1. Introduction
Dementia is a global health challenge, affecting an estimated 57 million people worldwide [
1]. Among the numerous psychological comorbidities associated with dementia, generalized anxiety disorder is particularly prevalent, with studies reporting a prevalence of up to 38% in this population, especially among individuals with mild cognitive impairment [
2]. Anxiety in dementia patients not only exacerbates cognitive and functional decline but also significantly diminishes their quality of life, creating a pressing need for effective interventions [
3]. Traditionally, pharmacological approaches have been the cornerstone of anxiety management in this population. However, these treatments often come with limitations, including adverse side effects, potential acceleration of cognitive decline, and limited emotional benefits. Consequently, there is a growing interest in exploring non-pharmacological strategies that can complement or even replace traditional methods, offering safer and more holistic alternatives.
Among the emerging non-pharmacological interventions, immersive virtual reality (IVR) has gained attention as a promising tool for mental health applications [
4]. IVR enables users to engage with personalized virtual environments that simultaneously stimulate multiple senses, creating immersive experiences that can evoke relaxation, reduce stress, and promote positive emotional states. This technology offers a unique opportunity to address anxiety in individuals with mild dementia or early-stage Alzheimer′s disease, providing tailored experiences that minimize risks while maximizing emotional and psychological benefits. Moreover, IVR can be adapted to the specific needs and preferences of each patient, making it a highly individualized intervention.
Recently, a scoping review by Buele et al. [
5] emphasized the emotional and user experience outcomes of VR in neurodegenerative disorders, noting improvements in apathy, mood, and quality of life—particularly in immersive systems designed with user adaptability in mind. These results suggest that IVR not only engages users effectively but may also yield psychophysiological benefits relevant to anxiety management.
In parallel, recent studies have increasingly examined the emotional benefits of nature-based virtual environments for individuals with dementia. Kim et al. demonstrated that immersive exposure to natural scenery in virtual reality can help reduce physiological stress and promote emotional relaxation in this population, underscoring the value of naturalistic virtual stimuli in dementia care [
6,
7]. Furthermore, a pilot study by Soares et al. [
8] explored the use of 360° videos of personally meaningful locations during reminiscence therapy with individuals living with dementia. Although no statistically significant differences were found between the immersive and non-immersive conditions in terms of anxiety and depression reduction, the approach demonstrated feasibility and acceptability, supporting the continued exploration of personalized immersive content.
Building on previous findings, our study explores the use of IVR as a non-pharmacological intervention to reduce anxiety and improve psychological well-being in individuals with mild dementia. Specifically, we investigate the effects of exposure to relaxing virtual environments, such as nature-based scenarios (e.g., Nature Treks VR) and 360-degree videos of personally significant places or activities. To evaluate the impact of IVR, we employ a multimodal assessment approach, including physiological measures (e.g., heart rate), standardized psychological questionnaires (e.g., STAI-r for anxiety and I-PANAS-SF for psychological well-being), observational records during IVR sessions, and subjective feedback from participants. Our hypothesis is that IVR-based interventions will significantly reduce anxiety levels and enhance emotional well-being in this population.
By examining the potential of IVR as a therapeutic tool, this study aims to contribute to the growing body of evidence on non-pharmacological interventions for dementia-related anxiety. Furthermore, we seek to determine whether IVR can be integrated into routine care practices to improve the quality of life and emotional resilience of individuals living with dementia.
3. Results
A repeated measures ANOVA was conducted to examine changes in heart rate (HR) across five time points within each session and to assess whether this pattern differed between the Experimental and Control groups. Mauchly’s test confirmed sphericity, and Levene’s test indicated homogeneity of variances across measurement points. The analysis revealed a significant main effect of Time (F(4,56) = 5.567,
p = 0.002, η
2 = 0.03), indicating that HR changed over the course of the sessions. However, the Time × Group interaction was not significant (F(4,56) = 1.189,
p = 0.326, η
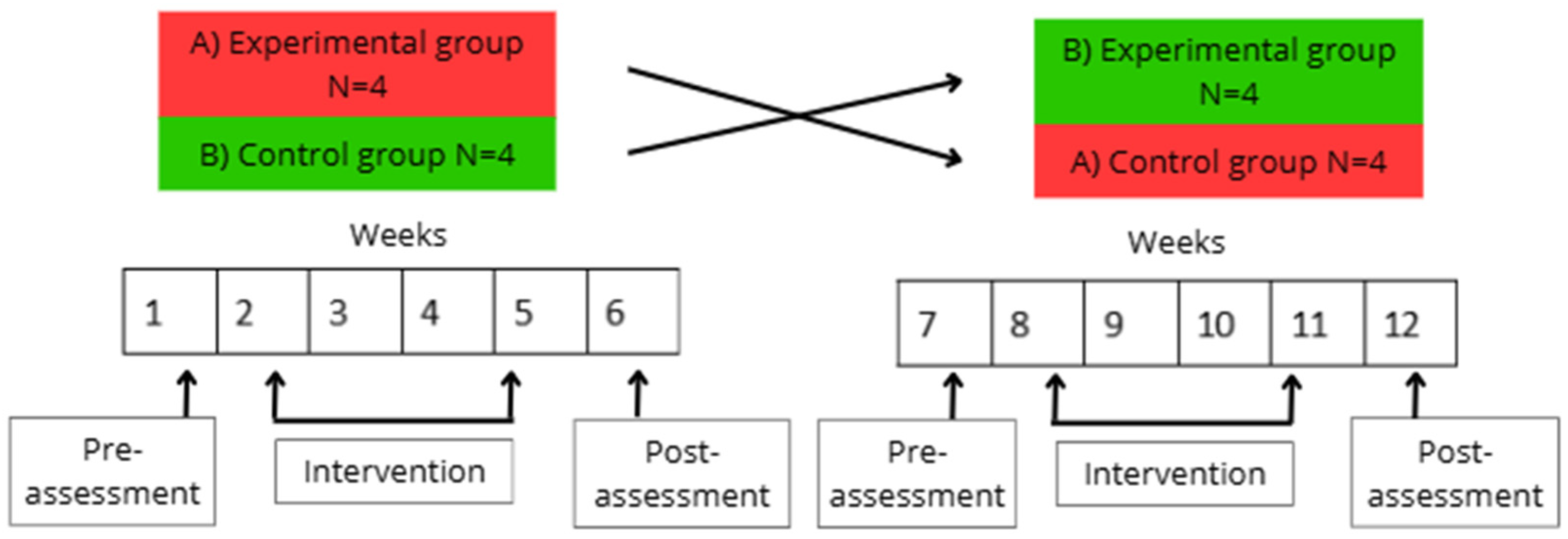
2 = 0.006), suggesting that overall HR trends did not differ significantly between conditions. Given the crossover design—where each participant experienced both conditions—it was methodologically appropriate to analyze each condition separately. This approach accounts for intra-individual variability and allows detection of condition-specific effects. In the Control group, HR remained stable throughout the session (F(4,28) = 1.252,
p = 0.312). In contrast, in the Experimental group, there was a significant effect of Time (F(4,28) = 7.117,
p < 0.001, η
2 = 0.504), prompting post hoc comparisons. Holm-adjusted pairwise tests showed that HR significantly decreased at 10 and 15 min compared to the baseline (PRE) (t = 4.507,
p = 0.001; t = 3.605,
p = 0.01, respectively), and was still significantly lower at 10 min compared to POST (t = 3.756,
p = 0.007). A marginal difference was also found between POST and 15 min (t = 2.854,
p = 0.056).
Figure 2 illustrates these HR trends across the five measurement points in both conditions.
We used a repeated measures ANOVA to evaluate the effects of Time (PRE vs. POST), Group (Experimental vs. Control), and their interaction on PANAS scores. Levene’s test confirmed homogeneity of variances at both PRE (p = 0.716) and POST (p = 0.387). Since only two time points were analyzed, sphericity testing was not applicable.
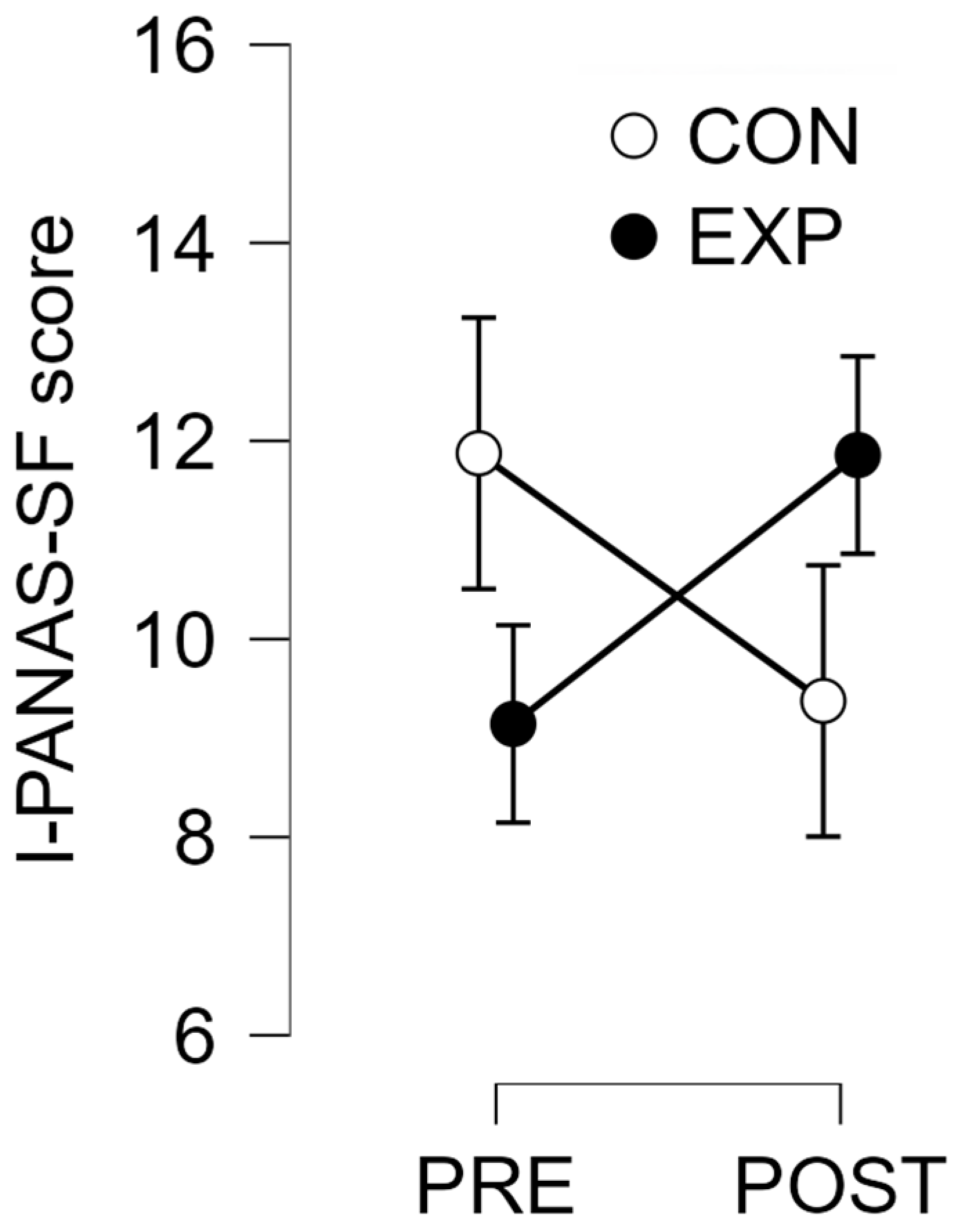
The analysis showed no significant main effect of Time (F(1,13) = 0.008, p = 0.932), indicating that overall PANAS scores did not change significantly from PRE to POST across both groups. There was also no significant main effect of Group (F(1,13) = 0.002, p = 0.961), meaning that PANAS scores were similar between the Experimental and Control groups. However, the interaction between Time and Group approached significance (F(1,13) = 4.497, p = 0.054, η2 = 0.062), suggesting a possible difference in how scores changed over time depending on the condition. When we analyzed each group separately, we found no significant change in the Control group (F(1,7) = 1.667, p = 0.238), and likewise, no significant change in the Experimental group (F(1,6) = 0.102, p = 0.102, η2 = 0.382). However, the effect size in the Experimental group indicates a moderate trend that may be meaningful with a larger sample.
To better understand the potential clinical relevance of the PANAS results, we calculated the minimal clinically important difference (MCID) using the 0.5 standard deviation method based on PRE-intervention PANAS scores. For the Experimental group, the MCID was 2.878, while the observed change from PRE to POST was +2.714—slightly below the threshold for clinical significance. In the Control group, the MCID was 2.528, and the observed change was −2.5, which also fell short of clinical significance.
Figure 3 shows a comparison of I-PANAS-SF scores at PRE and POST for both groups.
We also performed repeated measures ANOVAs on the state and trait subscales of the reduced State–Trait Anxiety Inventory (STAIr). For both dimensions, we found no significant main effect of Time (State: F(1,13) = 1.156, p = 0.302; Trait: F(1,13) = 1.384, p = 0.260), nor of Group (State: F(1,13) = 0.095, p = 0.762; Trait: F(1,13) = 0.245, p = 0.629). There were also no significant Time × Group interactions (State: F(1,13) = 1.156, p = 0.302; Trait: F(1,13) = 0.025, p = 0.876).
We analyzed behavioral responses by comparing the average scores recorded during the Nature Treks VR and YouTube video conditions across all sessions. The Shapiro–Wilk test confirmed that the data followed a normal distribution (W = 0.861,
p = 0.123). A paired-samples
t-test was conducted with the directional hypothesis that responses would be lower during the Nature Treks VR sessions. The analysis revealed a trend toward significance, with participants showing higher behavioral scores during the YouTube condition compared to Nature Treks VR (t(7) = 1.624,
p = 0.074).
Figure 4 illustrates the distribution of behavioral responses across both conditions.
Regarding the subjective response questionnaire, all participants consistently gave the maximum score of 4 points in every session, indicating uniformly positive emotional reactions to the Nature Treks VR intervention. They consistently reported feeling excited and calm, and none reported feelings of upset or anxiety. Additionally, all participants confirmed the perceived realism of the virtual scenarios in every session.
4. Discussion
The present study aimed to evaluate the physiological, emotional, behavioral, and subjective responses of individuals with dementia during exposure to immersive virtual reality (VR) environments compared to conventional digital activities. The results provide partial support for the hypothesis that immersive VR experiences elicit beneficial effects, particularly in terms of physiological relaxation and positive subjective evaluations, although changes in self-reported emotional states and anxiety did not reach statistical or clinical significance.
Regarding heart rate (HR), the analysis revealed a significant main effect of time, with more detailed analysis showing that the VR condition led to a progressive reduction in HR during the sessions. Specifically, HR significantly decreased at the 10 and 15 min points compared to baseline, suggesting a calming autonomic response associated with exposure to VR natural environments. This reduction in HR was not observed in the control condition, where heart rates remained stable throughout. These findings are in line with previous research demonstrating the relaxing effects of virtual nature exposure and its potential to reduce physiological arousal [
13]. The observed decrease in heart rate during immersive VR exposure may reflect an activation of parasympathetic processes indicative of autonomic relaxation—a response of particular relevance in older adults and individuals with dementia, given their vulnerability to stress-related physiological dysregulation. Autonomic nervous system (ANS) dysfunction is a well-documented feature of aging and dementia, contributing to impaired cardiovascular reactivity, diminished stress resilience, and reduced functional autonomy [
14]. In patients with dementia, studies have shown impaired heart rate responses, reflecting ANS deterioration [
15]. Against this backdrop, the physiological effects of immersive VR assume clinical relevance. The heart rate reductions observed in our study are consistent with prior research showing the capacity of VR interventions to modulate autonomic activity. For example, Mazgelytė et al. [
16] reported that a single session of VR-assisted respiratory biofeedback led to significant decreases in heart rate, respiratory rate, and skin conductance, alongside improvements in mood and reductions in cortisol levels, confirming a systemic autonomic calming response. Furthermore, Rault et al. [
17] observed anxiolytic effects following repeated sessions of VR relaxation in individuals with schizophrenia, highlighting the potential of IVR to serve as a transdiagnostic tool for stress regulation. In the context of dementia care, such physiological markers of relaxation may translate into practical benefits, such as reduced agitation or improved emotional regulation, especially when non-pharmacological approaches are prioritized. Supporting this, Kim and Kim [
18] found that older adults aged over 70 reported marked improvements in subjective mental health, including greater relaxation, happiness, and reduced stress, following exposure to immersive natural environments via IVR. Similarly, Veling et al. [
19] observed that immersive VR-based relaxation (VRelax), using 360° nature videos, was significantly more effective than standard relaxation exercises in reducing momentary anxiety and sadness in patients with psychiatric disorders. Taken together, our findings, supported by growing evidence in the literature, suggest that IVR may serve not only as a source of sensory engagement but also as a viable therapeutic strategy to promote physiological calm and enhance emotional well-being in older adults living with dementia.
In contrast, affective responses measured by the I-PANAS-SF scale did not show significant changes over time or between groups. Nonetheless, the interaction between time and group approached significance, and the observed change in I-PANAS-SF scores for the experimental group was very close to the calculated minimal clinically important difference (MCID). Specifically, while the MCID was calculated at 2.878, the observed improvement in the experimental condition was +2.714. Although this change did not strictly meet the threshold for clinical significance, its proximity to the MCID suggests a potentially promising trend that may reach meaningful levels with a larger sample or extended intervention periods. In contrast, the decrease observed in the control group did not meet the MCID threshold and may reflect random variation rather than a true effect. It is worth noting that in our study, I-PANAS-SF scores were obtained during the week preceding and following the intervention period, rather than immediately after each VR exposure. This delayed measurement may have limited the sensitivity to detect short-term mood enhancements. Supporting this interpretation, Chan et al. [
20] reported significant improvements in positive and negative affect immediately after VR sessions among community-dwelling older adults.
The analysis of state and trait anxiety scores using the reduced STAIr did not reveal any significant effects, indicating no measurable changes in perceived anxiety levels as a result of the interventions. This could be due to several factors, including limited sensitivity of the tool in this population, the brief duration of exposure, or the relatively stable nature of trait anxiety. Another important consideration is the timing of the assessments. In our study, anxiety was measured during the week prior and the week after the intervention period, potentially missing the immediate anxiolytic effects of the VR sessions. Supporting this hypothesis, Niki et al. [
21] demonstrated that immersive VR reminiscence significantly reduced anxiety in participants immediately following each exposure, with reductions exceeding the minimal clinically important difference for the STAI. Additionally, participants in their trial expressed a clear preference for live-action imagery over computer-generated scenes, suggesting that higher realism may enhance emotional engagement and therapeutic efficacy—a finding that aligns with our strategy of employing 360° photorealistic environments tailored to participant preferences.
Behavioral observations during the sessions indicated a trend toward higher behavioral response scores during the YouTube condition compared to the Nature Treks VR intervention. This suggests that participants were more responsive and engaged during the YouTube sessions, potentially due to the fact that these videos were directly related to their personal interests and were frequently requested by the participants themselves. Although the difference in behavioral responses did not reach statistical significance, the increased responsiveness to the YouTube condition—when compared to the inherently positive and calming effects observed during the Nature Treks VR exposure—may highlight the potential benefits of incorporating emotionally meaningful and personally relevant content into intervention programs. Although the videos were not typically autobiographical or personally familiar, their selection was driven by the participants’ own interests—such as iconic landmarks, concerts, or culturally significant places—which likely enhanced attentional engagement through increased relevance and perceived agency. This personalization, even in the absence of direct familiarity, may have acted as a moderating factor in behavioral responsiveness and should be considered in future studies comparing different types of immersive content. This finding is consistent with previous research emphasizing the importance of meaningful activities in fostering a sense of enjoyment and connection in individuals with dementia [
22]. Tailoring digital activities to align with individual preferences could foster greater engagement and emotional connection, thereby enhancing the overall therapeutic value of such interventions.
Of particular note are the findings from the subjective response questionnaire, which demonstrated uniformly positive evaluations of the VR experience. All participants consistently reported feeling excited and calm, without experiencing feelings of upset or anxiety, and unanimously rated the virtual scenarios as realistic. These consistent responses point to a strong acceptance and positive perception of the VR intervention among participants. Nevertheless, it is important to consider the potential influence of social desirability bias, particularly given the vulnerable population involved. Participants may have provided consistently positive responses, at least in part, due to a desire to please the researcher or as a consequence of limited insight into their emotional state, which is not uncommon in individuals with cognitive impairments. This possibility underscores the importance of triangulating self-report measures with objective behavioral and physiological data. Future studies could consider methods to reduce social desirability bias, such as implementing anonymous or confidential self-report procedures, as recommended by Setiawati et al. [
23], to enhance the validity of subjective feedback. We also plan to adopt a simplified three-point Likert scale to capture more nuanced emotional responses while preserving clarity and accessibility for individuals with cognitive impairments.
Regarding the feasibility of IVR integration into routine dementia care, recent studies offer encouraging evidence. Kim et al. [
6] showed that a five-week nature-based IVR program improved emotional states and quality of life in individuals with Alzheimer’s disease, despite minor usability challenges. Likewise, a scoping review by Rose et al. [
24] highlighted that semi- and fully immersive VR systems are generally well tolerated and provide valuable stimulation, particularly in early to moderate dementia stages. Complementing these findings, a recent systematic review and meta-analysis by Wen et al. [
25] concluded that VR-based nursing interventions significantly improve cognitive function, quality of life, activities of daily living, and reduce negative emotions in patients with dementia. These results collectively support the practical implementation of IVR as a non-pharmacological strategy to promote emotional resilience and well-being in dementia care settings.
Finally, our findings align with the conclusions of the recent scoping review by Buele et al. [
5], which reported that immersive VR interventions show positive effects on emotional well-being and neuropsychiatric symptoms in people with dementia, including reductions in apathy and depression. Although the review identified mixed results regarding cognitive improvements, it emphasized the therapeutic value of VR in enhancing emotional engagement and subjective well-being. In line with these observations, our study found physiological and self-reported indicators of emotional benefit following exposure to immersive, naturalistic VR environments, despite the absence of significant cognitive or anxiety-related changes. These results further support the use of IVR as a viable, non-pharmacological strategy to promote emotional health in dementia care, even if cognitive outcomes remain more variable and require further investigation.
Limitations and Future Directions
A primary limitation of this study is its small sample size, which restricts statistical power and limits the generalizability of the findings. Future studies should include larger and more diverse samples to confirm these preliminary results. Extending the intervention period may also allow for the detection of longer-term effects on emotional well-being. It is also worth noting that the variability in behavioral responses across participants likely reflects individual differences in expressiveness and baseline engagement, which are common in this population. Regarding physiological outcomes, heart rate (HR) was the only autonomic marker assessed. While HR is a widely accepted and accessible indicator of autonomic arousal, it does not capture the full complexity of physiological regulation. Future studies could benefit from including additional measures such as heart rate variability, skin conductance, or respiratory patterns to provide a more nuanced understanding of the physiological effects of immersive VR. Furthermore, the use of complementary assessment tools, such as proxy reports from caregivers or behavioral observation scales tailored for dementia populations, could provide a more comprehensive evaluation of the intervention’s impact.







{kind=link}
{kind=link}
{kind=link}
{kind=link}