

Machine Learning Prediction of Estimated Risk for Bipolar Disorders Using Hippocampal Subfield and Amygdala Nuclei Volumes

 , , , , , , , , , , add
Show full author list
, , , , , , , , , , add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Pre-Registration
2.2. Sample
2.3. Risk Assessment Instruments
2.4. MRI Acquisition and Preprocessing
2.5. Measured Variables
2.6. Quality Control and Data Exclusion
2.7. Statistical Analysis
2.8. Machine Learning Analysis
3. Results
3.1. Demographics
3.2. Statistical Analysis
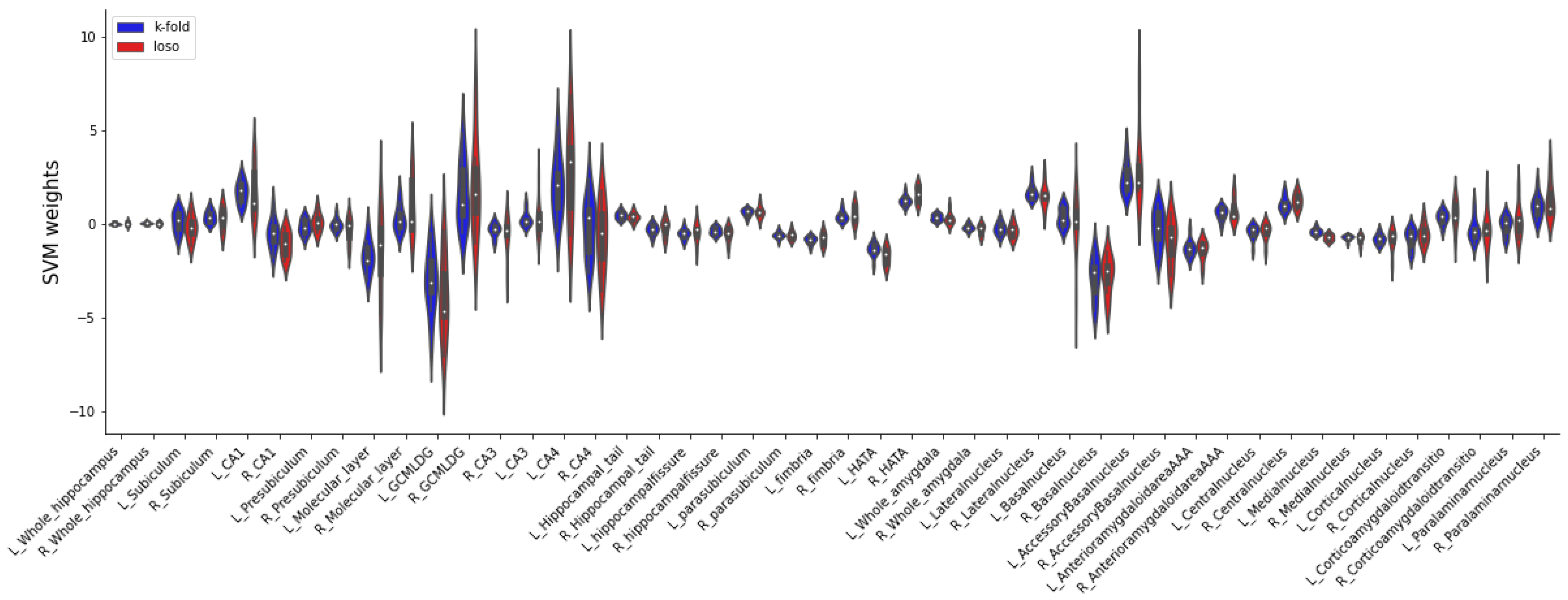
3.3. Machine Learning Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Inclusion and Exclusion Criteria for the Three Recruitment Pathways
- Youth and young adults consulting early recognition centres/facilities:
- Age: 15 to 35 years
- Consultation of an early recognition centre/facility
- Presence of at least one of the proposed risk factors for bipolar disorder: Family history of bipolar disorder, (sub)threshold affective symptomatology/depressive syndrome, hypomanic/mood swings, disturbances of circadian rhythm/sleep, other clinical hints
- Young individuals with diagnosed depression:
- Age: 15 to 35 years
- In- or outpatients with a depressive syndrome in the context of major depressive disorder, dysthymic disorder, cyclothymic disorder, minor depressive disorder, recurrent brief depressive disorder, adjustment disorder with depressed mood, depressive disorder Not Otherwise Specified (NOS)
- Patients with ADHD:
- Age: 15 to 35 years
- In- or outpatients with a clinically confirmed ADHD diagnosis
- Diagnosis of bipolar disorder, schizoaffective disorder, schizophrenia
- Diagnosis of anxiety, obsessive–compulsive or substance dependence disorder that fully explains the whole symptomatology
- Limited ability to comprehend the study
- Implied expressed negative declaration of intent to participate in the study by a minor and
- Acute suicidality
Appendix B

Appendix C

Appendix D


Appendix E

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BPSS-P | BARS | EPIbipolar | |
|---|---|---|---|
| Hippocampal subfields | |||
| CA1 | F(1, 258.392) = 0.015, p = 0. 984 | F(1, 253.719) = 0.418, p = 0.998 | F(2, 261.014) = 1.423, p = 0.581 |
| CA2/3 | F(1, 257.737) = 0.057, p = 0. 984 | F(1, 253.306) = 0.226, p = 0.998 | F(2, 260.560) = 0.531, p = 0.877 |
| CA4 | F(1, 256.403) = 0.002, p = 0. 984 | F(1, 252.530) = 0.133, p = 0.998 | F(2, 260.047) = 0.210, p = 0.896 |
| Molecular layer | F(1, 257.835) = 0.016, p = 0. 984 | F(1, 253.161) = 0.942, p = 0.998 | F(2, 260.538) = 1.143, p = 0.611 |
| GC ML DG | F(1, 256.400) = 0.044, p = 0. 984 | F(1, 252.529) = 0.115, p = 0.998 | F(2, 260.057) = 0.224, p = 0.896 |
| Hippocampal tail | F(1, 257.433) = 1.866, p = 0. 908 | F(1, 255.414) = 0.075, p = 0.998 | F(2, 262.303) = 1.186, p = 0.611 |
| Subiculum | F(1, 258.919) = 0.094, p = 0. 984 | F(1, 253.869) = 0.574, p = 0.998 | F(2, 261.239) = 0.712, p = 0.795 |
| Presubiculum | F(1, 258.126) = 0.146, p = 0. 984 | F(1, 252.960) = 0.994, p = 0.998 | F(2, 260.245) = 0.425, p = 0.877 |
| Parasubiculum | F(1, 252.592) = 0.131, p = 0. 984 | F(1, 254.835) = 0.095, p = 0.998 | F(2, 260.532) = 0.962, p = 0.672 |
| Fimbria | F(1, 238.399) = 0.184, p = 0. 984 | F(1, 256.843) = 0.844, p = 0.998 | F(2, 262.917) = 0.024, p = 0.976 |
| Hippocampal fissure | F(1, 258.786) = 2.610, p = 0. 749 | F(1, 254.065) = 0.001, p = 0.998 | F(2, 261.224) = 0.397, p = 0.877 |
| HATA | F(1, 259) = 1.138, p = 0. 984 | F(1, 254.478) = 0.000, p = 0.998 | F(2, 261.619) = 1.397, p = 0.581 |
| Nuclei of the amygdala | |||
| Cortical ncl. | F(1, 247.747) = 4.766, p = 0. 315 | F(1, 256.286) = 0.498, p = 0.998 | F(2, 262.740) = 2.239, p = 0.452 |
| Medial ncl. | F(1, 231.662) = 13.706, p = 0.0056 ** | F(1, 256.062) = 0.091, p = 0.998 | F(2, 262.792) = 0.089, p = 0.961 |
| Basal ncl. | F(1, 257.337) = 0.016, p = 0. 984 | F(1, 255.524) = 0.010, p = 0.998 | F(2, 262.493) = 2.233, p = 0.452 |
| Central ncl. | F(1, 259) = 0.500, p = 0. 984 | F(1, 257) = 0.014, p = 0.998 | F(2, 265) = 0.342, p = 0.877 |
| Lateral ncl. | F(1, 252.575) = 1.096, p = 0. 984 | F(1, 255.551) = 0.970, p = 0.998 | F(2, 262.244) = 4.214, p = 0.336 |
| Accessory basal ncl. | F(1, 249.097) = 0.004, p = 0. 984 | F(1, 256.320) = 0.003, p = 0.998 | F(2, 263.123) = 2.586, p = 0.452 |
| AAA | F(1, 233.022) = 0.000, p = 0. 984 | F(1, 256.675) = 0.648, p = 0.998 | F(2, 263.346) = 2.066, p = 0.452 |
| Corticoamygdaloid transition area | F(1, 247.829) = 0.009, p = 0. 984 | F(1, 255.937) = 0.010, p = 0.998 | F(2, 262.786) = 1.497, p = 0.581 |
| Paralaminar ncl. | F(1, 256.680) = 0.095, p = 0. 984 | F(1, 255.558) = 0.020, p = 0.998 | F(2, 262.455) = 2.375, p = 0.452 |
References
- Merikangas, K.R.; Jin, R.; He, J.-P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and Correlates of Bipolar Spectrum Disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Hu, C.; Ren, Z.; Bai, L.; Gao, F.; Lyu, J. Trends in the Incidence and DALYs of Bipolar Disorder at Global, Regional, and National Levels: Results from the Global Burden of Disease Study 2017. J. Psychiatr. Res. 2020, 125, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Drancourt, N.; Etain, B.; Lajnef, M.; Henry, C.; Raust, A.; Cochet, B.; Mathieu, F.; Gard, S.; MBailara, K.; Zanouy, L. Duration of Untreated Bipolar Disorder: Missed Opportunities on the Long Road to Optimal Treatment. Acta Psychiatr. Scand. 2013, 127, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Müller-Oerlinghausen, B.; Berghöfer, A.; Bauer, M. Bipolar Disorder. Lancet 2002, 359, 241–247. [Google Scholar] [CrossRef]
- Keramatian, K.; Chakrabarty, T.; Saraf, G.; Yatham, L. Transitioning to Bipolar Disorder: A Systematic Review of Prospective High-Risk Studies. Curr. Opin. Psychiatry, 2021; publish ahead of print. [Google Scholar] [CrossRef]
- Hajek, T.; Cullis, J.; Novak, T.; Kopecek, M.; Blagdon, R.; Propper, L.; Stopkova, P.; Duffy, A.; Hoschl, C.; Uher, R.; et al. Brain Structural Signature of Familial Predisposition for Bipolar Disorder: Replicable Evidence For Involvement of the Right Inferior Frontal Gyrus. Biol. Psychiatry 2013, 73, 144–152. [Google Scholar] [CrossRef]
- Kerner, B. Genetics of Bipolar Disorder. Appl. Clin. Genet. 2014, 7, 33–42. [Google Scholar] [CrossRef]
- Hafeman, D.M.; Merranko, J.; Goldstein, T.R.; Axelson, D.; Goldstein, B.I.; Monk, K.; Hickey, M.B.; Sakolsky, D.; Diler, R.; Iyengar, S.; et al. Assessment of a Person-Level Risk Calculator to Predict New-Onset Bipolar Spectrum Disorder in Youth at Familial Risk. JAMA Psychiatry 2017, 74, 841–847. [Google Scholar] [CrossRef]
- Post, R.M.; Altshuler, L.L.; Kupka, R.; McElroy, S.L.; Frye, M.A.; Rowe, M.; Grunze, H.; Suppes, T.; Keck, P.E.; Leverich, G.S.; et al. Multigenerational Transmission of Liability to Psychiatric Illness in Offspring of Parents with Bipolar Disorder. Bipolar Disord. 2018, 20, 432–440. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; De Micheli, A.; Rocchetti, M.; Cappucciati, M.; Ramella-Cravaro, V.; Rutigliano, G.; Bonoldi, I.; McGuire, P.; Falkenberg, I. Semistructured Interview for Bipolar at Risk States (SIBARS). Psychiatry Res. 2018, 264, 302–309. [Google Scholar] [CrossRef]
- Leopold, K.; Ritter, P.; Correll, C.U.; Marx, C.; Özgürdal, S.; Juckel, G.; Bauer, M.; Pfennig, A. Risk Constellations Prior to the Development of Bipolar Disorders: Rationale of a New Risk Assessment Tool. J. Affect. Disord. 2012, 136, 1000–1010. [Google Scholar] [CrossRef]
- Correll, C.U.; Olvet, D.M.; Auther, A.M.; Hauser, M.; Kishimoto, T.; Carrión, R.E.; Snyder, S.; Cornblatt, B.A. The Bipolar Prodrome Symptom Interview and Scale–Prospective (BPSS-P): Description and Validation in a Psychiatric Sample and Healthy Controls. Bipolar Disord. 2014, 16, 505–522. [Google Scholar] [CrossRef]
- Dwyer, D.B.; Falkai, P.; Koutsouleris, N. Machine Learning Approaches for Clinical Psychology and Psychiatry. Ann. Rev. Clin. Psychol. 2018, 14, 91–118. [Google Scholar] [CrossRef]
- Koutsouleris, N.; Dwyer, D.B.; Degenhardt, F.; Maj, C.; Urquijo-Castro, M.F.; Sanfelici, R.; Popovic, D.; Oeztuerk, O.; Haas, S.S.; Weiske, J.; et al. Multimodal Machine Learning Workflows for Prediction of Psychosis in Patients With Clinical High-Risk Syndromes and Recent-Onset Depression. JAMA Psychiatry 2021, 78, 195–209. [Google Scholar] [CrossRef]
- Arnone, D.; Cavanagh, J.; Gerber, D.; Lawrie, S.M.; Ebmeier, K.P.; McIntosh, A.M. Magnetic Resonance Imaging Studies in Bipolar Disorder and Schizophrenia: Meta-Analysis. Br. J. Psychiatry 2009, 195, 194–201. [Google Scholar] [CrossRef]
- Hibar, D.P.; Westlye, L.T.; Doan, N.T.; Jahanshad, N.; Cheung, J.W.; Ching, C.R.K.; Versace, A.; Bilderbeck, A.C.; Uhlmann, A.; Mwangi, B.; et al. Cortical Abnormalities in Bipolar Disorder: An MRI Analysis of 6503 Individuals from the ENIGMA Bipolar Disorder Working Group. Mol. Psychiatry 2018, 23, 932–942. [Google Scholar] [CrossRef]
- Hibar, D.P.; Westlye, L.T.; van Erp, T.G.M.; Rasmussen, J.; Leonardo, C.D.; Faskowitz, J.; Haukvik, U.K.; Hartberg, C.B.; Doan, N.T.; Agartz, I.; et al. Subcortical Volumetric Abnormalities in Bipolar Disorder. Mol. Psychiatry 2016, 21, 1710–1716. [Google Scholar] [CrossRef]
- Haukvik, U.K.; Gurholt, T.P.; Nerland, S.; Elvsåshagen, T.; Akudjedu, T.N.; Alda, M.; Alnæs, D.; Alonso-Lana, S.; Bauer, J.; Baune, B.T. In Vivo Hippocampal Subfield Volumes in Bipolar Disorder—A Mega-analysis from The Enhancing Neuro Imaging Genetics through Meta-Analysis Bipolar Disorder Working Group. Hum. Brain Mapp. 2022, 43, 385–398. [Google Scholar] [CrossRef]
- Haukvik, U.K.; Westlye, L.T.; Mørch-Johnsen, L.; Jørgensen, K.N.; Lange, E.H.; Dale, A.M.; Melle, I.; Andreassen, O.A.; Agartz, I. In Vivo Hippocampal Subfield Volumes in Schizophrenia and Bipolar Disorder. Biol. Psychiatry 2015, 77, 581–588. [Google Scholar] [CrossRef]
- Mathew, I.; Gardin, T.M.; Tandon, N.; Eack, S.; Francis, A.N.; Seidman, L.J.; Clementz, B.; Pearlson, G.D.; Sweeney, J.A.; Tamminga, C.A. Medial Temporal Lobe Structures and Hippocampal Subfields in Psychotic Disorders: Findings from the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP) Study. JAMA Psychiatry 2014, 71, 769–777. [Google Scholar] [CrossRef]
- Heller, A.S. Cortical-Subcortical Interactions in Depression: From Animal Models to Human Psychopathology. Front. Syst. Neurosci. 2016, 10, 20. [Google Scholar] [CrossRef]
- Nikolenko, V.N.; Oganesyan, M.V.; Rizaeva, N.A.; Kudryashova, V.A.; Nikitina, A.T.; Pavliv, M.P.; Shchedrina, M.A.; Giller, D.B.; Bulygin, K.V.; Sinelnikov, M.Y. Amygdala: Neuroanatomical and Morphophysiological Features in Terms of Neurological and Neurodegenerative Diseases. Brain Sci. 2020, 10, 502. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.; Nerland, S.; de Lange, A.-M.G.; Wortinger, L.A.; Hilland, E.; Andreassen, O.A.; Jørgensen, K.N.; Agartz, I. In Vivo Amygdala Nuclei Volumes in Schizophrenia and Bipolar Disorders. Schizophr. Bull. 2021, 47, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Bielau, H.; Trübner, K.; Krell, D.; Agelink, M.W.; Bernstein, H.-G.; Stauch, R.; Mawrin, C.; Danos, P.; Gerhard, L.; Bogerts, B. Volume Deficits of Subcortical Nuclei in Mood Disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2005, 255, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Rey, G.; Bolton, T.A.W.; Gaviria, J.; Piguet, C.; Preti, M.G.; Favre, S.; Aubry, J.-M.; Van De Ville, D.; Vuilleumier, P. Dynamics of Amygdala Connectivity in Bipolar Disorders: A Longitudinal Study across Mood States. Neuropsychopharmacology 2021, 46, 1693–1701. [Google Scholar] [CrossRef]
- Piguet, C.; Karahanoğlu, F.I.; Saccaro, L.F.; Van De Ville, D.; Vuilleumier, P. Mood Disorders Disrupt the Functional Dynamics, Not Spatial Organization of Brain Resting State Networks. NeuroImage Clin. 2021, 32, 102833. [Google Scholar] [CrossRef]
- Chen, C.-H.; Suckling, J.; Lennox, B.R.; Ooi, C.; Bullmore, E.T. A Quantitative Meta-Analysis of FMRI Studies in Bipolar Disorder: Meta-Analysis of FMRI Studies in BD. Bipolar Disord. 2011, 13, 1–15. [Google Scholar] [CrossRef]
- Saccaro, L.F.; Gaviria, J.; Ville, D.V.D.; Piguet, C. Dynamic Functional Hippocampal Markers of Residual Depressive Symptoms in Euthymic Bipolar Disorder. Brain Behav. 2023, e3010. [Google Scholar] [CrossRef]
- Luders, E.; Thompson, P.M.; Kurth, F.; Hong, J.-Y.; Phillips, O.R.; Wang, Y.; Gutman, B.A.; Chou, Y.-Y.; Narr, K.L.; Toga, A.W. Global and Regional Alterations of Hippocampal Anatomy in Long-term Meditation Practitioners. Hum. Brain Mapp. 2013, 34, 3369–3375. [Google Scholar] [CrossRef]
- Sani, G.; Simonetti, A.; Janiri, D.; Banaj, N.; Ambrosi, E.; De Rossi, P.; Ciullo, V.; Arciniegas, D.B.; Piras, F.; Spalletta, G. Association between Duration of Lithium Exposure and Hippocampus/Amygdala Volumes in Type I Bipolar Disorder. J. Affect. Disord. 2018, 232, 341–348. [Google Scholar] [CrossRef]
- Roeder, S.S.; Burkardt, P.; Rost, F.; Rode, J.; Brusch, L.; Coras, R.; Englund, E.; Håkansson, K.; Possnert, G.; Salehpour, M.; et al. Evidence for Postnatal Neurogenesis in the Human Amygdala. Commun. Biol. 2022, 5, 366. [Google Scholar] [CrossRef]
- Lucassen, P.J.; Oomen, C.A.; Naninck, E.F.G.; Fitzsimons, C.P.; Van Dam, A.-M.; Czeh, B.; Korosi, A. Regulation of Adult Neurogenesis and Plasticity by (Early) Stress, Glucocorticoids, and Inflammation. Cold Spring Harb. Perspect. Biol. 2015, 7, a021303. [Google Scholar] [CrossRef]
- Saccaro, L.F.; Schilliger, Z.; Dayer, A.; Perroud, N.; Piguet, C. Inflammation, Anxiety, and Stress in Bipolar Disorder and Borderline Personality Disorder: A Narrative Review. Neurosci. Biobehav. Rev. 2021, 127, 184–192. [Google Scholar] [CrossRef]
- Orru, G.; Pettersson-Yeo, W.; Marquand, A.F.; Sartori, G.; Mechelli, A. Using Support Vector Machine to Identify Imaging Biomarkers of Neurological and Psychiatric Disease: A Critical Review. Neurosci. Biobehav. Rev. 2012, 36, 1140–1152. [Google Scholar] [CrossRef]
- Mikolas, P.; Marxen, M.; Riedel, P.; Bröckel, K.; Martini, J.; Huth, F.; Berndt, C.; Vogelbacher, C.; Jansesn, A.; Kircher, T.; et al. Prediction of Estimated Risk for Bipolar Disorder Using Machine Learning and Structural MRI Features. Psychol. Med. 2023, 1–11. [Google Scholar] [CrossRef]
- Garg, A.; Mago, V. Role of Machine Learning in Medical Research: A Survey. Comput. Sci. Rev. 2021, 40, 100370. [Google Scholar] [CrossRef]
- Pfennig, A.; Leopold, K.; Martini, J.; Boehme, A.; Lambert, M.; Stamm, T.; Bermpohl, F.; Reif, A.; Kittel-Schneider, S.; Juckel, G. Improving Early Recognition and Intervention in People at Increased Risk for the Development of Bipolar Disorder: Study Protocol of a Prospective-Longitudinal, Naturalistic Cohort Study (Early-BipoLife). Int. J. Bipolar Disord. 2020, 8, 22. [Google Scholar] [CrossRef]
- Ritter, P.S.; Bermpohl, F.; Gruber, O.; Hautzinger, M.; Jansen, A.; Juckel, G.; Kircher, T.; Lambert, M.; Mulert, C.; Pfennig, A. Aims and Structure of the German Research Consortium BipoLife for the Study of Bipolar Disorder. Int. J. Bipolar Disord. 2016, 4, 26. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef]
- Pfennig, A.; Jabs, B.; Pfeiffer, S.; Weikert, B.; Leopold, K.; Bauer, M. Health care service experiences of bipolar patients in Germany survey prior to the introduction of the S3 Guideline for diagnostics and treatment of bipolar disorders. Nervenheilkunde 2011, 30, 333–340. [Google Scholar] [CrossRef]
- Lambert, M.; Bock, T.; Naber, D.; Löwe, B.; Schulte-Markwort, M.; Schäfer, I.; Gumz, A.; Degkwitz, P.; Schulte, B.; König, H.; et al. Die psychische Gesundheit von Kindern, Jugendlichen und jungen Erwachsenen—Teil 1: Häufigkeit, Störungspersistenz, Belastungsfaktoren, Service-Inanspruchnahme und Behandlungsverzögerung mit Konsequenzen. Fortschr. Neurol. Psychiatr. 2013, 81, 614–627. [Google Scholar] [CrossRef]
- Mikolas, P.; Bröckel, K.; Vogelbacher, C.; Müller, D.K.; Marxen, M.; Berndt, C.; Sauer, C.; Jung, S.; Fröhner, J.H.; Fallgatter, A.J.; et al. Individuals at Increased Risk for Development of Bipolar Disorder Display Structural Alterations Similar to People with Manifest Disease. Transl. Psychiatry 2021, 11, 485. [Google Scholar] [CrossRef] [PubMed]
- Vogelbacher, C.; Sommer, J.; Schuster, V.; Bopp, M.H.; Falkenberg, I.; Ritter, P.S.; Bermpohl, F.; Hindi Attar, C.; Rauer, L.; Einenkel, K.E. The German Research Consortium for the Study of Bipolar Disorder (BipoLife): A Magnetic Resonance Imaging Study Protocol. Int. J. Bipolar Disord. 2021, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Salat, D.H.; van der Kouwe, A.J.W.; Makris, N.; Ségonne, F.; Quinn, B.T.; Dale, A.M. Sequence-Independent Segmentation of Magnetic Resonance Images. Neuroimage 2004, 23, S69–S84. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Sereno, M.I.; Tootell, R.B.H.; Dale, A.M. High-Resolution Intersubject Averaging and a Coordinate System for the Cortical Surface. Hum. Brain Mapp. 1999, 8, 272–284. [Google Scholar] [CrossRef]
- Iglesias, J.E.; Augustinack, J.C.; Nguyen, K.; Player, C.M.; Player, A.; Wright, M.; Roy, N.; Frosch, M.P.; McKee, A.C.; Wald, L.L. A Computational Atlas of the Hippocampal Formation Using Ex Vivo, Ultra-High Resolution MRI: Application to Adaptive Segmentation of in Vivo MRI. Neuroimage 2015, 115, 117–137. [Google Scholar] [CrossRef]
- Saygin, Z.M.; Kliemann, D.; Iglesias, J.E.; van der Kouwe, A.J.; Boyd, E.; Reuter, M.; Stevens, A.; Van Leemput, K.; McKee, A.; Frosch, M.P. High-Resolution Magnetic Resonance Imaging Reveals Nuclei of the Human Amygdala: Manual Segmentation to Automatic Atlas. Neuroimage 2017, 155, 370–382. [Google Scholar] [CrossRef]
- Iglesias, J.E.; Van Leemput, K.; Augustinack, J.; Insausti, R.; Fischl, B.; Reuter, M.; Initiative, A.D.N. Bayesian Longitudinal Segmentation of Hippocampal Substructures in Brain MRI Using Subject-Specific Atlases. Neuroimage 2016, 141, 542–555. [Google Scholar] [CrossRef]
- Van Leemput, K.; Bakkour, A.; Benner, T.; Wiggins, G.; Wald, L.L.; Augustinack, J.; Dickerson, B.C.; Golland, P.; Fischl, B. Automated Segmentation of Hippocampal Subfields from Ultra-High Resolution in Vivo MRI. Hippocampus 2009, 19, 549–557. [Google Scholar] [CrossRef]
- Sämann, P.G.; Iglesias, J.E.; Gutman, B.; Grotegerd, D.; Leenings, R.; Flint, C.; Dannlowski, U.; Clarke-Rubright, E.K.; Morey, R.A.; Erp, T.G.M.; et al. FreeSurfer -based Segmentation of Hippocampal Subfields: A Review of Methods and Applications, with a Novel Quality Control Procedure for ENIGMA Studies and Other Collaborative Efforts. Hum. Brain Mapp. 2022, 43, 207–233. [Google Scholar] [CrossRef]
- Tesli, N.; van der Meer, D.; Rokicki, J.; Storvestre, G.; Røsæg, C.; Jensen, A.; Hjell, G.; Bell, C.; Fischer-Vieler, T.; Tesli, M.; et al. Hippocampal Subfield and Amygdala Nuclei Volumes in Schizophrenia Patients with a History of Violence. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 771–782. [Google Scholar] [CrossRef]
- Yücel, M.; Lorenzetti, V.; Suo, C.; Zalesky, A.; Fornito, A.; Takagi, M.J.; Lubman, D.I.; Solowij, N. Hippocampal Harms, Protection and Recovery Following Regular Cannabis Use. Transl. Psychiatry 2016, 6, e710. [Google Scholar] [CrossRef]
- Tozzi, L.; Garczarek, L.; Janowitz, D.; Stein, D.J.; Wittfeld, K.; Dobrowolny, H.; Lagopoulos, J.; Hatton, S.N.; Hickie, I.B.; Carballedo, A.; et al. Interactive Impact of Childhood Maltreatment, Depression, and Age on Cortical Brain Structure: Mega-Analytic Findings from a Large Multi-Site Cohort. Psychol. Med. 2020, 50, 1020–1031. [Google Scholar] [CrossRef]
- Mikolas, P.; Tozzi, L.; Doolin, K.; Farrell, C.; O’Keane, V.; Frodl, T. Effects of Early Life Adversity and FKBP5 Genotype on Hippocampal Subfields Volume in Major Depression. J. Affect. Disord. 2019, 252, 152–159. [Google Scholar] [CrossRef]
- Twait, E.L.; Blom, K.; Koek, H.L.; Zwartbol, M.H.T.; Ghaznawi, R.; Hendrikse, J.; Gerritsen, L.; Geerlings, M.I. UCC SMART Study Group Psychosocial Factors and Hippocampal Subfields: The Medea-7T Study. Hum. Brain Mapp. 2022, 44, 1964–1984. [Google Scholar] [CrossRef]
- Tozzi, L.; Farrell, C.; Booij, L.; Doolin, K.; Nemoda, Z.; Szyf, M.; Pomares, F.B.; Chiarella, J.; O’Keane, V.; Frodl, T. Epigenetic Changes of FKBP5 as a Link Connecting Genetic and Environmental Risk Factors with Structural and Functional Brain Changes in Major Depression. Neuropsychopharmacology 2018, 43, 1138–1145. [Google Scholar] [CrossRef]
- Klinitzke, G.; Romppel, M.; Häuser, W.; Brähler, E.; Glaesmer, H. The German Version of the Childhood Trauma Questionnaire (CTQ): Psychometric Characteristics in a Representative Sample of the General Population. Psychother. Psychosom. Med. Psychol. 2011, 62, 47–51. [Google Scholar]
- Esteban, O.; Birman, D.; Schaer, M.; Koyejo, O.O.; Poldrack, R.A.; Gorgolewski, K.J. MRIQC: Advancing the Automatic Prediction of Image Quality in MRI from Unseen Sites. PLoS ONE 2017, 12, e0184661. [Google Scholar] [CrossRef]
- Fjell, A.M.; Westlye, L.T.; Grydeland, H.; Amlien, I.; Espeseth, T.; Reinvang, I.; Raz, N.; Holland, D.; Dale, A.M.; Walhovd, K.B. Critical Ages in the Life Course of the Adult Brain: Nonlinear Subcortical Aging. Neurobiol. Aging 2013, 34, 2239–2247. [Google Scholar] [CrossRef]
- van Eijk, L.; Hansell, N.K.; Strike, L.T.; Couvy-Duchesne, B.; de Zubicaray, G.I.; Thompson, P.M.; McMahon, K.L.; Zietsch, B.P.; Wright, M.J. Region-Specific Sex Differences in the Hippocampus. Neuroimage 2020, 215, 116781. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Nunes, A.; Schnack, H.G.; Ching, C.R.K.; Agartz, I.; Akudjedu, T.N.; Alda, M.; Alnæs, D.; Alonso-Lana, S.; Bauer, J.; Baune, B.T.; et al. Using Structural MRI to Identify Bipolar Disorders—13 Site Machine Learning Study in 3020 Individuals from the ENIGMA Bipolar Disorders Working Group. Mol. Psychiatry 2020, 25, 2130–2143. [Google Scholar] [CrossRef] [PubMed]
- Ching, C.R.K.; Hibar, D.P.; Gurholt, T.P.; Nunes, A.; Thomopoulos, S.I.; Abé, C.; Agartz, I.; Brouwer, R.M.; Cannon, D.M.; Zwarte, S.M.C.; et al. What We Learn about Bipolar Disorder from Large-scale Neuroimaging: Findings and Future Directions from the ENIGMA Bipolar Disorder Working Group. Hum. Brain Mapp. 2020, 43, 56–82. [Google Scholar] [CrossRef] [PubMed]
- Lemm, S.; Blankertz, B.; Dickhaus, T.; Müller, K.-R. Introduction to Machine Learning for Brain Imaging. NeuroImage 2011, 56, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-Sampling Technique. JAIR 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Blumberg, H.P.; Kaufman, J.; Martin, A.; Whiteman, R.; Zhang, J.H.; Gore, J.C.; Charney, D.S.; Krystal, J.H.; Peterson, B.S. Amygdala and Hippocampal Volumes in Adolescents and Adults with Bipolar Disorder. Arch. Gen. Psychiatry 2003, 60, 1201–1208. [Google Scholar] [CrossRef]
- Cattarinussi, G.; Di Giorgio, A.; Wolf, R.C.; Balestrieri, M.; Sambataro, F. Neural Signatures of the Risk for Bipolar Disorder: A Meta-analysis of Structural and Functional Neuroimaging Studies. Bipolar Disord. 2019, 21, 215–227. [Google Scholar] [CrossRef]
- Pereira, F.; Mitchell, T.; Botvinick, M. Machine Learning Classifiers and FMRI: A Tutorial Overview. Neuroimage 2009, 45, S199–S209. [Google Scholar] [CrossRef]
- Claude, L.; Houenou, J.; Duchesnay, E.; Favre, P. Will Machine Learning Applied to Neuroimaging in Bipolar Disorder Help the Clinician? A Critical Review and Methodological Suggestions. Bipolar Disord. 2020, 22, 334–355. [Google Scholar] [CrossRef]
- Nieuwenhuis, M.; van Haren, N.E.M.; Hulshoff Pol, H.E.; Cahn, W.; Kahn, R.S.; Schnack, H.G. Classification of Schizophrenia Patients and Healthy Controls from Structural MRI Scans in Two Large Independent Samples. Neuroimage 2012, 61, 606–612. [Google Scholar] [CrossRef]
- Lupien, S.J.; Juster, R.-P.; Raymond, C.; Marin, M.-F. The Effects of Chronic Stress on the Human Brain: From Neurotoxicity, to Vulnerability, to Opportunity. Front. Neuroendocrinol. 2018, 49, 91–105. [Google Scholar] [CrossRef]
- Logtenberg, E.; Overbeek, M.F.; Pasman, J.A.; Abdellaoui, A.; Luijten, M.; van Holst, R.J.; Vink, J.M.; Denys, D.; Medland, S.E.; Verweij, K.J.H.; et al. Investigating the Causal Nature of the Relationship of Subcortical Brain Volume with Smoking and Alcohol Use. Br. J. Psychiatry 2022, 221, 377–385. [Google Scholar] [CrossRef]
- Hayano, F.; Nakamura, M.; Asami, T.; Uehara, K.; Yoshida, T.; Roppongi, T.; Otsuka, T.; Inoue, T.; Hirayasu, Y. Smaller Amygdala Is Associated with Anxiety in Patients with Panic Disorder. Psychiatry Clin. Neurosci. 2009, 63, 266–276. [Google Scholar] [CrossRef]
- Sala, M.; Perez, J.; Soloff, P.; Di Nemi, S.U.; Caverzasi, E.; Soares, J.C.; Brambilla, P. Stress and Hippocampal Abnormalities in Psychiatric Disorders. Eur. Neuropsychopharmacol. 2004, 14, 393–405. [Google Scholar] [CrossRef]

| Main Output | Hippocampal Subfields | Nuclei of the Amygdala |
|---|---|---|
| Hippocampus (total volume) Amygdala (total volume) Intracranial volume (ICV) | Hippocampal tail Subiculum Hippocampal fissure Presubiculum Parasubiculum Molecular Layer Granule cell layer of the dentate gyrus (GC ML DG) CA1 CA2/3 CA4 Fimbria Hippocampal amygdala transition area (HATA) | Lateral nucleus Basal nucleus Central nucleus Medial nucleus Cortical nucleus Accessory basal nucleus Paralaminar nucleus Corticoamygdaloid transition area Anterior amygdaloid area |
| Risk Assessment Instrument | BPSS-P (n = 264) | BARS (n = 262) | ||||
|---|---|---|---|---|---|---|
| Risk criterion fulfilled | No | Yes | Test | No | Yes | Test |
| n (%) | 205 (77.7) | 59 (22.3) | n/a | 74 (28.2) | 188 (71.8) | |
| Female (%) | 93 (45.4) | 34 (57.6) | χ2 = 2.759, p = 0.097 | 35 (47.3) | 91 (48.4) | χ2 = 0.026, p = 0.872 |
| Age (SD) | 24.88 (4.2) | 24.54 (4.7) | t = −0.532, df = 262, p = 0.595 | 24.39 (3.7) | 25.03 (4.6) | t = 1.075, df = 260, p = 0.283 |
| Education high school (%) | 165 (80.5) | 41 (69.5) | χ2 = 3.232, p = 0.072 | 62 (83.8) | 142 (75.5) | χ2 = 2.098, p = 0.148 |
| Recruitment pathway | ||||||
| Early recognition (%) | 91 (44.4) | 20 (33.9) | χ2 = 2.076, p = 0.354 | 35 (47.3) | 77 (41.0) | |
| Depression (%) | 87 (42.4) | 30 (50.8) | 23 (31.1) | 91 (48.4) | χ2 = 8.823, p = 0.012 * | |
| ADHD (%) | 27 (13.2) | 9 (15.3) | 16 (21.6) | 20 (10.6) | ||
| Psychiatric Medication | ||||||
| Yes (%) | 111 (54.1) | 39 (66.1) | χ2 = 2.669, p = 0.102 | 34 (45.9) | 115 (61.2) | χ2 = 5.018, p = 0.025 * |
| Substance Use | ||||||
Smoking status
| 97 (47.3) 94 (45.9) 14 (6.8) | 20 (33.9) 31 (52.5) 8 (13.6) | χ2 = 4.784, p = 0.091 | 42 (56.8) 27 (36.5) 5 (6.8) | 74 (39.4) 95 (50.5) 19 (10.1) | χ2 = 6.529, p = 0.038 * |
Cannabis present
| 147 (71.7) 17 (8.3) 12 (5.9) 15 (7.3) 14 (6.8) | 45 (76.3) 3 (5.1) 2 (3.4) 2 (3.4) 7 (11.9) | χ2 = 3.836, p = 0.429 | 61 (82.4) 4 (5.4) 3 (4.1) 3 (4.1) 3 (4.1) | 129 (68.6) 16 (8.5) 11 (5.9) 14 (7.4) 18 (9.6) | χ2 = 5.350, p = 0.253 |
Cannabis lifetime
| 84 (41.0) 46 (22.4) 9 (4.4) 24 (11.7) 42 (20.5) | 23 (39.0) 11 (18.6) 2 (3.4) 6 (10.2) 17 (28.8) | χ2 = 1.977, p = 0.740 | 38 (51.4) 16 (21.6) 2 (2.7) 7 (9.5) 11 (14.9) | 68 (36.2) 40 (21.3) 9 (4.8) 24 (12.8) 47 (25.0) | χ2 = 6.532, p = 0.163 |
| Risk Assessment Instrument | EPIbipolar (n = 271) | |||
|---|---|---|---|---|
| Risk criterion fulfilled | No-risk | Low-risk | High-risk | Test |
| n (%) | 30 (11.1) | 136 (50.2) | 105 (38.7) | n/a |
| Female (%) | 10 (33.3) | 62 (45.6) | 57 (54.3) | χ2 = 4.550, p = 0.103 |
| Age (SD) | 24.13 (3.03) | 25.40 (4.61) | 25.02 (4.34) | F = 0.570, df = 2, p = 0.566 |
| Education high school (%) | 24 (80.0) | 107 (78.7) | 81 (77.1) | χ2 = 0.144, p = 0.931 |
| Recruitment pathway | ||||
| Early recognition (%) | 14 (46.7) | 50 (36.8) | 51 (48.6) | χ2 = 23.707, p < 0.001 ** |
| Depression (%) | 5 (16.7) | 72 (52.9) | 43 (41.0) | |
| ADHD (%) | 11 (36.7) | 14 (10.3) | 11 (10.5) | |
| Psychiatric Medication | ||||
| Yes (%) | 11 (36.7) | 87 (64.0) | 57 (54.3) | χ2 = 8.077, p = 0.018 * |
| Substance Use | ||||
Smoking status
| 16 (53.3) 9 (30.0) 5 (16.7) | 64 (47.1) 64 (47.1) 8 (5.9) | 38 (36.2) 56 (53.3) 11 (10.5) | χ2 = 8.771, p = 0.067 |
Cannabis present
| 25 (83.3) 1 (3.3) 0 (0.0) 2 (6.7) 2 (6.7) | 96 (70.6) 11 (8.1) 8 (5.9) 8 (5.9) 13 (9.6) | 76 (72.4) 10 (9.5) 6 (5.7) 7 (6.7) 6 (5.7) | χ2 = 4.647, p = 0.795 |
Cannabis lifetime
| 14 (46.7) 8 (26.7) 0 (0.0) 3 (10.0) 5 (16.7) | 52 (38.2) 29 (21.3) 6 (4.4) 17 (12.5) 32 (23.5) | 44 (41.9) 21 (20.0) 5 (4.8) 11 (10.5) 24 (22.9) | χ2 = 3.173, p = 0.923 |
| Cohen’s Kappa (%) | Balanced Accuracy (%) | Sensitivity (%) | Specificity (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95% CI | 95% CI | 95% CI | 95% CI | |||||||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | |||||
| BPSS-P | ||||||||||||
| 10-fold | 0.275 | 0.149 | 0.401 | 66.9 | 59.2 | 74.6 | 63.0 | 49.7 | 76.3 | 63.0 | 49.7 | 76.3 |
| Leave-one-site-out | 0.197 | 0.033 | 0.361 | 61.9 | 52.0 | 71.9 | 45.0 | 17.7 | 72.2 | 78.9 | 60.2 | 97.7 |
| BARS | ||||||||||||
| 10-fold | −0.001 | −0.132 | 0.129 | 49.2 | 41.9 | 56.5 | 56.2 | 44.2 | 68.3 | 42.1 | 35.7 | 48.5 |
| Leave-one-site-out | −0.000 | −0.103 | 0.103 | 48.2 | 40.1 | 56.2 | 53.8 | 41.9 | 65.7 | 42.5 | 30.7 | 54.4 |
| EPIbipolar | ||||||||||||
| 10-fold | −0.049 | −0.143 | 0.045 | 45.0 | 35.3 | 54.8 | 66.8 | 58.0 | 75.5 | 23.3 | 7.2 | 39.4 |
| Leave-one-site-out | −0.027 | −0.203 | 0.148 | 46.2 | 35.6 | 56.8 | 62.4 | 44.4 | 80.5 | 30.0 | 15.2 | 44.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huth, F.; Tozzi, L.; Marxen, M.; Riedel, P.; Bröckel, K.; Martini, J.; Berndt, C.; Sauer, C.; Vogelbacher, C.; Jansen, A.; et al. Machine Learning Prediction of Estimated Risk for Bipolar Disorders Using Hippocampal Subfield and Amygdala Nuclei Volumes. Brain Sci. 2023, 13, 870. https://doi.org/10.3390/brainsci13060870
Huth F, Tozzi L, Marxen M, Riedel P, Bröckel K, Martini J, Berndt C, Sauer C, Vogelbacher C, Jansen A, et al. Machine Learning Prediction of Estimated Risk for Bipolar Disorders Using Hippocampal Subfield and Amygdala Nuclei Volumes. Brain Sciences. 2023; 13(6):870. https://doi.org/10.3390/brainsci13060870
Chicago/Turabian StyleHuth, Fabian, Leonardo Tozzi, Michael Marxen, Philipp Riedel, Kyra Bröckel, Julia Martini, Christina Berndt, Cathrin Sauer, Christoph Vogelbacher, Andreas Jansen, and et al. 2023. "Machine Learning Prediction of Estimated Risk for Bipolar Disorders Using Hippocampal Subfield and Amygdala Nuclei Volumes" Brain Sciences 13, no. 6: 870. https://doi.org/10.3390/brainsci13060870
APA StyleHuth, F., Tozzi, L., Marxen, M., Riedel, P., Bröckel, K., Martini, J., Berndt, C., Sauer, C., Vogelbacher, C., Jansen, A., Kircher, T., Falkenberg, I., Thomas-Odenthal, F., Lambert, M., Kraft, V., Leicht, G., Mulert, C., Fallgatter, A. J., Ethofer, T., ... Mikolas, P. (2023). Machine Learning Prediction of Estimated Risk for Bipolar Disorders Using Hippocampal Subfield and Amygdala Nuclei Volumes. Brain Sciences, 13(6), 870. https://doi.org/10.3390/brainsci13060870