
Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion

 ,
,
Abstract
1. Introduction
2. Materials and Methods
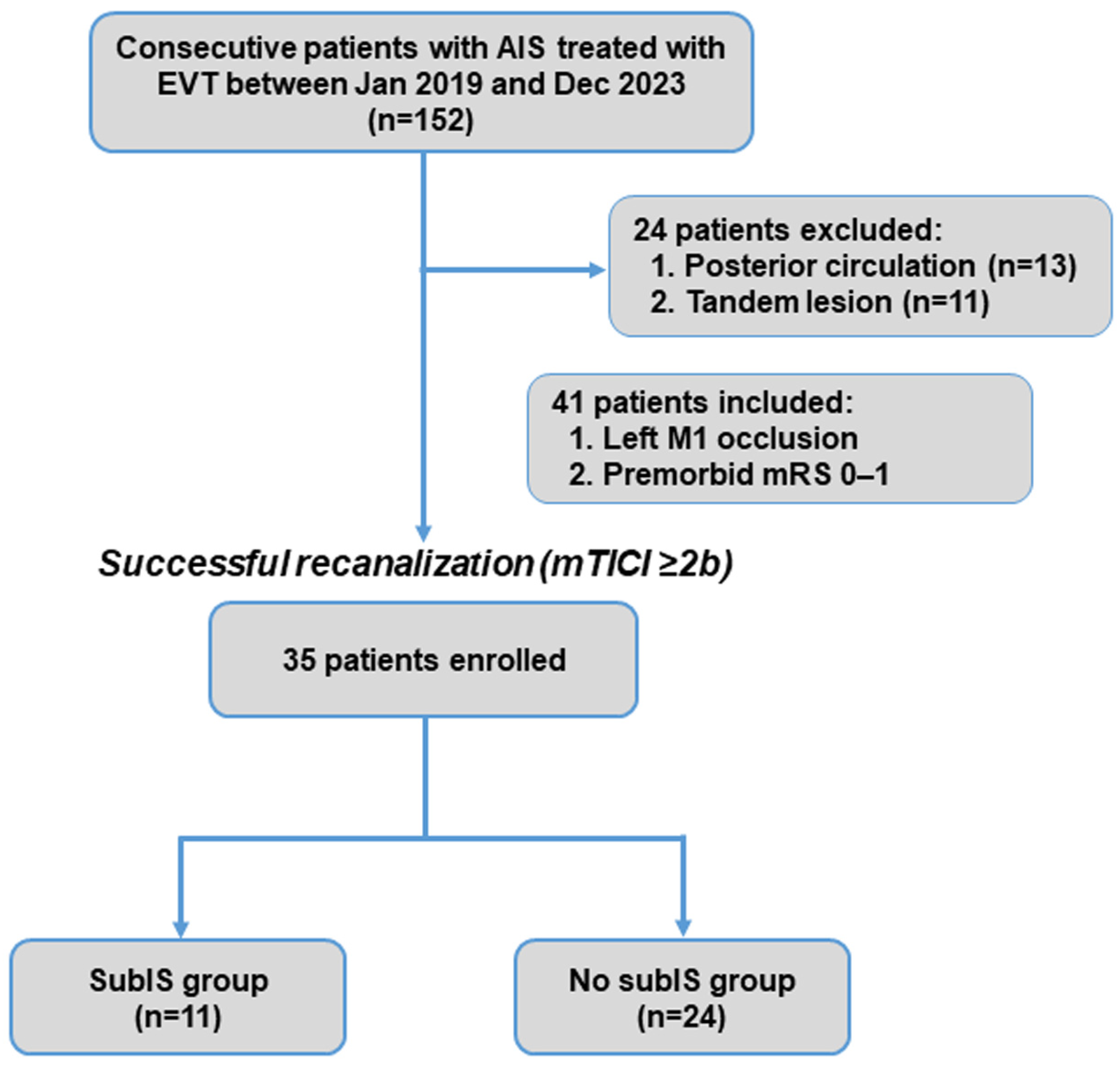
2.1. Study Design and Patient Definitions
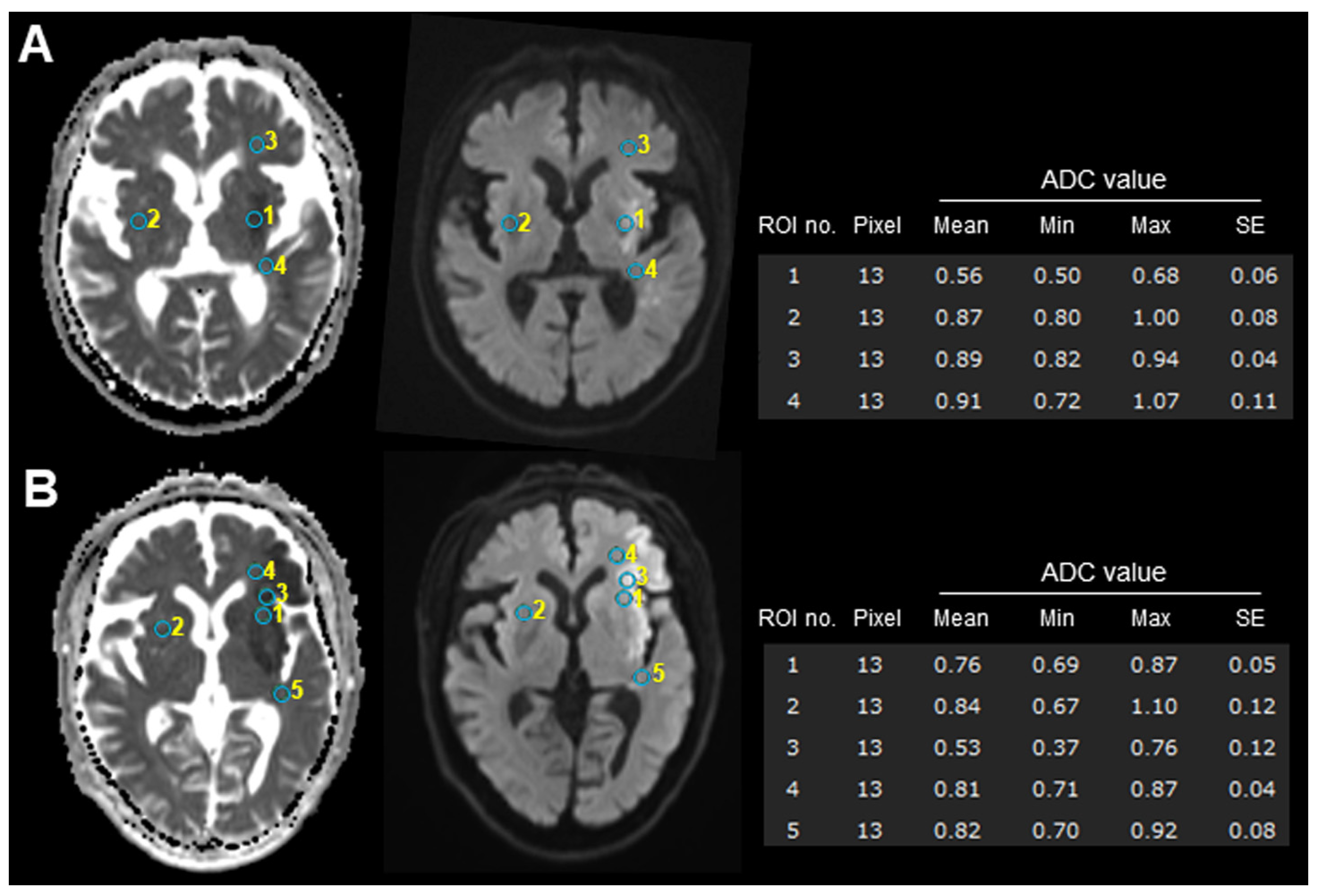
2.2. Data Collection
2.3. Outcome Assessments
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
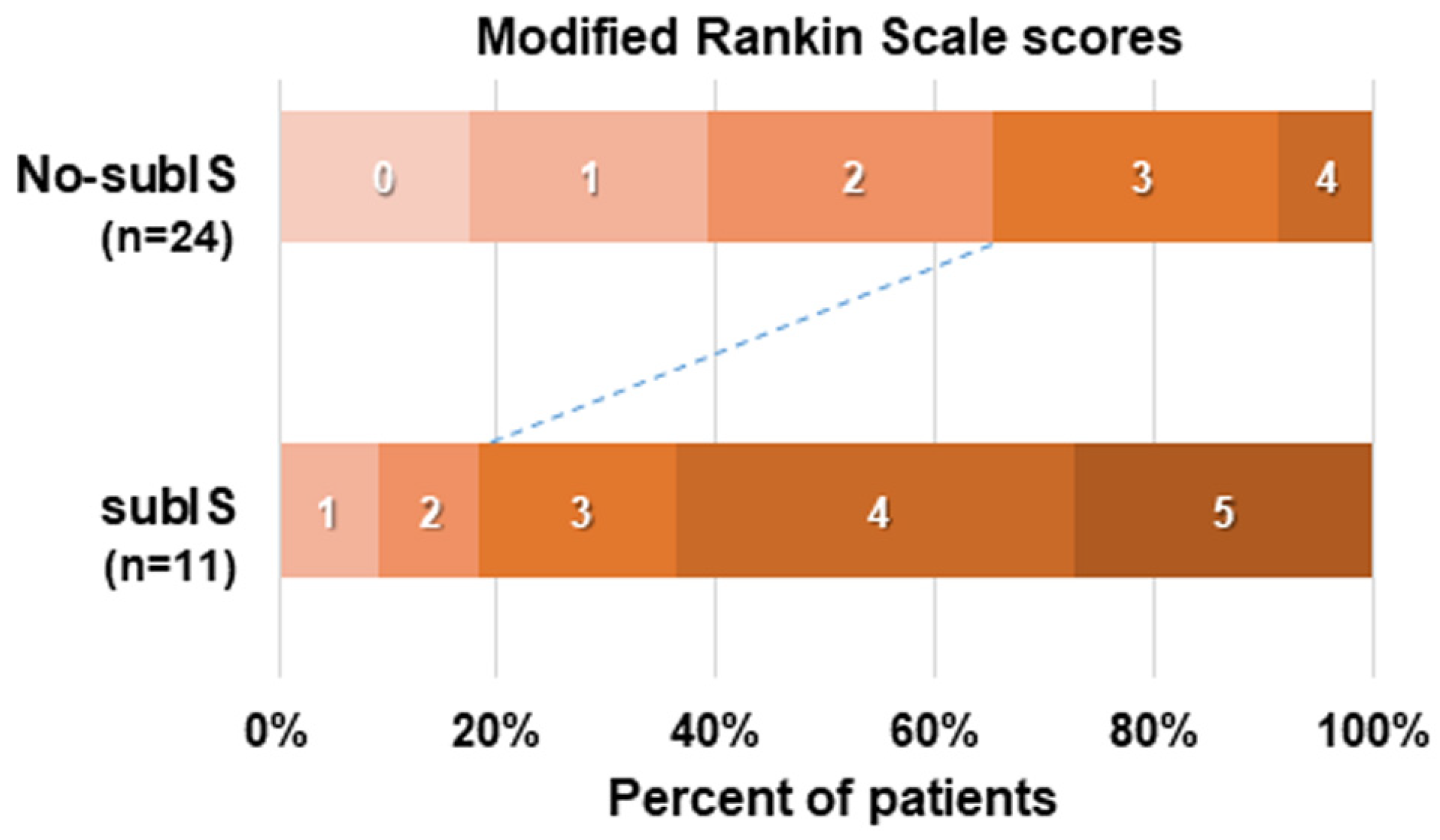
3.2. Clinical Outcomes and Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wada, S.; Yoshimura, S.; Miwa, K.; Iwanaga, Y.; Koga, M.; Toyoda, K. Current status and future aspects in the Japan Stroke Data Bank. Front. Neurol. 2023, 14, 1090136. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Che, R.; Xu, J.; Guo, W.; Chen, X.; Zhao, W.; Ren, C.; Jia, M.; Ji, X. Long term for patients with futile endovascular reperfusion after stroke. CNS Neurosci. Ther. 2024, 30, e14588. [Google Scholar] [CrossRef]
- Shen, H.; Killingsworth, M.C.; Bhaskar, S.M.M. Comprehensive meta-analysis of futile recanalization in acute ischemic stroke patients undergoing endovascular thrombectomy: Prevalence, factors, and clinical outcomes. Life 2023, 13, 1965. [Google Scholar] [CrossRef]
- Sun, Y.; Jou, E.; Nguyen, T.N.; Mofatteh, M.; Liang, Q.; Abdalkader, M.; Yan, Z.; Feng, M.; Li, X.; Li, G.; et al. Predictors of futile recanalization after endovascular treatment in acute ischemic stroke: A multi-center study. Front. Neurosci. 2023, 17, 1279366. [Google Scholar] [CrossRef]
- Li, Z.; Chu, Z.; Zhao, S.; Ma, L.; Yang, Q.; Huang, X.; Zhou, Z. Severe stroke patients with left-sided occlusion of the proximal anterior circulation benefit more from thrombectomy. Front. Neurol. 2019, 10, 551. [Google Scholar] [CrossRef]
- Mutoh, T.; Yoshida, Y.; Tatewaki, Y.; Chin, H.; Tochinai, R.; Moroi, J.; Ishikawa, T. Diffusion MRI fiber tractography and benzodiazepine SPECT imaging for assessing neural damage to the language Centers in an elderly patient after successful reperfusion therapy. Geriatrics 2024, 9, 30. [Google Scholar] [CrossRef]
- Pedraza, M.I.; de Lera, M.; Bos, D.; Calleja, A.I.; Cortijo, E.; Gómez-Vicente, B.; Reyes, J.; Coco-Martín, M.B.; Calonge, T.; Agulla, J.; et al. Brain Atrophy and the Risk of Futile Endovascular Reperfusion in Acute Ischemic Stroke. Stroke 2020, 51, 1514–1521. [Google Scholar] [CrossRef]
- Menon, B.K.; Qazi, E.; Nambiar, V.; Foster, L.D.; Yeatts, S.D.; Liebeskind, D.; Jovin, T.G.; Goyal, M.; Hill, M.D.; Tomsick, T.A.; et al. Differential Effect of Baseline Computed Tomographic Angiography Collaterals on Clinical Outcome in Patients Enrolled in the Interventional Management of Stroke III Trial. Stroke 2015, 46, 1239–1244. [Google Scholar] [CrossRef]
- Jeon, Y.S.; Kim, H.J.; Roh, H.G.; Lee, T.J.; Park, J.J.; Lee, S.B.; Lee, H.J.; Kwak, J.T.; Lee, J.S.; Ki, H.J. Impact of Collateral Circulation on Futile Endovascular Thrombectomy in Acute Anterior Circulation Ischemic Stroke. J. Korean Neurosurg. Soc. 2024, 67, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Al-Dasuqi, K.; Payabvash, S.; Torres-Flores, G.A.; Strander, S.M.; Nguyen, C.K.; Peshwe, K.U.; Kodali, S.; Silverman, A.; Malhotra, A.; Johnson, M.H.; et al. Effects of Collateral Status on Infarct Distribution Following Endovascular Therapy in Large Vessel Occlusion Stroke. Stroke 2020, 51, e193–e202. [Google Scholar] [CrossRef] [PubMed]
- Grange, S.; Grange, R.; Garnier, P.; Varvat, J.; Marinescu, D.; Barral, F.G.; Boutet, C.; Schneider, F.C. Boundary and vulnerability estimation of the internal borderzone using ischemic stroke lesion mapping. Sci. Rep. 2020, 10, 1662. [Google Scholar] [CrossRef]
- Efendizade, A.; Chaudhry, Z.A.; Velayudhan, V.; Bell, D.L. Letter by Efendizade et al. Regarding Article, “Effects of Collateral Status on Infarct Distribution Following Endovascular Therapy in Large Vessel Occlusion Stroke”. Stroke 2021, 52, e42–e43. [Google Scholar] [CrossRef]
- Kumral, E.; Ozdemirkiran, T.; Alper, Y. Strokes in the subinsular territory: Clinical, topographical, and etiological patterns. Neurology 2004, 63, 2429–2432. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.H.; Pullicino, P.M.; Benedict, R. Deep cerebral infarcts extending to the subinsular region. Stroke 2001, 32, 2272–2277. [Google Scholar] [CrossRef]
- Cereda, C.; Ghika, J.; Maeder, P.; Bogousslavsky, J. Strokes restricted to the insular cortex. Neurology 2002, 59, 1950–1955. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, V.; De Angelis, M.V.; Montemitro, C.; Russo, M.; Carrarini, C.; di Giannantonio, M.; Brighina, F.; Onofrj, M.; Werring, D.J.; Simister, R. Clinical presentation of strokes confined to the insula: A systematic review of literature. Neurol. Sci. 2021, 42, 1697–1704. [Google Scholar] [CrossRef]
- Yang, X.; Sun, D.; Huo, X.; Raynald, R.; Jia, B.; Tong, X.; Wang, A.; Ma, N.; Gao, F.; Mo, D.; et al. Futile reperfusion of endovascular treatment for acute anterior circulation large vessel occlusion in the ANGEL-ACT registry. J. Neurointerv. Surg. 2023, 15, e363–e368. [Google Scholar] [CrossRef]
- Cobb, S.R.; Mehringer, C.M.; Itabashi, H.H.; Pribram, H. CT of subinsular infarction and ischemia. AJNR Am. J. Neuroradiol. 1987, 8, 221–227. [Google Scholar]
- Brucher, J.M. Leukoencephalopathies in Anoxic-Ischemic Processes; Elsevier: Amsterdam, The Netherlands, 1985; Volume 47, pp. 525–549. [Google Scholar]
- Iwasaki, Y.; Igarashi, O.; Ichikawa, Y.; Ikeda, K. Strokes in the subinsular territory: Clinical, topographical, and etiological patterns. Neurology 2005, 64, 2164. [Google Scholar] [CrossRef] [PubMed]
- Arya, N.P.; Seth, N.H.; Burile, G.C.; Raghuveer, R. Targeted Physiotherapy for an Interesting Case of Spontaneously Resolving Extracapsular Infarct: A Case Report. Cureus 2024, 16, e52348. [Google Scholar] [CrossRef] [PubMed]
- Lanska, D.J. Strokes in the subinsular territory: Clinical, topographical, and etiological patterns. Neurology 2005, 65, 1146. [Google Scholar] [CrossRef] [PubMed]
- Varjačić, A.; Mantini, D.; Levenstein, J.; Slavkova, E.D.; Demeyere, N.; Gillebert, C.R. The role of left insula in executive set-switching: Lesion evidence from an acute stroke cohort. Cortex 2018, 107, 92–101. [Google Scholar] [CrossRef]
- Dick, A.S.; Garic, D.; Graziano, P.; Tremblay, P. The frontal aslant tract (FAT) and its role in speech, language and executive function. Cortex 2019, 111, 148–163. [Google Scholar] [CrossRef]
- Shen, H.; Huasen, B.B.; Killingsworth, M.C.; Bhaskar, S.M.M. Introducing the futile recanalization prediction score (FRPS): A novel approach to predict and mitigate ineffective recanalization after endovascular treatment of acute ischemic stroke. Neurol. Int. 2024, 16, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.R.; Li, B.H.; Zhang, Q.; Cheng, X.D.; Jia, L.J.; Zhou, S.; Yang, S.; Wang, J.H.; Yu, N.W. Predictors of futile recanalization after endovascular treatment of acute ischemic stroke. BMC Neurol. 2024, 24, 207. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 35) | subIS (n = 11) | No-subIS (n = 24) | p Value |
|---|---|---|---|---|
| Age, median (IQR) | 78 (72–86) | 81 (78–89) | 75 (72–83) | 0.04 * |
| Female gender, n (%) | 14 (40) | 3 (28) | 11 (46) | 0.25 |
| Hypertension, n (%) | 22 (63) | 7 (64) | 15 (63) | 0.62 |
| Diabetes mellitus, n (%) | 10 (29) | 5 (45) | 5 (21) | 0.13 |
| AF, n (%) | 12 (34) | 3 (27) | 9 (38) | 0.42 |
| Premorbid mRS, median (IQR) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.94 |
| Baseline SBP, mean (SD) | 161.0 (19.8) | 162.4 (21.6) | 160.3 (19.4) | 0.65 |
| Baseline NIHSS, median (IQR) | 17 (12–23) | 19 (18–24) | 15 (12–22) | 0.09 |
| Unknown onset stroke, n (%) | 10 (29) | 3 (27) | 7 (29) | 0.62 |
| Wake-up stroke, n (%) | 3 (9) | 2 (18) | 3 (13) | |
| Daytime-unwitnessed stroke, n (%) | 7 (20) | 1 (9) | 4 (16) | |
| ASPECTS, median (IQR) | 9 (8–10) | 9 (7–9) | 9 (8–10) | 0.32 |
| ADC value, mean (SD) | 0.59 (0.11) | 0.52 (0.08) | 0.62 (0.10) | 0.006 * |
| Treatment with IV alteplase, n (%) | 18 (51) | 6 (55) | 12 (50) | 0.55 |
| Time intervals, mean (SD) minutes | ||||
| OTD | 261 (345) | 246 (195) | 268 (394) | 0.21 |
| OTR | 363 (342) | 295 (83) | 388 (396) | 0.52 |
| PTR | 48 (26) | 43 (26) | 51 (26) | 0.18 |
| First pass, n (%) | 15 (43) | 6 (55) | 9 (38) | 0.28 |
| Stent retriever, n (%) | 29 (85) | 9 (82) | 20 (83) | 0.63 |
| TOAST, n (%) | ||||
| Large artery atherosclerosis | 2 (6) | 0 (0) | 2 (8) | |
| Cardioembolism | 27 (77) | 9 (82) | 18 (75) | |
| Other or undetermined | 6 (25) | 2 (18) | 4 (17) | |
| sICH, n (%) | 2 (6) | 1 (9) | 1 (4) | 0.54 |
| ENI, n (%) | 14 (40) | 3 (27) | 11 (46) | 0.25 |
| Three-month mRS, median (IQR) | 2 (2–4) | 4 (3–5) | 2 (1–3) | <0.001 * |
| Futile recanalization (mRS ≥ 3), n (%) | 17 (49) | 9 (81) | 8 (33) | 0.01 * |
| Variables | aOR | 95% CI | p Value |
|---|---|---|---|
| Age | 0.99 | 0.91–1.08 | 0.85 |
| NIHSS on admission | 1.13 | 0.98–1.30 | 0.09 |
| SubIS involvement | 10.52 | 1.53–72.3 | 0.017 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, Y.; Mutoh, T.; Tatewaki, Y.; Taki, Y.; Moroi, J.; Ishikawa, T. Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion. Brain Sci. 2024, 14, 885. https://doi.org/10.3390/brainsci14090885
Yoshida Y, Mutoh T, Tatewaki Y, Taki Y, Moroi J, Ishikawa T. Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion. Brain Sciences. 2024; 14(9):885. https://doi.org/10.3390/brainsci14090885
Chicago/Turabian StyleYoshida, Yasuyuki, Tatsushi Mutoh, Yasuko Tatewaki, Yasuyuki Taki, Junta Moroi, and Tatsuya Ishikawa. 2024. "Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion" Brain Sciences 14, no. 9: 885. https://doi.org/10.3390/brainsci14090885
APA StyleYoshida, Y., Mutoh, T., Tatewaki, Y., Taki, Y., Moroi, J., & Ishikawa, T. (2024). Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion. Brain Sciences, 14(9), 885. https://doi.org/10.3390/brainsci14090885