

Role of Immersive Virtual Reality in Motor Behaviour Decision-Making in Chronic Pain Patients
 , and
, and 
Abstract
1. Introduction
An Introductory Review to VR Effects on Chronic Pain
2. Immersive Virtual Reality as a Medium for Altering Sensorimotor Decision-Making in Chronic Pain Patients: A Neurophysiological Hypothesis
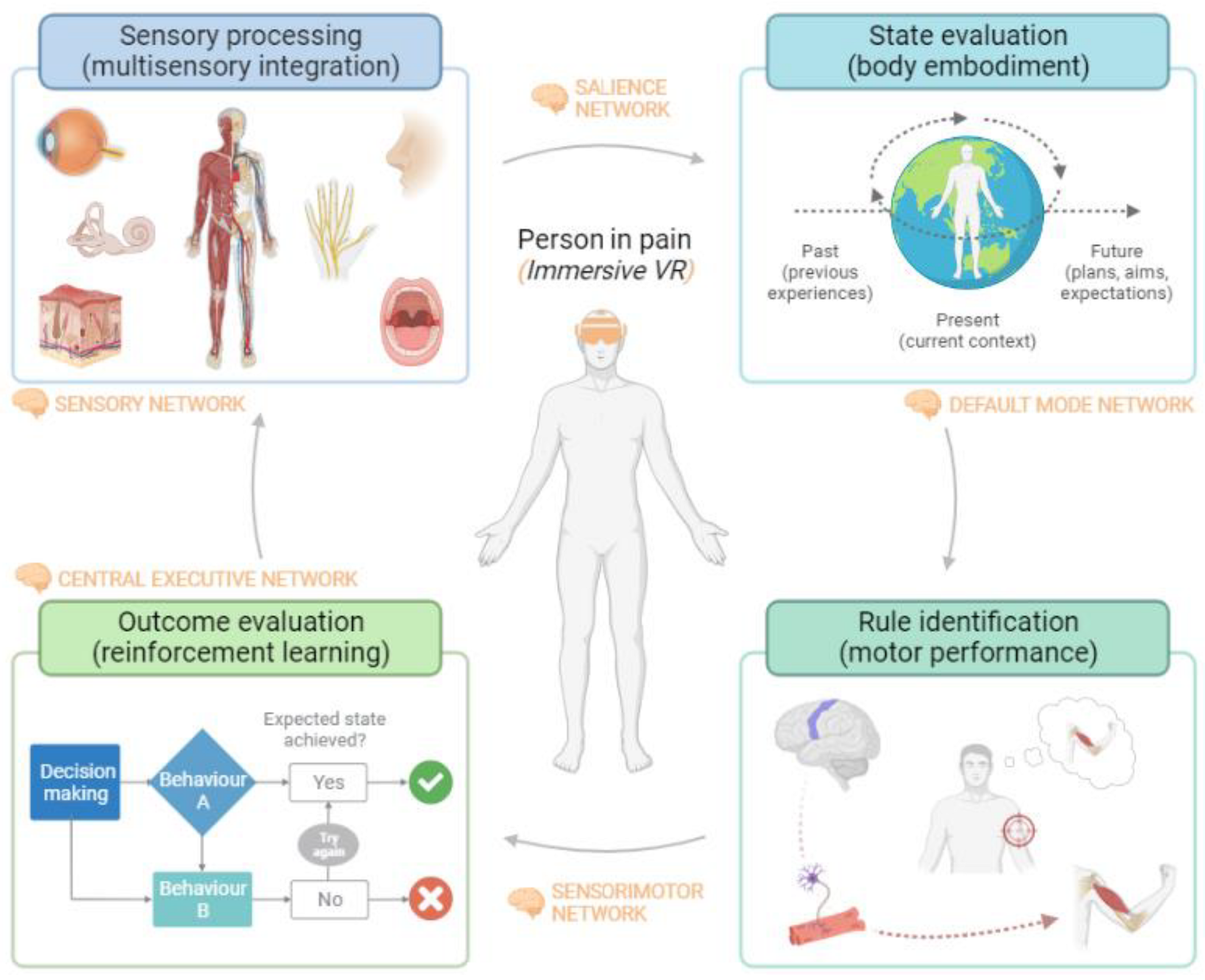
- New visual and auditory information provided by immersive virtual reality is integrated with other sensory stimuli and reaches the sensory cortex, which is associated with the first threat evaluation (sensory network) [30]. Activation of the sensory pathways triggers activation of the amygdala and insula, which are associated with the valence of the stimulus and the distress experienced by the person (salience network) [31].
- A change in the afferent sensory information can impact the current state evaluation of the environment and body image (the default mode network) [32]. This could modulate the bidirectional and inversely related link between the saliency network and the default mode network, allowing body image to be influenced by full-body virtual avatars.
- If the virtual environment is safe enough and does not present cues of threat, goal-directed motor commands will be activated instead of protective/defensive behaviors (sensorimotor network) [33]. That is particularly necessary in people with chronic pain, where altered motor behavior is common.
- Moving a person in pain in a safe environment can stimulate downward modulation of pain and promote analgesia [34]. Breaking the negative expectation of pain during movement can facilitate the extinction of fear memories acquired through contextual fear conditioning (the central executive network) [35,36]. The maintenance of this non-threatening environment could replace the fear memory with a new safety memory related to movement. This framework suggests that VR could be a potential tool to produce motor relearning in the context of pain [37].

2.1. Multisensory Integration Alterations in People with Chronic Pain
How VR Can Improve Multisensory Processing
2.2. Body Perception Disturbance in Chronic Pain Patients
How VR May Impact Body Embodiment
2.3. Pain-Related Movement Dysfunctions
How VR May Enhance Sensorimotor Performance
2.4. Threat Learning in Chronic Pain
How VR Can Induce Motor Reinforcement Learning
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Evidence Review of VR in Chronic Pain
| Review | Focus of Review | Study Details Number (N) Year Target Population | Methods Database Outcomes QoE | Main Findings | Limitations |
| Goudmann et al. [19] | Evaluate the effect of VR on several outcome parameters related to the application of VR in patients with chronic pain | 2022 N Studies = 41 N participants = 1232 Chronic pain (Fibromyalgia, Low back pain, neck pain, upper limb complex regional pain syndrome and phantom limb pain) | 4 Database Risk of bias varied between 8 out of 28 and 25 out of 28 Data from 25 studies were included in the meta-analysis Pain-related Outcomes kinesiophobia and fear, mood, satisfaction, expectations of pain, pain focus, time spent thinking about pain, self-efficacy, emotions, motivation, stress, catastrophizing, acceptability, global impression of change, ownership, and agency Functional outcomes Functional capacity Mobility Neuropsychological functions Experience of VR technology | A total of 23 studies used immersive VR techniques, and 18 used non-immersive techniques. VR intervention in patients with chronic pain had a positive effect on decrease pain, increase mobility and functional capacity. Overall effect of VR on several outcome measurements is not moderated by the type of VR intervention, type of pain or the objective of VR. | None of the included studies qualified for excellent methodological quality. Much heterogeneity is present in studies with VR methodology Authors mainly focused on the primary outcome variables and secondary outcomes were not always described in full detail an asymmetrical plot in experience of VR technology outcomes, which might be interpreted as an indication of publication bias. |
| Wittkopf et al. [145] | Evaluate the effect of immersive and non-immersive interactive VR on pain perception in patients with a clinical pain condition. | 2019 N Studies = 13 N participants = 469 Chronic pain (Low back pain, neck pain, neuropathic pain, phantom limb pain, ankylosing spondylitis, subacromial impingement syndrome and post-mastectomy) | 5 databases High risk of bias and small sample sizes. A meta-analysis could not be conducted due to differences in study designs and types of controls. Pain-related Outcomes were included | A total of 5 studies used immersive VR techniques, and 8 used non-immersive techniques. No difference in efficacy in immersive or non-immersive VR intervention. Interactive VRmay reduce pain | High risk of bias and small sample sizes on studies included Much heterogeneity in VR methodology (type, frequency, and duration of VR treatment) |
| Grassini [146] | Assessment of the efficacy of the use of VR for chronic pain management | 2022 N Studies = 9 N participants = 524 Chronic pain (Low back pain and neck pain) | 6 databases Low risk of bias and small sample sizes. A meta-analysis could not be conducted due to differences in study designs and types of controls. Pain-related Outcomes Tampa Scale for kinesiophobia (TSK) pain intensity Oswestry dysfunction index (ODI) neck disability index (NDI) were included | VR interventions may be useful for chronic pain management but was not superior to other types of interventions VR could be effective on NDI but no in RMD an TSK | Small number of included studies High heterogeneity was present in most of the outcomes No information about type of VR information A single author has conducted this study |
| Brea-Gómez et al. [147] | Analyze the effectiveness of VR in chronic low back pain. | 2021 N Studies = 14 N participants = 765 Chronic pain (Low back pain) | 4 databases Risk of bias varied between 13-27 out 28. Data from 11 studies were included in the meta-analysis Pain-related Outcomes Tampa Scale for kinesiophobia (TSK) Disability Questionnaire (RMDQ) Oswestry dysfunction index (ODI) 10-item Pain Self- Efficacy (10-PSEQ) Pain Catastrophizing Scale (PCS) isokinetic trunk flexion/extension with a dynamometer blood serum levels of stress hormones were included | A total of 2 studies used immersive VR techniques, and 12 used non-immersive techniques. VR can significantly reduce pain intensity and kinesiophobia in patients with chronic low back pain No significant differences were found in disability postintervention. | High heterogeneity between included Differences in the age ranges and in the clinical profile of the participants Small sample sizes on studies included High heterogeneity in VR methodology (type, frequency, and duration of VR treatment) |
| Gava et al. [136] | Analyze the current evidence regarding the use of games and virtual reality to improve mental health-related outcomes in patients with chronic musculoskeletal pain. | 2022 N Studies = 13 N participants = 680 Chronic musculoskeletal pain (back, neck, and shoulder pain; osteoarthritis; fibromyalgia) | 6 Database Risk of bias varied between 8 out of 28 and 25 out of 28 Data from 13 studies were included in the meta-analysis Pain-related Outcomes Fear-Avoidance Beliefs Questionnaire (FABQ) Tampa Kinesiophobia Scale (TSK) The Pain Catastrophizing Scale (PCS) Pain Anxiety Symptoms Scale Hospital Anxiety and Depression Scale | A total of 7 studies used immersive VR techniques, and 5 used non-immersive techniques (Exergames) VR intervention in patients with chronic musculoskeletal Pain are superior to other treatments to improve pain-related fear and superior to no treatment to improve anxiety. Gaming was not superior to other treatments or no treatment for improving pain catastrophizing, anxiety, and depression. | Very low or low quality of evidence of studies included Much heterogeneity is present in studies with VR gaming methodology (type, frequency, and duration of VR treatment) Publication bias was not assessed due to the limited number of included Studies. |
| Ahern et al. [148] | Evaluate effectiveness of VR technology in the management of individuals with acute, subacute, and chronic spinal pain. | 2020 N Studies = 7 N participants = 469 Spinal Chronic pain (neck pain, thoracic pain, or low back pain [LBP]) | 5 databases All 7 of the studies included had a high risk of bias Data from 2 studies were included in the meta-analysis Pain intensity Disability specific function, general health status, future visits to healthcare professionals, return to work, patient satisfaction, adverse events, global perceived effect (GPE), balance, and fear of movement. were included | A total of 1 studies used immersive VR techniques, and 6 used non-immersive techniques. The effect of VR ranged from no statistical significance to clinical significance, depending on the area of the spine being treated, the follow-up period being assessed, and the type of VR used. Difference in effect between VR and other included interventions was often small and not clinically significant higher-quality research on efficacy and effectiveness of VR is needed | The review was limited by the low number of included studies Young population in studies included, results may not be applicable to younger or older populations. Much heterogeneity in VR methodology (type, frequency, and duration of VR treatment) |
| Mallari et al. [149] | Compare the effectiveness of VR in reducing acute and chronic pain in adults. | 2019 N Studies = 20 N participants = No info Chronic pain (Musculoskeletal pain conditions (MSKP), four in neuropathic pain conditions (NP), one in a mixture of musculoskeletal and neuropathic pain conditions (MSKP-NP) and two in an unspecified pain condition (UnP). | 3 databases All chronic pain studies had fair to high quality assessment ratings. Data from 3 studies were included in the meta-analysis Pain-related Outcomes Range of motion (ROM), strength, function, balance, and gait | A total of 18 studies used immersive VR techniques, and 2 used non-immersive techniques. VR is an effective tool in reducing chronic pain, specially while the patient is immersed in the VR environment Further research is needed to assess the extent to which one needs to be immersed and present in a virtual environment in order to reduce pain, and the dosage necessary to maintain pain reductions in chronic pain over time. | Significant heterogeneity in study population and pain conditions Much heterogeneity in VR methodology (type, frequency, and duration of VR treatment) |
| Gumaa et al. [150] | Analyze the effectiveness of VR in chronic low back pain. | 2019 N Studies = 19 N participants = 765 Chronic pain (fibromyalgia, rheumatoid arthritis, Musculoskeletal pain conditions) | 5 databases Quality Assessment varied between 22–37 out 48. Data from 3 studies were included in the meta-analysis Pain-related Outcomes Functional outcomes Functional capacity Mobility | Evidence of VR effectiveness in individuals with chronic neck pain and shoulder impingement syndrome is promising For fibromyalgia, total knee arthroplasty, and back pain, the evidence of VR effectiveness compared with more traditional exercise is absent or inconclusive | Studies assessed psychosocial outcomes were excluded Heterogeneity in VR and physical therapist interventions as well as outcome measures Small sample sizes on studies included High heterogeneity in VR methodology (type, frequency, and duration of VR treatment) |
| Virtual Reality (VR); Tampa Scale for kinesiophobia (TSK); Oswestry dysfunction index (ODI); neck disability index (NDI); Roland Morris Disability Questionnaire (RMDQ); 10-item Pain Self-Efficacy (10-PSEQ); Pain Catastrophizing Scale (PCS); low back pain (LBP); Musculoskeletal pain conditions (MSKP); neuropathic pain conditions (NP); Range of motion (ROM). | |||||
References
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.; Vlaeyen, J.W.S.; Rief, W.; Barke, A.; Aziz, Q.; Benoliel, R.; Cohen, M.; Evers, S.; Giamberardino, M.A.; Goebel, A.; et al. The IASP classification of chronic pain for ICD-11: Chronic primary pain. Pain 2019, 160, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Haslbeck, J.M.B.; Sjouwerman, R.; Peters, M.L. Towards a dynamic account of chronic pain. Pain 2022, 163, E1038–E1039. [Google Scholar] [CrossRef]
- Ilundáin-Agurruza, J. Relational Pain: The Perspective from the Other Side of the Lens. Constr. Found. 2022, 17, 152–154. [Google Scholar]
- Tabor, A.; Van Ryckeghem, D.M.L.; Hasenbring, M.I. Pain Unstuck: The Role of Action and Motivation. Clin. J. Pain 2020, 36, 143–149. [Google Scholar] [CrossRef]
- Eccleston, C. Chronic pain as embodied defence: Implications for current and future psychological treatments. Pain 2018, 159, S17–S23. [Google Scholar] [CrossRef]
- Stilwell, P.; Harman, K. An enactive approach to pain: Beyond the biopsychosocial model. Phenomenol. Cogn. Sci. 2019, 18, 637–665. [Google Scholar] [CrossRef]
- Miyahara, K. Enactive pain and its sociocultural embeddedness. Phenomenol. Cogn. Sci. 2021, 20, 871–886. [Google Scholar] [CrossRef]
- Jones, M.; Edwards, I.; Gifford, L. Conceptual models for implementing biopsychosocial theory in clinical practice. Man Ther. 2002, 7, 2–9. [Google Scholar] [CrossRef]
- De Ridder, D.; Vanneste, S.; Smith, M.; Adhia, D. Pain and the Triple Network Model. Front. Neurol. 2022, 13, 272. [Google Scholar] [CrossRef] [PubMed]
- Georgeon, O.L.; Marshall, J.B.; Manzotti, R. ECA: An enactivist cognitive architecture based on sensorimotor modeling. Biol. Inspired. Cogn. Archit. 2013, 6, 46–57. [Google Scholar] [CrossRef]
- Kiverstein, J.; Kirchhoff, M.D.; Thacker, M. An Embodied Predictive Processing Theory of Pain Experience. Rev. Philos. Psychol. 2022, 13, 973–998. [Google Scholar] [CrossRef]
- Cormack, B.; Stilwell, P.; Coninx, S.; Gibson, J. The biopsychosocial model is lost in translation: From misrepresentation to an enactive modernization. Physiother. Theory Pract. 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Smrdu, M. Kaleidoscope of Pain: What and How Do You See Through It. Constr. Found. 2022, 17, 136–147. [Google Scholar]
- Levin, M.F.; Weiss, P.L.; Keshner, E.A.; Levin, M.F.; Weiss, P.L.; Keshner, E.A. Emergence of Virtual Reality as a Tool for Upper Limb Rehabilitation: Incorporation of Motor Control and Motor Learning Principles. Phys. Ther. 2015, 95, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Hutting, N.; Caneiro, J.P.; Ong’wen, O.M.; Miciak, M.; Roberts, L. Patient-centered care in musculoskeletal practice: Key elements to support clinicians to focus on the person. Musculoskelet. Sci. Pract. 2022, 57, 102434. [Google Scholar] [CrossRef]
- Trost, Z.; France, C.; Anam, M.; Shum, C. Virtual reality approaches to pain: Toward a state of the science. Pain 2021, 162, 325–331. [Google Scholar] [CrossRef]
- Goudman, L.; Jansen, J.; Billot, M.; Vets, N.; De Smedt, A.; Roulaud, M.; Rigoard, P.; Moens, M. Virtual Reality Applications in Chronic Pain Management: Systematic Review and Meta-analysis. JMIR Serious Games 2022, 10, e34402. [Google Scholar] [CrossRef]
- Slater, M. Immersion and the illusion of presence in virtual reality. Br. J. Psychol. 2018, 109, 431–433. [Google Scholar] [CrossRef]
- Harvie, D.S.; Smith, R.T.; Martin, D.; Hirsh, A.T.; Trost, Z. Editorial: Novel applications of virtual and mixed reality in pain research and treatment. Front. Virtual Real. 2022, 3, 142. [Google Scholar] [CrossRef]
- Austin, P.D. The Analgesic Effects of Virtual Reality for People with Chronic Pain: A Scoping Review. Pain Med. 2022, 23, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Keefe, F.J.; Huling, D.A.; Coggins, M.J.; Keefe, D.F.; Zachary Rosenthal, M.; Herr, N.R.; Hoffman, H.G. Virtual reality for persistent pain: A new direction for behavioral pain management. Pain 2012, 153, 2163–2166. [Google Scholar] [CrossRef] [PubMed]
- Simón-Vicente, L.; Rodríguez-Cano, S.; Delgado-Benito, V.; Ausín-Villaverde, V.; Cubo Delgado, E. Cybersickness. A systematic literature review of adverse effects related to virtual reality. Neurología 2022, in press. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors associated with virtual reality sickness in head-mounted displays: A systematic review and meta-analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and cybersickness in virtual reality are negatively related: A review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Indovina, P.; Barone, D.; Gallo, L.; Chirico, A.; de Pietro, G.; Giordano, A. Virtual Reality as a Distraction Intervention to Relieve Pain and Distress During Medical Procedures. Clin. J. Pain 2018, 34, 858–877. [Google Scholar] [CrossRef]
- La Touche, R. Introduciendo la dimensión motora dentro de la conceptualización de la experiencia del dolor. J. MOVE Ther. Sci. 2021, 3, 269–277. [Google Scholar] [CrossRef]
- Brady, N.; McVeigh, J.G.; McCreesh, K.; Rio, E.; Dekkers, T.; Lewis, J.S. Exploring the effectiveness of immersive Virtual Reality interventions in the management of musculoskeletal pain: A state-of-the-art review. Phys. Ther. Rev. 2021, 26, 262–275. [Google Scholar] [CrossRef]
- Kim, J.; Mawla, I.; Kong, J.; Lee, J.; Gerber, J.; Ortiz, A.; Kim, H.; Chan, S.-T.; Loggia, M.L.; Wasan, A.D.; et al. Somatotopically-specific primary somatosensory connectivity to salience and default mode networks encodes clinical pain. Pain 2019, 160, 1594. [Google Scholar] [CrossRef]
- De Ridder, D.; Adhia, D.; Vanneste, S. The anatomy of pain and suffering in the brain and its clinical implications. Neurosci. Biobehav. Rev. 2021, 130, 125–146. [Google Scholar] [CrossRef] [PubMed]
- Baliki, M.N.; Mansour, A.R.; Baria, A.T.; Apkarian, A.V. Functional reorganization of the default mode network across chronic pain conditions. PLoS ONE 2014, 9, e106133. [Google Scholar] [CrossRef] [PubMed]
- Gombaut, C.; Holmes, S.A. Sensorimotor Integration and Pain Perception: Mechanisms Integrating Nociceptive Processing. A Systematic Review and ALE-Meta Analysis. Front. Integr. Neurosci. 2022, 16, 1–12. [Google Scholar] [CrossRef]
- Colloca, L.; Raghuraman, N.; Wang, Y.; Akintola, T.; Brawn-Cinani, B.; Colloca, G.C.; Kier, C.; Varshney, A.; Murthi, S. Virtual reality: Physiological and behavioral mechanisms to increase individual pain tolerance limits. Pain 2020, 161, 2010. [Google Scholar] [CrossRef]
- Meulders, A. From fear of movement-related pain and avoidance to chronic pain disability: A state-of-the-art review. Curr. Opin. Behav. Sci. 2019, 26, 130–136. [Google Scholar] [CrossRef]
- Den Hollander, M.; Smeets, R.J.E.M.; Van Meulenbroek, T.; Van Laake-Geelen, C.C.M.; Baadjou, V.A.; Timmers, I. Exposure in Vivo as a Treatment Approach to Target Pain-Related Fear: Theory and New Insights From Research and Clinical Practice. Phys. Ther. 2022, 102, pzab270. [Google Scholar] [CrossRef]
- Boudreau, S.A.; Farina, D.; Falla, D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Man. Ther. 2010, 15, 410–414. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Vanneste, S.; Freeman, W. The Bayesian brain: Phantom percepts resolve sensory uncertainty. Neurosci. Biobehav. Rev. 2014, 44, 4–15. [Google Scholar] [CrossRef]
- Orbán, G.; Wolpert, D.M. Representations of uncertainty in sensorimotor control. Curr. Opin. Neurobiol. 2011, 21, 629–635. [Google Scholar] [CrossRef]
- Bach, D.R.; Dolan, R.J. Knowing how much you don’t know: A neural organization of uncertainty estimates. Nat. Rev. Neurosci. 2012, 13, 572–586. [Google Scholar] [CrossRef]
- Sündermann, O.; Flink, I.; Linton, S.J. My body is not working right: A cognitive behavioral model of body image and chronic pain. Pain 2020, 161, 1136–1139. [Google Scholar] [CrossRef] [PubMed]
- Talsma, D.; Senkowski, D.; Soto-Faraco, S.; Woldorff, M.G. The multifaceted interplay between attention and multisensory integration. Trends Cogn. Sci. 2010, 14, 400–410. [Google Scholar] [CrossRef]
- Kirsch, W.; Kunde, W. On the Role of Interoception in Body and Object Perception: A Multisensory-Integration Account. Perspect. Psychol. Sci. 2022, 18, 321–339. [Google Scholar] [CrossRef] [PubMed]
- Senkowski, D.; Höfle, M.; Engel, A.K. Crossmodal shaping of pain: A multisensory approach to nociception. Trends Cogn. Sci. 2014, 18, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Viceconti, A.; Camerone, E.M.; Luzzi, D.; Pentassuglia, D.; Pardini, M.; Ristori, D.; Rossettini, G.; Gallace, A.; Longo, M.R.; Testa, M. Explicit and implicit Own’s body and space perception in painful musculoskeletal disorders and rheumatic diseases: A systematic scoping review. Front. Hum. Neurosci. 2020, 14, 83. [Google Scholar] [CrossRef]
- Brumagne, S.; Diers, M.; Danneels, L.; Lorimer Moseley, G.; Hodges, P.W. Neuroplasticity of Sensorimotor Control in Low Back Pain. J. Orthop. Sport. Phys. 2019, 49, 402–414. [Google Scholar] [CrossRef]
- Barbosa, A.M.; José-Jandre dos Reis, F.; Caseiro, M.; Barbero, M.; Falla, D.; Siriani de Oliveira, A. Clinical evaluation of somatosensory integrity in people with chronic shoulder pain. Musculoskelet. Sci. Pract. 2021, 53, 102364. [Google Scholar] [CrossRef]
- Catley, M.J.; O’Connell, N.E.; Berryman, C.; Ayhan, F.F.; Moseley, G.L. Is tactile acuity altered in people with chronic pain? A systematic review and meta-analysis. J. Pain 2014, 15, 985–1000. [Google Scholar] [CrossRef]
- Vittersø, A.D.; Halicka, M.; Buckingham, G.; Proulx, M.J.; Bultitude, J.H. The sensorimotor theory of pathological pain revisited. Neurosci. Biobehav. Rev. 2022, 139, 104735. [Google Scholar] [CrossRef]
- Jenkins, L.C.; Chang, W.J.; Buscemi, V.; Liston, M.; Skippen, P.; Cashin, A.G.; McAuley, J.H.; Schabrun, S.M. Low Somatosensory Cortex Excitability in the Acute Stage of Low Back Pain Causes Chronic Pain. J. Pain 2022, 23, 289–304. [Google Scholar] [CrossRef]
- Don, S.; Voogt, L.; Meeus, M.; De Kooning, M.; Nijs, J. Sensorimotor Incongruence in People with Musculoskeletal Pain: A Systematic Review. Pain Pract. 2017, 17, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Flor, H. Targeting cortical representations in the treatment of chronic pain: A review. Neurorehabil. Neural. Repair 2012, 26, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Bushnell, M.C.; Čeko, M.; Low, L.A. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef]
- Reddan, M.C.; Wager, T.D. Brain systems at the intersection of chronic pain and self-regulation. Neurosci. Lett. 2019, 702, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Luque-Suarez, A. Which Psychological Factors Are Involved in the Onset and/or Persistence of Musculoskeletal Pain? An Umbrella Review of Systematic Reviews and Meta-Analyses of Prospective Cohort Studies. Clin. J. Pain 2020, 36, 626–637. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Matias-Soto, J.; Luque-Suarez, A. “My Pain Is Unbearable…I Cannot Recognize Myself!” Emotions, Cognitions, and Behaviors of People Living With Musculoskeletal Disorders: An Umbrella Review. J. Orthop. Sport. Phys. Ther. 2022, 52, 243–261. [Google Scholar] [CrossRef]
- Ahmadpour, N.; Randall, H.; Choksi, H.; Gao, A.; Vaughan, C.; Poronnik, P. Virtual Reality interventions for acute and chronic pain management. Int. J. Biochem. Cell Biol. 2019, 114, 105568. [Google Scholar] [CrossRef]
- Barcatta, K.; Holl, E.; Battistutta, L.; van der Meulen, M.; Rischer, K.M. When Less Is More: Investigating Factors Influencing the Distraction Effect of Virtual Reality From Pain. Front. Pain Res. 2022, 2, 126. [Google Scholar] [CrossRef]
- Press, C.; Taylor-Clarke, M.; Kennett, S.; Haggard, P. Visual enhancement of touch in spatial body representation. Exp. Brain Res. 2004, 154, 238–245. [Google Scholar] [CrossRef]
- Haggard, P.; Taylor-Clarke, M.; Kennett, S. Tactile perception, cortical representation and the bodily self. Curr. Biol. 2003, 13, R170–R173. [Google Scholar] [CrossRef]
- Longo, M.R.; Betti, V.; Aglioti, S.M.; Haggard, P. Visually induced analgesia: Seeing the body reduces pain. J. Neurosci. 2009, 29, 12125–12130. [Google Scholar] [CrossRef] [PubMed]
- Longo, M.R.; Iannetti, G.D.; Mancini, F.; Driver, J.; Haggard, P. Linking Pain and the Body: Neural Correlates of Visually Induced Analgesia. J. Neurosci. 2012, 32, 2601. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Richards, T.L.; Bills, A.R.; Van Oostrom, T.; Magula, J.; Seibel, E.J.; Sharar, S.R. Using FMRI to study the neural correlates of virtual reality analgesia. CNS Spectr. 2006, 11, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.I.; Belmont, K.A.; Thomas, D.A. The neurobiology of virtual reality pain attenuation. Cyberpsychol. Behav. 2007, 10, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Huynh, V.; Bekrater-Bodmann, R.; Fröhner, J.; Vogt, J.; Beckerle, P. Robotic hand illusion with tactile feedback: Unravelling the relative contribution of visuotactile and visuomotor input to the representation of body parts in space. PLoS ONE 2019, 14, e0210058. [Google Scholar] [CrossRef]
- Christ, O.; Reiner, M. Perspectives and possible applications of the rubber hand and virtual hand illusion in non-invasive rehabilitation: Technological improvements and their consequences. Neurosci. Biobehav. Rev. 2014, 44, 33–44. [Google Scholar] [CrossRef]
- Kokkinara, E.; Slater, M. Measuring the Effects through Time of the Influence of Visuomotor and Visuotactile Synchronous Stimulation on a Virtual Body Ownership Illusion. Perception 2014, 43, 43–58. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Diaz Gonzalez, A.M.; Slater, M.; Sanchez-Vives, M.V. Decreasing Pain Ratings in Chronic Arm Pain Through Changing a Virtual Body: Different Strategies for Different Pain Types. J. Pain 2019, 20, 685–697. [Google Scholar] [CrossRef]
- Leemhuis, E.; De Gennaro, L.; Pazzaglia, A.M. Disconnected Body Representation: Neuroplasticity Following Spinal Cord Injury. J. Clin. Med. 2019, 8, 2144. [Google Scholar] [CrossRef]
- De Haan, E.H.F.; Dijkerman, H.C. Somatosensation in the Brain: A Theoretical Re-evaluation and a New Model. Trends Cogn. Sci. 2020, 24, 529–541. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Donegan, T.; Bottiroli, S.; Sandrini, G.; Sanchez-Vives, M.V.; Tassorelli, C. Immersive Virtual Reality and Virtual Embodiment for Pain Relief. Front. Hum. Neurosci. 2019, 13, 279. [Google Scholar] [CrossRef] [PubMed]
- Barra, J.; Giroux, M.; Metral, M.; Cian, C.; Luyat, M.; Kavounoudias, A.; Guerraz, M. Functional properties of extended body representations in the context of kinesthesia. Neurophysiol. Clin. 2020, 50, 455–465. [Google Scholar] [CrossRef]
- Von Piekartz, H.; Paris-Alemany, A.; Florencio, L.; De, C.F.; Peñas, L. Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review. Appl. Sci. 2021, 11, 6857. [Google Scholar] [CrossRef]
- Shimada, S. Multisensory and Sensorimotor Integration in the Embodied Self: Relationship between Self-Body Recognition and the Mirror Neuron System. Sensors 2022, 22, 5059. [Google Scholar] [CrossRef] [PubMed]
- Chancel, M.; Ehrsson, H.H.; Ma, W.J. Uncertainty-based inference of a common cause for body ownership. eLife 2022, 11, e77221. [Google Scholar] [CrossRef]
- Tsakiris, M.; Longo, M.R.; Haggard, P. Having a body versus moving your body: Neural signatures of agency and body-ownership. Neuropsychologia 2010, 48, 2740–2749. [Google Scholar] [CrossRef]
- Pei, Y.; Zhang, Y.; Zhu, Y.; Zhao, Y.; Zhou, F.; Huang, M.; Wu, L.; Gong, H. Hyperconnectivity and high temporal variability of the primary somatosensory cortex in low-back-related leg pain: An fMRI study of static and dynamic functional connectivity. J. Pain Res. 2020, 13, 1665–1675. [Google Scholar] [CrossRef]
- Haslam, B.S.; Butler, D.S.; Moseley, G.L.; Kim, A.S.; Carey, L.M. “My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain. Brain Sci. 2022, 12, 1331. [Google Scholar] [CrossRef]
- Trojan, J.; Diers, M.; Valenzuela-Moguillansky, C.; Torta, D.M.E. Body, space, and pain. Front. Hum. Neurosci. 2014, 8, 2013–2015. [Google Scholar] [CrossRef]
- Lotze, M.; Moseley, G.L. Role of distorted body image in pain. Curr. Rheumatol. Rep. 2007, 9, 488–496. [Google Scholar] [CrossRef]
- Van Dijk, M.T.; van Wingen, G.A.; van Lammeren, A.; Blom, R.M.; de Kwaasteniet, B.P.; Scholte, H.S.; Denys, D. Neural Basis of Limb Ownership in Individuals with Body Integrity Identity Disorder. PLoS ONE 2013, 8, e72212. [Google Scholar] [CrossRef] [PubMed]
- Cardini, F.; Longo, M.R. Congruency of body-related information induces somatosensory reorganization. Neuropsychologia 2016, 84, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K.; Mantovani, F. Neuroscience of Virtual Reality: From Virtual Exposure to Embodied Medicine. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 82. [Google Scholar] [CrossRef] [PubMed]
- Harvie, D.S.; Kelly, J.; Kluver, J.; Deen, M.; Spitzer, E.; Coppieters, M.W. A randomized controlled pilot study examining immediate effects of embodying a virtual reality superhero in people with chronic low back pain. Disabil. Rehabil. Assist. Technol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Leemhuis, E.; Giuffrida, V.; Giannini, A.M.; Pazzaglia, M. A Therapeutic Matrix: Virtual Reality as a Clinical Tool for Spinal Cord Injury-Induced Neuropathic Pain. Brain Sci. 2021, 11, 1201. [Google Scholar] [CrossRef]
- Senkowski, D.; Heinz, A. Chronic pain and distorted body image: Implications for multisensory feedback interventions. Neurosci. Biobehav. Rev. 2016, 69, 252–259. [Google Scholar] [CrossRef]
- Vartiainen, N.; Kirveskari, E.; Kallio-Laine, K.; Kalso, E.; Forss, N. Cortical reorganization in primary somatosen-sory cortex in patients with unilateral chronic pain. J. Pain 2009, 10, 854–859. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Maselli, A.; Malighetti, C.; Realdon, O.; Mantovani, F.; Riva, G. Virtual Body Ownership Illusions for Mental Health: A Narrative Review. J. Clin. Med. 2021, 10, 139. [Google Scholar] [CrossRef]
- Samad, M.; Chung, A.J.; Shams, L. Perception of Body Ownership Is Driven by Bayesian Sensory Inference. PLoS ONE 2015, 10, e0117178. [Google Scholar] [CrossRef]
- Martini, M. Real, rubber or virtual: The vision of “one’s own” body as a means for pain modulation. A narrative review. Conscious Cogn. 2016, 43, 143–151. [Google Scholar] [CrossRef]
- Pyasik, M.; Ciorli, T.; Pia, L. Full body illusion and cognition: A systematic review of the literature. Neurosci. Biobehav. Rev. 2022, 143, 104926. [Google Scholar] [CrossRef]
- Matamala-gomez, M.; Nierula, B.; Donegan, T.; Slater, M.; Sanchez-vives, M.V. Manipulating the Perceived Shape and Color of a Virtual Limb Can Modulate Pain Responses. J. Clin. Med. 2020, 9, 291. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.M.; Coppieters, M.W.; Kluver, J.; Deen, M.; Rio, E.; Harvie, D.S. “It made you feel like you’ve still got it”: Experiences of people with chronic low back pain undertaking a single session of body image training in virtual reality. Physiother. Theory Pract. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Buetler, K.A.; Penalver-Andres, J.; Özen, Ö.; Ferriroli, L.; Müri, R.M.; Cazzoli, D.; Marchal-Crespo, L. “Tricking the Brain” Using Immersive Virtual Reality: Modifying the Self-Perception Over Embodied Avatar Influences Motor Cortical Excitability and Action Initiation. Front. Hum. Neurosci. 2022, 15, 814. [Google Scholar] [CrossRef] [PubMed]
- Tsakiris, M.; Prabhu, G.; Haggard, P. Having a body versus moving your body: How agency structures body-ownership. Conscious Cogn. 2006, 15, 423–432. [Google Scholar] [CrossRef]
- Levin, M.F.; Demers, M. Motor learning in neurological rehabilitation. Disabil. Rehabil. 2020, 43, 3445–3453. [Google Scholar] [CrossRef]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Butera, K.A.; Fox, E.J.; George, S.Z. Point of View Toward a Transformed Understanding: From Pain and Movement to Pain With Movement. Phys. Ther. 2016, 96, 22–24. [Google Scholar] [CrossRef]
- Mccabe, C.S.; Cohen, H.; Blake, D.R. Somaesthetic disturbances in fibromyalgia are exaggerated by sensory motor conflict: Implications for chronicity of the disease? Rheumatology 2007, 46, 1587–1592. [Google Scholar] [CrossRef]
- Fullwood, D.; Means, S.; Merriwether, E.N.; Chimenti, R.L.; Ahluwalia, S.; Booker, S.Q. Toward understanding movement-evoked pain (MEP) and its measurement: A scoping review. Clin. J. Pain 2021, 37, 61–78. [Google Scholar] [CrossRef]
- Othman, R.; Swain, N.; Tumilty, S.; Jayakaran, P.; Mani, R. Sensitivity to movement-evoked pain, central sensitivity symptoms, and pro-nociceptive profiles in people with chronic shoulder pain: A parallel-group cross-sectional investigation. Pain Pract. 2023, 23, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Kantak, S.S.; Johnson, T.; Zarzycki, R. Linking Pain and Motor Control: Conceptualization of Movement Deficits in Patients With Painful Conditions. Phys. Ther. 2022, 102, pzab289. [Google Scholar] [CrossRef] [PubMed]
- Holmes, S.A.; Kim, A.; Borsook, D. The brain and behavioral correlates of motor-related analgesia (MRA). Neurobiol. Dis. 2021, 148, 105158. [Google Scholar] [CrossRef] [PubMed]
- Timmers, I.; Quaedflieg, C.W.E.M.; Hsu, C.; Heathcote, L.C.; Rovnaghi, C.R.; Simons, L.E. The interaction between stress and chronic pain through the lens of threat learning. Neurosci. Biobehav. Rev. 2019, 107, 641–655. [Google Scholar] [CrossRef]
- Neige, C.; Mavromatis, N.; Gagné, M.; Bouyer, L.J.; Mercier, C. Effect of movement-related pain on behaviour and corticospinal excitability changes associated with arm movement preparation. J. Physiol. 2018, 596, 2917–2929. [Google Scholar] [CrossRef]
- Karos, K.; Meulders, A.; Gatzounis, R.; Seelen, H.A.M.; Geers, R.P.G.; Vlaeyen, J.W.S. Fear of pain changes movement: Motor behaviour following the acquisition of pain-related fear. Eur. J. Pain 2017, 21, 1432–1442. [Google Scholar] [CrossRef]
- Guccione, A.A.; Neville, B.T.; George, S.Z. Optimization of Movement: A Dynamical Systems Approach to Movement Systems as Emergent Phenomena. Phys. Ther. 2019, 99, 3–9. [Google Scholar] [CrossRef]
- Van Dieën, J.H.; Flor, H.; Hodges, P.W. Low-Back Pain Patients Learn to Adapt Motor Behavior With Adverse Secondary Consequences. Exerc. Sport. Sci. Rev. 2017, 45, 223–229. [Google Scholar] [CrossRef]
- Bock, O. Sensorimotor Adaptation. In Encyclopedia of the Sciences of Learning; Springer: Boston, MA, USA, 2012; pp. 3036–3038. Available online: https://link.springer.com/referenceworkentry/10.1007/978-1-4419-1428-6_548 (accessed on 1 March 2023).
- Rothgangel, A.; Bekrater-Bodmann, R. Mirror therapy versus augmented/virtual reality applications: Towards a tailored mechanism-based treatment for phantom limb pain. Pain Manag. 2019, 9, 151–159. [Google Scholar] [CrossRef]
- La Touche, R. Métodos de representación del movimiento en rehabilitación. Construyendo un marco conceptual para la aplicación en clínica. J. MOVE Ther. Sci. 2020, 2, 152–159. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; Reina-Varona, Á.; Castillo-García, J.; La Touche, R.; Angulo-Díaz-Parreño, S.; Suso-Martí, L. Pain relief by movement representation strategies: An umbrella and mapping review with meta-meta-analysis of motor imagery, action observation and mirror therapy. Eur. J. Pain 2022, 26, 284–309. [Google Scholar] [CrossRef] [PubMed]
- Suso-Martí, L.; La Touche, R.; Angulo-Díaz-Parreño, S.; Cuenca-Martínez, F. Effectiveness of motor imagery and action observation training on musculoskeletal pain intensity: A systematic review and meta-analysis. Eur J. Pain 2020, 24, 886–901. [Google Scholar] [CrossRef]
- Rizzo, M.; Petrini, L.; Claudio Del Percio, L.; Arendt-Nielsen, L.; Babiloni, C. Neurophysiological Oscillatory Mechanisms Underlying the Effect of Mirror Visual Feedback-Induced Illusion of Hand Movements on Nociception and Cortical Activation. 2022. Available online: https://europepmc.org/article/ppr/ppr56435 (accessed on 1 March 2023).
- Cuenca-Martínez, F.; Suso-Martí, L.; León-Hernández, J.V.; La Touche, R. The Role of Movement Representation Techniques in the Motor Learning Process: A Neurophysiological Hypothesis and a Narrative Review. Brain Sci. 2020, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Lotze, M.; Moseley, G.L. Clinical and Neurophysiological Effects of Progressive Movement Imagery Training for Pathological Pain. J. Pain 2022, 23, 1480–1491. [Google Scholar] [CrossRef] [PubMed]
- Kober, S.E.; Settgast, V.; Brunnhofer, M.; Augsdörfer, U.; Wood, G. Move your virtual body: Differences and similarities in brain activation patterns during hand movements in real world and virtual reality. Virtual Real. 2022, 26, 501–511. [Google Scholar] [CrossRef]
- Ng, Y.L.; Ma, F.; Ho, F.K.; Ip, P.; Fu, K.w. Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: A systematic review and meta-analysis of randomized controlled trials. Comput. Hum. Behav. 2019, 99, 278–291. [Google Scholar] [CrossRef]
- Song, J.S.; Yamada, Y.; Kataoka, R.; Wong, V.; Spitz, R.W.; Bell, Z.W.; Loenneke, J.P. Training-induced hypoalgesia and its potential underlying mechanisms. Neurosci. Biobehav. Rev. 2022, 141, 104858. [Google Scholar] [CrossRef]
- Lima, L.V.; Abner, T.S.S.; Sluka, K.A. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J. Physiol. 2017, 595, 4141–4150. [Google Scholar] [CrossRef]
- Wewege, M.A.; Jones, M.D. Exercise-Induced Hypoalgesia in Healthy Individuals and People With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. J. Pain 2021, 22, 21–31. [Google Scholar] [CrossRef]
- Carey, C.; Naugle, K.E.; Aqeel, D.; Ohlman, T.; Naugle, K.M. Active Gaming as a Form of Exercise to Induce Hypoalgesia. Games Health J. 2017, 6, 255–261. [Google Scholar] [CrossRef]
- Evans, E.; Naugle, K.E.; Ovispo, A.; Kaleth, A.S.; Arnold, B.; Naugle, K.M. Active Virtual Reality Games Reduce Pain Sensitivity in Young, Healthy Adults. Front. Virtual Real. 2021, 2, 150. [Google Scholar] [CrossRef]
- Wender, C.L.A.; Ahn, S.J.; O’Connor, P.J. Interactive Virtual Reality Reduces Quadriceps Pain during High-Intensity Cycling. Med. Sci. Sport. Exerc. 2019, 51, 2088–2097. [Google Scholar] [CrossRef] [PubMed]
- Kami, K.; Tajima, F.; Senba, E. Brain Mechanisms of Exercise-Induced Hypoalgesia: To Find a Way Out from “Fear-Avoidance Belief”. Int. J. Mol. Sci. 2022, 23, 2886. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Lluch Girbés, E.; Lundberg, M.; Malfliet, A.; Sterling, M. Exercise therapy for chronic musculoskeletal pain: Innovation by altering pain memories. Man. Ther. 2015, 20, 216–220. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Crombez, G. Behavioral Conceptualization and Treatment of Chronic Pain. Annu. Rev. Clin. Psychol. 2020, 16, 187–212. [Google Scholar] [CrossRef] [PubMed]
- Seymour, B. Pain: A Precision Signal for Reinforcement Learning and Control. Neuron 2019, 101, 1029–1041. [Google Scholar] [CrossRef]
- Schlitt, F.; Schmidt, K.; Merz, C.J.; Wolf, O.T.; Kleine-borgmann, J. Impaired pain-related threat and safety learning in patients with chronic back pain. Pain 2022, 163, 1560–1570. [Google Scholar] [CrossRef]
- Lin, C.; Zhuo, S.; Peng, W. Ongoing pain facilitates emotional decision-making behaviors. Brain Sci. Adv. 2022, 8, 38–49. [Google Scholar] [CrossRef]
- Borsook, D.; Edwards, R.; Elman, I.; Becerra, L.; Levine, J. Pain and analgesia: The value of salience circuits. Prog. Neurobiol. 2013, 104, 93–105. [Google Scholar] [CrossRef]
- De Baets, L.; Matheve, T.; Timmermans, A. The Association between Fear of Movement, Pain Catastrophizing, Pain Anxiety, and Protective Motor Behavior in Persons with Peripheral Joint Conditions of a Musculoskeletal Origin: A Systematic Review. Am. J. Phys. Med. Rehabil. 2020, 99, 941–949. [Google Scholar] [CrossRef]
- Christe, G.; Benaim, C.; Luthi, F.; Jolles, B.M.; Favre, J. Reduction in pain-related fear is not associated with improvement in spinal biomechanics but with decrease in movement-evoked pain in patients with chronic low back pain. Pain Pract. 2022, 23, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Matheve, T.; De Baets, L.; Bogaerts, K.; Timmermans, A. Lumbar range of motion in chronic low back pain is predicted by task-specific, but not by general measures of pain-related fear. Eur. J. Pain 2019, 23, 1171–1184. [Google Scholar] [CrossRef] [PubMed]
- Vachon-Presseau, E.; Centeno, M.V.; Ren, W.; Berger, S.E.; Tétreault, P.; Ghantous, M.; Baria, A.; Farmer, M.; Baliki, M.N.; Schnitzer, T.J.; et al. The Emotional Brain as a Predictor and Amplifier of Chronic Pain. J. Dent. Res. 2016, 95, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Gava, V.; Fialho, H.R.F.; Calixtre, L.B.; Barbosa, G.M.; Kamonseki, D.H. Effects of Gaming on Pain-Related Fear, Pain Catastrophizing, Anxiety, and Depression in Patients with Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Games Health J. 2022, 11, 369–384. [Google Scholar] [CrossRef]
- Wang, S.; Sun, J.; Yin, X.; Li, H. Effect of virtual reality technology as intervention for people with kinesiophobia: A meta-analysis of randomised controlled trials. J. Clin. Nurs. 2022, 1–13. [Google Scholar] [CrossRef]
- Chen, Q.L.; Heinricher, M.M. Descending Control Mechanisms and Chronic Pain. Curr. Rheumatol. Rep. 2019, 21, 13. [Google Scholar] [CrossRef]
- Coninx, S.; Stilwell, P. Pain and the field of affordances: An enactive approach to acute and chronic pain. Synthese 2021, 199, 7835–7863. [Google Scholar] [CrossRef]
- Yarossi, M.; Mangalam, M.; Naufel, S.; Tunik, E. Virtual Reality as a Context for Adaptation. Front. Virtual Real. 2021, 2, 139. [Google Scholar] [CrossRef]
- Caneiro, J.P.; Smith, A.; Bunzli, S.; Linton, S.; Moseley, G.L.; O’Sullivan, P. From Fear to Safety: A Roadmap to Recovery from Musculoskeletal Pain. Phys. Ther. 2021, 102, pzab271. [Google Scholar] [CrossRef]
- Osiurak, F.; Rossetti, Y.; Badets, A. What is an affordance? 40 years later. Neurosci. Biobehav. Rev. 2017, 77, 403–417. [Google Scholar] [CrossRef]
- Coninx, S.; Ray, B.M.; Stilwell, P. Unpacking an affordance-based model of chronic pain: A video game analogy. Phenomenol. Cogn. Sci. 2023, 1–24. [Google Scholar] [CrossRef]
- Cheung, K.L.; Tunik, E.; Adamovich, S.V.; Boyd, L.A. Neuroplasticity and Virtual Reality. In Virtual Reality for Physical and Motor Rehabilitation; Springer: New York, NY, USA, 2014; pp. 5–24. [Google Scholar]
- Wittkopf, P.G.; Lloyd, D.M.; Coe, O.; Yacoobali, S.; Billington, J. The effect of interactive virtual reality on pain perception: A systematic review of clinical studies. Disabil. Rehabil. 2020, 42, 3722–3733. [Google Scholar] [CrossRef]
- Grassini, S. Virtual Reality Assisted Non-Pharmacological Treatments in Chronic Pain Management: A Systematic Review and Quantitative Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4071. [Google Scholar] [CrossRef]
- Brea-Gómez, B.; Torres-Sánchez, I.; Ortiz-Rubio, A.; Calvache-Mateo, A.; Cabrera-Martos, I.; López-López, L.; Valenza, M.C. Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 11806. [Google Scholar] [CrossRef] [PubMed]
- Ahern, M.M.; Dean, L.V.; Stoddard, C.C.; Agrawal, A.; Kim, K.; Cook, C.E.; Narciso Garcia, A. The Effectiveness of Virtual Reality in Patients With Spinal Pain: A Systematic Review and Meta-Analysis. Pain Pract. 2020, 20, 656–675. [Google Scholar] [CrossRef] [PubMed]
- Mallari, B.; Spaeth, E.K.; Goh, H.; Boyd, B.S. Virtual reality as an analgesic for acute and chronic pain in adults: A systematic review and meta-analysis. J. Pain Res. 2019, 12, 2053–2085. [Google Scholar] [CrossRef]
- Gumaa, M.; Youssef, A.R. Is Virtual Reality Effective in Orthopedic Rehabilitation? A Systematic Review and Meta-Analysis. Phys. Ther. 2019, 99, 1304–1325. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Model | Contributions |
|---|---|
| Model of mature organism (MOM) | In 1990, Gifford proposed a complex dynamic view of the patient’s health experience. In his model of the mature organism (MOM), he introduced fundamental pathways in the interactions between the body and the environment through sensory information [10]. |
| The triple network model | The triple network model offers a unified framework to understand the central neurophysiological mechanisms that occur in the experience of pain. First, the influence of the sensory network may modulate the salience network (related to the emotional response to sensory stimuli e.g., suffering). Second, the interrelationship with the default network shapes body self-concept through body embodiment. Thirdly, the response at the level of the executive central network and the sensorimotor network regulates the response through both action and behavior [11]. |
| Embodied Predictive Processing Theory of Pain | This model based on the Enactive Markov Decision Process (EMDP) attempts to explain the embedded complex interaction between perception and action through the sensorimotor system, where motivational factors modulate behavior based on both positive and negative reinforcement learning mechanisms [12]. The model aimed to maintain the functional integrity of the body through the process of prediction error minimization [13]. |
| Enactive-biopsychosocial approach | An enactive-biopsychosocial approach emphasizes that human experiences are influenced by the interactive relationship between the subject and the world, with the brain and body being mediators of that relationship [8]. This framework could help us understand the complexity of the pain experience that is intrinsically embodied and embedded in an environment [14]. This model adds the idea that pain experience incorporates action as a response to the environment, which includes the sensorimotor system. The enactive model shows that pain cannot be reduced to its neurophysiological underpinnings [15]. |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Systematic review and/or meta-analysis assessing the efficacy of virtual reality therapy intervention(s) for chronic pain | Including evaluative, psychological, and/or non-virtual intervention(s) |
| Systematic review and/or meta-analysis with an adequate description of methodology | Non full text available |
| Published in a peer reviewed journal | |
| Published since year 2017 | |
| Written in the English language |
| Concept | Definition |
|---|---|
| Body image | It refers to implicit cortical maps that encode movement and position of the body |
| Body embodiment | The experience of our self as the whole set of sensations that emerges from being in, having and controlling a body |
| Body ownership | It is the feeling that “this body belongs to me” |
| Body Agency | The perception that “I am the one who caused this action” |
| Co-location | being in precise place, in time and space. |
| Body perception disturbance | It refers to an alteration in the size, shape or position of the experienced physical self |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerra-Armas, J.; Flores-Cortes, M.; Pineda-Galan, C.; Luque-Suarez, A.; La Touche, R. Role of Immersive Virtual Reality in Motor Behaviour Decision-Making in Chronic Pain Patients. Brain Sci. 2023, 13, 617. https://doi.org/10.3390/brainsci13040617
Guerra-Armas J, Flores-Cortes M, Pineda-Galan C, Luque-Suarez A, La Touche R. Role of Immersive Virtual Reality in Motor Behaviour Decision-Making in Chronic Pain Patients. Brain Sciences. 2023; 13(4):617. https://doi.org/10.3390/brainsci13040617
Chicago/Turabian StyleGuerra-Armas, Javier, Mar Flores-Cortes, Consolacion Pineda-Galan, Alejandro Luque-Suarez, and Roy La Touche. 2023. "Role of Immersive Virtual Reality in Motor Behaviour Decision-Making in Chronic Pain Patients" Brain Sciences 13, no. 4: 617. https://doi.org/10.3390/brainsci13040617
APA StyleGuerra-Armas, J., Flores-Cortes, M., Pineda-Galan, C., Luque-Suarez, A., & La Touche, R. (2023). Role of Immersive Virtual Reality in Motor Behaviour Decision-Making in Chronic Pain Patients. Brain Sciences, 13(4), 617. https://doi.org/10.3390/brainsci13040617