
Cognitive Control After ACL Reconstruction: A Cross-Sectional Study on Impaired Proactive Inhibition Compared to Healthy Controls

 , , and
, , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Participants
2.3. Procedure
2.3.1. Familiarisation Session
2.3.2. Experimental Session
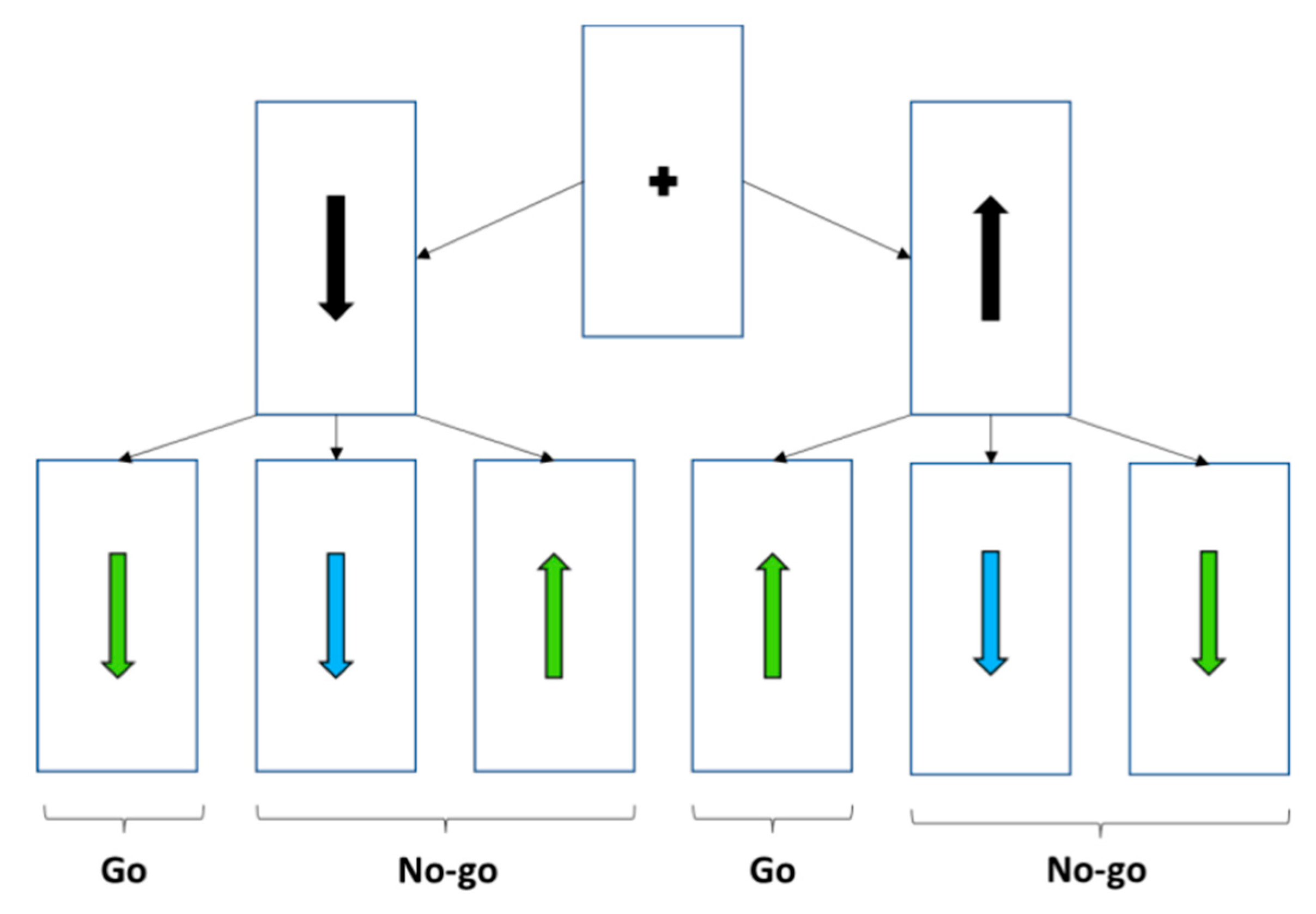
2.3.3. Cognitive Task
2.3.4. Statistical Analysis
3. Results
3.1. Verification of the Attribution of Go Stimulus Appearance Percentages to Each Condition of the Cognitive Task
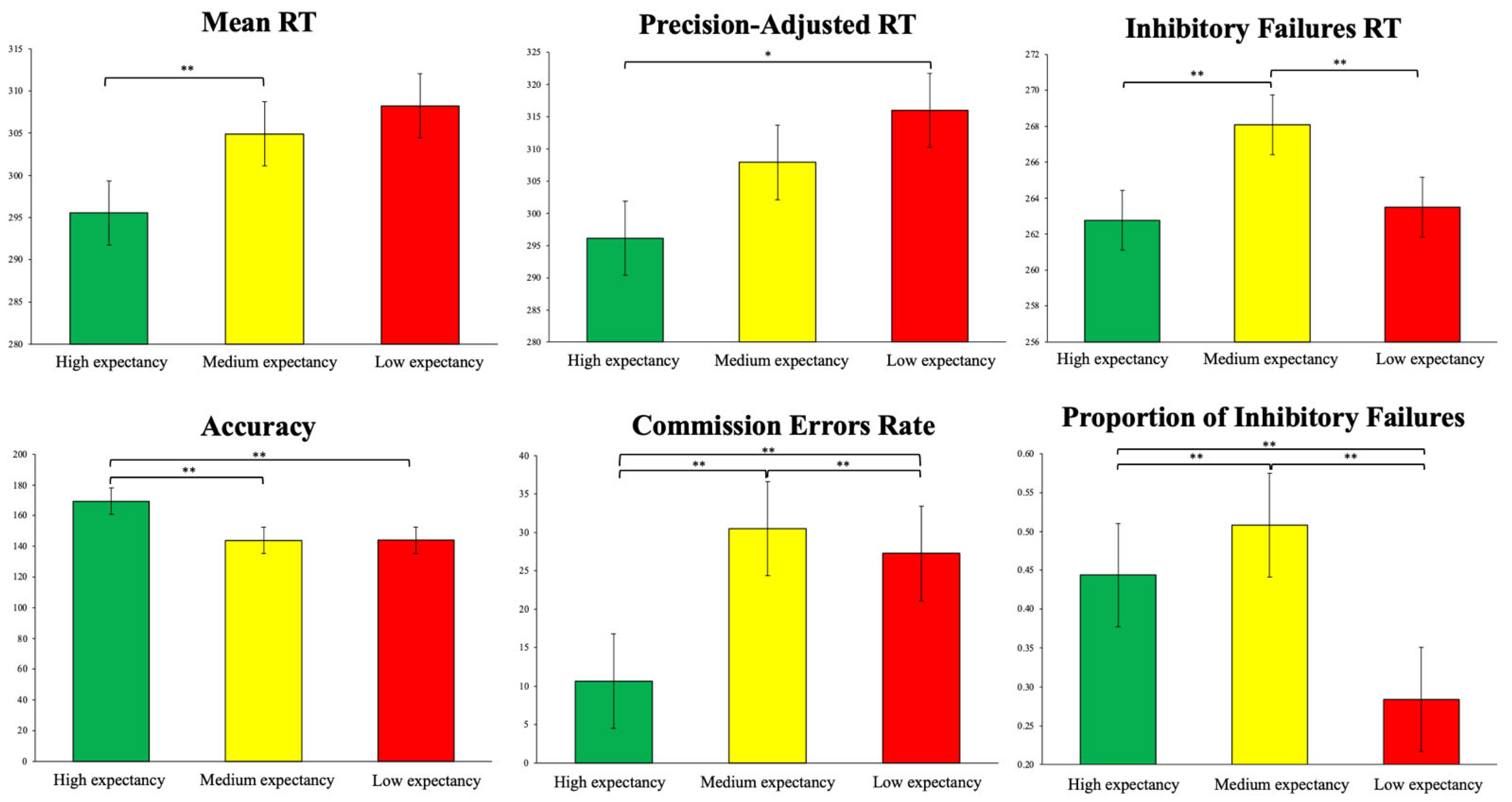
3.2. Cognitive Performance Differences Between Experimental Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poulsen, E.; Goncalves, G.H.; Bricca, A.; Roos, E.M.; Thorlund, J.B.; Juhl, C.B. Knee osteoarthritis risk is increased 4-6 fold after knee injury–a systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 1454–1463. [Google Scholar] [CrossRef] [PubMed]
- Ross, B.J.; Savage-Elliott, I.; Brown, S.M.; Mulcahey, M.K. Return to play and performance after primary ACL reconstruction in American football players: A systematic review. Orthop. J. Sports Med. 2020, 8, 2325967120959654. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W. Assessing the return on investment of injury prevention procedures in professional football. Sports Med. 2019, 49, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Marmura, H.; Bryant, D.M.; Getgood, A.M. Infographic. Sex differences and ACL injuries. Br. J. Sports Med. 2021, 55, 1313–1314. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Roewer, B.D.; Ford, K.R. Letter to the editor regarding “Effect of low pass filtering on joint moments from inverse dynamics: Implications for injury prevention”. J. Biomech. 2012, 45, 2058. [Google Scholar] [CrossRef]
- Piskin, D.; Benjaminse, A.; Dimitrakis, P.; Gokeler, A. Neurocognitive and neurophysiological functions related to ACL injury: A framework for neurocognitive approaches in rehabilitation and return-to-sports tests. Sports Health 2022, 14, 549–555. [Google Scholar] [CrossRef]
- Ashford, M.; Abraham, A.; Poolton, J. Understanding a player’s decision-making process in team sports: A systematic review of empirical evidence. Sports 2021, 9, 65. [Google Scholar] [CrossRef]
- Boden, B.P.; Sheehan, F.T. Mechanism of non-contact ACL injury: OREF Clinical Research Award 2021. J. Orthop. Res. 2022, 40, 531–540. [Google Scholar] [CrossRef]
- Jiménez-Martínez, J.; Gutiérrez-Capote, A.; Alarcón-López, F.; Leicht, A.; Cárdenas-Vélez, D. Relationship between cognitive demands and biomechanical indicators associated with anterior cruciate ligament injury: A systematic review. Sports Med. 2025, 55, 145–165. [Google Scholar] [CrossRef]
- Deodato, M.; Qualizza, C.; Martini, M.; Mazzari, L.; Furlanis, G.; Buoite Stella, A.; Manganotti, P. Efficacy of dual-task augmented reality rehabilitation in non-hospitalized adults with self-reported long COVID fatigue and cognitive impairment: A pilot study. Neurol. Sci. 2024, 45, 1325–1333. [Google Scholar] [CrossRef]
- Abdallat, R.; Sharouf, F.; Button, K.; Al-Amri, M. Dual-task effects on performance of gait and balance in people with knee pain: A systematic scoping review. J. Clin. Med. 2020, 9, 1554. [Google Scholar] [CrossRef] [PubMed]
- Leng, X.; Yee, D.; Ritz, H.; Shenhav, A. Dissociable influences of reward and punishment on adaptive cognitive control. PLoS Comput. Biol. 2021, 17, e1009737. [Google Scholar] [CrossRef] [PubMed]
- Gratton, G.; Cooper, P.; Fabiani, M.; Carter, C.S.; Karayanidis, F. Dynamics of cognitive control: Theoretical bases, paradigms, and a view for the future. Psychophysiology 2018, 55, e13016. [Google Scholar] [CrossRef]
- Best, J.R.; Miller, P.H. A developmental perspective on executive function. Child Dev. 2010, 81, 1641–1660. [Google Scholar] [CrossRef]
- Klenberg, L.; Korkman, M.; Lahti-Nuuttila, P. Differential development of attention and executive functions in 3-to 12-year-old Finnish children. Dev. Neuropsychol. 2001, 20, 407–428. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Friedman, N.P.; Miyake, A. The relations among inhibition and interference control functions: A latent-variable analysis. J. Exp. Psychol. Gen. 2004, 133, 101. [Google Scholar] [CrossRef]
- Xie, L.; Ren, M.; Cao, B.; Li, F. Distinct brain responses to different inhibitions: Evidence from a modified Flanker Task. Sci. Rep. 2017, 7, 6657. [Google Scholar] [CrossRef]
- Zhang, D.; Ding, H.; Wang, X.; Qi, C.; Luo, Y. Enhanced response inhibition in experienced fencers. Sci. Rep. 2015, 5, 16282. [Google Scholar] [CrossRef]
- Jacobson, J.; Matthaeus, L. Athletics and executive functioning: How athletic participation and sport type correlate with cognitive performance. Psychol. Sport Exerc. 2014, 15, 521–527. [Google Scholar] [CrossRef]
- Nuri, L.; Shadmehr, A.; Ghotbi, N.; Attarbashi Moghadam, B. Reaction time and anticipatory skill of athletes in open and closed skill-dominated sport. Eur. J. Sport Sci. 2013, 13, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Radvansky, G.A.; Zacks, J.M. Event boundaries in memory and cognition. Curr. Opin. Behav. Sci. 2017, 17, 133–140. [Google Scholar] [CrossRef]
- Carson, H.J.; Collins, D. Implementing the Five-A Model of technical refinement: Key roles of the sport psychologist. J. Appl. Sport Psychol. 2016, 28, 392–409. [Google Scholar] [CrossRef] [PubMed]
- Sperl, L.; Gergeleit, T.; Cañal-Bruland, R. On the role of different subdimensions of inhibition for successful motor skill change. Hum. Mov. Sci. 2021, 77, 102801. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Groneberg, D.A. Neurocognitive function and musculoskeletal injury risk in sports: A systematic review. J. Sci. Med. Sport 2022, 25, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Giesche, F.; Wilke, J.; Engeroff, T.; Niederer, D.; Hohmann, H.; Vogt, L.; Banzer, W. Are biomechanical stability deficits during unplanned single-leg landings related to specific markers of cognitive function? J. Sci. Med. Sport 2020, 23, 82–88. [Google Scholar] [CrossRef]
- Bertozzi, F.; Fischer, P.D.; Hutchison, K.A.; Zago, M.; Sforza, C.; Monfort, S.M. Associations between cognitive function and ACL injury-related biomechanics: A systematic review. Sports Health 2023, 15, 855–866. [Google Scholar] [CrossRef]
- Gokeler, A.; McKeon, P.O.; Hoch, M.C. Shaping the functional task environment in sports injury rehabilitation: A framework to integrate perceptual-cognitive training in rehabilitation. Athl. Train. Sports Health Care 2020, 12, 283–292. [Google Scholar] [CrossRef]
- Grooms, D.R.; Onate, J.A. Neuroscience application to noncontact anterior cruciate ligament injury prevention. Sports Health 2016, 8, 149–152. [Google Scholar] [CrossRef]
- Abreu, A.M.; Macaluso, E.; Azevedo, R.T.; Cesari, P.; Urgesi, C.; Aglioti, S.M. Action anticipation beyond the action observation network: A functional magnetic resonance imaging study in expert basketball players. Eur. J. Neurosci. 2012, 35, 1646–1654. [Google Scholar] [CrossRef]
- Yu, Q.; Chau, B.K.; Lam, B.Y.; Wong, A.W.; Peng, J.; Chan, C.C. Neural processes of proactive and reactive controls modulated by motor-skill experiences. Front. Hum. Neurosci. 2019, 13, 404. [Google Scholar] [CrossRef] [PubMed]
- Braver, T.S. The variable nature of cognitive control: A dual mechanisms framework. Trends Cogn. Sci. 2012, 16, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Bravi, R.; Gavazzi, G.; Benedetti, V.; Giovannelli, F.; Grasso, S.; Panconi, G.; Viggiano, M.P.; Minciacchi, D. Effect of different sport environments on proactive and reactive motor inhibition: A study on open-and closed-skilled athletes via mouse-tracking procedure. Front. Psychol. 2022, 13, 1042705. [Google Scholar] [CrossRef]
- van den Wildenberg, W.P.; Ridderinkhof, K.R.; Wylie, S.A. Towards conceptual clarification of proactive inhibitory control: A review. Brain Sci. 2022, 12, 1638. [Google Scholar] [CrossRef]
- Wang, C.-H.; Chang, C.-C.; Liang, Y.-M.; Shih, C.-M.; Chiu, W.-S.; Tseng, P.; Hung, D.L.; Tzeng, O.J.; Muggleton, N.G.; Juan, C.-H. Open vs. closed skill sports and the modulation of inhibitory control. PLoS ONE 2013, 8, e55773. [Google Scholar] [CrossRef] [PubMed]
- Brevers, D.; Dubuisson, E.; Dejonghe, F.; Dutrieux, J.; Petieau, M.; Cheron, G.; Verbanck, P.; Foucart, J. Proactive and reactive motor inhibition in top athletes versus nonathletes. Percept. Mot. Ski. 2018, 125, 289–312. [Google Scholar] [CrossRef]
- Moran, R.N.; Grooms, D.R. Individual and Combined Effects of Sport-Related Concussion and Anterior Cruciate Ligament Injury on Neurocognitive and Neuromechanical Reaction Time. J. Athl. Train. 2025, 60, 3–10. [Google Scholar] [CrossRef]
- Emami, F.; Negahban, H.; Sinaei, E.; Mostafaee, N.; Shahtahmassebi, B.; Ebrahimzadeh, M.H.; Mehravar, M. The Effects of Various Cognitive Tasks Including Working Memory, Visuospatial, and Executive Function on Postural Control in Patients With Anterior Cruciate Ligament Injury. Mot. Control 2024, 28, 193–209. [Google Scholar] [CrossRef]
- Balser, N.; Lorey, B.; Pilgramm, S.; Stark, R.; Bischoff, M.; Zentgraf, K.; Williams, A.M.; Munzert, J. Prediction of human actions: Expertise and task-related effects on neural activation of the action observation network. Hum. Brain Mapp. 2014, 35, 4016–4034. [Google Scholar] [CrossRef]
- Piras, A.; Lobietti, R.; Squatrito, S. Response time, visual search strategy, and anticipatory skills in volleyball players. J. Ophthalmol. 2014, 2014, 189268. [Google Scholar] [CrossRef]
- Gutiérrez-Capote, A.; Jiménez-Martínez, J.; Madinabeitia, I.; de Orbe-Moreno, M.; Pesce, C.; Cardenas, D. Sport as cognition enhancer from childhood to young adulthood: A systematic review focused on sport modality. Int. J. Sport Exerc. Psychol. 2024, 22, 395–427. [Google Scholar] [CrossRef]
- Costello, S.E.; O’Neill, B.V.; Howatson, G.; van Someren, K.; Haskell-Ramsay, C.F. Detrimental effects on executive function and mood following consecutive days of repeated high-intensity sprint interval exercise in trained male sports players. J. Sports Sci. 2022, 40, 783–796. [Google Scholar] [CrossRef] [PubMed]
- Cesari, V.; Marinari, E.; Laurino, M.; Gemignani, A.; Menicucci, D. Attention-dependent physiological correlates in sleep-deprived young healthy humans. Behav. Sci. 2021, 11, 22. [Google Scholar] [CrossRef]
- Gutiérrez-Capote, A.; Madinabeitia, I.; Alarcón, F.; Torre, E.; Jiménez-Martínez, J.; Cárdenas, D. Acute effect of complexity in basketball on cognitive capacity. Front. Psychol. 2024, 15, 1376961. [Google Scholar] [CrossRef] [PubMed]
- Papadelis, C.; Kourtidou-Papadeli, C.; Vlachogiannis, E.; Skepastianos, P.; Bamidis, P.; Maglaveras, N.; Pappas, K. Effects of mental workload and caffeine on catecholamines and blood pressure compared to performance variations. Brain Cogn. 2003, 51, 143–154. [Google Scholar] [CrossRef]
- Vocat, R.; Pourtois, G.; Vuilleumier, P. Unavoidable errors: A spatio-temporal analysis of time-course and neural sources of evoked potentials associated with error processing in a speeded task. Neuropsychologia 2008, 46, 2545–2555. [Google Scholar] [CrossRef] [PubMed]
- Matsui, N.; Bamba, E. Evaluative cognition and attention allocation in human interface. Syst. Comput. Jpn. 1988, 19, 79–86. [Google Scholar] [CrossRef]
- Gavazzi, G.; Rossi, A.; Orsolini, S.; Diciotti, S.; Giovannelli, F.; Salvadori, E.; Pantoni, L.; Mascalchi, M.; Viggiano, M.P. Impulsivity trait and proactive cognitive control: An fMRI study. Eur. J. Neurosci. 2019, 49, 1171–1179. [Google Scholar] [CrossRef]
- Giovannelli, F.; Mastrolorenzo, B.; Rossi, A.; Gavazzi, G.; Righi, S.; Zaccara, G.; Viggiano, M.; Cincotta, M. Relationship between impulsivity traits and awareness of motor intention. Eur. J. Neurosci. 2016, 44, 2455–2459. [Google Scholar] [CrossRef]
- Verbruggen, F.; Logan, G.D. Proactive adjustments of response strategies in the stop-signal paradigm. J. Exp. Psychol. Hum. Percept. Perform. 2009, 35, 835. [Google Scholar] [CrossRef]
- Swanik, C.B.; Covassin, T.; Stearne, D.J.; Schatz, P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am. J. Sports Med. 2007, 35, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Smeets, A.; Verschueren, S.; Staes, F.; Claes, S.; Vandenneucker, H.; Vanrenterghem, J. 198 Challenging ACL reconstructed athletes and their sensorimotor system at return-to-sport: A vital step towards exposing the roots of their neuromuscular deficits. Br. J. Sports Med. 2021, 55 (Suppl. 1), A77.3–A78. [Google Scholar]
- Lucci, G.; Berchicci, M.; Perri, R.; Spinelli, D.; Di Russo, F. Effect of target probability on pre-stimulus brain activity. Neuroscience 2016, 322, 121–128. [Google Scholar] [CrossRef]
- Waskom, M.L.; Frank, M.C.; Wagner, A.D. Adaptive engagement of cognitive control in context-dependent decision making. Cereb. Cortex 2017, 27, 1270–1284. [Google Scholar] [CrossRef]
- Herman, D.C.; Barth, J.T. Drop-jump landing varies with baseline neurocognition: Implications for anterior cruciate ligament injury risk and prevention. Am. J. Sports Med. 2016, 44, 2347–2353. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.L.; Quintana, C.; Hoch, M. The relationship between neurocognitive function and biomechanics: A critically appraised topic. J. Sport Rehabil. 2020, 30, 327–332. [Google Scholar] [CrossRef]
- Cooper, P.S.; Garrett, P.M.; Rennie, J.L.; Karayanidis, F. Task uncertainty can account for mixing and switch costs in task-switching. PLoS ONE 2015, 10, e0131556. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.J.; Anderson, M.C. Inhibitory processes and the control of memory retrieval. Trends Cogn. Sci. 2002, 6, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Sperl, L.; Cañal-Bruland, R. Interindividual differences in the capability to change automatized movement patterns. Acta Psychol. 2020, 204, 103027. [Google Scholar] [CrossRef]
- Diekfuss, J.A.; Grooms, D.R.; Yuan, W.; Dudley, J.; Foss, K.D.B.; Thomas, S.; Ellis, J.D.; Schneider, D.K.; Leach, J.; Bonnette, S. Does brain functional connectivity contribute to musculoskeletal injury? A preliminary prospective analysis of a neural biomarker of ACL injury risk. J. Sci. Med. Sport 2019, 22, 169–174. [Google Scholar] [CrossRef]
- Swanik, C.B. Brains and sprains: The brain’s role in noncontact anterior cruciate ligament injuries. J. Athl. Train. 2015, 50, 1100–1102. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Athletes | ACLR Athletes | |
|---|---|---|
| N (Male/Female) | 20/10 | 22/8 |
| Years of practical experience | 9.26 ± 1.44 | 8.83 ± 1.21 |
| Age (years) | 21.24 ± 5.87 | 22.36 ± 6.12 |
| Height (m) | 179.11 ± 15.32 | 80.66 ± 13.65 |
| Body mass (kg) | 175.93 ± 9.40 | 76.34 ± 9.65 |
| BMI (kg·m−2) | 20.23 ± 0.43 | 20.93 ± 0.34 |
| Healthy Athletes | ACLR Athletes | ||||
|---|---|---|---|---|---|
| M | SD | M | SD | p | |
| Overall task | |||||
| Mean RT | 284.73 | 31.20 | 325.22 | 57.31 | 0.002 |
| Precision-Adjusted RT | 288.27 | 29.69 | 328.28 | 56.02 | 0.011 |
| Inhibitory Failures RT | 238.81 | 30.31 | 297.24 | 54.9 | <0.001 |
| Accuracy | 471.43 | 41.22 | 439.46 | 31.15 | 0.003 |
| Commission Errors Rate | 58.28 | 32.11 | 80.44 | 25.85 | 0.026 |
| Proportion of Inhibitory Failures | 0.33 | 0.18 | 0.45 | 0.15 | 0.008 |
| High-expectancy condition | |||||
| Mean RT | 272.41 | 37.61 | 324.72 | 56.97 | <0.001 |
| Precision-Adjusted RT | 272.51 | 35.49 | 325.05 | 56.13 | <0.001 |
| Inhibitory Failures RT | 236.87 | 30.28 | 294.52 | 55.06 | <0.001 |
| Accuracy | 170.57 | 6.20 | 167.59 | 8.63 | 0.181 |
| Commission Errors Rate | 8.90 | 5.60 | 12.8 | 5.52 | 0.011 |
| Proportion of Inhibitory Failures | 0.37 | 0.23 | 0.55 | 0.23 | 0.011 |
| Medium-expectancy condition | |||||
| Mean RT | 287.67 | 31.59 | 326.50 | 59.13 | 0.002 |
| Precision-Adjusted RT | 290.73 | 28.42 | 328.77 | 57.00 | <0.001 |
| Inhibitory Failures RT | 242.03 | 30.34 | 300.04 | 55.36 | <0.001 |
| Accuracy | 151.50 | 17.81 | 132.82 | 14.84 | 0.068 |
| Commission Errors Rate | 24.76 | 14.18 | 37.12 | 13.55 | 0.002 |
| Proportion of Inhibitory Failures | 0.42 | 0.23 | 0.65 | 0.21 | 0.002 |
| Low-expectancy condition | |||||
| Mean RT | 295.18 | 27.87 | 325.06 | 59.49 | 0.002 |
| Precision-Adjusted RT | 301.60 | 27.89 | 333.10 | 56.81 | 0.018 |
| Inhibitory Failures RT | 237.54 | 30.31 | 295.35 | 55.22 | 0.014 |
| Accuracy | 149.37 | 17.80 | 136.09 | 10.15 | 0.010 |
| Commission Errors Rate | 24.72 | 12.76 | 30.2 | 8.49 | 0.074 |
| Proportion of Inhibitory Failures | 0.26 | 0.13 | 0.32 | 0.08 | 0.093 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Martínez, J.; Gutiérrez-Capote, A.; Madinabeitia, I.; Cárdenas, D.; Alarcón, F. Cognitive Control After ACL Reconstruction: A Cross-Sectional Study on Impaired Proactive Inhibition Compared to Healthy Controls. Brain Sci. 2025, 15, 497. https://doi.org/10.3390/brainsci15050497
Jiménez-Martínez J, Gutiérrez-Capote A, Madinabeitia I, Cárdenas D, Alarcón F. Cognitive Control After ACL Reconstruction: A Cross-Sectional Study on Impaired Proactive Inhibition Compared to Healthy Controls. Brain Sciences. 2025; 15(5):497. https://doi.org/10.3390/brainsci15050497
Chicago/Turabian StyleJiménez-Martínez, Jesús, Alejandro Gutiérrez-Capote, Iker Madinabeitia, David Cárdenas, and Francisco Alarcón. 2025. "Cognitive Control After ACL Reconstruction: A Cross-Sectional Study on Impaired Proactive Inhibition Compared to Healthy Controls" Brain Sciences 15, no. 5: 497. https://doi.org/10.3390/brainsci15050497
APA StyleJiménez-Martínez, J., Gutiérrez-Capote, A., Madinabeitia, I., Cárdenas, D., & Alarcón, F. (2025). Cognitive Control After ACL Reconstruction: A Cross-Sectional Study on Impaired Proactive Inhibition Compared to Healthy Controls. Brain Sciences, 15(5), 497. https://doi.org/10.3390/brainsci15050497