Abstract
Agomelatine (AGM) is one of the latest atypical antidepressants, prescribed exclusively for the treatment of depression in adults. AGM belongs to the pharmaceutical class of melatonin agonist and selective serotonin antagonist (“MASS”), as it acts both as a selective agonist of melatonin receptors MT1 and MT2, and as a selective antagonist of 5-HT2C/5-HT2B receptors. AGM is involved in the resynchronization of interrupted circadian rhythms, with beneficial effects on sleep patterns, while antagonism on serotonin receptors increases the availability of norepinephrine and dopamine in the prefrontal cortex, with an antidepressant and nootropic effect. The use of AGM in the pediatric population is limited by the scarcity of data. In addition, few studies and case reports have been published on the use of AGM in patients with attention deficit and hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). Considering this evidence, the purpose of this review is to report the potential role of AGM in neurological developmental disorders. AGM would increase the expression of the cytoskeleton-associated protein (ARC) in the prefrontal cortex, with optimization of learning, long-term memory consolidation, and improved survival of neurons. Another important feature of AGM is the ability to modulate glutamatergic neurotransmission in regions associated with mood and cognition. With its synergistic activity a melatoninergic agonist and an antagonist of 5-HT2C, AGM acts as an antidepressant, psychostimulant, and promoter of neuronal plasticity, regulating cognitive symptoms, resynchronizing circadian rhythms in patients with autism, ADHD, anxiety, and depression. Given its good tolerability and good compliance, it could potentially be administered to adolescents and children.
1. Introduction
Agomelatine (AGM) is a melatonin analog with antidepressant properties prescribed for the treatment of depression in adults. It was approved by the European Medicines Agency (EMA) in 2009 and the Therapeutic Goods Administration in Australia in 2010 [1,2]. This molecule is also effective in the treatment of generalized anxiety disorder (GAD) [2,3,4], as well as in bipolar depression, alcohol abuse, and migraines [2,5,6].
Due to the paucity of clinical trials in the pediatric population, the safety and efficacy of AGM in children and adolescents have not yet been established.
AGM Pharmacology
AGM belongs to the pharmaceutical class of melatonin agonist and selective serotonin antagonist (MASS) since it acts synergistically as a selective agonist of the melatoninergic receptors MT1 and MT2, and a selective antagonist of 5-HT2C/5-HT2B receptors [7]. As an agonist of MT1/MT2, AGM has positive effects on the sleep–wake cycle, while as an antagonist of postsynaptic 5-HT2C receptors, it increases the availability of norepinephrine and dopamine in the prefrontal cortex with an antidepressant and nootropic effect [8]. In addition, antagonism of 5-HT2C may modulate the GABAergic pathway by the activation of GABA neurons in the amygdala, bed nucleus of stria terminalis, and hippocampus, with an anxiolytic activity [1,7].
After oral administration, AGM is rapidly absorbed (>75%) in the gastrointestinal tract, although extensive first-pass metabolism cuts its bioavailability to less than 5%. AGM is mostly metabolized by different hepatic cytochromes (CYP450, CYP1A2, and CYP2C9), and the resulting catabolites (mainly 3 hydroxyAGM and 7 desmethyl AGM) are largely eliminated by urinary excretion. Its mean half-life (t1/2) is approximately 2 h [2,7,8,9].
A recent meta-analysis, which included randomized and head-to-head trials of 21 antidepressants for the acute treatment of major depressive disorder (MDD) in adults, highlighted the good efficacy and tolerability of this compound [10]. Moreover, several studies also demonstrated the low incidence of side effects of AGM in anxiety disorders, particularly in GAD [4], and also in obsessive–compulsive disorder (OCD), both in monotherapy and in combination with other drugs [11,12,13,14,15].
Side effects, such as dizziness or nausea, are usually classified as mild or moderate. Of note, the risk of liver injury is dose-dependent and the main risk factors promoting hepatotoxicity include female gender, polypharmacy, and old age [16]. However, there is no agreement on this issue, as different research did not confirm these risk factors [2,17]. Regarding hepatotoxicity, EMA recommends performing liver function tests before starting treatment and then after approximately 3, 6, 12, and 24 weeks. If an elevation of transaminases is detected, these exams should be repeated within 48 h and agomelatine should be discontinued if the increase results in being more than three times above the limit of the normal range [18]. AGM tolerability has been considered throughout clinical trials, as a key benefit for treatment initiation and long-term adherence [1,14]. The lack of early relapse on switching to a placebo supports a minimal discontinuation syndrome [19].
The use of AGM in the pediatric population is limited by the paucity of data. Only one study investigated the efficacy of agomelatine among adolescents with MDD. This randomized, double-blind, multicenter study tested the short-term antidepressant efficacy and safety of AGM (10 mg or 25 mg per day) versus placebo with active control (fluoxetine 10–20 mg depending on symptom severity) after 12 weeks on patients aged 7–17 years. The AGM highest dosage of 25 mg/day resulted in an improvement versus placebo, with a similar effect for fluoxetine in adolescents but not in children. No unexpected safety signals were observed with agomelatine, with no significant weight gain or effect on suicidal behaviors [20].
2. Clinical Use of Agomelatine in ADHD and ASD
Here we provide an overview of the recent literature on the use of AGM in patients with ASD and ADHD.
2.1. ADHD
There is a limited number of clinical studies on the use of AGM in the ADHD population. We report on six articles. Three of them are single cases and two are clinical trials. All studies included children and adolescents. (Table 1).

Table 1.
Clinical use of AGM in ADHD patients.
In 2012, Niederhofer et al. demonstrated greater efficacy of add-on AGM (25 mg/day) to ongoing treatment with methylphenidate (MPH) or atomoxetine compared to placebo in a sample of 10 boys with ADHD (age range 17–19 years, M:F = 8:2) [7,8]. Patients treated showed less hyperactivity, greater tolerance to frustration, less irritability, and overall better affective modulation. Few side effects were observed, suggesting that AGM is a valid therapeutic option, especially in ADHD patients with sleep disorders (70% ADHD), anxiety, or oppositional–provocative comorbid disorder [21].
The addition of AGM (25 mg/day) to MPH in a 13-year-old female with severe ADHD, insomnia, and dysphoria resulted in clinical improvement and a global enhancement of MPH’s cognitive and behavioral effects. Good tolerability and no drug interactions were reported [22]. More recently (2020), the same authors reported an interesting case of a 15 year old girl with drug-resistant ADHD, who responded only to agomelatine (25 mg/die) [24].
In a cohort of 54 children with ADHD aged between 6 and 15 years of age, a pharmacological study compared the efficacy of MPH (20–30 mg/die depending on weight) with AGM (15–25 mg/day depending on weight) over about 6 weeks. No statistically significant difference emerged between the two randomized groups in terms of efficacy according to the parent and teacher ADHD Rating Scale-IV. Agomelatine was well-tolerated and also improved insomnia [23].
In ADHD patients have reduced neural tissue volume, particularly in the right frontal and parietal cortices, in association with hypo-functioning catecholaminergic circuits in the prefrontal cortex, which may explain the finding of AGM being comparatively effective as MPH for ADHD treatment [25,26].
2.2. ASD
The impact of AGM on ASD has been studied in the adult population or in animal models, with the exception of a single case report of a 10 year old child. (Table 2).
Table 2.
Clinical use of AGM in ASD patients.
In 2015, Nagury emphasized the therapeutic efficacy of AGM on a 10-year-old autistic patient with severe behavioral disorder and insomnia, poorly responsive to aripiprazole and risperidone. Clinical improvement in terms of irritability, hyperactivity, and stereotypes was reported after the administration of AGM (25 mg/day) as monotherapy [28].
In the same year, Ballester conducted a randomized, cross-double-blind, multicenter study of 25 patients with ASD (M:F = 20:5) with an average age of approximately 32 years.
Participants were randomized to receive AGM (25 mg/die) or placebo for 3 months, at two different moments. Functional circadian rhythm markers (i.e., wrist temperature, actimetry, and position [TAP]) and salivary cortisol were measured during a week at the beginning and at the end of each period. Significant differences in improving circadian rhythms in the AGM group were noticed. AGM was effective in improving sleep patterns in ASD compared with placebo [29].
Later, the same group published a cross-sectional, randomized, triple-blind, placebo-controlled study conducted on 23 adult patients with ASD and intellectual disability with associated sleep disturbance. The results show a significant improvement in the sleep structure in the group treated with AGM, in terms of increased total night-time sleep time, sleep stability, and phase correction. The adverse effects were minimal [30].
In animal models of ASD induced by prenatal administration of valproic acid (VPA) in mice (2015), it was observed that the administration of AGM was associated with a reduction in autistic-like behaviors, a decrease in oxidative and nitrosative markers, and inflammation [31].
Previously, in 2011, Niederhofer demonstrated that AGM (25 mg/die) was not more efficient compared to duloxetine (40 mg/day), respectively, in one and two adult patients with ASD and intellectual disability. In addition, no major adverse effects were reported [27].
3. Potential Effects of AGM in Neurodevelopmental Disorders
Despite belonging to different and well-defined nosographic entities, neurodevelopmental disorders and, more broadly, psychiatric disorders seem to share common etiopathogenetic mechanisms, with consequent symptomatic overlap [32,33,34,35].
Numerous pieces of evidence show how the pathophysiology of ASD, ADHD, anxiety, and depression is multifactorial, involving different mechanisms such as neuroinflammation, oxidative stress, and glutamatergic dysfunction [33,34,35,36,37,38,39,40,41,42]. These pathways are complementary and strictly interconnected, able to activate a self-amplifying vicious circle [38,39,40,41].
There is currently no specific cure for the symptomatic core of autism, while psychotropic medication aims to alleviate psychiatric and behavioral problems such as aggression, self-injury, impulsivity, hyperactivity, irritability, anxiety, and mood disorders. Benefits have been reported with (i) atypical antipsychotics for aggression, self-injurious behavior, or temper tantrums; (ii) selective serotonin reuptake inhibitors (SSRI) for anxiety and repetitive behaviors; and (iii) psychostimulants or opioid antagonists for hyperactivity [43].
Psychostimulants are still considered the most effective therapy for children, adolescents, and adults with ADHD. The first choice drug is MPH [44,45,46,47]. Among noradrenergic modulators approved for the treatment of ADHD, we find tricyclic antidepressants with secondary amine structures such as desipramine and nortriptyline, alpha-2 adrenergic agonists including clonidine and guanfacine, indirect agonists such as bupropion, and atomoxetine, which is a selective blocker of the reuptake of noradrenaline [45,48].
In general, AGM treatment would aim not only to reduce depressive and anxiolytic symptoms, but also to prevent relapses, chronicity, and complications, and improve social and functional adaptation.
Anxiety and depression co-occur frequently with ADHD and ASD, increasing their clinical severity [49,50,51,52,53,54].
Although available antidepressants significantly ameliorate these disorders, they take several weeks to exert their full efficacy. Furthermore, many patients respond inadequately and co-morbid symptoms are often not well-controlled, leading to problems of poor tolerance, including gastrointestinal disturbances, weight gain, sleep disturbances, sexual dysfunction, and discontinuation effects [55].
3.1. Melatoninergic Action
Sleep is a fundamental operating state of the central nervous system and occupies up to a third of the human life span. Human research demonstrated a central role of sleep in mental health, influencing a wide range of cognitive and emotional functions such as memory consolidation, problem-solving, creativity, affective reactivity, and management of interpersonal conflicts [56,57,58,59,60].
Genes associated with circadian rhythm regulation have been found to be related to many mental diseases, and the function of dopaminergic and serotonergic networks has been shown to interplay with circadian and sleep biological mechanisms [61].
Neurobiological balance between arousal and de-arousal is disturbed in most mental disorders and likely represents a basic dimension for brain function [56,62]. From this point of view, it can be assumed that sleep impairment plays a relevant role in facilitating and maintaining mental disorders and that transdiagnostic treatment of sleep disturbance may improve intervention outcomes [61,62].
An intrinsic melatonin deficiency has been supposed to dysregulate sleep architecture [63].
Some studies found abnormal concentrations of melatonin in the urine and blood of patients with neurodevelopment disorders, corresponding to altered circadian release patterns [34,64,65].
Melatonin is an indole hormone that is enzymatically synthesized in the pineal gland from the amino acid tryptophan by N-acetylation and subsequent O-methylation of 5-HT [66]. Its secretion is inhibited by light and regulated by the circadian clock located in the hypothalamic suprachiasmatic nuclei. In humans, this neurohormone is mainly produced in the pineal gland, gastrointestinal tract, and retina, but only melatonin secretion by the pineal gland and retina follows a typical circadian rhythm [67]. At the onset of darkness, reduced retinal input leads to the disinhibition of enzymes responsible for melatonin synthesis [68]. (Figure 1). This increased synthesis leads to the highest nocturnal plasma concentrations of approximately 80 to 120 pg/mL between 2 and 4 h. Then, melatonin levels decrease until daylight onset, with low (10–20 pg/mL) concentrations during the daytime [67]. A study by Sadeh et al. demonstrated that infants with an immature pattern of melatonin secretion showed a delayed peak in melatonin levels, with more fragmented sleep during the night [69].
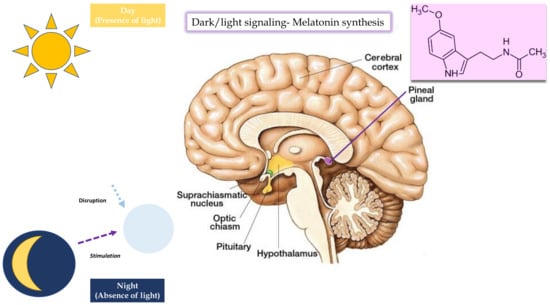
Figure 1.
Dark/light signaling, melatonin synthesis.
Due to the low bioavailability of melatonin as a supplement, AGM would represent a better pharmacological strategy for restoring melatoninergic homeostasis and physiological circadian rhythmicity [41,70].
3.2. Anti-Inflammatory and Oxidative Stress Action
Melatonin regulates several biological functions since it shows anti-inflammatory, antioxidant, and free radical scavenging properties.
Several authors argue that the depletion of endogenous melatonin could be explained by hyperactivation of the Kynurenines pathway (KP) from tryptophan, with the subsequent reduction in its bioavailability for the synthesis first of serotonin and then of melatonin [71,72,73]. Kynurenines represent a heterogeneous group of neuroactive catabolites, which mediate different pathways such as neuroinflammation, redox homeostasis, and glutamatergic toxicity by acting directly and indirectly on neurotransmitter systems involved in the pathogenesis of psychiatric disorders [72]. (Figure 2).
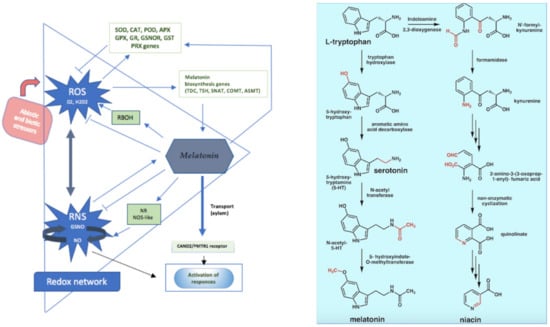
Figure 2.
Melatonin antioxidant properties and tryptophan metabolic pathway.
The shift of tryptophan towards the KP seems to be promoted by high concentrations of pro-inflammatory cytokines (IL-6, INF-y), ROS/NOS, and cortisol, which are associated with neuroinflammation, oxidative stress, and HPA-overactivation [39,41,71,72,73].
Interestingly, polymorphisms localized in genes involved in the tryptophan catabolic pathway may modulate the response to antidepressant treatment. Polymorphism of tryptophan hydroxylase-1 and -2 (TPH1- TPH2) and kynurenine aminotransferase I (KATI) genes may be associated with a lack of response to conventional antidepressant therapy since they can change messenger RNA (mRNA) and protein expression levels or methylation status of promoter regions [74,75,76,77,78].
Studies on animal models highlighted how the administration of AGM may modulate the transduction of mRNA and protein, as well as the expression of genes involved in the tryptophan pathway in the blood and brain structures [74,75]. This potentially may protect the brain from the neurotoxic consequences, due to the conversion of kynurenic acid (KYNA) to quinolinic acid (QUIN).
Furthermore, AGM treatment ameliorated inflammatory responses by decreasing the protein levels of inflammasome components, and by inhibiting microglial activation through the toll-like receptor 4/NOD-like receptor protein 3 (TLR4/NLRP3) signaling pathway [79].
Oxidative stress may be associated with the development of depression, ASD, and ADHD. A recent pre-clinical study shows that chronic administration of AGM modifies the expression level and methylation status of the promoter region of genes involved in oxidative and nitrosative stress. Stressed rats treated with AGM displayed a significantly lower glutathione peroxidase 4 (Gpx4) level in the hypothalamus [74]. Additionally, for the evaluation of the effect of AGM on oxidative stress and inflammation, glutathione (GSH), malondialdehyde (MDA), tumor necrosis factor (TNF), and interleukin-6 (IL-6) levels were analyzed in immortalized mouse hippocampal neuronal cell HT-22 and in hippocampal tissues in male rats. AGM significantly attenuated oxidative stress and inflammation due to the cisplatin insult in vitro and in vivo, and ameliorated the neuronal pathology in the hippocampus, which is strongly related to cognition and memory [80].
3.3. Neurotrophic, Anti-Glutamatergic, and Anxiolytic Actions
One of the most relevant effects of melatonin and, therefore, of AGM, is the activation of the gene expression of the neurotrophic factor brain-derived neurotrophic factor (BDNF) in the prefrontal cortex, hippocampus, subventricular area, and olfactory tubercle [42,81]. BDNF is responsible for neurogenesis and neuronal trophism, underpinning neuronal plasticity [81]. Neurogenesis (especially hippocampal neurogenesis) has been implicated in cognitive processes such as learning, memory, pattern separation, and cognitive flexibility [82,83]. Abnormal neuronal plasticity leads to an inability to adapt to stressful stimuli, with reduced resilience and dysfunctional behaviors [81,84,85,86]. Furthermore, AGM would increase the expression of the activity-regulated cytoskeleton-associated protein (ARC) in the prefrontal cortex [87,88]. ARC regulates glutamatergic synapse plasticity and its expression is induced in a number of brain regions following emotionally relevant experiences, including exposure to novelty, environmental enrichment, and stressful experiences. It is also involved in other cognitive functions such as memory consolidation, spatial learning, and memory, and fear learning [87].
AGM has been shown to modulate glutamatergic neurotransmission in regions associated with mood and cognition. More precisely, AGM reduces the stress-induced release of glutamate in the prefrontal and frontal cortex [38]. In predisposed subjects, exposure to intense and chronic stress excessively activates excessively the hypothalamic–pituitary–adrenal (HPA) axis, causing a high release of ACTH and cortisol [88,89]. High concentrations of glucocorticoids lead to an excessive release of glutamate, with the imbalance between inhibition/excitation of the neuronal circuits and consequent glutamatergic excitotoxicity [89].
Excitotoxicity promotes abnormal neurogenesis and neuronal plasticity, as well as dysfunction in the default mode network, and visual and auditory systems, with the onset of cognitive deficits, general dyspraxia, behavioral changes, social dysfunction, and EEG abnormalities/seizures [63,90].
In animal studies, chronic AGM administration (3 weeks) increased cell proliferation and neurogenesis in the ventral dentate gyrus (a region implicated in fear-related behaviors) and prevented transcription of the interleukin-1β (IL-1β) and metabotropic glutamatergic receptor (mGluR) genes [91].
AGM also displayed robust anxiolytic properties in rats [1]. Early life adversity (e.g., social isolation rearing) has profound effects on neurodevelopment, altering 5-HT and other neurotransmitters, leading to anxiety, depression, and antisocial behavior in later stages [92]. Social isolation rearing is known to destabilize circadian rhythms while altered circadian fluctuation of different neuropeptides, such as vasopressin, oxytocin, and corticosterone has been described in chronic anxiety states [93]. In rats, social isolation rearing is associated with reduced plasma corticosterone and oxytocin and increased vasopressin.
Given the chronobiotic effects of AGM through simultaneous stimulation of MT1/MT2 and blockade of 5-HT2C receptors in the suprachiasmatic nucleus, during chronic stress, AGM may regulate oxytocin and vasopressin release by resynchronizing related neuropeptide rhythm disorders [94]. Thus, the anxiolytic effect of AGM could also be attributed to a decrease in vasopressin and an increase in oxytocin levels [92,93].
3.4. 5-HT2C Antagonist Action
Dopaminergic and noradrenergic pathway dysfunction in the frontal cortex represents one of the neurobiological mechanisms underlying psychiatric disorders. The frontal cortex plays a fundamental role in cognitive processes and the regulation of behavior and emotions [94,95,96].
Impairment in this area leads to loss of motivation and disinhibition, considered clinical key features of depression, ADHD, ASD, and some anxiety disorders [96,97,98].
Neuroimaging techniques prove that symptomatologic overlap between those disorders is linked to dysfunction in specific neuroanatomical areas. In depressed patients, the basal activity of the dorsolateral prefrontal cortex is reduced; in the ADHD population, the frontal cortex and some basal ganglia (caudate nucleus and the pale globe) are smaller [99,100,101], and characterized by a slower activation with less oxygen consumption [102]. In ASD patients, synaptic and neurotransmitter dissociation between the prefrontal cortex and other brain regions has been noted, which, in turn, has been correlated to social and communication impairment [103,104,105,106].
AGM inhibits the release of dopamine and norepinephrine, by blocking 5-HT2C presynaptic receptors, enhancing its transmission in the prefrontal cortex [48]. The increase in norepinephrine and dopamine availability in the frontal cortex acts both as antidepressant and psychostimulant.
This innovative mechanism for an antidepressant provides more physiological activation of the areas of executive functions such as working memory and decision-making processes, improving, theoretically, ASD and ADHD functioning. In particular, AGM seems to ameliorate intentional cognition and discriminatory attention, leading to less irritability and better affective regulation, as shown in patients on treatment [107,108].
4. Potential Therapeutic Role of AGM against SARS-CoV-2
Melatonin has been recently identified among the top five molecules with potential anti-SARS-CoV-19 action [109].
It has been hypothesized that melatonin significantly inhibits inflammasome stimulation, which could indirectly reduce the intensity of the cytokine storm following infection [110]. Moreover, it can promote the restoration of circadian rhythm and mitochondrial metabolism and can regulate the cellular oxidative status, favoring cell survival in the lung under stress and inflammatory conditions [111,112].
In a one-silico study, it was demonstrated that melatonin could act as a SARS-CoV-2 main protease (Mpro) inhibitor [113]. Another preclinical study showed that melatonin, AGM, and ramelteon can bind to host cell angiotensin-converting enzyme 2 receptors (ACE 2) and viral receptor-binding domain (RBD) [112,114,115], preventing viral entry into the host cells [112]. More recently, in transgenic mice expressing human ACE 2 receptor (K18-hACE 2), strongly susceptible to SARS-CoV-2 infection, daily melatonin, AGM, or ramelteon administration delayed the occurrence of severe clinical outcomes, with the improvement in survival, especially with a high melatonin dose [116].
By restoring antioxidant and inflammatory status and sleep patterns in COVID-19 patients, AGM could serve as an adjuvant in COVID-19 disease management [117]. It is to be reiterated that it could also be used as an antidepressant to manage the psychiatric complications of COVID-19 infection [112].
5. Conclusions
Comorbidity is the rule and not the exception in mental illnesses, making it important to spread the focus from specific disorders to psychobiological mechanisms that cut across mental disorders.
In the pediatric population, the strict categorical approach to psychopathology is much more difficult than in the adult population. During childhood and adolescence, psychiatric symptoms appear as much more nuanced and variable, in line with the different ages of development and the immaturity of the internal psychic systems.
Therefore, the idea of a symptomatologic continuum among mental disorders constitutes an increasingly pressing concept. According to what has been said, the use of multi-target drugs that act on specific symptoms, modulating simultaneously the pathological background, would allow not only the customization of therapy according to the patient’s need, but also the treatment of different pathological conditions. With its synergistic activity as a melatoninergic agonist and 5-HT2C antagonist, AGM acts as an antidepressant, a psychostimulant, and a promoter of neuronal plasticity, regulating cognitive, affective symptoms, and resynchronizing circadian rhythms in patients with autism, ADHD, anxiety, and depression. It is considered to have a favorable side-effect profile, without the weight gain, sexual side-effects, or discontinuation syndrome seen with traditional antidepressants such as SSRI/SNRIs.
Given its good tolerability and good compliance, AGM can be potentially administered to teenagers and children. To bypass the current gap of data on the use of AGM in developmental patients, controlled clinical trials are needed. The high frequency with which anxiety, depression, and sleep disorders co-occur in ASD and ADHD, in conjunction with their unique impact on functioning, adult outcome, and quality of life, is critical to consider how to best prevent and treat these disorders among children and adolescents. Also, considering the historical moment and the personal and family upheaval that the COVID-19 emergency has created and is still creating, it is not surprising to detect an exponential growth of affective, cognitive, and behavioral symptoms, as well as sleep disturbances, among children and adolescents with neurodevelopmental disorders. This phenomenon could be presumably correlated to pandemic-related stress and higher anxiety levels in vulnerable adolescents and young adults [118,119]. In this scenario, using a versatile and tolerable drug such as AGM would represent an innovative opportunity to improve the therapeutic perspective of chronic neurodevelopmental disorders. Modulation of neurocircuits in developmental age would improve clinical outcomes, preventing chronicity of therapy and, of course, bringing a reduction in dysmetabolic side effects.
Author Contributions
Conceptualization, A.N.P., R.S., M.C. and G.M. (Giovanni Messina); methodology, R.S. and A.B.; software, G.M. (Gabriella Marsala); validation, A.V. (Anna Valenzano) and V.M.; formal analysis, M.D.S. and M.I.D.S.; investigation, A.V. (Antonio Ventriglio) and L.M.; resources, M.M.; data curation, G.M. (Giovanni Messina); writing—original draft preparation, R.S.; writing—review and editing, R.S., M.C. and R.P.; visualization, A.N.P. and G.C.; supervision, G.M. (Giovanni Messina) and M.C.; project administration, G.M. (Giovanni Messina); funding acquisition, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- de Bodinat, C.; Guardiola-Lemaitre, B.; Mocaër, E.; Renard, P.; Muñoz, C.; Millan, M.J. AGM, the First Melatonergic Antidepressant: Discovery, Characterization and Development. Nat. Rev. Drug Discov. 2010, 9, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Grassi, S.; Serati, M.; Altamura, A.C. AGM for the Treatment of Generalized Anxiety Disorder. Expert Opin. Pharmacother. 2017, 18, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Pae, C.-U. AGM: A New Option for Treatment of Depression? Expert Opin. Pharmacother. 2014, 15, 443–447. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, D.; Conti, C.M.; Marini, S.; Ferri, F.; Iasevoli, F.; Valchera, A.; Fornaro, M.; Cavuto, M.; Srinivasan, V.; Perna, G.; et al. Is There a Role for AGM in the Treatment of Anxiety Disorders? A Review of Published Data. Int. J. Immunopathol. Pharmacol. 2013, 26, 299–304. [Google Scholar] [CrossRef] [PubMed]
- De Berardis, D.; Fornaro, M.; Serroni, N.; Campanella, D.; Rapini, G.; Olivieri, L.; Srinivasan, V.; Iasevoli, F.; Tomasetti, C.; De Bartolomeis, A.; et al. AGM beyond Borders: Current Evidences of Its Efficacy in Disorders Other than Major Depression. Int. J. Mol. Sci. 2015, 16, 1111–1130. [Google Scholar] [CrossRef]
- Fornaro, M.; McCarthy, M.J.; De Berardis, D.; De Pasquale, C.; Tabaton, M.; Martino, M.; Colicchio, S.; Cattaneo, C.I.; D’Angelo, E.; Fornaro, P. Adjunctive AGM Therapy in the Treatment of Acute Bipolar II Depression: A Preliminary Open Label Study. Neuropsychiatr. Dis. Treat. 2013, 9, 243–251. [Google Scholar] [CrossRef]
- Gahr, M. AGM in the Treatment of Major Depressive Disorder: An Assessment of Benefits and Risks. Curr. Neuropharmacol. 2014, 12, 287–398. [Google Scholar] [CrossRef]
- Millan, M.J.; Gobert, A.; Lejeune, F.; Dekeyne, A.; Newman-Tancredi, A.; Pasteau, V.; Rivet, J.-M.; Cussac, D. The Novel Melatonin Agonist AGM (S20098) Is an Antagonist at 5-Hydroxytryptamine2C Receptors, Blockade of Which Enhances the Activity of Frontocortical Dopaminergic and Adrenergic Pathways. J. Pharmacol. Exp. Ther. 2003, 306, 954–964. [Google Scholar] [CrossRef]
- Sansone, R.A.; Sansone, L.A. AGM: A Novel Antidepressant. Innov. Clin. Neurosci. 2011, 8, 10–14. [Google Scholar]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative Efficacy and Acceptability of 21 Antidepressant Drugs for the Acute Treatment of Adults with Major Depressive Disorder: A Systematic Review and Network Meta-Analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef]
- Potměšil, P. What Combinations of AGM with Other Antidepressants Could Be Successful during the Treatment of Major Depressive Disorder or Anxiety Disorders in Clinical Practice? Ther. Adv. Psychopharmacol. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Coles, M.E.; Goodman, M.H. A Systematic Review of Case Studies Testing a Melatonergic Agonist/ 5HT2c Antagonist for Individuals with Obsessive Compulsive Disorder. J. Anxiety Disord. 2020, 69, 102173. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Ahokas, A.; Jarema, M.; Avedisova, A.S.; Vavrusova, L.; Chaban, O.; Gruget, C.; Olivier, V.; Picarel-Blanchot, F.; de Bodinat, C. Efficacy and Safety of AGM (10 or 25 Mg/Day) in Non-Depressed out-Patients with Generalized Anxiety Disorder: A 12-Week, Double- Blind, Placebo-Controlled Study. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2017, 27, 526–537. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Khoo, J.-P.; Picarel-Blanchot, F.; Olivier, V.; Van Ameringen, M. Efficacy of AGM 25–50 Mg for the Treatment of Anxious Symptoms and Functional Impairment in Generalized Anxiety Disorder: A Meta-Analysis of Three Placebo-Controlled Studies. Adv. Ther. 2021, 38, 1567–1583. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Deng, H.; Wan, J.; Zhou, Y.; Zhou, Y.; Song, B.; Wang, X. Comparative Remission Rates and Tolerability of Drugs for Generalised Anxiety Disorder: A Systematic Review and Network Meta-Analysis of Double-Blind Randomized Controlled Trials. Front. Pharmacol. 2020, 11, 580858. [Google Scholar] [CrossRef]
- Freiesleben, S.D.; Furczyk, K. A Systematic Review of AGM-Induced Liver Injury. J. Mol. Psychiatry 2015, 3, 4. [Google Scholar] [CrossRef]
- Perlemuter, G.; Cacoub, P.; Valla, D.; Guyader, D.; Saba, B.; Batailler, C.; Moore, K. Characterisation of AGM-Induced Increase in Liver Enzymes: Frequency and Risk Factors Determined from a Pooled Analysis of 7605 Treated Patients. CNS Drugs 2016, 30, 877–888. [Google Scholar] [CrossRef]
- Procedure No. EMEA/H/C/000916. Ema/97539/2009. Available online: https://www.ema.europa.eu/en/documents/assessment-report/thymanax-epar-public-assessment-report_en.pdf (accessed on 5 March 2023).
- Goodwin, G.M.; Emsley, R.; Rembry, S.; Rouillon, F.; AGM Study Group. AGM Prevents Relapse in Patients with Major Depressive Disorder without Evidence of a Discontinuation Syndrome: A 24-Week Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Psychiatry 2009, 70, 1128–1137. [Google Scholar] [CrossRef]
- Arango, C.; Buitelaar, J.K.; Fegert, J.M.; Olivier, V.; Pénélaud, P.-F.; Marx, U.; Chimits, D.; Falissard, B.; Barylnik, J.; Birdeanu, L.; et al. Safety and Efficacy of AGM in Children and Adolescents with Major Depressive Disorder Receiving Psychosocial Counselling: A Double-Blind, Randomised, Controlled, Phase 3 Trial in Nine Countries. Lancet Psychiatry 2022, 9, 113–124. [Google Scholar] [CrossRef]
- Niederhofer, H. AGM Treatment with Adolescents with ADHD. J. Atten. Disord. 2012, 16, 530–532. [Google Scholar] [CrossRef]
- Salardini, E.; Zeinoddini, A.; Kohi, A.; Mohammadi, M.-R.; Mohammadinejad, P.; Khiabany, M.; Shahriari, M.; Akhondzadeh, S. AGM as a Treatment for Attention- Deficit/Hyperactivity Disorder in Children and Adolescents: A Double-Blind, Randomized Clinical Trial. J. Child Adolesc. Psychopharmacol. 2016, 26, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Haya Al Mutairi, A.N. AGM Augmenting Partial Stimulant Response in ADHD and Mitigating Stimulant-Induced Insomnia and Anxiety. J. Child Adolesc. Behav. 2015, 3, 1000208. [Google Scholar] [CrossRef]
- Naguy, A.; Alamiri, B. Successful AGM Monotherapy for an Adolescent with Attention Deficit Hyperactivity Disorder and Comorbid Migraine. CNS Spectr. 2020, 27, 134–135. [Google Scholar] [CrossRef] [PubMed]
- Purper-Ouakil, D.; Ramoz, N.; Lepagnol-Bestel, A.-M.; Gorwood, P.; Simonneau, M. Neurobiology of Attention Deficit/Hyperactivity Disorder. Pediatr. Res. 2011, 69, 69R–76R. [Google Scholar] [CrossRef] [PubMed]
- Curatolo, P.; Paloscia, C.; D’Agati, E.; Moavero, R.; Pasini, A. The Neurobiology of Attention Deficit/Hyperactivity Disorder. Eur. J. Paediatr. Neurol. EJPN Off. J. Eur. Paediatr. Neurol. Soc. 2009, 13, 299–304. [Google Scholar] [CrossRef]
- Niederhofer, H. Efficacy of Duloxetine and AGM Does Not Exceed That of Other Antidepressants in Patients with Autistic Disorder: Preliminary Results in 3 Patients. Prim. Care Companion CNS Disord. 2011, 13, PCC.10l01038. [Google Scholar] [CrossRef]
- Naguy, A.; Tajali, A.A. AGM Addressing Behavioural Facets in Autism. J. Psychiatry 2015, 18. [Google Scholar] [CrossRef]
- Ballester, P.; Martínez, M.J.; Inda, M.-M.; Javaloyes, A.; Richdale, A.L.; Muriel, J.; Belda, C.; Toral, N.; Morales, D.; Fernández, E.; et al. Evaluation of AGM for the Treatment of Sleep Problems in Adults with Autism Spectrum Disorder and Co-Morbid Intellectual Disability. J. Psychopharmacol. 2019, 33, 1395–1406. [Google Scholar] [CrossRef]
- Ballester, P.; Martínez, M.J.; Javaloyes, A.; Hernández, L.; Peiró, A.M. Agomelatine Effectiveness in Sleep Disturbances in Autism Spectrum Disorder. Clin. Ther. 2015, 37, e132–e133. [Google Scholar] [CrossRef]
- Kumar, H.; Sharma, B.M.; Sharma, B. Benefits of AGM in Behavioral, Neurochemical and Blood Brain Barrier Alterations in Prenatal Valproic Acid Induced Autism Spectrum Disorder. Neurochem. Int. 2015, 91, 34–45. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- White, S.W.; Roberson-Nay, R. Anxiety, Social Deficits, and Loneliness in Youth with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, K.; Godbout, R. Melatonin and Comorbidities in Children with Autism Spectrum Disorder. Curr. Dev. Disord. Rep. 2018, 5, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and Depression in Adults with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Zappulo, E.; Militerni, R.; Pascotto, A.; Borgia, G.; Bravaccio, C. Etiopathogenesis of Autism Spectrum Disorders: Fitting the Pieces of the Puzzle Together. Med. Hypotheses 2013, 81, 26–35. [Google Scholar] [CrossRef]
- Giana, G.; Romano, E.; Porfirio, M.C.; D’Ambrosio, R.; Giovinazzo, S.; Troianiello, M.; Barlocci, E.; Travaglini, D.; Granstrem, O.; Pascale, E.; et al. Detection of Auto-Antibodies to DAT in the Serum: Interactions with DAT Genotype and Psycho-Stimulant Therapy for ADHD. J. Neuroimmunol. 2015, 278, 212–222. [Google Scholar] [CrossRef]
- Santos, P.; Herrmann, A.P.; Elisabetsky, E.; Piato, A. Anxiolytic Properties of Compounds That Counteract Oxidative Stress, Neuroinflammation, and Glutamatergic Dysfunction: A Review. Rev. Bras. Psiquiatr. Sao Paulo Braz. 1999 2019, 41, 168–178. [Google Scholar] [CrossRef]
- Savino, R.; Carotenuto, M.; Polito, A.N.; Di Noia, S.; Albenzio, M.; Scarinci, A.; Ambrosi, A.; Sessa, F.; Tartaglia, N.; Messina, G. Analyzing the Potential Biological Determinants of Autism Spectrum Disorder: From Neuroinflammation to the Kynurenine Pathway. Brain Sci. 2020, 10, 631. [Google Scholar] [CrossRef]
- Frye, R.E.; Delatorre, R.; Taylor, H.; Slattery, J.; Melnyk, S.; Chowdhury, N.; James, S.J. Redox Metabolism Abnormalities in Autistic Children Associated with Mitochondrial Disease. Transl. Psychiatry 2013, 3, e273. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. Melatonin in Autism Spectrum Disorders: A Systematic Review and Meta-Analysis: Review. Dev. Med. Child Neurol. 2011, 53, 783–792. [Google Scholar] [CrossRef]
- Ramírez-Rodríguez, G.; Klempin, F.; Babu, H.; Benítez-King, G.; Kempermann, G. Melatonin Modulates Cell Survival of New Neurons in the Hippocampus of Adult Mice. Neuropsychopharmacology 2009, 34, 2180–2191. [Google Scholar] [CrossRef]
- Lacivita, E.; Perrone, R.; Margari, L.; Leopoldo, M. Targets for Drug Therapy for Autism Spectrum Disorder: Challenges and Future Directions. J. Med. Chem. 2017, 60, 9114–9141. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Couture, J. A Review of the Pathophysiology, Etiology, and Treatment of Attention-Deficit Hyperactivity Disorder (ADHD). Ann. Pharmacother. 2014, 48, 209–225. [Google Scholar] [CrossRef] [PubMed]
- Lyon, G.J.; Coffey, B.J. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 3rd Ed. J. Clin. Psychiatry 2008, 69, 1023. [Google Scholar] [CrossRef]
- Cortese, S.; Brown, T.E.; Corkum, P.; Gruber, R.; O’Brien, L.M.; Stein, M.; Weiss, M.; Owens, J. Assessment and Management of Sleep Problems in Youths with Attention- Deficit/Hyperactivity Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 784–796. [Google Scholar] [CrossRef] [PubMed]
- on behalf of Lombardy ADHD Group; Reale, L.; Bartoli, B.; Cartabia, M.; Zanetti, M.; Costantino, M.A.; Canevini, M.P.; Termine, C.; Bonati, M. Comorbidity Prevalence and Treatment Outcome in Children and Adolescents with ADHD. Eur. Child Adolesc. Psychiatry 2017, 26, 1443–1457. [Google Scholar] [CrossRef]
- Andrade, C. Stahl′s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications. Mens Sana Monogr. 2010, 8, 146. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- DeFilippis, M.; Wagner, K.D. Management of Treatment-Resistant Depression in Children and Adolescents. Paediatr. Drugs 2014, 16, 353–361. [Google Scholar] [CrossRef]
- Goodyer, I.M. Editorial Perspective: Antidepressants and the Depressed Adolescent. Child Adolesc. Ment. Health 2018, 23, 137–140. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.-P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef]
- Amray, A.N.; Munir, K.; Jahan, N.; Motiwala, F.B.; Naveed, S. Psychopharmacology of Pediatric Anxiety Disorders: A Narrative Review. Cureus 2019, 11, e5487. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-Month and Lifetime Prevalence and Lifetime Morbid Risk of Anxiety and Mood Disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, T.P. Depressive Disorders: Treatment Failures and Poor Prognosis over the Last 50 Years. Pharmacol. Res. Perspect. 2019, 7, e00472. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Nanovska, S.; Regen, W.; Spiegelhalder, K.; Feige, B.; Nissen, C.; Reynolds, C.F.; Riemann, D. Sleep and Mental Disorders: A Meta-Analysis of Polysomnographic Research. Psychol. Bull. 2016, 142, 969–990. [Google Scholar] [CrossRef]
- Landmann, N.; Kuhn, M.; Piosczyk, H.; Feige, B.; Baglioni, C.; Spiegelhalder, K.; Frase, L.; Riemann, D.; Sterr, A.; Nissen, C. The Reorganisation of Memory during Sleep. Sleep Med. Rev. 2014, 18, 531–541. [Google Scholar] [CrossRef]
- Landmann, N.; Kuhn, M.; Maier, J.-G.; Spiegelhalder, K.; Baglioni, C.; Frase, L.; Riemann, D.; Sterr, A.; Nissen, C. REM Sleep and Memory Reorganization: Potential Relevance for Psychiatry and Psychotherapy. Neurobiol. Learn. Mem. 2015, 122, 28–40. [Google Scholar] [CrossRef]
- Gordon, A.M.; Chen, S. The Role of Sleep in Interpersonal Conflict: Do Sleepless Nights Mean Worse Fights? Soc. Psychol. Personal. Sci. 2014, 5, 168–175. [Google Scholar] [CrossRef]
- Guadagni, V.; Burles, F.; Ferrara, M.; Iaria, G. The Effects of Sleep Deprivation on Emotional Empathy. J. Sleep Res. 2014, 23, 657–663. [Google Scholar] [CrossRef]
- Harvey, A.G.; Murray, G.; Chandler, R.A.; Soehner, A. Sleep Disturbance as Transdiagnostic: Consideration of Neurobiological Mechanisms. Clin. Psychol. Rev. 2011, 31, 225–235. [Google Scholar] [CrossRef]
- Harvey, A.G. A Transdiagnostic Approach to Treating Sleep Disturbance in Psychiatric Disorders. Cogn. Behav. Ther. 2009, 38 (Suppl. 1), 35–42. [Google Scholar] [CrossRef]
- Marotta, R.; Risoleo, M.C.; Messina, G.; Parisi, L.; Carotenuto, M.; Vetri, L.; Roccella, M. The Neurochemistry of Autism. Brain Sci. 2020, 10, 163. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Beidel, D.C.; Turner, S.M.; Lewin, D.S. Preliminary Evidence for Sleep Complaints among Children Referred for Anxiety. Sleep Med. 2006, 7, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ritvo, E.R.; Ritvo, R.; Yuwiler, A.; Brothers, A.; Freeman, B.J.; Plotkin, S. Elevated Daytime Melatonin Concentrations in Autism: A Pilot Study. Eur. Child Adolesc. Psychiatry 1993, 2, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Laino, D.; D’Alonzo, R.; Mencarelli, A.; Di Genova, L.; Fattorusso, A.; Argentiero, A.; Mencaroni, E. Pediatric Sleep Disturbances and Treatment with Melatonin. J. Transl. Med. 2019, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Lalanne, S.; Fougerou-Leurent, C.; Anderson, G.M.; Schroder, C.M.; Nir, T.; Chokron, S.; Delorme, R.; Claustrat, B.; Bellissant, E.; Kermarrec, S.; et al. Melatonin: From Pharmacokinetics to Clinical Use in Autism Spectrum Disorder. Int. J. Mol. Sci. 2021, 22, 1490. [Google Scholar] [CrossRef] [PubMed]
- Grivas, T.B.; Savvidou, O.D. Melatonin the “Light of Night” in Human Biology and Adolescent Idiopathic Scoliosis. Scoliosis 2007, 2, 6. [Google Scholar] [CrossRef]
- Sadeh, A. Sleep and Melatonin in Infants: A Preliminary Study. Sleep 1997, 20, 185–191. [Google Scholar]
- Rossignol, D.A.; Frye, R.E. Mitochondrial Dysfunction in Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. Mol. Psychiatry 2012, 17, 290–314. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Maes, M. Interactions of Tryptophan and Its Catabolites with Melatonin and the Alpha 7 Nicotinic Receptor in Central Nervous System and Psychiatric Disorders: Role of the Aryl Hydrocarbon Receptor and Direct Mitochondria Regulation. Int. J. Tryptophan Res. IJTR 2017, 10, 1178646917691738. [Google Scholar] [CrossRef] [PubMed]
- Schwarcz, R.; Stone, T.W. The Kynurenine Pathway and the Brain: Challenges, Controversies and Promises. Neuropharmacology 2017, 112, 237–247. [Google Scholar] [CrossRef]
- Fujigaki, H.; Yamamoto, Y.; Saito, K. L-Tryptophan-Kynurenine Pathway Enzymes Are Therapeutic Target for Neuropsychiatric Diseases: Focus on Cell Type Differences. Neuropharmacology 2017, 112, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Wigner, P.; Synowiec, E.; Jóźwiak, P.; Czarny, P.; Bijak, M.; Barszczewska, G.; Białek, K.; Szemraj, J.; Gruca, P.; Papp, M.; et al. The Changes of Expression and Methylation of Genes Involved in Oxidative Stress in Course of Chronic Mild Stress and Antidepressant Therapy with AGM. Genes 2020, 11, 644. [Google Scholar] [CrossRef] [PubMed]
- Wigner, P.; Czarny, P.; Synowiec, E.; Bijak, M.; Talarowska, M.; Galecki, P.; Szemraj, J.; Sliwinski, T. Variation of Genes Encoding KAT1, AADAT and IDO1 as a Potential Risk of Depression Development. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2018, 52, 95–103. [Google Scholar] [CrossRef]
- Anderson, G.; Maes, M. Redox Regulation and the Autistic Spectrum: Role of Tryptophan Catabolites, Immuno-Inflammation, Autoimmunity and the Amygdala. Curr. Neuropharmacol. 2014, 12, 148–167. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.F. Quest for Biomarkers of Treatment-Resistant Depression: Shifting the Paradigm toward Risk. Front. Psychiatry 2013, 4, 57. [Google Scholar] [CrossRef]
- Zhang, X.; Gainetdinov, R.R.; Beaulieu, J.-M.; Sotnikova, T.D.; Burch, L.H.; Williams, R.B.; Schwartz, D.A.; Krishnan, K.R.R.; Caron, M.G. Loss-of-Function Mutation in Tryptophan Hydroxylase-2 Identified in Unipolar Major Depression. Neuron 2005, 45, 11–16. [Google Scholar] [CrossRef]
- Chumboatong, W.; Khamchai, S.; Tocharus, C.; Govitrapong, P.; Tocharus, J. AGM Exerts an Anti-Inflammatory Effect by Inhibiting Microglial Activation Through TLR4/NLRP3 Pathway in PMCAO Rats. Neurotox. Res. 2022, 40, 259–266. [Google Scholar] [CrossRef]
- Cankara, F.N.; Günaydın, C.; Çelik, Z.B.; Şahin, Y.; Pekgöz, Ş.; Erzurumlu, Y.; Gülle, K. AGM Confers Neuroprotection against Cisplatin-Induced Hippocampal Neurotoxicity. Metab. Brain Dis. 2021, 36, 339–349. [Google Scholar] [CrossRef]
- Manda, K.; Reiter, R.J. Melatonin Maintains Adult Hippocampal Neurogenesis and Cognitive Functions after Irradiation. Prog. Neurobiol. 2010, 90, 60–68. [Google Scholar] [CrossRef]
- Markham, A.; Bains, R.; Franklin, P.; Spedding, M. Changes in Mitochondrial Function Are Pivotal in Neurodegenerative and Psychiatric Disorders: How Important Is BDNF? Br. J. Pharmacol. 2014, 171, 2206–2229. [Google Scholar] [CrossRef]
- Sasaki, R.; Kojima, S.; Onishi, H. Do Brain-Derived Neurotrophic Factor Genetic Polymorphisms Modulate the Efficacy of Motor Cortex Plasticity Induced by Non-Invasive Brain Stimulation? A Systematic Review. Front. Hum. Neurosci. 2021, 15, 742373. [Google Scholar] [CrossRef] [PubMed]
- Abellaneda-Pérez, K.; Martin-Trias, P.; Cassé-Perrot, C.; Vaqué-Alcázar, L.; Lanteaume, L.; Solana, E.; Babiloni, C.; Lizio, R.; Junqué, C.; Bargalló, N.; et al. BDNF Val66Met Gene Polymorphism Modulates Brain Activity Following RTMS-Induced Memory Impairment. Sci. Rep. 2022, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Cheeran, B.; Talelli, P.; Mori, F.; Koch, G.; Suppa, A.; Edwards, M.; Houlden, H.; Bhatia, K.; Greenwood, R.; Rothwell, J.C. A Common Polymorphism in the Brain-Derived Neurotrophic Factor Gene (BDNF) Modulates Human Cortical Plasticity and the Response to RTMS. J. Physiol. 2008, 586, 5717–5725. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Ji, Y.-S.; Sun, X.; Liu, X.-H.; Chen, Z.-Y. Brain-Derived Neurotrophic Factor (BDNF)-Induced Mitochondrial Motility Arrest and Presynaptic Docking Contribute to BDNF- Enhanced Synaptic Transmission. J. Biol. Chem. 2014, 289, 1213–1226. [Google Scholar] [CrossRef]
- Penrod, R.D.; Kumar, J.; Smith, L.N.; McCalley, D.; Nentwig, T.B.; Hughes, B.W.; Barry, G.M.; Glover, K.; Taniguchi, M.; Cowan, C.W. Activity-regulated cytoskeleton-associated protein (Arc/Arg3.1) regulates anxiety- and novelty-related behaviors. Genes Brain Behavior. 2019, 18, e12561. [Google Scholar] [CrossRef]
- Lim, C.K.; Essa, M.M.; de Paula Martins, R.; Lovejoy, D.B.; Bilgin, A.A.; Waly, M.I.; Al-Farsi, Y.M.; Al-Sharbati, M.; Al-Shaffae, M.A.; Guillemin, G.J. Altered Kynurenine Pathway Metabolism in Autism: Implication for Immune-Induced Glutamatergic Activity: Altered Kynurenine Pathway Metabolism in ASD. Autism Res. 2016, 9, 621–631. [Google Scholar] [CrossRef]
- Musazzi, L.; Racagni, G.; Popoli, M. Stress, Glucocorticoids and Glutamate Release: Effects of Antidepressant Drugs. Neurochem. Int. 2011, 59, 138–149. [Google Scholar] [CrossRef]
- Casanova, M.F.; Shaban, M.; Ghazal, M.; El-Baz, A.S.; Casanova, E.L.; Sokhadze, E.M. Ringing Decay of Gamma Oscillations and Transcranial Magnetic Stimulation Therapy in Autism Spectrum Disorder. Appl. Psychophysiol. Biofeedback 2021, 46, 161–173. [Google Scholar] [CrossRef]
- Sonmez, A.I.; Almorsy, A.; Ramsey, L.B.; Strawn, J.R.; Croarkin, P.E. Novel Pharmacological Treatments for Generalized Anxiety Disorder: Pediatric Considerations. Depress. Anxiety 2020, 37, 747–759. [Google Scholar] [CrossRef]
- Harvey, B.H.; Regenass, W.; Dreyer, W.; Möller, M. Social Isolation Rearing-Induced Anxiety and Response to AGM in Male and Female Rats: Role of Corticosterone, Oxytocin, and Vasopressin. J. Psychopharmacol. Oxf. Engl. 2019, 33, 640–646. [Google Scholar] [CrossRef]
- McClung, C.A. How Might Circadian Rhythms Control Mood? Let Me Count the Ways. Biol. Psychiatry 2013, 74, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Floden, D.; Vallesi, A.; Stuss, D.T. Task Context and Frontal Lobe Activation in the Stroop Task. J. Cogn. Neurosci. 2011, 23, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Koresh, O.; Kozlovsky, N.; Kaplan, Z.; Zohar, J.; Matar, M.A.; Cohen, H. The Long-Term Abnormalities in Circadian Expression of Period 1 and Period 2 Genes in Response to Stress Is Normalized by AGM Administered Immediately after Exposure. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2012, 22, 205–221. [Google Scholar] [CrossRef] [PubMed]
- Coull, J.T.; Frith, C.D.; Büchel, C.; Nobre, A.C. Orienting Attention in Time: Behavioural and Neuroanatomical Distinction between Exogenous and Endogenous Shifts. Neuropsychologia 2000, 38, 808–819. [Google Scholar] [CrossRef]
- Davidson, R.J.; Pizzagalli, D.; Nitschke, J.B.; Putnam, K. Depression: Perspectives from Affective Neuroscience. Annu. Rev. Psychol. 2002, 53, 545–574. [Google Scholar] [CrossRef]
- Casey, B.J.; Castellanos, F.X.; Giedd, J.N.; Marsh, W.L.; Hamburger, S.D.; Schubert, A.B.; Vauss, Y.C.; Vaituzis, A.C.; Dickstein, D.P.; Sarfatti, S.E.; et al. Implication of Right Frontostriatal Circuitry in Response Inhibition and Attention-Deficit/Hyperactivity Disorder. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 374–383. [Google Scholar] [CrossRef]
- Castellanos, F.X.; Giedd, J.N.; Marsh, W.L.; Hamburger, S.D.; Vaituzis, A.C.; Dickstein, D.P.; Sarfatti, S.E.; Vauss, Y.C.; Snell, J.W.; Lange, N.; et al. Quantitative Brain Magnetic Resonance Imaging in Attention- Deficit Hyperactivity Disorder. Arch. Gen. Psychiatry 1996, 53, 607–616. [Google Scholar] [CrossRef]
- Filipek, P.A.; Semrud-Clikeman, M.; Steingard, R.J.; Renshaw, P.F.; Kennedy, D.N.; Biederman, J. Volumetric MRI Analysis Comparing Subjects Having Attention-Deficit Hyperactivity Disorder with Normal Controls. Neurology 1997, 48, 589–601. [Google Scholar] [CrossRef]
- Mataró, M.; Garcia-Sánchez, C.; Junqué, C.; Estévez-González, A.; Pujol, J. Magnetic Resonance Imaging Measurement of the Caudate Nucleus in Adolescents with Attention-Deficit Hyperactivity Disorder and Its Relationship with Neuropsychological and Behavioral Measures. Arch. Neurol. 1997, 54, 963–968. [Google Scholar] [CrossRef]
- Silberstein, R.B.; Farrow, M.; Levy, F.; Pipingas, A.; Hay, D.A.; Jarman, F.C. Functional Brain Electrical Activity Mapping in Boys with Attention-Deficit/Hyperactivity Disorder. Arch. Gen. Psychiatry 1998, 55, 1105–1112. [Google Scholar] [CrossRef]
- Cheng, W.; Rolls, E.T.; Gu, H.; Zhang, J.; Feng, J. Autism: Reduced Connectivity between Cortical Areas Involved in Face Expression, Theory of Mind, and the Sense of Self. Brain J. Neurol. 2015, 138 Pt 5, 1382–1393. [Google Scholar] [CrossRef]
- Kosaka, H.; Omori, M.; Munesue, T.; Ishitobi, M.; Matsumura, Y.; Takahashi, T.; Narita, K.; Murata, T.; Saito, D.N.; Uchiyama, H.; et al. Smaller Insula and Inferior Frontal Volumes in Young Adults with Pervasive Developmental Disorders. NeuroImage 2010, 50, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Casanova, M.F.; Sokhadze, E.; Opris, I.; Wang, Y.; Li, X. Autism Spectrum Disorders: Linking Neuropathological Findings to Treatment with Transcranial Magnetic Stimulation. Acta Paediatr. Oslo Nor. 1992 2015, 104, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Bauman, M.L.; Kemper, T.L. Neuroanatomic Observations of the Brain in Autism: A Review and Future Directions. Int. J. Dev. Neurosci. Off. J. Int. Soc. Dev. Neurosci. 2005, 23, 183–187. [Google Scholar] [CrossRef]
- Niederhofer, H. Treating ADHD with AGM. J. Atten. Disord. 2012, 16, 346–348. [Google Scholar] [CrossRef]
- Sara, S.J. The Locus Coeruleus and Noradrenergic Modulation of Cognition. Nat. Rev. Neurosci. 2009, 10, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Hou, Y.; Shen, J.; Huang, Y.; Martin, W.; Cheng, F. Network-Based Drug Repurposing for Novel Coronavirus 2019-NCoV/SARS-CoV-2. Cell Discov. 2020, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.A.; Hennig, A.; Martino, D. Relationship between COVID 19 and Movement Disorders: A Narrative Review. Eur. J. Neurol. 2021, 29, 1243–1253. [Google Scholar] [CrossRef]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in Influenza, COVID-19, and Other Viral Infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
- Yadalam, P.K.; Balaji, T.M.; Varadarajan, S.; Alzahrani, K.J.; Al-Ghamdi, M.S.; Baeshen, H.A.; Alfarhan, M.F.A.; Khurshid, Z.; Bhandi, S.; Jagannathan, R.; et al. Assessing the Therapeutic Potential of AGM, Ramelteon, and Melatonin against SARS-CoV-2. Saudi J. Biol. Sci. 2022, 29, 3140–3150. [Google Scholar] [CrossRef]
- Feitosa, E.L.; Júnior, F.T.D.S.S.; Nery Neto, J.A.D.O.; Matos, L.F.L.; Moura, M.H.D.S.; Rosales, T.O.; De Freitas, G.B.L. COVID-19: Rational Discovery of the Therapeutic Potential of Melatonin as a SARS-CoV-2 Main Protease Inhibitor. Int. J. Med. Sci. 2020, 17, 2133–2146. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-Converting Enzyme 2 Is a Functional Receptor for the SARS Coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Lan, J.; Ge, J.; Yu, J.; Shan, S.; Zhou, H.; Fan, S.; Zhang, Q.; Shi, X.; Wang, Q.; Zhang, L.; et al. Structure of the SARS-CoV-2 Spike Receptor-Binding Domain Bound to the ACE2 Receptor. Nature 2020, 581, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Cecon, E.; Izabelle, C.; Poder, S.L.; Real, F.; Zhu, A.; Tu, L.; Ghigna, M.R.; Klonjkowski, B.; Bomsel, M.; Jockers, R.; et al. Therapeutic Potential of Melatonin and Melatonergic Drugs on K18 HACE2 Mice Infected with SARS-CoV-2. J. Pineal Res. 2022, 72, e12772. [Google Scholar] [CrossRef] [PubMed]
- Brusco, L.I.; Cruz, P.; Cangas, A.V.; Rojas, C.G.; Vigo, D.E.; Cardinali, D.P. Efficacy of Melatonin in Non-Intensive Care Unit Patients with COVID-19 Pneumonia and Sleep Dysregulation. Melatonin Res. 2021, 4, 173–188. [Google Scholar] [CrossRef]
- Savino, R.; Polito, A.N.; Arcidiacono, G.; Poliseno, M.; Lo Caputo, S. Neuropsychiatric Disorders in Pediatric Long COVID-19: A Case Series. Brain Sci. 2022, 12, 514. [Google Scholar] [CrossRef]
- de Sousa Moreira, J.L.; Barbosa, S.M.B.; Vieira, J.G.; Chaves, N.C.B.; Felix, E.B.G.; Feitosa, P.W.G.; da Cruz, I.S.; da Silva, C.G.L.; Neto, M.L.R. The Psychiatric and Neuropsychiatric Repercussions Associated with Severe Infections of COVID-19 and Other Coronaviruses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110159. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).