, D.A.; Morefli-Pires, R.O. Trajetórias sociais de gays e lésbicas moradores de rua de Florianópolis (SC), 2016. Rev. Estud. Fem. 2018, 26, e45995. [Google Scholar] [CrossRef]
- Holmes, S.E.; Hinz, R.; Conen, S.; Gregory, C.J.; Maflhews, J.C.; Anton-Rodriguez, J.M.; Gerhard, A. Elevated translocator protein in anterior cingulate in major depression and a role for inflammation in suicidal thinking: A positron emission tomography study. Biol. Psychiatry 2018, 83, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office on Drugs and Crime (UNODC). Relatório Mundial Sobre Drogas 2019: 35 Milhões de Pessoas em Todo o Mundo Sofrem de Transtornos Por Uso de Drogas, Enquanto Apenas 1 em Cada 7 Pessoas Recebe Tratamento. Available online: https://www.unodc.org/lpo-brazil/pt/frontpage/2019/06/relatrio-mundial-sobre-drogas-2019_-35-milhes-de-pessoas-em-todo-o-mundo-sofrem-de-transtornos-por-uso-de-drogas--enquanto-apenas-1-em-cada-7-pessoas-recebe-tratamento.html (accessed on 19 April 2025).
- Nascimento, V.F.; Ferreira, K.A.; Haflori, T.Y.; Terças-Treflel, A.C.P.; Lemes, A.G.; Luis, M.A.V. Relações de pessoas em situação de rua com uso de substâncias psicoativas. Rev. Soc. Hum. 2022, 35, e43479. [Google Scholar] [CrossRef]
- Alberti, A.; Coelho, D.R.A.; Vieira, W.F.; Iser, B.M.; Lampert, R.M.F.; Traebert, E.; Silva BBd Oliveira BHd Leão, G.M.; Souza Gd Dallacosta, F.M.; Kades, G.; Madeira, K.; et al. Factors associated with the development of depression and the influence of obesity on depressive disorders: A narrative review. Biomedicines 2024, 12, 1994. [Google Scholar] [CrossRef]
- Richardson, A.; Baune, B.T. Neuroinflammation and neuroprogression in depression: Effects of alternative drug treatments. Brain Behav. Immun. Health 2022, 23, 100554. [Google Scholar] [CrossRef]
- Machado da Silva, M.; Koek, W.; Taffe, M.A.; Moeller, F.G. Role of Microglia in Psychostimulant Addiction. Curr. Neuropharmacol. 2023, 21, 585–596. [Google Scholar]
- Lynch, F.L.; Peterson, E.L.; Lu, C.Y.; Hu, Y.; Rossom, R.C.; Waitzfelder, B.E.; Owen-Smith, A.A.; Hubley, S.; Prabhakar, D.; Williams, L.K.; et al. Substance Use Disorders and Risk of Suicide in a General US Population: A Case Control Study. Addict. Sci. Clin. Pract. 2020, 15, 14. [Google Scholar] [CrossRef]
- Athey, A.; Shaff, J.; Kahn, G.; Brodie, K.; Ryan, T.C.; Sawyer, H.; DeVinney, A.; Nestadt, P.S.; Wilcox, H.C. Association of substance use with suicide mortality: An updated systematic review and meta-analysis. Drug Alcohol Depend. Rep. 2025, 14, 100310. [Google Scholar] [CrossRef]
- Richer, I.; Bertrand, K.; Vandermeerschen, J.; Roy, É. A prospective cohort study of non-fatal accidental overdose among street youth: The link with suicidal ideation. Drug Alcohol Rev. 2012, 32, 398–404. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim Epidemiológico—Suicídio: Saber, Agir e Prevenir; Ministério da Saúde: Brasília, Brazil, 2017; Volume 48, No. 30.
- Felger, J.C.; Lotrich, F.E. Inflammatory cytokines in depression: Neurobiological mechanisms and therapeutic implications. Neuroscience 2013, 246, 199–229. [Google Scholar] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Joanna Briggs Institute (JBI). Scoping Reviews Resources. Available online: https://jbi.global/scoping-review-network/resources (accessed on 19 April 2025).
- Arnautovska, U.; Sveticic, J.; De Leo, D. What differentiates homeless persons who died by suicide from other suicides in Australia? A comparative analysis using a unique mortality register. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 49, 583–589. [Google Scholar] [CrossRef]
- Nilsson, S.F.; Hjorthoj, C.R.; Erlangsen, A.; Nordentoft, M. Suicide and unintentional injury mortality among homeless people: A Danish nationwide register-based cohort study. Eur. J. Public Health 2013, 24, 50–56. [Google Scholar] [CrossRef]
- Oppong Asante, K.; Meyer-Weid, A. Prevalence and predictors of suicidal ideations and attempts among homeless children and adolescents in Ghana. J. Child Adolesc. Ment. Health 2017, 29, 27–37. [Google Scholar] [CrossRef]
- Auerswald, C.L.; Lin, J.S.; Parriofl, A. Six-year mortality in a street-recruited cohort of homeless youth in San Francisco, California. PeerJ 2016, 4, e1909. [Google Scholar] [CrossRef] [PubMed]
- Moskowid, A.; Stein, J.A.; Lightfoot, M. The mediating roles of stress and maladaptive behaviors on self-harm and suicide attempts among runaway and homeless youth. J. Youth Adolesc. 2012, 42, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Rhoades, H.; Winetrobe, H.; Rice, E. Prescription drug misuse among homeless youth. Drug Alcohol Depend. 2014, 138, 229–233. [Google Scholar] [CrossRef]
- Roy, É. Mortality in a cohort of street youth in Montreal. JAMA 2004, 292, 569. [Google Scholar] [CrossRef]
- Sibthorpe, B.; Drinkwater, J.; Gardner, K.; Bammer, G. Drug use, binge drinking and attempted suicide among homeless and potentially homeless youth. Aust. N. Z. J. Psychiatry 1995, 29, 248–256. [Google Scholar] [CrossRef]
- Barak, Y.; Cohen, A.; Aizenberg, D. Suicide among the homeless. Crisis 2004, 25, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Jun, J.S.; Kim, Y.J.; Roh, S.; Moon, S.S.; Bukonda, N.; Hines, L. Mental health, substance abuse, and suicide among homeless adults. J. Evid.-Inf. Soc. Work 2017, 14, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, R.; Padilha, É.; Dias, C.G.; Bofli, L. Vulnerabilidades da população em situação de rua ao comportamento suicida. Rev. Enferm. UFPE Online 2019, 13, 431–437. [Google Scholar] [CrossRef]
- Sinyor, M.; Kozloff, N.; Reis, C.; Schaffer, A. An observational study of suicide death in homeless and precariously housed people in Toronto. Can. J. Psychiatry 2017, 62, 501–505. [Google Scholar] [CrossRef]
- Bonner, A.; Luscombe, C. Suicide and homelessness. J. Public Ment. Health 2009, 8, 7–19. [Google Scholar] [CrossRef]
- Devin, J.; Lyons, S.; Murphy, L.; O’Sullivan, M.; Lynn, E. Factors associated with suicide in people who use drugs: A scoping review. BMC Psychiatry 2023, 23, 51. [Google Scholar] [CrossRef]
- Died, T.L. Substance misuse, suicidal ideation, and suicide attempts among a national sample of homeless. J. Soc. Serv. Res. 2010, 37, 1–18. [Google Scholar] [CrossRef]
- Henkind, R.; Carmichael, H.; Stearns, D.R.; Thomas, M.; Abbifl, D.; Myers, Q.W.O.; Velopulos, C.G. Suicide among persons experiencing homelessness. J. Surg. Res. 2023, 284, 213–220. [Google Scholar] [CrossRef]
- Hodes, G.E.; Kana, V.; Menard, C.; Merad, M.; Russo, S.J. Neuroimmune mechanisms of depression. Nat. Neurosci. 2016, 19, 418–428. [Google Scholar] [CrossRef]
- Calcia, M.A.; Bonsall, D.R.; Bloomfield, P.S.; Selvaraj, S.; Pariante, C.M.; Howes, O.D. Stress and neuroinflammation: A systematic review of the effects of stress on microglial activation and its implications for mental illness. Psychopharmacology 2016, 233, 1637–1650. [Google Scholar] [CrossRef]
- Schwarz, J.M.; Bilbo, S.D. Adolescent morphine exposure affects long-term microglial function and later-life relapse liability in a model of addiction. J. Neurosci. 2013, 33, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ho, R.C.; Mak, A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-α) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: A meta-analysis and meta-regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef]
- Capuron, L.; Miller, A.H. Immune system to brain signaling: Neuropsychopharmacological implications. Pharmacol. Ther. 2011, 130, 226–238. [Google Scholar] [CrossRef] [PubMed]
- National Alliance to End Homelessness. National Alliance to End Homelessness; National Alliance to End Homelessness: Washington, DC, USA, 2022. [Google Scholar]
- Ministério dos Direitos Humanos e da Cidadania (MDHC). Relatório Sobre População em Situação de Rua. 2023. Available online: https://www.gov.br/mdh/pt-br/navegue-por-temas/populacao-em-situacao-de-rua/publicacoes/relat_pop_rua_digital.pdf (accessed on 29 May 2025).
- Instituto de Pesquisa Econômica Aplicada (IPEA). Estimativa da População em Situação de Rua no Brasil. 2023. Available online: https://repositorio.ipea.gov.br/bitstream/11058/12642/13/TD_2944_web.pdf (accessed on 29 May 2025).
- Mendes, K.T.; Ronzani, T.M.; Paiva, F.S. População em situação de rua, vulnerabilidades e drogas: Uma revisão sistemática. Psicol. Soc. 2019, 31, e169056. [Google Scholar] [CrossRef]
- Oliveira, G.B.; Higa, D.M.; Araujo, J.C.S.; Selusnhaki, A.M.; Reis, T.C.M.; Azevêdo, A.V.S. Pessoas em situação de rua: Revisão sistemática. Estud. Interdisc. Psicol. 2020, 11, 40–58. [Google Scholar] [CrossRef]
- National Health Care for the Homeless Council. Suicide and Homelessness: Data Trends in Suicide and Mental Health Among Homeless Populations. May 2018. Available online: https://www.nhchc.org/wp-content/uploads/2018/05/suicide-fact-sheet.pdf (accessed on 29 May 2025).
- Arensman, E.; Mhuircheartaigh, N.; Corcoran, P. Briefing: Self-Harm and Suicide Among Homeless People. National Suicide Research Foundation, 2014. Available online: https://www.nsrf.ie/wp-content/uploads/2021/06/Briefing-Self-Harm-and-Suicide-among-Homeless-People-02-11-2014.pdf (accessed on 29 May 2025).
- Hartmann, M.C.P.; Santos, D.L.; Claro, H.G.; Pires, D.E.P.; Silva, A.T.M.; Pereira, M.O. Suicidal Ideation and Attempts Among Street Youth in Brazil: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 6676. [Google Scholar]


{kind=link}
{kind=link}
| Focus of the Article | Year/Month of Publication | Journal | Country (City) | Author(s) |
|---|---|---|---|---|
| 155 youth aged 12–17; 54% reported physical abuse, 28% sexual abuse, and 73% a family history of PAS use; 24% were hospitalized due to PAS use and 45% attempted suicide; higher rates in females. | 1995 | Aust. N. Z. J. Psychiatry | Australia | Sibthorpe B. et al. |
| 1192 individuals; 156 deaths over 9 years; 9 suicides (all men, avg age 34); most had secondary education; 1 had PAS use history; 4 had psychiatric comorbidities; 6 used hanging. | 2004 | Crisis | Israel | Barak Yoram et al. |
| 26 deaths among youth with SUD: 13 suicides, 8 overdoses, 2 injuries, 1 hepatitis, and 1 heart disease; homelessness and current PAS use associated with deaths. | 2004 | JAMA | Canada (Montreal) | Roy Elise et al. |
| 428 youth with SUD; family dysfunction and history of suicide in the family indirectly affect suicidal ideation among homeless youth. | 2009 | Journal of Adolescence | USA | Jorgensen Edan L. et al. |
| Descriptive study, discussed vulnerabilities related to homelessness and suicide among individuals with SUD. | 2009 | J. Public Ment. Health | UK | Bonner A., Luscombe C. |
| LGBT and female youth more likely to engage in self-harm and suicide attempts; predictors included emotional distress, stress, parental PAS use, and bullying. | 2010 | Journal of Youth and Adolescence | USA | Moskowid Amanda et al. |
| Accidental overdoses significantly associated with suicidal ideation; contributing factors: homelessness, injection PAS use, and polysubstance use. | 2013 | Drug and Alcohol Review | Australia | Richer Isabelle et al. |
| 92 homeless individuals (82 men and 10 women); suicide rate nearly twice that of non-homeless; majority were young, unemployed men with PAS use and untreated mental illness. | 2014 | Social Psychiatry and Psychiatric Epidemiology | Australia (Queensland) | Arnautovska U. et al. |
| 32,010 individuals aged 16 or older (70.5% male) with SUD; suicide rate of 174.4/100,000 and unintentional injury rate of 463.3/100,000. Higher suicide risk among individuals with schizophrenia spectrum and SUD. | 2013 | European Journal of Public Health | Denmark | Nilsson Feodor Sandra et al. |
| 451 youth with SUD (opioids, sedatives, and stimulants); access via prescriptions from family and friends; misuse associated with hard drug use, unprotected sex, and suicidal tendencies. | 2015 | Drug Alcohol Dependence | USA | Rhoades Harmony et al. |
| 218 youths in San Francisco; mortality rate of 9.6/100,000 person-years; rate 10× higher than general youth; main causes: suicide and PAS use. | 2016 | PeerJ | USA (San Francisco) | Auerswald L. Collete et al. |
| 156 homeless adults; anxiety was associated with higher rates of suicidal ideation and attempts. Individuals with SUD showed increased suicidal behavior. The study suggested addressing mental health and SUD through support services. | 2017 | Journal of Evidence-Informed Social Work | USA | Lee Hag Kyoung et al. |
| 227 children and adolescents (122 men, 105 women); suicidal ideation and attempts associated with smoking, past/current alcohol and marijuana use, and involvement in prostitution. Highlights the urgency of training professionals to assess suicide risk and provide care pathways for this vulnerable group. | 2017 | J Criança Adolesc Ment Health | Ghana | Asante Kwaku Oppong, Weid-Anna Meyer |
| Among homeless individuals, higher rates of suicide observed in young, Black, male, non-veterans; more likely to have SUD and a history of suicidal thoughts or attempts; most died in public spaces. | 2023 | Journal of Surgical Research | USA | Henkind Rebecca et al. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Campos, D.A.; Alberti, A.; Seganfredo Camargo, C.E.; Mayer, A.B.; de Oliveira Junior, J.B.; Almeida Schonmeier, N.L.; Lampert, R.; Kades, G.; da Silva, B.B.; Leão, G.M.; et al. Suicide, Psychoactive Substances, and Homelessness: A Scoping Review. Brain Sci. 2025, 15, 602. https://doi.org/10.3390/brainsci15060602
de Campos DA, Alberti A, Seganfredo Camargo CE, Mayer AB, de Oliveira Junior JB, Almeida Schonmeier NL, Lampert R, Kades G, da Silva BB, Leão GM, et al. Suicide, Psychoactive Substances, and Homelessness: A Scoping Review. Brain Sciences. 2025; 15(6):602. https://doi.org/10.3390/brainsci15060602
Chicago/Turabian Stylede Campos, Dalvan Antonio, Adriano Alberti, Carlos Eduardo Seganfredo Camargo, Andréia Biolchi Mayer, João Batista de Oliveira Junior, Nayara Lisboa Almeida Schonmeier, Rose Lampert, Gabriela Kades, Bruna Becker da Silva, Graziela Marques Leão, and et al. 2025. "Suicide, Psychoactive Substances, and Homelessness: A Scoping Review" Brain Sciences 15, no. 6: 602. https://doi.org/10.3390/brainsci15060602
APA Stylede Campos, D. A., Alberti, A., Seganfredo Camargo, C. E., Mayer, A. B., de Oliveira Junior, J. B., Almeida Schonmeier, N. L., Lampert, R., Kades, G., da Silva, B. B., Leão, G. M., Crivilim, D. A. P., Hur Soares, B., de Jesus, J. A., Zavorski, E. B., Souza, R., de Carvalho, R. P. D., Vieira, A. P. A., Kanan, L. A., & da Cunha, N. V. (2025). Suicide, Psychoactive Substances, and Homelessness: A Scoping Review. Brain Sciences, 15(6), 602. https://doi.org/10.3390/brainsci15060602