

A New Perspective on the Cavernous Sinus as Seen through Multiple Surgical Corridors: Anatomical Study Comparing the Transorbital, Endonasal, and Transcranial Routes and the Relative Coterminous Spatial Regions
 ,
,  , , ,
, , ,
Abstract
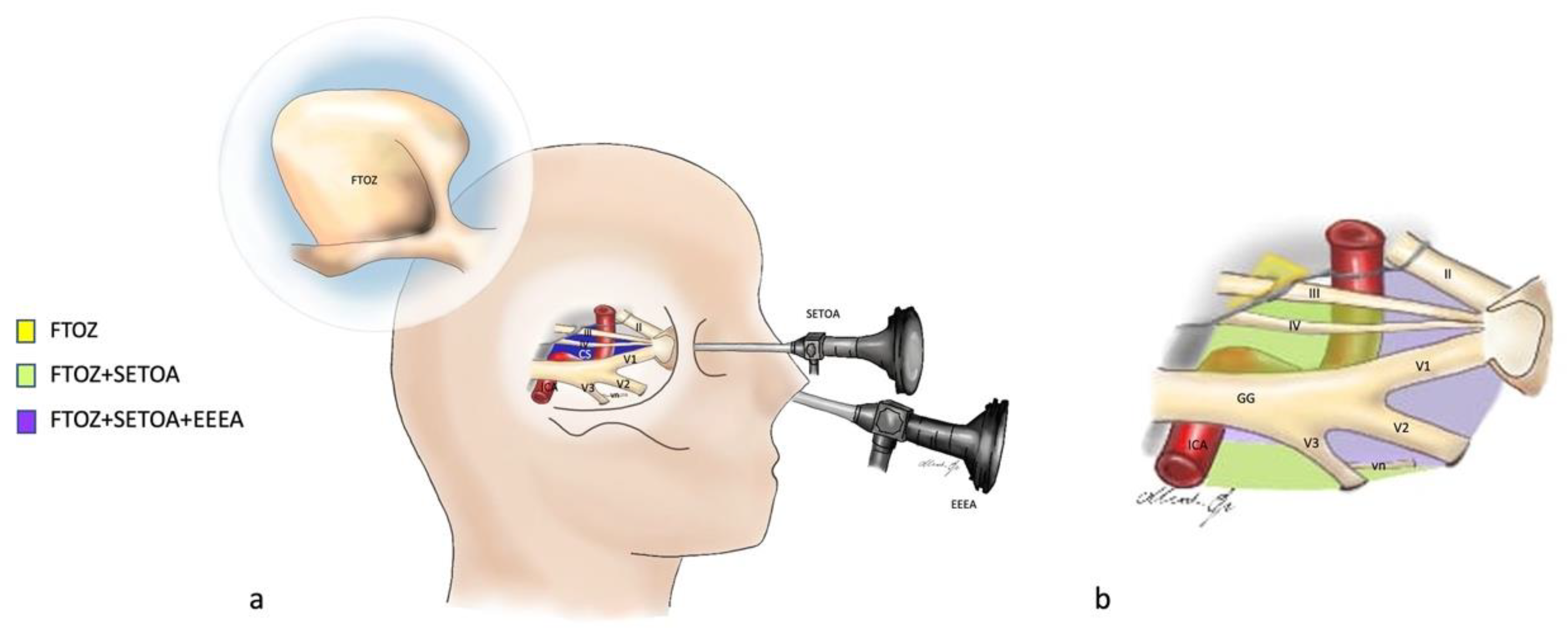
:1. Introduction
2. Materials and Methods
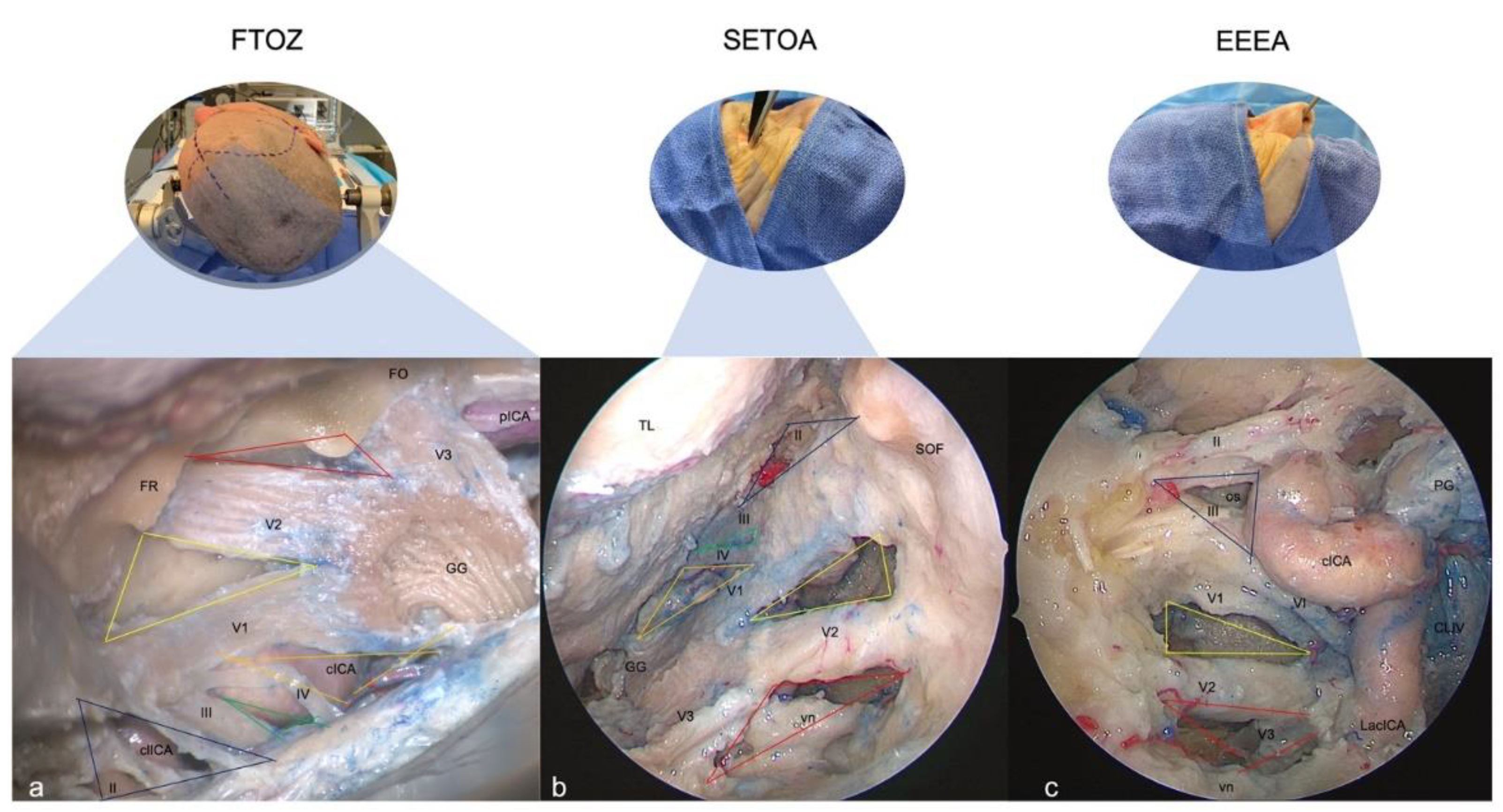
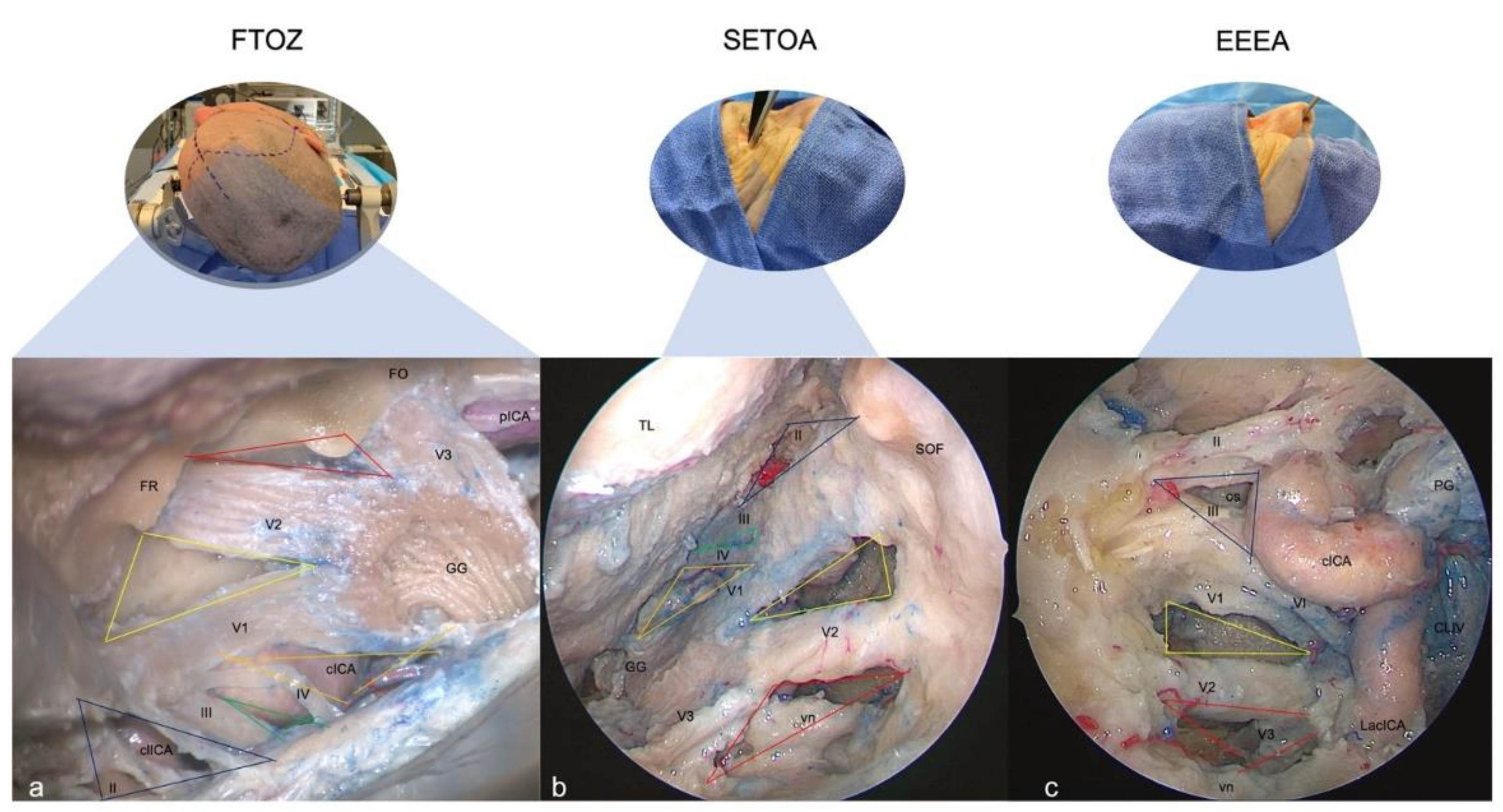
2.1. Fronto-Temporo-Orbito-Zygomatic (FTOZ) Approach
2.2. Superior Eyelid Transorbital Endoscopic Approach (SETOA)
2.3. Extended Endoscopic Endonasal Transsphenoidal Transethmoidal Approach (EEEA)
3. Results
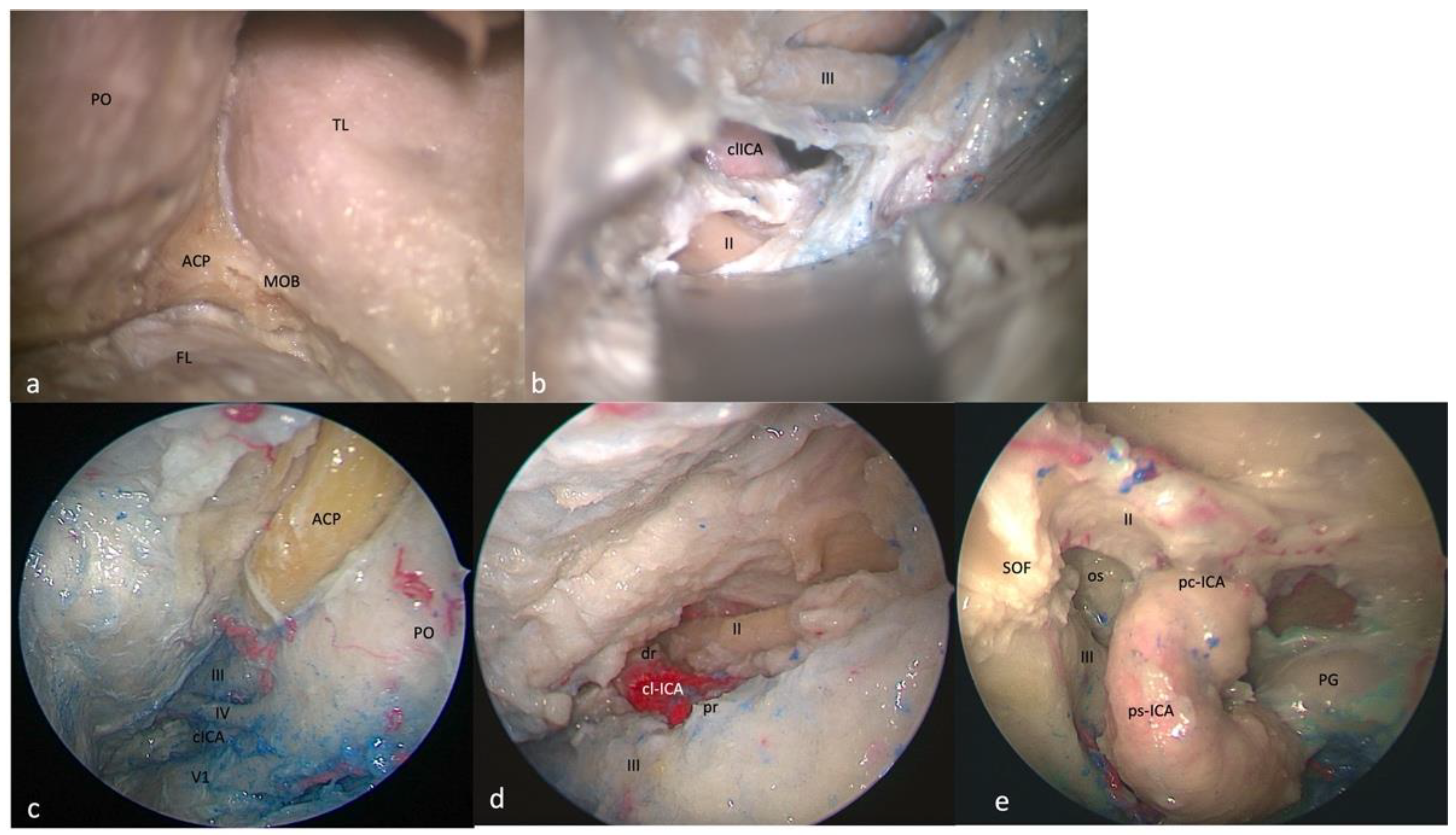
3.1. Clinoid Triangle (Dolenc’s Triangle)
3.1.1. FTOZ Perspective
3.1.2. SETOA Perspective
3.1.3. EEEA Perspective
3.2. Oculomotor Triangle (Hakuba’s Triangle)
3.2.1. FTOZ Perspective
3.2.2. SETOA Perspective
3.2.3. EEEA Perspective
3.3. Supratrochlear Triangle (Paramedian)
3.3.1. FTOZ Perspective
3.3.2. SETOA Perspective
3.3.3. EEEA Perspective
3.4. Infratrochlear Triangle (Parkinson’s triangle)
3.4.1. FTOZ Perspective
3.4.2. SETOA Perspective
3.4.3. EEEA Perspective
3.5. Anteromedial Triangle (Mullan’s Triangle)
3.5.1. FTOZ Perspective
3.5.2. SETOA Perspective
3.5.3. EEEA Perspective
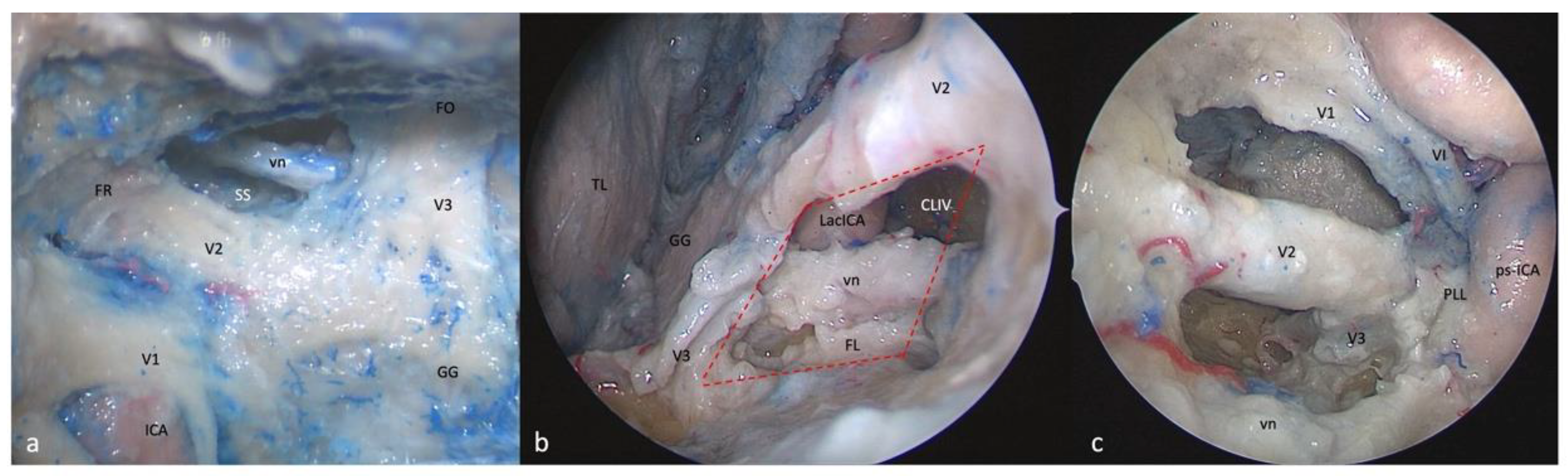
3.6. Anterolateral Triangle
3.6.1. FTOZ Perspective
3.6.2. SETOA Perspective
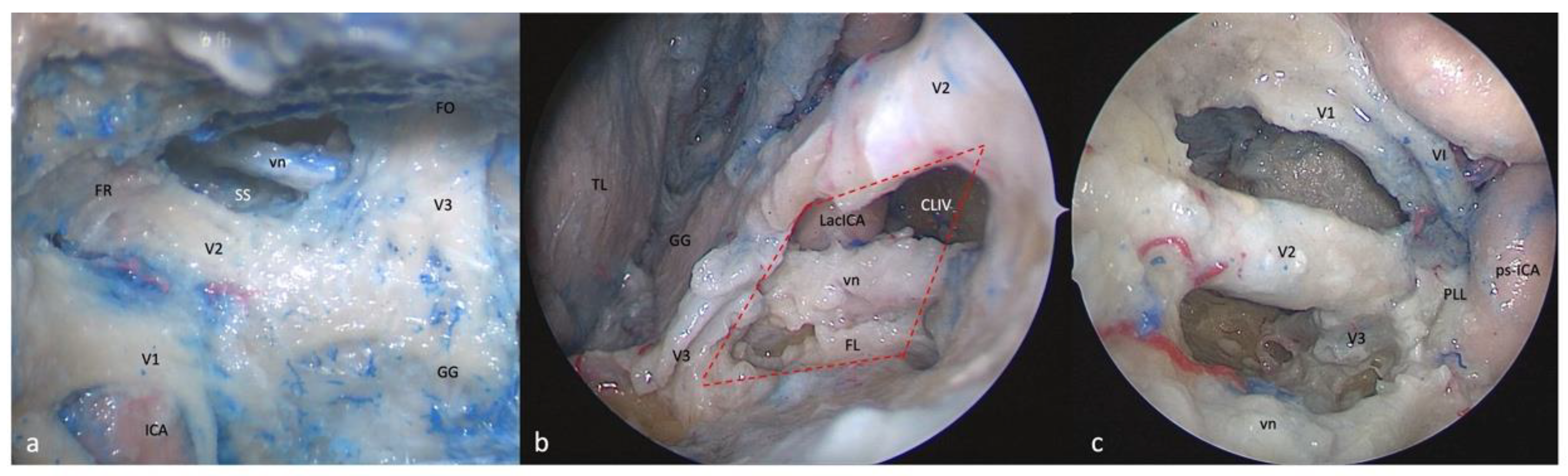
- (a)
- A wider superior window (“supravidian”) that discloses two corridors in relationship to the lacerum segments of the ICA: a “medial supravidian corridor” leading to the lower clivus, and a “lateral supravidian corridor” leading, after gentle lateralization of the Gasserian ganglion, to the medial aspect of the Meckel’s cave and the terminal portion of the horizontal petrous ICA (pICA).
- (b)
- A narrow inferior window (“infravidian”) that includes the inferior portion of the foramen lacerum distally, and the sphenoid sinus proximally.
3.6.3. EEEA Perspective
4. Discussion
4.1. Anatomical Considerations
4.2. Surgical Nuances
4.3. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SETOA | Superior eyelid transorbital endoscopic approach |
| EEEA | Extended endoscopic endonasal approach |
| ICA | Internal carotid artery |
| GG | Gasserian ganglion |
| MOB | Meningo-orbital band |
| MMA | Middle meningeal artery |
| CS | Cavernous sinus |
| FL | Foramen lacerum |
| PL | Petrolingual ligament |
| vn | Vidian nerve |
| pICA | Petrous internal carotid artery |
| FTOZ | Fronto-t’emporo-orbito-zygomatic |
| MC | Meckel’s cave |
References
- Vural, A.; Carobbio, A.L.C.; Ferrari, M.; Rampinelli, V.; Schreiber, A.; Mattavelli, D.; Doglietto, F.; Buffoli, B.; Rodella, L.F.; Taboni, S.; et al. Transorbital endoscopic approaches to the skull base: A systematic literature review and anatomical description. Neurosurg. Rev. 2021, 44, 2857–2878. [Google Scholar] [CrossRef] [PubMed]
- Corvino, S.; Guizzardi, G.; Sacco, M.; Corrivetti, F.; Bove, I.; Enseñat, J.; Colamaria, A.; Prats-Galino, A.; Solari, D.; Cavallo, L.M.; et al. The feasibility of three port endonasal, transorbital, and sublabial approach to the petroclival region: Neurosurgical audit and multiportal anatomic quantitative investigation. Acta Neurochir. 2023, 165, 1821–1831. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, D. A surgical approach to the cavernous portion of the carotid artery. Anatomical studies and case report. J. Neurosurg. 1965, 23, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Harris, F.S.; Rhoton, A.L. Anatomy of the cavernous sinus. A microsurgical study. J. Neurosurg. 1976, 45, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Rhoton, A.L.; Theele, D.; Barry, M.E. Surgical approaches to the cavernous sinus: A microsurgical study. Neurosurgery 1990, 26, 903–932. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Wei, X.; Zhao, C. Microsurgical anatomical study of the wall of the cavernous sinus. Zhonghua Yi Xue Za Zhi 1996, 76, 855–858. [Google Scholar]
- Jian, F.Z.; Santoro, A.; Innocenzi, G.; Wang, X.W.; Liu, S.S.; Cantore, G. Frontotemporal orbitozygomatic craniotomy to exposure the cavernous sinus and its surrounding regions. Microsurgical anatomy. J. Neurosurg. Sci. 2001, 45, 19–28. [Google Scholar]
- Yasuda, A.; Campero, A.; Martins, C.; Rhoton, A.L.; Ribas, G.C. The medial wall of the cavernous sinus: Microsurgical anatomy. Neurosurgery 2004, 55, 179–189; discussion 189–190. [Google Scholar] [CrossRef]
- Isolan, G.R.; Krayenbühl, N.; de Oliveira, E.; Al-Mefty, O. Microsurgical Anatomy of the Cavernous Sinus: Measurements of the Triangles in and around It. Skull Base 2007, 17, 357–367. [Google Scholar] [CrossRef]
- Sekhar, L.N.; Burgess, J.; Akin, O. Anatomical study of the cavernous sinus emphasizing operative approaches and related vascular and neural reconstruction. Neurosurgery 1987, 21, 806–816. [Google Scholar] [CrossRef]
- Al-Mefty, O.; Smith, R.R. Surgery of tumors invading the cavernous sinus. Surg. Neurol. 1988, 30, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Cusimano, M.D.; Sekhar, L.N.; Sen, C.N.; Pomonis, S.; Wright, D.C.; Biglan, A.W.; Jannetta, P.J. The results of surgery for benign tumors of the cavernous sinus. Neurosurgery 1995, 37, 1–9; discussion 9–10. [Google Scholar] [CrossRef] [PubMed]
- Dolenc, V. Direct microsurgical repair of intracavernous vascular lesions. J. Neurosurg. 1983, 58, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Hakuba, A.; Matsuoka, Y.; Suzuki, T.; Komiyama, M.; Jin, T.B.; Inoue, Y. Direct Approaches to Vascular Lesions in the Cavernous Sinus via the Medial Triangle. In The Cavernous Sinus: A Multidisciplinary Approach to Vascular and Tumorous Lesions; Dolenc, V.V., Ed.; Springer: Vienna, Austria, 1987; pp. 272–284. [Google Scholar] [CrossRef]
- Rhoton, A.L. The cavernous sinus, the cavernous venous plexus, and the carotid collar. Neurosurgery 2002, 51, S375–S410. [Google Scholar] [CrossRef] [PubMed]
- Doglietto, F.; Lauretti, L.; Frank, G.; Pasquini, E.; Fernandez, E.; Tschabitscher, M.; Maira, G. Microscopic and endoscopic extracranial approaches to the cavernous sinus: Anatomic study. Neurosurgery 2009, 64, 413–421; discussion 421–422. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, F.; Haque, M.; Kawsar, K.; Ara, S.; Mohammod, Q.; Sarker, M.; Goel, A. Transcranial microsurgical and endoscopic endonasal cavernous sinus (CS) anatomy: A cadaveric study. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2012, 73, 296–306. [Google Scholar] [CrossRef]
- Alfieri, A.; Jho, H.D. Endoscopic endonasal approaches to the cavernous sinus: Surgical approaches. Neurosurgery 2001, 49, 354–360; discussion 352–360. [Google Scholar] [CrossRef]
- Alfieri, A.; Jho, H.D. Endoscopic endonasal cavernous sinus surgery: An anatomic study. Neurosurgery 2001, 48, 827–836; discussion 827–836. [Google Scholar]
- Cavallo, L.M.; Cappabianca, P.; Galzio, R.; Iaconetta, G.; de Divitiis, E.; Tschabitscher, M. Endoscopic transnasal approach to the cavernous sinus versus transcranial route: Anatomic study. Neurosurgery 2005, 56, 379–389; discussion 379–389. [Google Scholar] [CrossRef]
- Dallan, I.; Di Somma, A.; Prats-Galino, A.; Solari, D.; Alobid, I.; Turri-Zanoni, M.; Fiacchini, G.; Castelnuovo, P.; Catapano, G.; de Notaris, M. Endoscopic transorbital route to the cavernous sinus through the meningo-orbital band: A descriptive anatomical study. J. Neurosurg. 2017, 127, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.; Guizzardi, G.; Di Somma, A.; Lopez, P.; Mato, D.; Enseñat, J.; Prats-Galino, A. Comparison of Accessibility to Cavernous Sinus Areas Throughout Endonasal, Transorbital, and Transcranial Approaches: Anatomic Study With Quantitative Analysis. Oper. Neurosurg. (Hagerstown) 2023, 24, e271–e280. [Google Scholar] [CrossRef] [PubMed]
- Jung, I.H.; Yoo, J.; Choi, S.; Lim, S.H.; Ko, J.; Roh, T.H.; Hong, J.B.; Kim, E.H. Endoscopic transorbital approach to the cavernous sinus: Cadaveric anatomy study and clinical application. Front. Oncol. 2022, 12, 962598. [Google Scholar] [CrossRef]
- Bakan, A.A.; Alkan, A.; Kurtcan, S.; Aralaşmak, A.; Tokdemir, S.; Mehdi, E.; Özdemir, H. Cavernous Sinus: A Comprehensive Review of its Anatomy, Pathologic Conditions, and Imaging Features. Clin. Neuroradiol. 2015, 25, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Bouthillier, A.; van Loveren, H.R.; Keller, J.T. Segments of the internal carotid artery: A new classification. Neurosurgery 1996, 38, 425–432; discussion 423–432. [Google Scholar] [CrossRef]
- Labib, M.A.; Prevedello, D.M.; Carrau, R.; Kerr, E.E.; Naudy, C.; Abou Al-Shaar, H.; Corsten, M.; Kassam, A. A road map to the internal carotid artery in expanded endoscopic endonasal approaches to the ventral cranial base. Neurosurgery 2014, 10 (Suppl. S3), 448–471; discussion 471. [Google Scholar] [CrossRef]
- Yaşargil, M.G.; Reichman, M.V.; Kubik, S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J. Neurosurg. 1987, 67, 463–466. [Google Scholar] [CrossRef]
- Oikawa, S.; Mizuno, M.; Muraoka, S.; Kobayashi, S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy. Technical note. J. Neurosurg. 1996, 84, 297–299. [Google Scholar] [CrossRef]
- Zabramski, J.M.; Kiriş, T.; Sankhla, S.K.; Cabiol, J.; Spetzler, R.F. Orbitozygomatic craniotomy. Technical note. J. Neurosurg. 1998, 89, 336–341. [Google Scholar] [CrossRef]
- Fukuda, H.; Evins, A.I.; Burrell, J.C.; Iwasaki, K.; Stieg, P.E.; Bernardo, A. The Meningo-Orbital Band: Microsurgical Anatomy and Surgical Detachment of the Membranous Structures through a Frontotemporal Craniotomy with Removal of the Anterior Clinoid Process. J. Neurol. Surg. B Skull Base 2014, 75, 125–132. [Google Scholar] [CrossRef]
- Froelich, S.C.; Aziz, K.M.; Levine, N.B.; Theodosopoulos, P.V.; van Loveren, H.R.; Keller, J.T. Refinement of the extradural anterior clinoidectomy: Surgical anatomy of the orbitotemporal periosteal fold. Neurosurgery 2007, 61, 179–185; discussion 176–185. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, A.; Evins, A.I.; Barbagli, G.; Kim, M.G.; Kim, N.; Xia, J.J.; Nonaka, M.; Stieg, P.E. Tailored Surgical Access to the Cavernous Sinus and Parasellar Region: Assessment of Cavernous Sinus Entry Corridors and the Periclinoid and Pericavernous Surgical Maneuvers. World Neurosurg. 2023, 171, e253–e275. [Google Scholar] [CrossRef] [PubMed]
- Di Somma, A.; Andaluz, N.; Cavallo, L.M.; Topczewski, T.E.; Frio, F.; Gerardi, R.M.; Pineda, J.; Solari, D.; Enseñat, J.; Prats-Galino, A.; et al. Endoscopic transorbital route to the petrous apex: A feasibility anatomic study. Acta Neurochir. 2018, 160, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Moe, K.S.; Bergeron, C.M.; Ellenbogen, R.G. Transorbital neuroendoscopic surgery. Neurosurgery 2010, 67, ons16–ons28. [Google Scholar] [CrossRef]
- Corrivetti, F.; de Notaris, M.; Di Somma, A.; Dallan, I.; Enseñat, J.; Topczewski, T.; Solari, D.; Cavallo, L.M.; Cappabianca, P.; Prats-Galino, A. “Sagittal Crest”: Definition, Stepwise Dissection, and Clinical Implications from a Transorbital Perspective. Oper. Neurosurg. (Hagerstown) 2022, 22, e206–e212. [Google Scholar] [CrossRef]
- Wanibuchi, M.; Murakami, G.; Yamashita, T.; Minamida, Y.; Fukushima, T.; Friedman, A.H.; Fujimiya, M.; Houkin, K. Midsubtemporal ridge as a predictor of the lateral loop formed by the maxillary nerve and mandibular nerve: A cadaveric morphological study. Neurosurgery 2011, 69, ons95–ons98; discussion ons98. [Google Scholar] [CrossRef]
- Corvino, S.; Armocida, D.; Offi, M.; Pennisi, G.; Burattini, B.; Mondragon, A.V.; Esposito, F.; Cavallo, L.M.; de Notaris, M. The anterolateral triangle as window on the foramen lacerum from transorbital corridor: Anatomical study and technical nuances. Acta Neurochir. (Wien) 2023. [Google Scholar] [CrossRef]
- López, C.B.; Di Somma, A.; Cepeda, S.; Arrese, I.; Sarabia, R.; Agustín, J.H.; Topczewski, T.E.; Enseñat, J.; Prats-Galino, A. Extradural anterior clinoidectomy through endoscopic transorbital approach: Laboratory investigation for surgical perspective. Acta Neurochir. 2021, 163, 2177–2188. [Google Scholar] [CrossRef]
- Cavallo, L.M.; de Divitiis, O.; Aydin, S.; Messina, A.; Esposito, F.; Iaconetta, G.; Talat, K.; Cappabianca, P.; Tschabitscher, M. Extended endoscopic endonasal transsphenoidal approach to the suprasellar area: Anatomic considerations—Part 1. Neurosurgery 2008, 62, 1202–1212. [Google Scholar] [CrossRef]
- Ferrareze Nunes, C.; Lieber, S.; Truong, H.Q.; Zenonos, G.; Wang, E.W.; Snyderman, C.H.; Gardner, P.A.; Fernandez-Miranda, J.C. Endoscopic endonasal transoculomotor triangle approach for adenomas invading the parapeduncular space: Surgical anatomy, technical nuances, and case series. J. Neurosurg. 2018, 130, 1304–1314. [Google Scholar] [CrossRef]
- Fernandez-Miranda, J.C.; Zwagerman, N.T.; Abhinav, K.; Lieber, S.; Wang, E.W.; Snyderman, C.H.; Gardner, P.A. Cavernous sinus compartments from the endoscopic endonasal approach: Anatomical considerations and surgical relevance to adenoma surgery. J. Neurosurg. 2018, 129, 430–441. [Google Scholar] [CrossRef]
- Almeida, J.P.; de Andrade, E.; Reghin-Neto, M.; Radovanovic, I.; Recinos, P.F.; Kshettry, V.R. From Above and Below: The Microsurgical Anatomy of Endoscopic Endonasal and Transcranial Microsurgical Approaches to the Parasellar Region. World Neurosurg. 2022, 159, e139–e160. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, A.; Campero, A.; Martins, C.; Rhoton, A.L.; de Oliveira, E.; Ribas, G.C. Microsurgical anatomy and approaches to the cavernous sinus. Neurosurgery 2005, 56, 4–27; discussion 24–27. [Google Scholar] [CrossRef] [PubMed]
- Woodworth, G.F.; Patel, K.S.; Shin, B.; Burkhardt, J.K.; Tsiouris, A.J.; McCoul, E.D.; Anand, V.K.; Schwartz, T.H. Surgical outcomes using a medial-to-lateral endonasal endoscopic approach to pituitary adenomas invading the cavernous sinus. J. Neurosurg. 2014, 120, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Hong, S.D.; Woo, K.I.; Kim, Y.D.; Choi, J.W.; Seol, H.J.; Lee, J.I.; Shin, H.J.; Nam, D.H.; Kong, D.S. Endoscopic Endonasal Versus Transorbital Surgery for Middle Cranial Fossa Tumors: Comparison of Clinical Outcomes Based on Surgical Corridors. World Neurosurg. 2019, 122, e1491–e1504. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, F.; Komatsu, M.; Inoue, T.; Tschabitscher, M. Endoscopic supraorbital extradural approach to the cavernous sinus: A cadaver study. J. Neurosurg. 2011, 114, 1331–1337. [Google Scholar] [CrossRef]
- Corvino, S.; Sacco, M.; Somma, T.; Berardinelli, J.; Ugga, L.; Colamaria, A.; Corrivetti, F.; Iaconetta, G.; Kong, D.-S.; de Notaris, M. Functional and clinical outcomes after superior eyelid transorbital endoscopic approach for spheno-orbital meningiomas: Illustrative case and literature review. Neurosurg. Rev. 2022, 46, 1–12. [Google Scholar] [CrossRef]
- Inamasu, J.; Guiot, B.H. Iatrogenic carotid artery injury in neurosurgery. Neurosurg. Rev. 2005, 28, 239–247; discussion 248. [Google Scholar] [CrossRef]
- AlQahtani, A.; London, N.R.; Castelnuovo, P.; Locatelli, D.; Stamm, A.; Cohen-Gadol, A.A.; Elbosraty, H.; Casiano, R.; Morcos, J.; Pasquini, E.; et al. Assessment of Factors Associated With Internal Carotid Injury in Expanded Endoscopic Endonasal Skull Base Surgery. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 364–372. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Triangles | Clinoidal (Dolenc) | Supratrochlear | Infratrochlear (Parkinson) | Anteromedial (Mullan) | Anterolateral | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boundaries | - Lower border of II c.n. superiorly; - Upper border of III c.n. inferiorly | - Lower border of III c.n. superiorly; - Upper border of IV c.n. inferiorly | - Lower border of IV c.n. superiorly; - Upper border of V1 inferiorly | - Lower border of V1 superiorly; - Upper border of V2 inferiorly | - Lower border of V2 superiorly; - Upper border of V3 inferiorly | ||||||||||
| Approach | FTOZ | SETOA | EEEA | FTOZ | SETOA | EEEA | FTOZ | SETOA | EEEA | FTOZ | SETOA | EEEA | FTOZ | SETOA | EEEA |
| Surgical maneuvers for the exposition | Anterior clinoidectomy (augmented by peri-cavernous maneuvers) | Anterior clinoidectomy | --- | Peeling of the LWCS and middle fossa | Peeling of the LWCS and middle fossa | --- | Peeling of the LWCS and middle fossa | Peeling of the LWCS and middle fossa | --- | Peeling of the LWCS and middle fossa | Peeling of the LWCS and middle fossa | Removal of lateral wall of the sphenoid sinus | Peeling of the LWCS and middle fossa | Peeling of the LWCS and middle fossa | Removal of lateral wall of the sphenoid sinus |
| Content | cl-ICA, between upper and lower dural rings | cl-ICA, between upper and lower dural rings | Optic strut or optic-carotid recess | hc-ICA and MHT, ILT | hc-ICA | --- | Posterior bend of the c-ICA with MHT, VI c.n. | Superior half and posterior bend of posterior c-ICA with MHT | ILT; VI c.n. | Sphenoid sinus | Inferior half of the posterior segment of c-ICA; VI c.n. | Venous structures | Sphenoid sinus | Lacerum ICA; Sympathetic carotid plexus; FL; PLL; Vidian nerve and artery; | --- |
| Indications | Meningioma ACP, carotid-ophthalmic aneurysm | Meningioma ACP | --- | Schwan-nomas, CS tumors | Schwan-nomas, CS tumors | Pit- adenoma, chondro-sarcomas with lateral extension up to the CS lateral wall | Aneurysm or fistula of proximal c-ICA, CS tumors | Schwannomas, CS tumors | Pit- adenoma, chondro-sarcomas with lateral extension up to the CS lateral wall | Middle fossa tumors with CS invasion | Small lesion involving the anteroinferior compartment of CS | Pit- adenoma, chondro-sarcomas with lateral extension up to the CS lateral wall | --- | Small lesion involving the anteroinferior compartment of CS | Pit- adenoma, chondro-sarcomas with lateral extension up to the CS lateral wall |
| Safety of surgical access | Low risk  | Low risk  | Low risk  | Mid risk  | Mid risk  | Mid risk  | Mid risk  | Mid risk  | Mid risk  | Low risk  | Mid risk  | Low risk  | Low risk  | Low risk  | Low risk  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corvino, S.; Villanueva-Solórzano, P.L.; Offi, M.; Armocida, D.; Nonaka, M.; Iaconetta, G.; Esposito, F.; Cavallo, L.M.; de Notaris, M. A New Perspective on the Cavernous Sinus as Seen through Multiple Surgical Corridors: Anatomical Study Comparing the Transorbital, Endonasal, and Transcranial Routes and the Relative Coterminous Spatial Regions. Brain Sci. 2023, 13, 1215. https://doi.org/10.3390/brainsci13081215
Corvino S, Villanueva-Solórzano PL, Offi M, Armocida D, Nonaka M, Iaconetta G, Esposito F, Cavallo LM, de Notaris M. A New Perspective on the Cavernous Sinus as Seen through Multiple Surgical Corridors: Anatomical Study Comparing the Transorbital, Endonasal, and Transcranial Routes and the Relative Coterminous Spatial Regions. Brain Sciences. 2023; 13(8):1215. https://doi.org/10.3390/brainsci13081215
Chicago/Turabian StyleCorvino, Sergio, Pedro L. Villanueva-Solórzano, Martina Offi, Daniele Armocida, Motonobu Nonaka, Giorgio Iaconetta, Felice Esposito, Luigi Maria Cavallo, and Matteo de Notaris. 2023. "A New Perspective on the Cavernous Sinus as Seen through Multiple Surgical Corridors: Anatomical Study Comparing the Transorbital, Endonasal, and Transcranial Routes and the Relative Coterminous Spatial Regions" Brain Sciences 13, no. 8: 1215. https://doi.org/10.3390/brainsci13081215
APA StyleCorvino, S., Villanueva-Solórzano, P. L., Offi, M., Armocida, D., Nonaka, M., Iaconetta, G., Esposito, F., Cavallo, L. M., & de Notaris, M. (2023). A New Perspective on the Cavernous Sinus as Seen through Multiple Surgical Corridors: Anatomical Study Comparing the Transorbital, Endonasal, and Transcranial Routes and the Relative Coterminous Spatial Regions. Brain Sciences, 13(8), 1215. https://doi.org/10.3390/brainsci13081215