
Tolerability and Effectiveness of Cathodal Transcranial Direct Current Stimulation in Children with Refractory Epilepsy: A Case Series

Abstract
1. Introduction
2. Material and Methods
2.1. tDCS
2.2. Outcome Measures
2.3. EEG
2.4. Statistical Analysis
3. Results
3.1. Stimulus Parameters
3.2. Outcomes
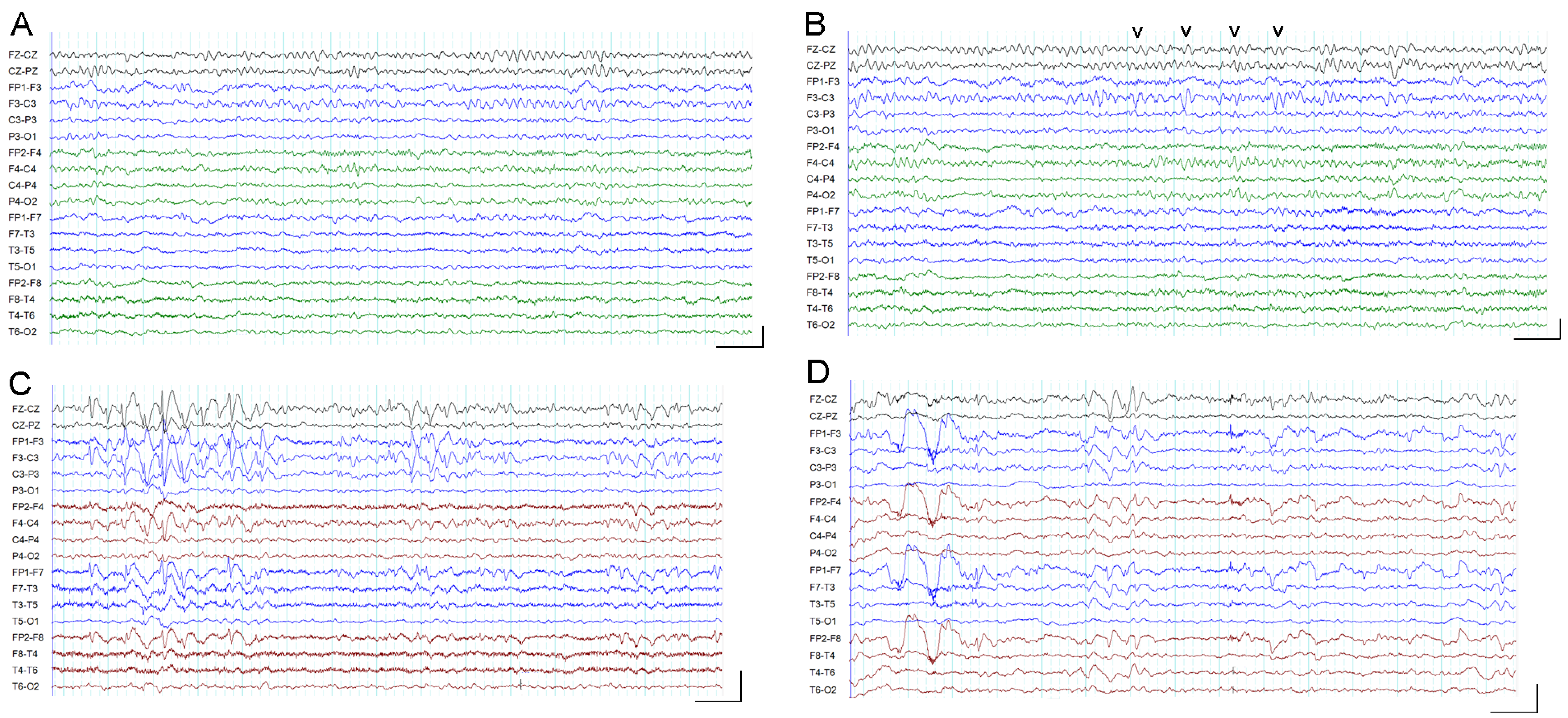
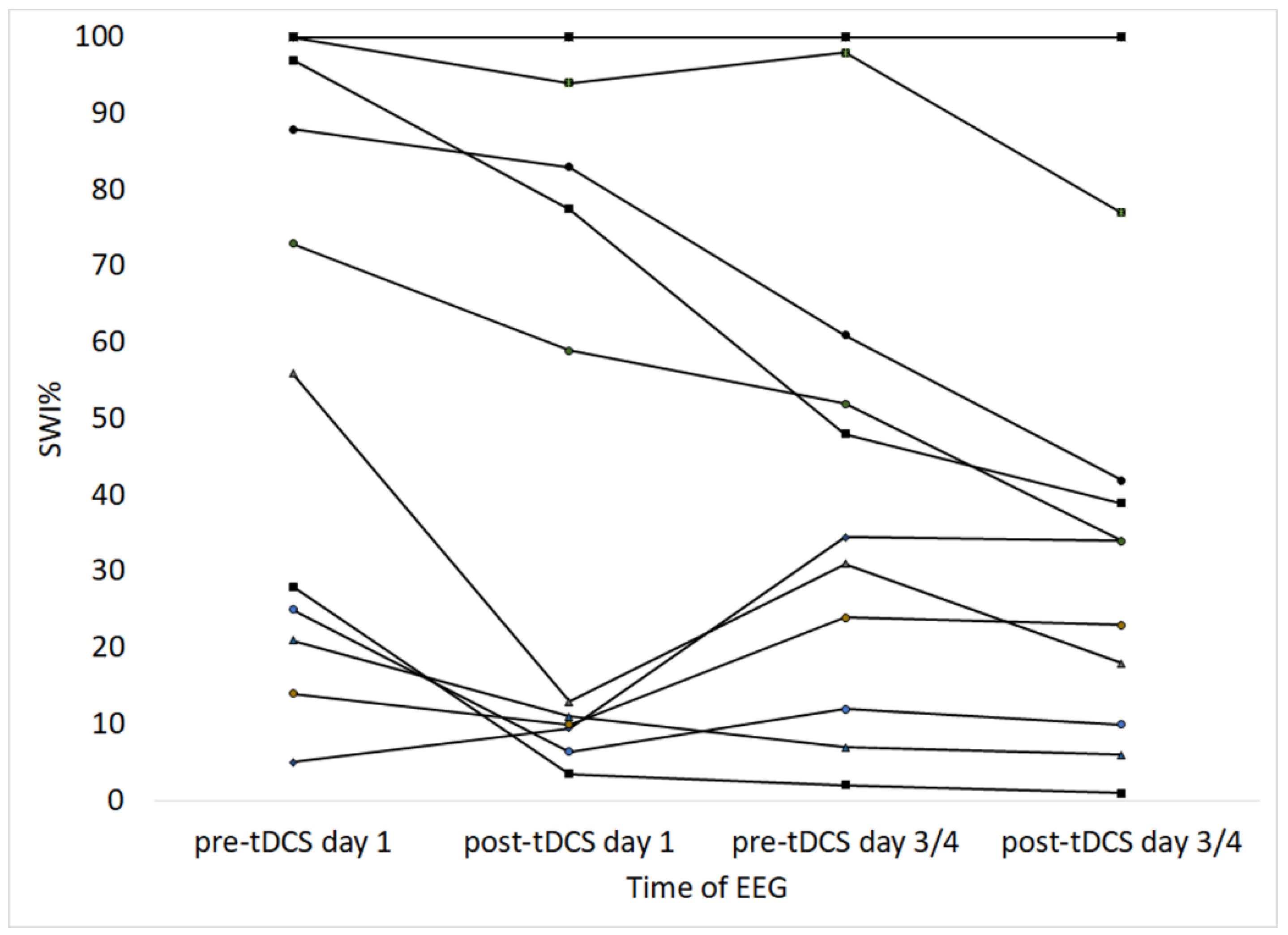
3.3. EEG and Spike Wave Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASM | Antiseizure medications |
| CSE | Convulsive status epilepticus |
| EEG | Electroencephalogram |
| DRE | Drug-resistant epilepsy |
| NIBS | Non-invasive brain stimulation |
| QOL | Quality of life |
| SWI | Spike wave index |
| tDCS | Transcranial direct current stimulation |
| vEEG | Video electroencephalogram |
References
- Geerts, A.; Arts, W.F.; Stroink, H.; Peeters, E.; Brouwer, O.; Peters, B.; Laan, L.; Van Donselaar, C. Course and outcome of childhood epilepsy: A 15-year follow-up of the Dutch Study of Epilepsy in Childhood. Epilepsia 2010, 51, 1189–1197. [Google Scholar] [CrossRef]
- Sultana, B.; Panzini, M.-A.; Carpentier, A.V.; Comtois, J.; Rioux, B.; Gore, G.; Bauer, P.R.; Kwon, C.-S.; Jetté, N.; Josephson, C.B.; et al. Incidence and Prevalence of Drug-Resistant Epilepsy: A Systematic Review and Meta-analysis. Neurology 2021, 96, 805–817. [Google Scholar] [CrossRef] [PubMed]
- Ben-Menachem, E. AAN/AES Guidelines on Use of New AEDS. Epilepsy Curr. 2005, 5, 30–32. [Google Scholar] [CrossRef]
- French, J.A. Refractory Epilepsy: Clinical Overview. Epilepsia 2007, 48 (Suppl. S1), 3–7. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.E.; Bowen, J.M.; Snead, O.C.; Elliott, I.; Donner, E.; Weiss, S.K.; Otsubo, H.; Ochi, A.; Drake, J.; Rutka, J.T.; et al. Access to surgery for paediatric patients with medically refractory epilepsy: A systems analysis. Epilepsy Res. 2013, 107, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Morrison-Levy, N.; Go, C.; Ochi, A.; Otsubo, H.; Drake, J.; Rutka, J.; Weiss, S.K. Children with autism spectrum disorders and drug-resistant epilepsy can benefit from epilepsy surgery. Epilepsy Behav. 2018, 85, 200–204. [Google Scholar] [CrossRef]
- Rosati, A.; De Masi, S.; Guerrini, R. Antiepileptic Drug Treatment in Children with Epilepsy. CNS Drugs 2015, 29, 847–863. [Google Scholar] [CrossRef]
- Ghosh, S.; Nagarajan, L. Non-invasive brain stimulation in childhood epilepsy. J. Int. Child Neurol. Assoc. 2016, 16, 113. [Google Scholar] [CrossRef]
- Sudbrack-Oliveira, P.; Barbosa, M.Z.; Thome-Souza, S.; Razza, L.B.; Gallucci-Neto, J.; Valiengo, L.D.C.L.; Brunoni, A.R. Transcranial direct current stimulation (tDCS) in the management of epilepsy: A systematic review. Seizure 2021, 86, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Du, Q.; Huang, Z.; Li, L.; Zhang, Z.; Zhang, L.; Zhao, X.; Zhao, X.; Li, T.; Lin, Y.; et al. Transcranial Direct Current Stimulation for Patients With Pharmacoresistant Epileptic Spasms: A Pilot Study. Front. Neurol. 2019, 10, 50. [Google Scholar] [CrossRef]
- Yang, D.; Wang, Q.; Xu, C.; Fang, F.; Fan, J.; Li, L.; Du, Q.; Zhang, R.; Wang, Y.; Lin, Y.; et al. Transcranial direct current stimulation reduces seizure frequency in patients with refractory focal epilepsy: A randomized, double-blind, sham-controlled, and three-arm parallel multicenter study. Brain Stimul. 2020, 13, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Auvichayapat, N.; Rotenberg, A.; Gersner, R.; Ngodklang, S.; Tiamkao, S.; Tassaneeyakul, W.; Auvichayapat, P. Transcranial Direct Current Stimulation for Treatment of Refractory Childhood Focal Epilepsy. Brain Stimul. 2013, 6, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Auvichayapat, N.; Sinsupan, K.; Tunkamnerdthai, O.; Auvichayapat, P. Transcranial Direct Current Stimulation for Treatment of Childhood Pharmacoresistant Lennox–Gastaut Syndrome: A Pilot Study. Front. Neurol. 2016, 7, 66. [Google Scholar] [CrossRef] [PubMed]
- Zoghi, M.; O’Brien, T.J.; Kwan, P.; Cook, M.J.; Galea, M.; Jaberzadeh, S. Cathodal transcranial direct-current stimulation for treatment of drug-resistant temporal lobe epilepsy: A pilot randomized controlled trial. Epilepsia Open 2016, 1, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Yook, S.-W.; Park, S.-H.; Seo, J.-H.; Kim, S.-J.; Ko, M.-H. Suppression of Seizure by Cathodal Transcranial Direct Current Stimulation in an Epileptic Patient—A Case Report -. Ann. Rehabil. Med. 2011, 35, 579–582. [Google Scholar] [CrossRef]
- Tekturk, P.; Erdogan, E.T.; Kurt, A.; Kocagoncu, E.; Küçük, Z.; Kinay, D.; Yapici, Z.; Aksu, S.; Baykan, B.; Karamursel, S. Transcranial direct current stimulation improves seizure control in patients with Rasmussen encephalitis. Epileptic Disord. 2016, 18, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Assenza, G.; Campana, C.; Assenza, F.; Pellegrino, G.; Di Pino, G.; Fabrizio, E.; Fini, R.; Tombini, M.; Di Lazzaro, V. Cathodal transcranial direct current stimulation reduces seizure frequency in adults with drug-resistant temporal lobe epilepsy: A sham controlled study. Brain Stimul. 2017, 10, 333–335. [Google Scholar] [CrossRef]
- Shelyakin, A.M.; Preobrazhenskaya, I.G.; Kassil’, M.V.; Bogdanov, O.V. The effects of transcranial micropolarization on the severity of convulsive fits in children. Neurosci. Behav. Physiol. 2001, 31, 555–560. [Google Scholar] [CrossRef]
- Meiron, O.; Gale, R.; Namestnic, J.; Bennet-Back, O.; Gebodh, N.; Esmaeilpour, Z.; Mandzhiyev, V.; Bikson, M. Antiepileptic Effects of a Novel Non-invasive Neuromodulation Treatment in a Subject With Early-Onset Epileptic Encephalopathy: Case Report With 20 Sessions of HD-tDCS Intervention. Front. Neurosci. 2019, 13, 547. [Google Scholar] [CrossRef]
- San-Juan, D.; Calcáneo, J.D.D.D.C.; González-Aragón, M.F.; Maldonado, L.B.; Avellán, M.; Argumosa, E.V.G.; Fregni, F. Transcranial direct current stimulation in adolescent and adult Rasmussen’s encephalitis. Epilepsy Behav. 2011, 20, 126–131. [Google Scholar] [CrossRef]
- San-Juan, D.; López, D.A.E.; Gregorio, R.V.; Trenado, C.; Aragón, M.F.-G.; Morales-Quezada, L.; Ruiz, A.H.; Hernandez-González, F.; Alcaraz-Guzmán, A.; Anschel, D.J.; et al. Transcranial Direct Current Stimulation in Mesial Temporal Lobe Epilepsy and Hippocampal Sclerosis. Brain Stimul. 2016, 10, 28–35. [Google Scholar] [CrossRef] [PubMed]
- San-Juan, D.; Morales-Quezada, L.; Garduño, A.J.O.; Alonso-Vanegas, M.; González-Aragón, M.F.; López, D.A.E.; Gregorio, R.V.; Anschel, D.J.; Fregni, F. Transcranial Direct Current Stimulation in Epilepsy. Brain Stimul. 2015, 8, 455–464. [Google Scholar] [CrossRef] [PubMed]
- San-Juan, D.; Sarmiento, C.I.; González, K.M.; Barraza, J.M.O. Successful Treatment of a Drug-Resistant Epilepsy by Long-term Transcranial Direct Current Stimulation: A Case Report. Front. Neurol. 2018, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- San-Juan, D. Cathodal Transcranial Direct Current Stimulation in Refractory Epilepsy: A Noninvasive Neuromodulation Therapy. J. Clin. Neurophysiol. 2021, 38, 503–508. [Google Scholar] [CrossRef]
- Kaye, H.L.; San-Juan, D.; Salvador, R.; Biagi, M.C.; Dubreuil-Vall, L.; Damar, U.; Pascual-Leone, A.; Ruffini, G.; Shafi, M.M.; Rotenberg, A. Personalized, Multisession, Multichannel Transcranial Direct Current Stimulation in Medication-Refractory Focal Epilepsy: An Open-Label Study. J. Clin. Neurophysiol. 2023, 40, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.-C.; Ouyang, C.-S.; Chiang, C.-T.; Yang, R.-C.; Wu, R.-C.; Wu, H.-C. Cumulative effect of transcranial direct current stimulation in patients with partial refractory epilepsy and its association with phase lag index-A preliminary study. Epilepsy Behav. 2018, 84, 142–147. [Google Scholar] [CrossRef]
- Daoud, M.; Salvador, R.; El Youssef, N.; Fierain, A.; Garnier, E.; Biagi, M.C.; Medina Villalon, S.; Wendling, F.; Benar, C.; Ruffini, G.; et al. Stereo-EEG based personalized multichannel transcranial direct current stimulation in drug-resistant epilepsy. Clin Neurophysiol. 2022, 137, 142–151. [Google Scholar] [CrossRef]
- Tsuboyama, M.; Kaye, H.L.; Rotenberg, A. Review of Transcranial Magnetic Stimulation in Epilepsy. Clin. Ther. 2020, 42, 1155–1168. [Google Scholar] [CrossRef]
- Grippe, T.C.; Brasil-Neto, J.P.; Boechat-Barros, R.; Cunha, N.S.; Oliveira, P.L. Interruption of Epilepsia Partialis Continua by Transcranial Direct Current Stimulation. Brain Stimul. 2015, 8, 1227–1228. [Google Scholar] [CrossRef]
- Karvigh, S.A.; Motamedi, M.; Arzani, M.; Roshan, J.H.N. HD-tDCS in refractory lateral frontal lobe epilepsy patients. Seizure 2017, 47, 74–80. [Google Scholar] [CrossRef]
- Meiron, O.; Gale, R.; Namestnic, J.; Bennet-Back, O.; David, J.; Gebodh, N.; Adair, D.; Esmaeilpour, Z.; Bikson, M. High-Definition transcranial direct current stimulation in early onset epileptic encephalopathy: A case study. Brain Inj. 2018, 32, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Thome-Souza, S.; Nitsche, M.A.; Freedman, S.D.; Valente, K.D.; Pascual-Leone, A. A controlled clinical trial of cathodal DC polarization in patients with refractory epilepsy. Epilepsia 2006, 47, 335–342. [Google Scholar] [CrossRef]
- Monte-Silva, K.; Kuo, M.-F.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Shaping the Optimal Repetition Interval for Cathodal Transcranial Direct Current Stimulation (tDCS). J. Neurophysiol. 2010, 103, 1735–1740. [Google Scholar] [CrossRef]
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Allen Hauser, W.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2010, 51, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Connolly, A.; Sabaz, M.; Lawson, J.; Bye, A. Cairns quality of life in childhood epilepsy: Validating the qolce. J. Paediatr. Child Health 2005, 41, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S.; et al. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef]
- Connelly, L.M. Research considerations: Power analysis and effect size. Medsurg Nurs. Off. J. Acad. Med.-Surg. Nurses 2008, 17, 41–42. [Google Scholar]
- Steriade, M. Cellular Substrates of Brain Rhythms. In Electroencephalography: Basic Principles, Clinical Applications, and Related Fields, 3rd ed.; Niedermeyer, E., Lopes Da Silva, F., Eds.; Williams & Wilkins: Baltimore: Baltimore, MD, USA, 1993; pp. 27–62. [Google Scholar]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.; Chen, R.; Cohen, L.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Monte-Silva, K.; Kuo, M.-F.; Hessenthaler, S.; Fresnoza, S.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Induction of Late LTP-Like Plasticity in the Human Motor Cortex by Repeated Non-Invasive Brain Stimulation. Brain Stimul. 2013, 6, 424–432. [Google Scholar] [CrossRef]
- Batsikadze, G.; Moliadze, V.; Paulus, W.; Kuo, M.-F.; Nitsche, M.A. Partially non-linear stimulation intensity-dependent effects of direct current stimulation on motor cortex excitability in humans. J. Physiol. 2013, 591, 1987–2000. [Google Scholar] [CrossRef] [PubMed]
- Polania, R.; Nitsche, M.A.; Paulus, W. Modulating functional connectivity patterns and topological functional organization of the human brain with transcranial direct current stimulation. Hum. Brain Mapp. 2011, 32, 1236–1249. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case No. and Gender | Age at tDCS (Years) | Age of Onset of Seizures | Seizure Types | Interictal Epileptiform Discharges | Epilepsy Classification | Etiology of Epilepsy | Development | No. of ASMs Tried | Other Treatments | Seizure Frequency |
|---|---|---|---|---|---|---|---|---|---|---|
| 1F | 17 | 3 m | FS, FS with SG | Focal RH | FE | Cortical dysplasia | Delayed | 13 | Steroids, folinic acid, pyridoxine | Variable, often >20/day |
| 2M | 17 | 2 y 5 m | GTC, AtS, FS | Focal RH > LH | FE | Rassmussen’s forme fruste | Delayed | 9 | IVIG, ketogenic diet | Variable, upto 80/day |
| 3F | 17 | 12 y | GTC, MS, AS, FS, NCSE | Generalized, focal occ RH + LH | GGE + IPOE | Not identified | Regression | 11 | VNS, ketogenic diet | Variable, two to three GTCS/day, innumerable MS/day |
| 4F | 4 | 3 m | GTC, AAS, MS, FS, CSE | Generalized, multifocal | FE + GE | Dravet syndrome | Delayed | 11 | Pyridoxine, prednisolone, ketogenic diet, IVIG, biotin | Innumerable per day, frequent status, in and out of hospital |
| 5F | 3 | 6 y | FS, FS with SG | Focal RH | FE | Rassmussen’s form fruste | WNL | 6 | Regular IVIG every 4 weeks, alternating with pulsed dexamethazone for 3 days every 4 weeks | 25–30/day |
| 6F | 3 | 2 y 2 m | FS, FS with SG | Focal RH, ESES RH | FE | Cortical dysplasia | WNL | 7 | None | >50/day |
| 7M | 3 | 1 y 2 m | FS, TS, FS with SG | Focal LH | FE | Cortical dyspasia | Delayed | 16 | Ketogenic diet, IVIG, IV methyl prednisolone, epilepsy surgery | Innumerable seizures per day, frequent status, in and out of hospital |
| 8F | 10 | 2 y 2 m | FS, TS, AtS, AAS | Multifocal LH > RH | FE | HSV encephalitis | Delayed | 14 | VNS, steroids, IVIG | 10 seizures per month, up to two to three per day |
| 9M | 7 | 6 m | FS, TS, AAS, GTC | Multifocal RH + LH | FE + GE | Not identified | Delayed | 7 | None | 30 seizures per month |
| 10M | 12 | 8 m | FS, FS with SG, HS | Focal LH | FE | Cortical dysplasia | Delayed | 11 | None | From one per week to one to two per day |
| 11M | 16 | 12 y 6 m | FS, AAS | Multifocal RH + LH | FE | Focal scarring following cranial surgery | WNL | 9 | None | One to two per day |
| 12M | 13 | 10 m | FS, FS with SG | Focal LH | FE | Cortical dysplasia | Delayed | 13 | Epilepsy surgery | One per week |
| Case No. and Gender | Age at tDCS (Years) | Antiseizure Medications at tDCS | Duration of Epilepsy at tDCS (Years) | Days of tDCS | Stimulation Amplitude (mA) | Cathode Location | Anode Location | No. of Seizures in 2 Weeks Pre-tDCS | No. of Seizures in 2 Weeks Post-tDCS | Other Improvements After tDCS at 2 Weeks | Adverse Effects of tDCS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1F | 17 | LCM, OXC, ZON | 17 | 4 | 1 | F4 | LSO | 4 | 4 | More alert, happier, less moody | Headache, irritation |
| 2M | 17 | LCM, TPM | 7 | 4 | 1 | P4, T4 | RSO, midline SO | Innumerable (up to 80/day) | Innumerable | None | Irritation |
| 3F | 17 | CLON, LTG, LEV, TPM, VPA | 7 | 3 | 1 | C1, C2 | LSO, RSO | ~40 | ~40 | Happier and spoke more clearly | Headache |
| 4F | 4 | TPM, PB, RUF, LEV | 3 | 3 | 0.8 | C1, C2 | LSO, RSO | Innumerable | Innumerable | Reduced ICU admissions for status for several months, more alert | None |
| 5F | 3 | LTG, PER, immunotherapy | 7 | 4 | 0.8 | C4 | RSO | ~20 | ~20 | None | Itchiness |
| 6F | 3 | SUL, LEV | 1 | 4 | 0.8 | C4, T4 | RSO, midline SO | >50 | >50 | None | Irritation |
| 7M | 3 | LTG, RTG, PTY, NZP | 2 | 3 | 0.8 | F3 | LSO | Innumerable | Innumerable | None | Seizure |
| 8F | 10 | ZON, CLOB, LCM | 8 | 4 | 1 | F3, F4 | LSO, RSO | 7 | 6 | None | None |
| 9M | 7 | VPA | 7 | 3 | 0.8 | F5, F6 | LSO, RSO | 13 | 14 | More alert, sleeps better, walking better | None |
| 10M | 12 | LEV, LTG | 11 | 4 | 0.8 | F3 | LSO | 14 | 13 | None | Unsteady gait |
| 11M | 16 | SUL, LTG | 4 | 3 | 1 | F3, F4 | LSO, RSO | ~20 | ~20 | None | None |
| 12M | 13 | PB, LCM, CBZ | 13 | 4 | 0.8 | Fp1, F3 | LSO, midline SO | 1 | 0 | More alert, playing sport | Headache |
| Case No. | First Day of tDCS | Last Day of tDCS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| and | Before tDCS | After tDCS | Before tDCS | After tDCS | ||||||
| Gender | Awake | Sleep | Awake | Sleep | Awake | Sleep | Awake | Sleep | ||
| SWI% | SWI% | SWI% | SWI% | Other Observations | SWI% | SWI% | SWI% | SWI% | Other Observations | |
| 1F | 25 | 6.4 | ↑β activity post-tDCS | 12 | 10 | ↑β activity post-tDCS | ||||
| 2M | 88 | 83 | ↑β activity post-tDCS | 61 | 42 | |||||
| 3F | 100 | 100 | 100 | 100 | ↓spike density post-tDCS | |||||
| 4F | 97 | 77.5 | ↑β activity post-tDCS | 48 | 39 | |||||
| 5F | 28 | 3.5 | 2 | 1 | ↑β activity post-tDCS | |||||
| 6F | 100 | 100 | 94 | ↑β activity, ↓spike density post-tDCS | 98 | 77 | ||||
| 7M | 5 | 12.5 | 9.5 | 10 | Seizure before tDCS | 34.5 | 34 | Seizure before and after tDCS | ||
| 8F | 100 | 100 | ↑β activity, ↓spike density post-tDCS | 100 | 100 | ↑β activity, ↓spike density post-tDCS | ||||
| 9M | 56 | 13 | ↑β activity, ↓spike density post-tDCS | 31 | 67 | 18 | ↑β activity, ↓spike density post-tDCS | |||
| 10M | 14 | 10 | ↓spike density post-tDCS | 24 | 23 | ↑β activity post-tDCS | ||||
| 11M | 21 | 11 | ↑β activity post-tDCS | 7 | 6 | |||||
| 12M | 73 | 80 | 59 | ↑β activity, less asymmetry post-tDCS | 52 | 57 | 34 | 38 | ↑β activity, less asymmetry post-tDCS | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghosh, S.; Nagarajan, L. Tolerability and Effectiveness of Cathodal Transcranial Direct Current Stimulation in Children with Refractory Epilepsy: A Case Series. Brain Sci. 2023, 13, 760. https://doi.org/10.3390/brainsci13050760
Ghosh S, Nagarajan L. Tolerability and Effectiveness of Cathodal Transcranial Direct Current Stimulation in Children with Refractory Epilepsy: A Case Series. Brain Sciences. 2023; 13(5):760. https://doi.org/10.3390/brainsci13050760
Chicago/Turabian StyleGhosh, Soumya, and Lakshmi Nagarajan. 2023. "Tolerability and Effectiveness of Cathodal Transcranial Direct Current Stimulation in Children with Refractory Epilepsy: A Case Series" Brain Sciences 13, no. 5: 760. https://doi.org/10.3390/brainsci13050760
APA StyleGhosh, S., & Nagarajan, L. (2023). Tolerability and Effectiveness of Cathodal Transcranial Direct Current Stimulation in Children with Refractory Epilepsy: A Case Series. Brain Sciences, 13(5), 760. https://doi.org/10.3390/brainsci13050760