
Neuropsychological Evaluation and Functional Magnetic Resonance Imaging Tasks in the Preoperative Assessment of Patients with Brain Tumors: A Systematic Review

 ,
,  and
and
Abstract
:1. Introduction
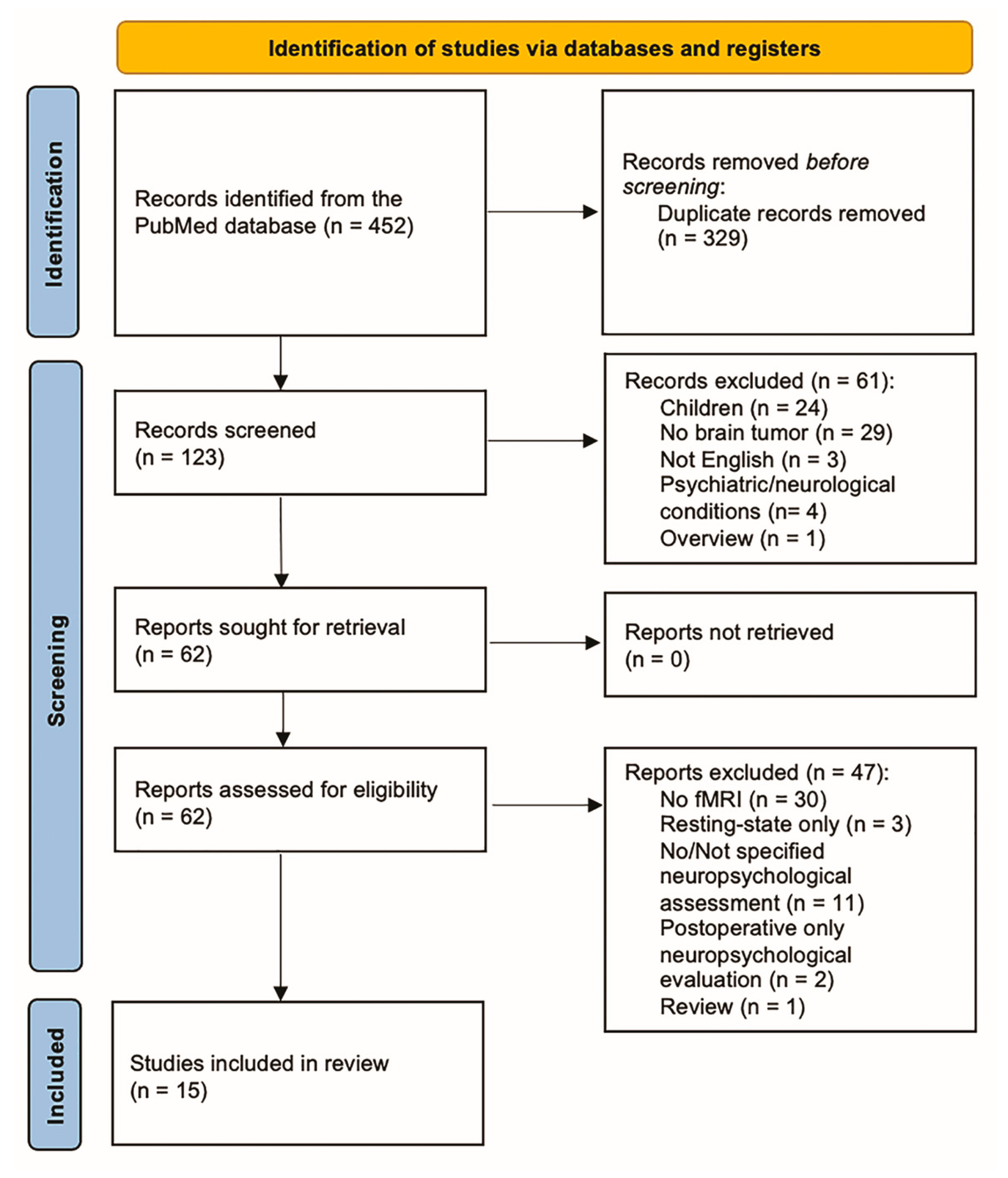
2. Materials and Methods
3. Results
3.1. Sensorimotor Functions
3.2. Language
3.3. Executive Functions
3.4. Additional Studies (PRISMA Qualitative Analysis)
4. Discussion
4.1. Anatomo-Functional Correlations of fMRI Mapping and Cognitive Performance
4.2. Integration of fMRI Data and Neuropsychological Assessment
4.3. Role of fMRI-Positive Regions during Surgery
4.4. Patient-Tailored Protocols According to the Lesion Site and Plasticity Evaluation
4.5. Limitations of the Current Study
4.6. Future Perspectives
- -
- Preoperative and postoperative evaluations, as longitudinal comparisons have not been made extensively in the previous literature;
- -
- fMRI tasks focused on specific cognitive functions and put in perspective with relative neuropsychological assessments, also taking into account the tumor site and hemisphere;
- -
- Correlations of specific neuropsychological tests with experimental fMRI tasks’ results to identify clinical criteria for the indication of preoperative fMRI.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ius, T.; Pignotti, F.; Della Pepa, G.M.; La Rocca, G.; Somma, T.; Isola, M.; Battistella, C.; Gaudino, S.; Polano, M.; Dal Bo, M.; et al. A Novel Comprehensive Clinical Stratification Model to Refine Prognosis of Glioblastoma Patients Undergoing Surgical Resection. Cancers 2020, 12, 386. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Clavreul, A.; Menei, P. Intratumoral Heterogeneity in Glioblastoma: Don’t Forget the Peritumoral Brain Zone. Neuro-Oncology 2015, 17, 1322–1332. [Google Scholar] [CrossRef]
- Weller, M.; Van Den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Brandes, A.A.; Tosoni, A.; Franceschi, E.; Reni, M.; Gatta, G.; Vecht, C. Glioblastoma in Adults. Crit. Rev. Oncol./Hematol. 2008, 67, 139–152. [Google Scholar] [CrossRef]
- Chuang, D.F.; Lin, X. Targeted Therapies for the Treatment of Glioblastoma in Adults. Curr. Oncol. Rep. 2019, 21, 61. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.E.; Jo, Y.; Shim, W.H.; Nam, S.J.; Kim, J.H.; Yoo, R.-E.; Choi, S.H.; Kim, H.S. Incorporating Diffusion- and Perfusion-Weighted MRI into a Radiomics Model Improves Diagnostic Performance for Pseudoprogression in Glioblastoma Patients. Neuro-Oncology 2019, 21, 404–414. [Google Scholar] [CrossRef]
- Öz, G.; Alger, J.R.; Barker, P.B.; Bartha, R.; Bizzi, A.; Boesch, C.; Bolan, P.J.; Brindle, K.M.; Cudalbu, C.; Dinçer, A.; et al. Clinical Proton MR Spectroscopy in Central Nervous System Disorders. Radiology 2014, 270, 658–679. [Google Scholar] [CrossRef]
- Mazzucchi, E.; La Rocca, G.; Ius, T.; Sabatino, G.; Della Pepa, G.M. Multimodality Imaging Techniques to Assist Surgery in Low-Grade Gliomas. World Neurosurg. 2020, 133, 423–425. [Google Scholar] [CrossRef]
- Li, Y.M.; Suki, D.; Hess, K.; Sawaya, R. The Influence of Maximum Safe Resection of Glioblastoma on Survival in 1229 Patients: Can We Do Better than Gross-Total Resection? JNS 2016, 124, 977–988. [Google Scholar] [CrossRef]
- Sanai, N.; Berger, M.S. Surgical Oncology for Gliomas: The State of the Art. Nat. Rev. Clin. Oncol. 2018, 15, 112–125. [Google Scholar] [CrossRef]
- Wende, T.; Hoffmann, K.-T.; Meixensberger, J. Tractography in Neurosurgery: A Systematic Review of Current Applications. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2020, 81, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Katsevman, G.A.; Turner, R.C.; Urhie, O.; Voelker, J.L.; Bhatia, S. Utility of Sodium Fluorescein for Achieving Resection Targets in Glioblastoma: Increased Gross- or near-Total Resections and Prolonged Survival. J. Neurosurg. 2020, 132, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A Multivariate Analysis of 416 Patients with Glioblastoma Multiforme: Prognosis, Extent of Resection, and Survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Gogos, A.J.; Young, J.S.; Morshed, R.A.; Hervey-Jumper, S.L.; Berger, M.S. Awake Glioma Surgery: Technical Evolution and Nuances. J. Neurooncol. 2020, 147, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Roland, J.L.; Hacker, C.D.; Leuthardt, E.C. A Review of Passive Brain Mapping Techniques in Neurological Surgery. Neurosurgery 2021, 88, 15–24. [Google Scholar] [CrossRef]
- Raffa, G.; Conti, A.; Scibilia, A.; Sindorio, C.; Quattropani, M.C.; Visocchi, M.; Germanò, A.; Tomasello, F. Functional Reconstruction of Motor and Language Pathways Based on Navigated Transcranial Magnetic Stimulation and DTI Fiber Tracking for the Preoperative Planning of Low Grade Glioma Surgery: A New Tool for Preservation and Restoration of Eloquent Networks. In Trends in Reconstructive Neurosurgery; Visocchi, M., Mehdorn, H.M., Katayama, Y., Von Wild, K.R.H., Eds.; Acta Neurochirurgica Supplement; Springer International Publishing: Cham, Switzerland, 2017; Volume 124, pp. 251–261. ISBN 978-3-319-39545-6. [Google Scholar]
- Spena, G.; Nava, A.; Cassini, F.; Pepoli, A.; Bruno, M.; D’Agata, F.; Cauda, F.; Sacco, K.; Duca, S.; Barletta, L.; et al. Preoperative and Intraoperative Brain Mapping for the Resection of Eloquent-Area Tumors. A Prospective Analysis of Methodology, Correlation, and Usefulness Based on Clinical Outcomes. Acta Neurochir. 2010, 152, 1835–1846. [Google Scholar] [CrossRef]
- Manan, H.A.; Franz, E.A.; Yahya, N. Utilization of Functional MRI Language Paradigms for Preoperative Mapping: A Systematic Review. Neuroradiology 2020, 62, 353–367. [Google Scholar] [CrossRef]
- Castellano, A.; Cirillo, S.; Bello, L.; Riva, M.; Falini, A. Functional MRI for Surgery of Gliomas. Curr. Treat. Opt. Neurol. 2017, 19, 34. [Google Scholar] [CrossRef]
- Dierker, D.; Roland, J.L.; Kamran, M.; Rutlin, J.; Hacker, C.D.; Marcus, D.S.; Milchenko, M.; Miller-Thomas, M.M.; Benzinger, T.L.; Snyder, A.Z.; et al. Resting-State Functional Magnetic Resonance Imaging in Presurgical Functional Mapping. Neuroimaging Clin. N. Am. 2017, 27, 621–633. [Google Scholar] [CrossRef]
- Silva, M.A.; See, A.P.; Essayed, W.I.; Golby, A.J.; Tie, Y. Challenges and Techniques for Presurgical Brain Mapping with Functional MRI. NeuroImage Clin. 2018, 17, 794–803. [Google Scholar] [CrossRef]
- Black, D.F.; Vachha, B.; Mian, A.; Faro, S.H.; Maheshwari, M.; Sair, H.I.; Petrella, J.R.; Pillai, J.J.; Welker, K. American Society of Functional Neuroradiology–Recommended FMRI Paradigm Algorithms for Presurgical Language Assessment. AJNR Am. J. Neuroradiol. 2017, 38, E65–E73. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, G.; Sciortino, T.; Rossi, M.; Leonetti, A.; Fornia, L.; Conti Nibali, M.; Casarotti, A.; Pessina, F.; Riva, M.; Cerri, G.; et al. Preserving Executive Functions in Nondominant Frontal Lobe Glioma Surgery: An Intraoperative Tool. J. Neurosurg. 2019, 131, 474–480. [Google Scholar] [CrossRef] [PubMed]
- DeYoe, E.A.; Raut, R.V. Visual Mapping Using Blood Oxygen Level Dependent Functional Magnetic Resonance Imaging. Neuroimaging Clin. N. Am. 2014, 24, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Pujol, J.; Deus, J.; Acebes, J.J.; Villanueva, A.; Aparicio, A.; Soriano-Mas, C.; Ortiz, H.; Conesa, G. Identification of the Sensorimotor Cortex with Functional MRI: Frequency and Actual Contribution in a Neurosurgical Context. J. Neuroimaging 2008, 18, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Bizzi, A. Presurgical Mapping of Verbal Language in Brain Tumors with Functional MR Imaging and MR Tractography. Neuroimaging Clin. N. Am. 2009, 19, 573–596. [Google Scholar] [CrossRef]
- Acevedo-Vergara, K.; Perez-Florez, M.; Ramirez, A.; Torres-Bayona, S.; Dau, A.; Salva, S.; Maloof, D.; Garcia, C.; Luque, M.; Guillen-Burgos, H.F. Cognitive Deficits in Adult Patients with High-Grade Glioma: A Systematic Review. Clin. Neurol. Neurosurg. 2022, 219, 107296. [Google Scholar] [CrossRef]
- Wolf, J.; Campos, B.; Bruckner, T.; Vogt, L.; Unterberg, A.; Ahmadi, R. Evaluation of Neuropsychological Outcome and “Quality of Life” after Glioma Surgery. Langenbecks Arch. Surg. 2016, 401, 541–549. [Google Scholar] [CrossRef]
- Romero-Garcia, R.; Owen, M.; McDonald, A.; Woodberry, E.; Assem, M.; Coelho, P.; Morris, R.C.; Price, S.J.; Santarius, T.; Suckling, J.; et al. Assessment of Neuropsychological Function in Brain Tumor Treatment: A Comparison of Traditional Neuropsychological Assessment with App-Based Cognitive Screening. Acta Neurochir. 2022, 164, 2021–2034. [Google Scholar] [CrossRef]
- MacDonald, M.E.; Pike, G.B. MRI of Healthy Brain Aging: A Review. NMR Biomed. 2021, 34, e4564. [Google Scholar] [CrossRef]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R.; Misra, S. Machine Learning with Multimodal Neuroimaging Data to Classify Stages of Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Cogn. Neurodyn. 2023, 1–20. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A New Tool to Assess Risk of Bias in Systematic Reviews Was Developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Kamada, K.; Takeuchi, F.; Kuriki, S.; Todo, T.; Morita, A.; Sawamura, Y. Dissociated Expressive and Receptive Language Functions on Magnetoencephalography, Functional Magnetic Resonance Imaging, and Amobarbital Studies: Case Report and Review of the Literature. JNS 2006, 104, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Papagno, C.; Miracapillo, C.; Casarotti, A.; Romero Lauro, L.J.; Castellano, A.; Falini, A.; Casaceli, G.; Fava, E.; Bello, L. What Is the Role of the Uncinate Fasciculus? Surgical Removal and Proper Name Retrieval. Brain 2011, 134, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Bizzi, A.; Nava, S.; Ferrè, F.; Castelli, G.; Aquino, D.; Ciaraffa, F.; Broggi, G.; DiMeco, F.; Piacentini, S. Aphasia Induced by Gliomas Growing in the Ventrolateral Frontal Region: Assessment with Diffusion MR Tractography, Functional MR Imaging and Neuropsychology. Cortex 2012, 48, 255–272. [Google Scholar] [CrossRef]
- Kristo, G.; Raemaekers, M.; Rutten, G.-J.; De Gelder, B.; Ramsey, N.F. Inter-Hemispheric Language Functional Reorganization in Low-Grade Glioma Patients after Tumour Surgery. Cortex 2015, 64, 235–248. [Google Scholar] [CrossRef]
- Sierpowska, J.; Gabarrós, A.; Fernandez-Coello, A.; Camins, À.; Castañer, S.; Juncadella, M.; De Diego-Balaguer, R.; Rodríguez-Fornells, A. Morphological Derivation Overflow as a Result of Disruption of the Left Frontal Aslant White Matter Tract. Brain Lang. 2015, 142, 54–64. [Google Scholar] [CrossRef]
- Arbula, S.; Pacella, V.; De Pellegrin, S.; Rossetto, M.; Denaro, L.; D’Avella, D.; Della Puppa, A.; Vallesi, A. Addressing the Selective Role of Distinct Prefrontal Areas in Response Suppression: A Study with Brain Tumor Patients. Neuropsychologia 2017, 100, 120–130. [Google Scholar] [CrossRef]
- Lang, S.; Gaxiola-Valdez, I.; Opoku-Darko, M.; Partlo, L.A.; Goodyear, B.G.; Kelly, J.J.P.; Federico, P. Functional Connectivity in Frontoparietal Network: Indicator of Preoperative Cognitive Function and Cognitive Outcome Following Surgery in Patients with Glioma. World Neurosurg. 2017, 105, 913–922.e2. [Google Scholar] [CrossRef]
- De Baene, W.; Jansma, M.J.; Schouwenaars, I.T.; Rutten, G.-J.M.; Sitskoorn, M.M. Task-Evoked Reconfiguration of the Fronto-Parietal Network Is Associated with Cognitive Performance in Brain Tumor Patients. Brain Imaging Behav. 2020, 14, 2351–2366. [Google Scholar] [CrossRef] [PubMed]
- Zacharia, T.T.; Eslinger, P.J. Functional MRI Activation Patterns of Cerebellum in Patients with Epilepsy and Brain Tumors. Clin. Anat. 2019, 32, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Argiris, G.; Budai, R.; Maieron, M.; Ius, T.; Skrap, M.; Tomasino, B. Neurosurgical Lesions to Sensorimotor Cortex Do Not Impair Action Verb Processing. Sci. Rep. 2020, 10, 523. [Google Scholar] [CrossRef]
- Leote, J.; Loução, R.; Viegas, C.; Lauterbach, M.; Perez-Hick, A.; Monteiro, J.; Nunes, R.G.; Ferreira, H.A. Impact of Navigated Task-Specific FMRI on Direct Cortical Stimulation. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2020, 81, 555–564. [Google Scholar] [CrossRef]
- Schouwenaars, I.T.; De Dreu, M.J.; Rutten, G.-J.M.; Ramsey, N.F.; Jansma, J.M. A Functional MRI Study of Presurgical Cognitive Deficits in Glioma Patients. Neuro-Oncol. Pract. 2021, 8, 81–90. [Google Scholar] [CrossRef]
- Mitolo, M.; Zoli, M.; Testa, C.; Morandi, L.; Rochat, M.J.; Zaccagna, F.; Martinoni, M.; Santoro, F.; Asioli, S.; Badaloni, F.; et al. Neuroplasticity Mechanisms in Frontal Brain Gliomas: A Preliminary Study. Front. Neurol. 2022, 13, 867048. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Andres, A.; Cunillera, T.; Rico, I.; Naval-Baudin, P.; Camins, A.; Fernandez-Coello, A.; Gabarrós, A.; Rodriguez-Fornells, A. The Role of the Anterior Insular Cortex in Self-Monitoring: A Novel Study Protocol with Electrical Stimulation Mapping and Functional Magnetic Resonance Imaging. Cortex 2022, 157, 231–244. [Google Scholar] [CrossRef]
- Yamamoto, A.K.; Sanjuán, A.; Pope, R.; Parker Jones, O.; Hope, T.M.H.; Prejawa, S.; Oberhuber, M.; Mancini, L.; Ekert, J.O.; Garjardo-Vidal, A.; et al. The Effect of Right Temporal Lobe Gliomas on Left and Right Hemisphere Neural Processing During Speech Perception and Production Tasks. Front. Hum. Neurosci. 2022, 16, 803163. [Google Scholar] [CrossRef]
- Amiez, C.; Kostopoulos, P.; Champod, A.-S.; Collins, D.L.; Doyon, J.; Maestro, R.D.; Petrides, M. Preoperative Functional Magnetic Resonance Imaging Assessment of Higher-Order Cognitive Function in Patients Undergoing Surgery for Brain Tumors. JNS 2008, 108, 258–268. [Google Scholar] [CrossRef]
- Quirarte, J.A.; Kumar, V.A.; Liu, H.-L.; Noll, K.R.; Wefel, J.S.; Lang, F.F. Language Supplementary Motor Area Syndrome Correlated with Dynamic Changes in Perioperative Task-Based Functional MRI Activations: Case Report. J. Neurosurg. 2021, 134, 1738–1742. [Google Scholar] [CrossRef]
- Alexopoulos, G.; Cikla, U.; El Tecle, N.; Kulkarni, N.; Pierson, M.; Mercier, P.; Kemp, J.; Coppens, J.; Mahmoud, S.; Sehi, M.; et al. The Value of White Matter Tractography by Diffusion Tensor Imaging in Altering a Neurosurgeon’s Operative Plan. World Neurosurg. 2019, 132, e305–e313. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; D’Andrea, G.; Minniti, G.; Mastronardi, L.; Ferrante, L.; Fantozzi, L.M.; Bozzao, A. Presurgical Planning and MR-Tractography Utility in Brain Tumour Resection. Eur. Radiol. 2009, 19, 2798–2808. [Google Scholar] [CrossRef]
- Kuchcinski, G.; Mellerio, C.; Pallud, J.; Dezamis, E.; Turc, G.; Rigaux-Viode, O.; Malherbe, C.; Roca, P.; Leclerc, X.; Varlet, P.; et al. Three-Tesla Functional MR Language Mapping: Comparison with Direct Cortical Stimulation in Gliomas. Neurology 2015, 84, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Giussani, C.; Roux, F.-E.; Ojemann, J.; Sganzerla, E.P.; Pirillo, D.; Papagno, C. Is Preoperative Functional Magnetic Resonance Imaging Reliable for Language Areas Mapping in Brain Tumor Surgery? Review of Language Functional Magnetic Resonance Imaging and Direct Cortical Stimulation Correlation Studies. Neurosurgery 2010, 66, 113–120. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Patients (N) | WHO Grade | Hemisphere and Location | Surgery | Cognitive Function Domain | fMRI Tasks | Neuropsychological Tests | Awake Surgery Assessment | ||
|---|---|---|---|---|---|---|---|---|---|---|
| L | R | NA/Both | ||||||||
| [40] | 25 | 18 HGG 7 LGG | 7 prefrontal HGG 1 prefrontal LGG | 4 prefrontal HGG 3 prefrontal LGG | 7 non-prefrontal HGG 3 non-prefrontal LGG | Y | Executive | Go/No-Go task | MMSE, IQ, Verbal short-term memory and working memory Selective and divided attention visuospatial short-term memory Phonemic fluency | N |
| [44] | 20 | 13 HGG 7 LGG | 2 premotor HGG 4 motor HGG 2 sensorimotor HGG 1 parasagittal HGG 2 premotor LGG 2 motor LGG 1 L sensorimotor LGG | 1 premotor HGG 2 motor HGG 1 sensorimotor HGG 1 premotor LGG 1 motor LGG | - | N | Sensorimotor Language | Motor localizer tasks, general motor imagery ability, conceptual knowledge of actions, lexical grammar processing, verb naming | Nonverbal intelligence Visuospatial short-term memory Constructional apraxia Visuospatial/constructive ability and planning Attentional neglect Visuoconceptual and visuomotor tracking Verbal short-term memory Buccofacial and ideomotor apraxia Noun naming and phonemic fluency | N |
| [37] | 19 | 13 HGG 6 LGG | ventrolateral frontal (anterior and posterior groups) | - | - | N | Language | Verb generation task, orofacial apraxia | Phonemic fluency Semantic fluency Orofacial apraxia | N |
| [42] | 26 | 13 HGG 13 LGG | 8 HGG 7 LGG | 5 HGG 6 LGG | 4 of the HGG were frontal 10 of the LGG were frontal (Side NA) | N | Executive | N-back task | Cognitive flexibility (shifting attention) | N |
| [48] | 1 | II | 1 fronto-insular | - | - | Y | Executive | Stroop task | Executive functions and attention Working memory Inhibition Mental flexibility Set shifting abilities Verbal fluency (semantic and phonological) Language production and naming Verbal comprehension Insular-related functioning (Empathy scale and emotion recognition) Mood | Y |
| [35] | 1 | II | - | 1 insular | - | Y | Language | Verb generation task, abstract/concrete categorization | Language functions IQ Memory Visual retention | N |
| [38] | 20 | 3 HGG 15 LGG | 6 frontal 1 fronto-temporal 1 parietal 1 fronto-parietal 2 temporo-occipital 1 temporo-parietal 2 temporal | 4 frontal 1 fronto-temporal 1 parietal | - | Y | Language | Verb generation task | IQ Abstract reasoning Cognitive processing speed Executive functioning Attention Working memory | Y |
| [41] | 16 | 11 HGG 5 LGG | 8 frontal 2 insular 1 temporal 1 frontoparietal | 2 frontal 1 temporoparietal 1 temporal | - | Y | Executive Sensorimotor Language | N-back task, motor and language tasks | National Institutes of Health Cognitive Battery | N |
| [45] | 18 | 11 HGG 7 LGG | 10 frontal 5 temporal 1 insular 2 parietal | - | - | Y | Language Sensorimotor | Verb generation, semantic and syntactic decision tasks, motor tasks | Picture-naming Nonverbal visual semantic decision Verb-generation task | Y |
| [47] | 15 | 10 HGG 5 LGG | 10 frontal | 5 frontal | - | Y | Language | Phonemic fluency task | MMSE, IQ Naming Phonemic verbal fluency Category fluency Short-term verbal memory and episodic memory Visuospatial short-term memory span and long-term visuospatial memory Visuoconstructive and planning abilities Attention and executive functions Depression and anxiety Cognitive reserve | Y |
| [36] | 44 | 19 HGG 25 LGG | frontal and temporal | - | - | Y | Language | Word generation, picture naming tasks | Non-verbal intelligence Verbal and visuospatial, short- and long-term memory Selective and divided attention Orofacial, ideomotor, and constructional apraxia Spatial cognition Phonemic and semantic fluency Naming tasks Sentence comprehension Repetition | Y |
| [46] | 46 | 25 HGG 21 LGG | 13 HGG 10 LGG (possible involvement of central executive network or default mode network) | 12 HGG 10 LGG (possible involvement of central executive network or default mode network) | 1 LGG both | N | Executive | N-back task | Cognitive performance | N |
| [39] | 1 | III | premotor | - | - | Y | Language | Verb generation task | SMA functions Picture description Semantic and phonological verbal fluency Motor execution Processing speed Working memory Verbs and nouns generation | Y |
| [49] | 19 | HGG and LGG | - | 3 posterosuperior temporal lobe | 16 supratentorial (controls, NA) | Y | Language | Speech perception, object recognition, auditory short-term memory holding | Behavioral testing with language-related and cognitive non-language tasks | N |
| [43] | 23 | NA | - | - | 23 | N | Sensorimotor Language Executive | Sensorimotor processing, language, working memory, executive function, visual function, auditory function | MoCa | N |
| Author | Patients (N) | WHO Grade | Surgery | fMRI Tasks | fMRI Measures | Neuropsychological Tests (Related to Task) | Main Results | Awake Surgery | Task during Awake Surgery |
|---|---|---|---|---|---|---|---|---|---|
| [44] | 20 | 13 HGG 7 LGG | N | Motor localizer tasks General motor imagery ability Conceptual knowledge of actions | Somatotopic cortical mapping (mouth, hand and feet) Imagery questions (joint movement, hands spatial position during action production) Mental rotation task Kissing and Dancing Test | Visuospatial short-term memory Constructional apraxia Visuospatial/constructive ability and planning Attentional neglect Visuoconceptual and visuomotor tracking Buccofacial and ideomotor apraxia | Involvement of the motor system in motor imagery processes | N | |
| [41] | 16 | 11 HGG 5 LGG | Y | Motor tasks | NA | FPN functional connectivity is related to cognitive outcomes after surgery | Y | NA | |
| [45] | 18 | 11 HGG 7 LGG | Y | Motor tasks | NA | Picture-naming Nonverbal visual semantic decision task Verb-generation task | Navigated fMRI data did not influence DCS in practice | Y | Picture naming, nonverbal visual semantic decision task |
| [43] | 23 | NA | N | Sensorimotor processing | Finger tapping Toe movement Lip movement | MoCa (Montreal Cognitive Assessment) | Simultaneous cerebellar activation across different cognitive domains (except visual) | N |
| Author | Patients (N) | WHO Grade | Surgery | fMRI Tasks | fMRI Measures | Neuropsychological Tests (Related to Task) | Main Results | Awake Surgery | Task during Awake Surgery |
|---|---|---|---|---|---|---|---|---|---|
| [44] | 20 | 13 HGG 7 LGG | N | Lexical grammar processing Verb naming | Verbs conjugation discrimination Verb oral naming task from BADA | Nonverbal intelligence Noun naming Phonemic fluency | Lexico-semantic processing of action not compromised by sensorimotor area lesion | N | |
| [37] | 19 | 13 HGG 6 LGG | N | Verb generation task | Verb generation | Phonemic fluency Semantic fluency Orofacial apraxia | Functional activation of pars opercularis | N | |
| [35] | 1 | II | Y | Verb generation task Abstract/concrete categorization | Silent verb generation related to a noun Categorization of a word | Language functions IQ Memory Visual Retention | Activation of left frontal regions | N | |
| [38] | 20 | 3 HGG 15 LGG | Y | Verb generation task | Covert articulation of a verb related to a noun | IQ | Perilesional functional reorganization of language areas | Y | Motor and language tasks |
| [45] | 18 | 11 HGG 7 LGG | Y | Verb generation task Semantic and syntactic decision tasks | Silent verb generation related to a noun Judgment of the semantic correctness of phrases | Picture-naming Nonverbal visual semantic decision Verb-generation task | DCS duration is not reduced by the use of fMRI mapping | Y | Picture naming Nonverbal visual semantic decision task |
| [47] | 15 | 10 HGG 5 LGG | Y | Phonemic fluency task | Covert generation of a noun starting with a given letter | MMSE, IQ Naming Phonemic verbal fluency Category fluency Short-term verbal memory and episodic memory | Left hemispheric dominance in temporal and parietal regions | Y | Specific language tests |
| [36] | 44 | 19 HGG 25 LGG | Y | Word generation Picture naming tasks | Language dominance | Non-verbal intelligence Orofacial, ideomotor, and constructional apraxia Phonemic and semantic fluency Naming tasks Sentence comprehension Repetition | Role of the uncinate fasciculus in the retrieval of a word form for proper names | Y | Language with blocks of items (living, non-living, faces, verbs) |
| [39] | 1 | III | Y | Verb generation task | Covert generation of a verb starting with a given noun | Picture description Semantic and phonological verbal fluency Verbs and nouns generation | No functional change post-surgically in the verb generation task | Y | Language tasks (ability to repeat words and non-words and to generate verbs) |
| [49] | 19 | HGG and LGG | Y | Speech perception Object recognition Auditory short-term memory holding | Recognition of the semantic relationship | Behavioral testing with language-related and cognitive non-language tasks | Importance of right temporal lobe for language processing | N | |
| [43] | 23 | NA | N | Language processing | Word generation Verb generation Sentence completion | MoCa | Simultaneous cerebellar activation across different cognitive domains (except visual) | N |
| Author | Patients (N) | WHO Grade | Surgery | fMRI Tasks | fMRI Measures | Neuropsychological Tests (Related to Task) | Main Results | Awake Surgery | Task during Awake Surgery |
|---|---|---|---|---|---|---|---|---|---|
| [40] | 25 | 18 HGG 7 LGG | Y | Go/No-Go task | Omissions and false alarms | MMSE, IQ, Verbal short-term memory and working memory Selective and divided attention Visuospatial short-term memory | Prefrontal areas underlie broader cognitive control processes (response selection, target detection) | N | |
| [42] | 26 | 13 HGG 13 LGG | N | N-back task | 2-back congruent conditions | Attention shifting | FPN plastic capacity plays a role in cognitive deficits | N | |
| [48] | 1 | II | Y | Stroop task | Informative feedback blocks | Executive functions Attention Working memory Inhibition Mental flexibility Set shifting abilities Insular-related functioning (empathy scale and emotion recognition) | Role of the insula in self-monitoring | Y | Awake mapping multimodal protocol (modified version of the Stroop task) |
| [41] | 16 | 11 HGG 5 LGG | Y | N-back task | Difference between 0-back and 2-back congruent conditions | National Institutes of Health Cognitive Battery | FPN connectivity is associated with cognitive performance | N | |
| [46] | 46 | 25 HGG 21 LGG | N | N-back task | Difference between 0-back and 2-back congruent conditions | Cognitive performance | Cognitive deficits associated with reduced DMN | N | |
| [43] | 23 | NA | N | Working memory, executive function | N-back task | MoCa | Simultaneous cerebellar activation across different cognitive domains (except visual) | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pertichetti, M.; Corbo, D.; Belotti, F.; Saviola, F.; Gasparotti, R.; Fontanella, M.M.; Panciani, P.P. Neuropsychological Evaluation and Functional Magnetic Resonance Imaging Tasks in the Preoperative Assessment of Patients with Brain Tumors: A Systematic Review. Brain Sci. 2023, 13, 1380. https://doi.org/10.3390/brainsci13101380
Pertichetti M, Corbo D, Belotti F, Saviola F, Gasparotti R, Fontanella MM, Panciani PP. Neuropsychological Evaluation and Functional Magnetic Resonance Imaging Tasks in the Preoperative Assessment of Patients with Brain Tumors: A Systematic Review. Brain Sciences. 2023; 13(10):1380. https://doi.org/10.3390/brainsci13101380
Chicago/Turabian StylePertichetti, Marta, Daniele Corbo, Francesco Belotti, Francesca Saviola, Roberto Gasparotti, Marco Maria Fontanella, and Pier Paolo Panciani. 2023. "Neuropsychological Evaluation and Functional Magnetic Resonance Imaging Tasks in the Preoperative Assessment of Patients with Brain Tumors: A Systematic Review" Brain Sciences 13, no. 10: 1380. https://doi.org/10.3390/brainsci13101380
APA StylePertichetti, M., Corbo, D., Belotti, F., Saviola, F., Gasparotti, R., Fontanella, M. M., & Panciani, P. P. (2023). Neuropsychological Evaluation and Functional Magnetic Resonance Imaging Tasks in the Preoperative Assessment of Patients with Brain Tumors: A Systematic Review. Brain Sciences, 13(10), 1380. https://doi.org/10.3390/brainsci13101380