
The Role of Bone-Anchored Hearing Devices and Remote Microphones in Children with Congenital Unilateral Hearing Loss
 ,
,  , ,
, ,
Abstract
:1. Introduction
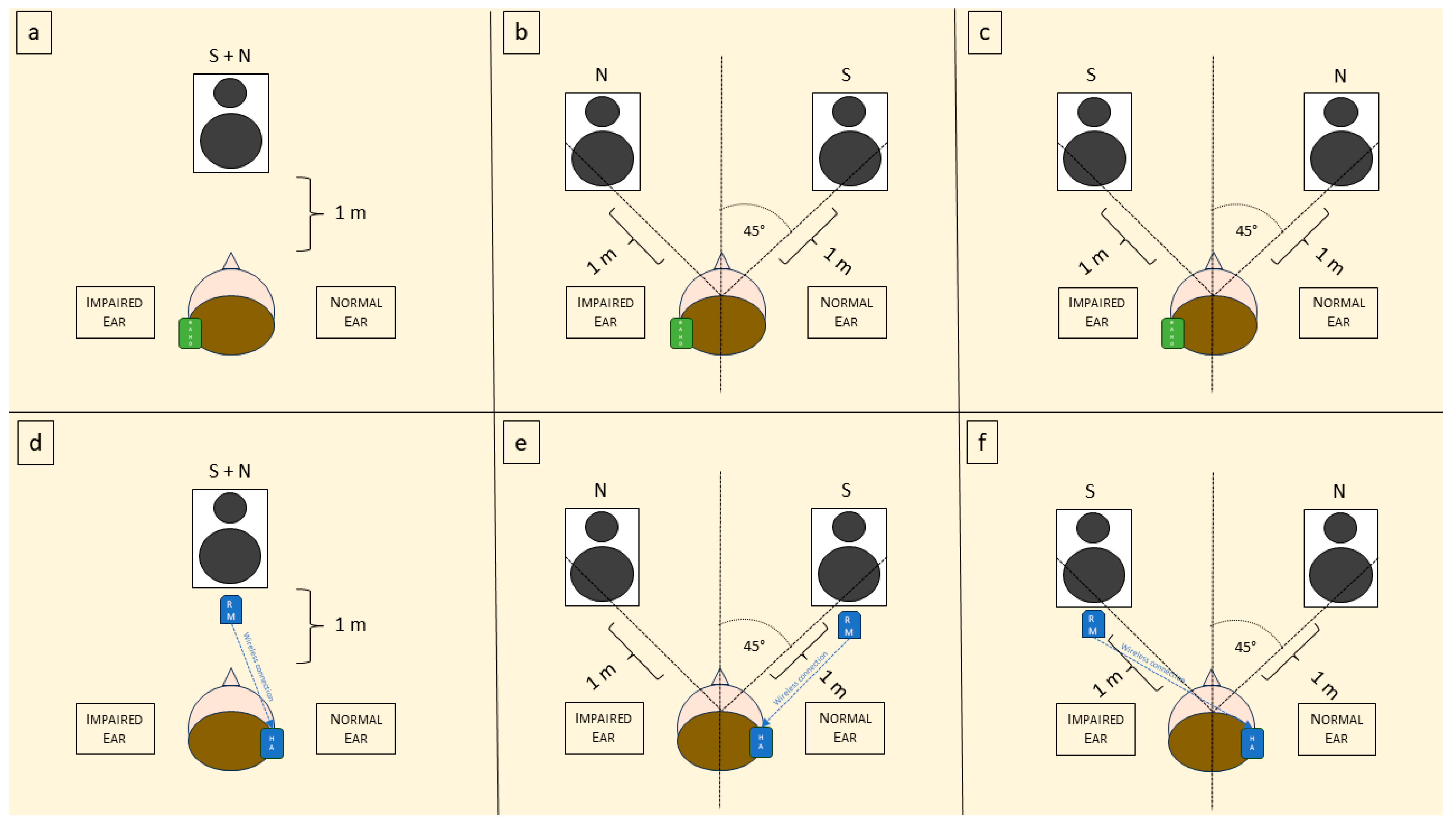
2. Materials and Methods
- Enrolment criteria were the following:
- Age < 16 years and >5 years;
- No previous experience with hearing devices or RM;
- Appropriate development of speech and language;
- Presence of SSD (defined as unilateral sensorineural hearing loss with a pure tone average hearing threshold at 250 Hz, 500 Hz, 1000 Hz, and 2000 Hz (PTA) ≥ 65 Db, with a contralateral PTA < 30 dB) or presence of UAA.
- Exclusion criteria were the following:
- Multihandicap and/or cognitive impairment.
Statistical Analysis
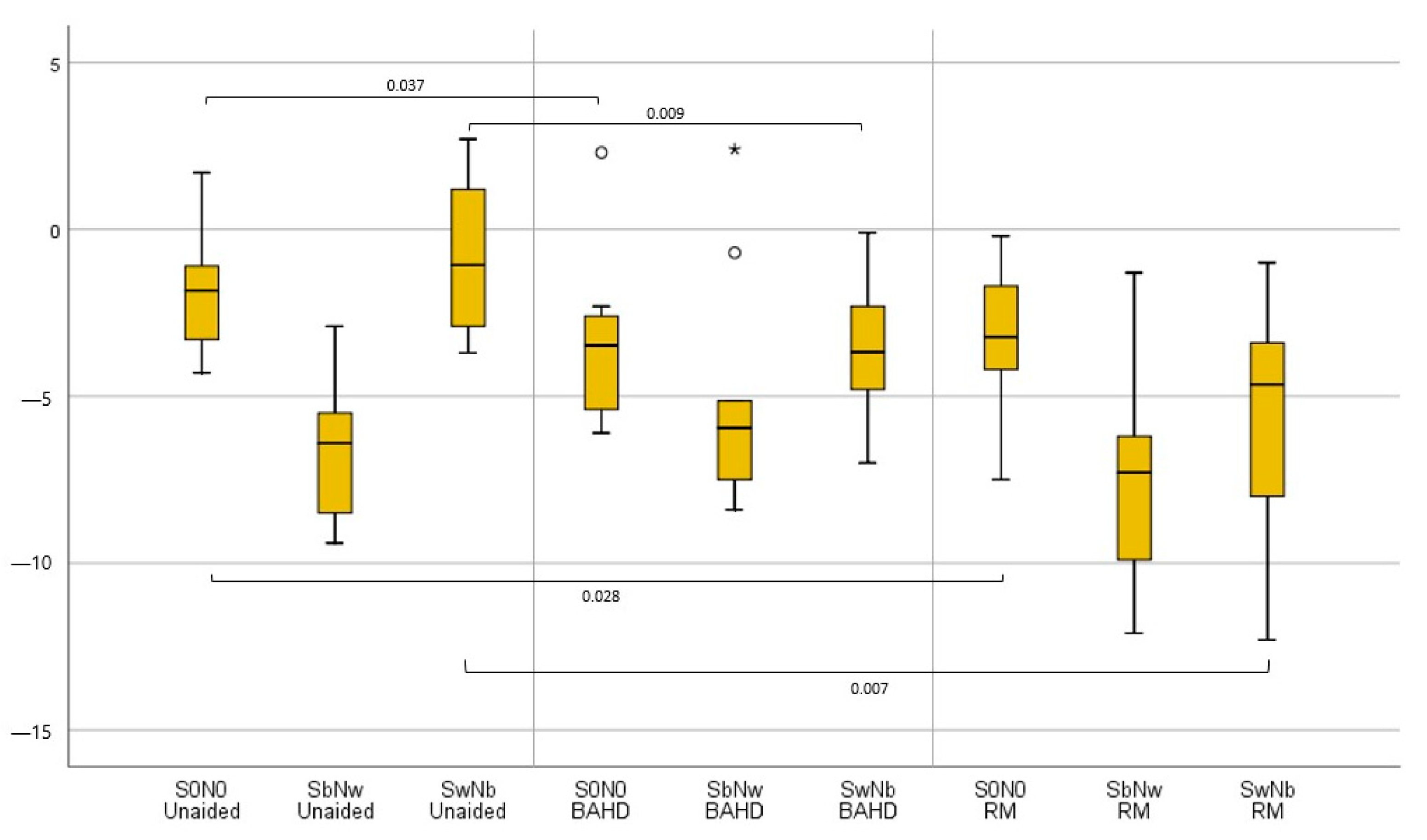
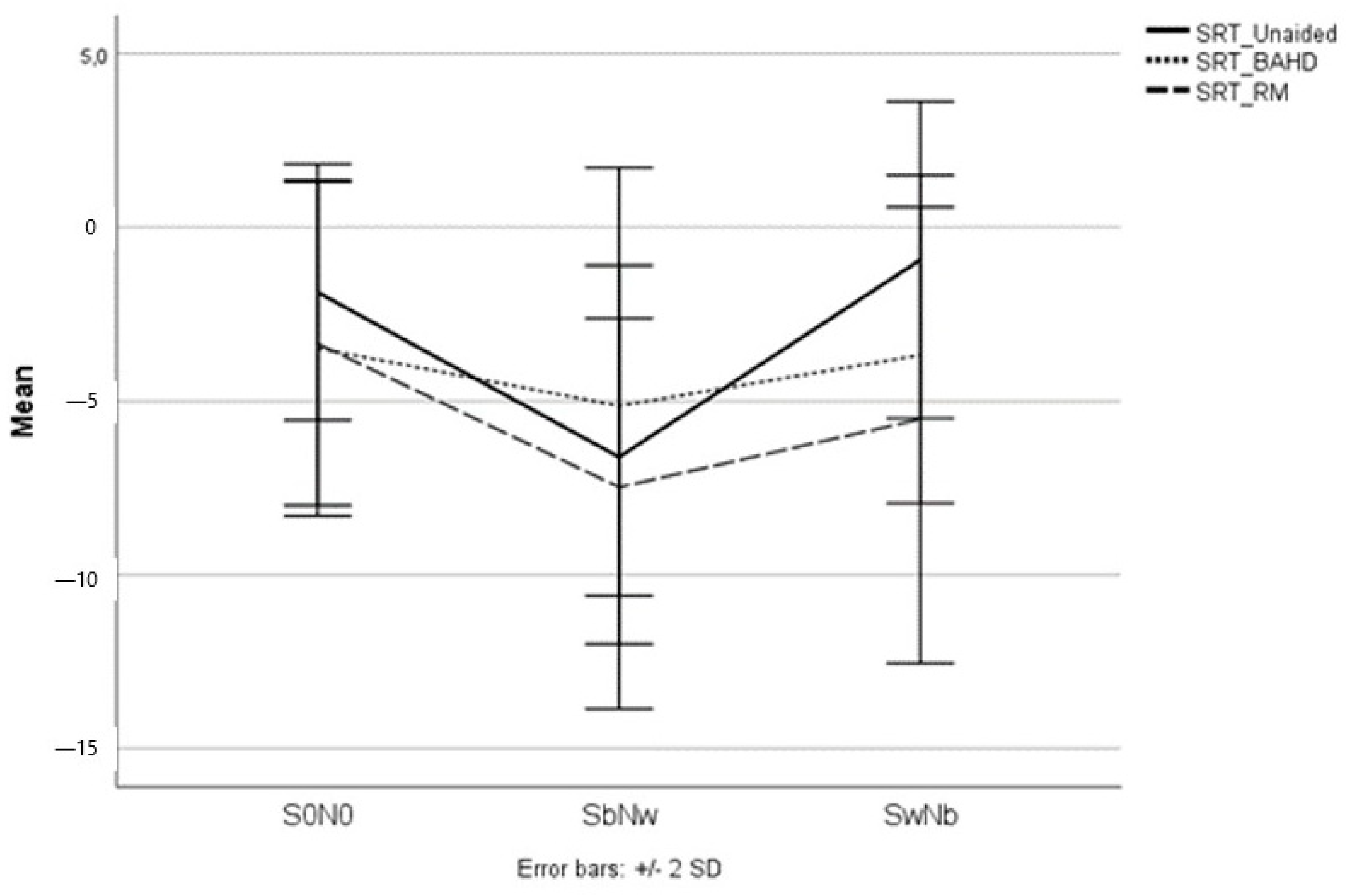
3. Results
3.1. UHL Population
3.1.1. BAHD vs. Unaided
3.1.2. RM vs. Unaided
3.1.3. BAHD vs. RM
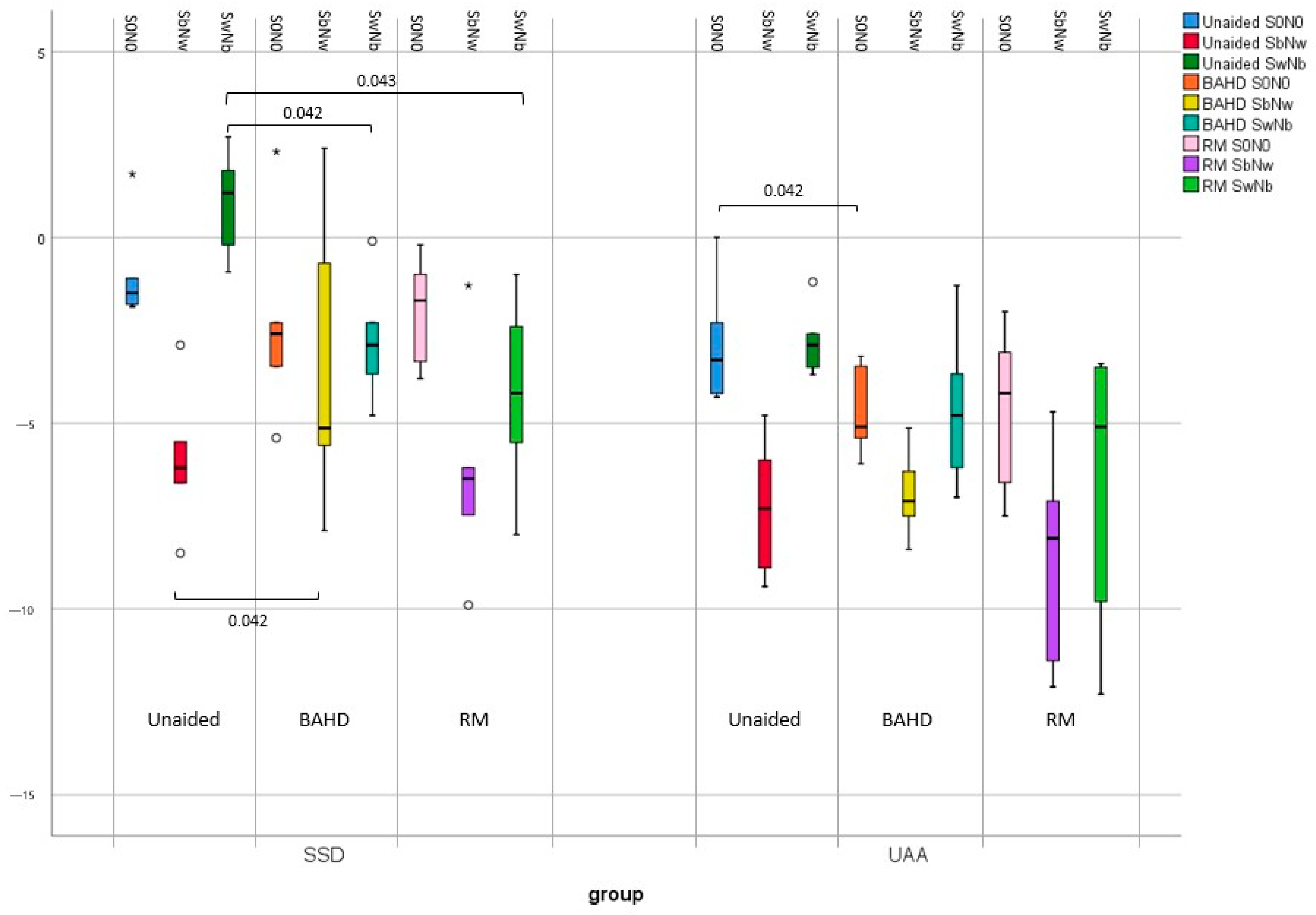
3.2. SSD Subgroup
3.2.1. BAHD vs. Unaided
3.2.2. RM vs. Unaided
3.2.3. BAHD vs. RM
3.3. UAA Subgroup
3.3.1. BAHD vs. Unaided
3.3.2. RM vs. Unaided
3.3.3. BAHD vs. RM
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kral, A.; Hubka, P.; Heid, S.; Tillein, J. Single-Sided Deafness Leads to Unilateral Aural Preference within an Early Sensitive Period. Brain 2013, 136, 180–193. [Google Scholar] [CrossRef]
- van Wieringen, A.; Boudewyns, A.; Sangen, A.; Wouters, J.; Desloovere, C. Unilateral Congenital Hearing Loss in Children: Challenges and Potentials. Hear. Res. 2019, 372, 29–41. [Google Scholar] [CrossRef]
- Bess, F.H.; Tharpe, A.M. Unilateral Hearing Impairment in Children. Pediatrics 1984, 74, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Bess, F.H.; Tharpe, A.M. Performance and Management of Children with Unilateral Sensorineural Hearing Loss. Scand. Audiol. Suppl. 1988, 30, 75–79. [Google Scholar] [PubMed]
- Bess, F.H.; Tharpe, A.M. An Introduction to Unilateral Sensorineural Hearing Loss in Children. Ear Hear. 1986, 7, 3–13. [Google Scholar] [CrossRef]
- Fitzpatrick, E.M.; Gaboury, I.; Durieux-Smith, A.; Coyle, D.; Whittingham, J.; Nassrallah, F. Auditory and Language Outcomes in Children with Unilateral Hearing Loss. Hear. Res. 2019, 372, 42–51. [Google Scholar] [CrossRef]
- Lewis, D.; Schmid, K.; O’Leary, S.; Spalding, J.; Heinrichs-Graham, E.; High, R. Effects of Noise on Speech Recognition and Listening Effort in Children With Normal Hearing and Children With Mild Bilateral or Unilateral Hearing Loss. J. Speech Lang. Hear. Res. 2016, 59, 1218–1232. [Google Scholar] [CrossRef] [PubMed]
- Porter, A.; Sheeran, N.; Hood, M.; Creed, P. Decision-Making Following Identification of an Infant’s Unilateral Hearing Loss: Parent and Professional Perspectives. Int. J. Pediatr. Otorhinolaryngol. 2021, 148, 110822. [Google Scholar] [CrossRef]
- Reeder, R.M.; Cadieux, J.; Firszt, J.B. Quantification of Speech-in-Noise and Sound Localisation Abilities in Children with Unilateral Hearing Loss and Comparison to Normal Hearing Peers. Audiol. Neuro-Otol. 2015, 20 (Suppl. S1), 745. [Google Scholar] [CrossRef]
- Klee, T.M.; Davis-Dansky, E. A Comparison of Unilaterally Hearing-Impaired Children and Normal-Hearing Children on a Battery of Standardized Language Tests. Ear. Hear. 1986, 7, 27–37. [Google Scholar] [CrossRef]
- Lieu, J.E.C. Unilateral Hearing Loss in Children: Speech-Language and School Performance. B-ENT 2013, 9 (Suppl. S21), 107–115. [Google Scholar]
- Lieu, J.E.C.; Tye-Murray, N.; Fu, Q. Longitudinal Study of Children with Unilateral Hearing Loss. Laryngoscope 2012, 122, 2088–2095. [Google Scholar] [CrossRef] [PubMed]
- Je, L. Speech-Language and Educational Consequences of Unilateral Hearing Loss in Children. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 542. [Google Scholar] [CrossRef]
- Carpenter, D.; Dougherty, W.; Sindhar, S.; Friesen, T.-N.; Lieu, J.; Kesser, B.W. Are Children with Unilateral Hearing Loss More Tired? Int. J. Pediatr. Otorhinolaryngol. 2022, 155, 111075. [Google Scholar] [CrossRef] [PubMed]
- Blauert, J. Spatial Hearing: The Psychophysics of Human Sound Localization; MIT Press: Boston, MA, USA, 1997; ISBN 978-0-262-02413-6. [Google Scholar]
- Forli, F.; Lazzerini, F.; Canelli, R.; Lorenzoni, F.; Franciosi, B.; Berrettini, S.; Bruschini, L. Extended-Hearing Targeted Screening for Congenital Cytomegalovirus Infection. Minerva Pediatr. 2021, 2021, 287. [Google Scholar] [CrossRef]
- Aldè, M.; Binda, S.; Primache, V.; Pellegrinelli, L.; Pariani, E.; Pregliasco, F.; Di Berardino, F.; Cantarella, G.; Ambrosetti, U. Congenital Cytomegalovirus and Hearing Loss: The State of the Art. J. Clin. Med. 2023, 12, 4465. [Google Scholar] [CrossRef]
- Smith, R.J.; Iwasa, Y.; Schaefer, A.M. Pendred Syndrome/Nonsyndromic Enlarged Vestibular Aqueduct. In GeneReviews®; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Forli, F.; Lazzerini, F.; Auletta, G.; Bruschini, L.; Berrettini, S. Enlarged Vestibular Aqueduct and Mondini Malformation: Audiological, Clinical, Radiologic and Genetic Features. Eur. Arch. Otorhinolaryngol. 2021, 278, 2305–2312. [Google Scholar] [CrossRef]
- Park, L.R.; Griffin, A.M.; Sladen, D.P.; Neumann, S.; Young, N.M. American Cochlear Implant Alliance Task Force Guidelines for Clinical Assessment and Management of Cochlear Implantation in Children With Single-Sided Deafness. Ear. Hear. 2022, 43, 255–267. [Google Scholar] [CrossRef]
- Rauch, A.-K.; Arndt, S.; Aschendorff, A.; Beck, R.; Speck, I.; Ketterer, M.C.; Jakob, T.F.; Hassepass, F. Long-Term Results of Cochlear Implantation in Children with Congenital Single-Sided Deafness. Eur. Arch. Otorhinolaryngol. 2021, 278, 3245–3255. [Google Scholar] [CrossRef]
- Benchetrit, L.; Ronner, E.A.; Anne, S.; Cohen, M.S. Cochlear Implantation in Children With Single-Sided Deafness: A Systematic Review and Meta-Analysis. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 58–69. [Google Scholar] [CrossRef]
- Marx, M.; Mosnier, I.; Vincent, C.; Bonne, N.-X.; Bakhos, D.; Lescanne, E.; Flament, J.; Bernardeschi, D.; Sterkers, O.; Fraysse, B.; et al. Treatment Choice in Single-Sided Deafness and Asymmetric Hearing Loss. A Prospective, Multicentre Cohort Study on 155 Patients. Clin. Otolaryngol. 2021, 46, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Wazen, J.J.; Spitzer, J.B.; Ghossaini, S.N.; Fayad, J.N.; Niparko, J.K.; Cox, K.; Brackmann, D.E.; Soli, S.D. Transcranial Contralateral Cochlear Stimulation in Unilateral Deafness. Otolaryngol. Head Neck Surg. 2003, 129, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Yuen, H.-W.; Bodmer, D.; Smilsky, K.; Nedzelski, J.M.; Chen, J.M. Management of Single-Sided Deafness with the Bone-Anchored Hearing Aid. Otolaryngol. Head Neck Surg. 2009, 141, 16–23. [Google Scholar] [CrossRef] [PubMed]
- McCreery, R.W.; Venediktov, R.A.; Coleman, J.J.; Leech, H.M. An Evidence-Based Systematic Review of Directional Microphones and Digital Noise Reduction Hearing Aids in School-Age Children with Hearing Loss. Am. J. Audiol. 2012, 21, 295–312. [Google Scholar] [CrossRef]
- Nelson, L.H.; Poole, B.; Muñoz, K. Preschool Teachers’ Perception and Use of Hearing Assistive Technology in Educational Settings. Lang. Speech Hear. Serv. Sch. 2013, 44, 239–251. [Google Scholar] [CrossRef]
- Moeller, M.P.; Donaghy, K.F.; Beauchaine, K.L.; Lewis, D.E.; Stelmachowicz, P.G. Longitudinal Study of FM System Use in Nonacademic Settings: Effects on Language Development. Ear. Hear. 1996, 17, 28–41. [Google Scholar] [CrossRef]
- Walker, E.A.; Curran, M.; Spratford, M.; Roush, P. Remote Microphone Systems for Preschool-Age Children Who Are Hard of Hearing: Access and Utilization. Int. J. Audiol. 2019, 58, 200–207. [Google Scholar] [CrossRef]
- American Academy of Audiology. Clinical Practice Guidelines: Remote Microphone Hearing Assistance Technologies for Children and Youth from Birth to 21 Years; American Academy of Audiology: Reston, VA, USA, 2011. [Google Scholar]
- Asp, F.; Stokroos, R.J.; Agterberg, M.J.H. Toward Optimal Care for Children With Congenital Unilateral Aural Atresia. Front. Neurol. 2021, 12, 687070. [Google Scholar] [CrossRef]
- Gray, L.; Kesser, B.; Cole, E. Understanding Speech in Noise after Correction of Congenital Unilateral Aural Atresia: Effects of Age in the Emergence of Binaural Squelch but Not in Use of Head-Shadow. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1281–1287. [Google Scholar] [CrossRef]
- Nadaraja, G.S.; Gurgel, R.K.; Kim, J.; Chang, K.W. Hearing Outcomes of Atresia Surgery versus Osseointegrated Bone Conduction Device in Patients with Congenital Aural Atresia: A Systematic Review. Otol. Neurotol. 2013, 34, 1394–1399. [Google Scholar] [CrossRef]
- Moon, I.J.; Byun, H.; Jin, S.H.; Kwon, S.; Chung, W.-H.; Hong, S.H.; Cho, Y.-S. Sound Localization Performance Improves after Canaloplasty in Unilateral Congenital Aural Atresia Patients. Otol. Neurotol. 2014, 35, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Vogt, K.; Desmet, J.; Janssen, A.M.; Agterberg, M.J.H.; Snik, A.F.M. Unexplained Variation in Benefit of Treatment of Congenital Unilateral Aural Atresia: A Review of the Literature. Audiol. Neurootol. 2021, 26, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Hirth, D.; Weiss, R.; Stöver, T.; Kramer, S. Audiological Benefit and Subjective Satisfaction with the ADHEAR Hearing System in Children with Unilateral Conductive Hearing Loss. Eur. Arch. Otorhinolaryngol. 2021, 278, 2781–2788. [Google Scholar] [CrossRef]
- Zhao, C.; Liu, Y.; Yang, J.; Chen, P.; Gao, M.; Zhao, S. Sound-Localisation Performance in Patients with Congenital Unilateral Microtia and Atresia Fitted with an Active Middle Ear Implant. Eur. Arch. Otorhinolaryngol. 2021, 278, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Yang, J.; Liu, Y.; Gao, M.; Chen, P.; Zheng, J.; Zhao, S. Horizontal Sound Localisation and Speech Perception in Bonebridge-Implanted Single-Sided Deafness Patients. J. Laryngol. Otol. 2020, 2020, 899. [Google Scholar] [CrossRef] [PubMed]
- Lailach, S.; Zahnert, T.; Maurer, J.; Hempel, J.-M.; Koitschev, A.; Hollfelder, D.; Frenzel, H.; Wollenberg, B.; Arndt, S. The Vibrating Ossicular Prosthesis in Children and Adolescents: A Retrospective Study. Eur. Arch. Otorhinolaryngol. 2020, 277, 55–60. [Google Scholar] [CrossRef]
- Mylanus, E.A.M.; Hua, H.; Wigren, S.; Arndt, S.; Skarzynski, P.H.; Telian, S.A.; Briggs, R.J.S. Multicenter Clinical Investigation of a New Active Osseointegrated Steady-State Implant System. Otol. Neurotol. 2020, 41, 1249–1257. [Google Scholar] [CrossRef]
- Goycoolea, M.; Ribalta, G.; Tocornal, F.; Levy, R.; Alarcón, P.; Bryman, M.; Cagnacci, B.; Catenacci, C.; Oyanguren, V.; Vilches, I.; et al. Clinical Performance of the OsiaTM System, a New Active Osseointegrated Implant System. Results from a Prospective Clinical Investigation. Acta Otolaryngol. 2020, 140, 212–219. [Google Scholar] [CrossRef]
- Agterberg, M.J.H.; Hol, M.K.S.; Cremers, C.W.R.J.; Mylanus, E.A.M.; van Opstal, A.J.; Snik, A.F.M. Conductive Hearing Loss and Bone Conduction Devices: Restored Binaural Hearing? Adv. Otorhinolaryngol. 2011, 71, 84–91. [Google Scholar] [CrossRef]
- Snik, A.; Agterberg, M.; Bosman, A. How to Quantify Binaural Hearing in Patients with Unilateral Hearing Using Hearing Implants. Audiol. Neurootol. 2015, 20 (Suppl. S1), 44–47. [Google Scholar] [CrossRef]
- Puglisi, G.E.; di Berardino, F.; Montuschi, C.; Sellami, F.; Albera, A.; Zanetti, D.; Albera, R.; Astolfi, A.; Kollmeier, B.; Warzybok, A. Evaluation of Italian Simplified Matrix Test for Speech-Recognition Measurements in Noise. Audiol. Res. 2021, 11, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Arndt, S.; Laszig, R.; Aschendorff, A.; Hassepass, F.; Beck, R.; Wesarg, T. Cochlear Implant Treatment of Patients with Single-Sided Deafness or Asymmetric Hearing Loss. HNO 2017, 65, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Forli, F.; Berrettini, S.; Bruschini, L.; Canelli, R.; Lazzerini, F. Cochlear Implantation in Patients with Asymmetric Hearing Loss: Reporting and Discussing the Benefits in Speech Perception, Speech Reception Threshold, Squelch Abilities, and Patients’ Reported Outcomes. J. Laryngol. Otol. 2022, 136, 964–969. [Google Scholar] [CrossRef]
- Berrettini, S.; Ghirri, P.; Lazzerini, F.; Lenzi, G.; Forli, F. Newborn Hearing Screening Protocol in Tuscany Region. Ital. J. Pediatr. 2017, 43, 82. [Google Scholar] [CrossRef] [PubMed]
- Bonne, N.-X.; Hanson, J.-N.; Gauvrit, F.; Risoud, M.; Vincent, C. Long-Term Evaluation of Sound Localisation in Single-Sided Deaf Adults Fitted with a BAHA Device. Clin. Otolaryngol. 2019, 44, 898–904. [Google Scholar] [CrossRef]
- Fuchsmann, C.; Tringali, S.; Disant, F.; Buiret, G.; Dubreuil, C.; Froehlich, P.; Truy, E. Hearing Rehabilitation in Congenital Aural Atresia Using the Bone-Anchored Hearing Aid: Audiological and Satisfaction Results. Acta Otolaryngol. 2010, 130, 1343–1351. [Google Scholar] [CrossRef]
- Brotto, D.; Sorrentino, F.; Cazzador, D.; Maritan, F.; Montino, S.; Agostinelli, A.; Zanoletti, E.; Martini, A.; Bovo, R.; Trevisi, P. Benefits of Bone Conduction Hearing Aid in Children with Unilateral Aural Atresia. Acta Otorhinolaryngol. Ital. 2023, 43, 221–226. [Google Scholar] [CrossRef]
- Agterberg, M.J.H.; Snik, A.F.M.; Van de Goor, R.M.G.; Hol, M.K.S.; Van Opstal, A.J. Sound-Localization Performance of Patients with Single-Sided Deafness Is Not Improved When Listening with a Bone-Conduction Device. Hear. Res. 2019, 372, 62–68. [Google Scholar] [CrossRef]
- Kim, G.; Ju, H.M.; Lee, S.H.; Kim, H.-S.; Kwon, J.A.; Seo, Y.J. Efficacy of Bone-Anchored Hearing Aids in Single-Sided Deafness: A Systematic Review. Otol. Neurotol. 2017, 38, 473–483. [Google Scholar] [CrossRef]
- Bruschini, L.; Canelli, R.; Morandi, A.; Cambi, C.; Fiacchini, G.; Berrettini, S.; Forli, F. Bone Anchored Hearing Aids for the Treatment of Asymmetric Hearing Loss. J. Int. Adv. Otol. 2020, 16, 313–317. [Google Scholar] [CrossRef]
- Nelissen, R.C.; Agterberg, M.J.H.; Hol, M.K.S.; Snik, A.F.M. Three-Year Experience with the Sophono in Children with Congenital Conductive Unilateral Hearing Loss: Tolerability, Audiometry, and Sound Localization Compared to a Bone-Anchored Hearing Aid. Eur. Arch. Otorhinolaryngol. 2016, 273, 3149–3156. [Google Scholar] [CrossRef] [PubMed]
- Hol, M.K.S.; Nelissen, R.C.; Agterberg, M.J.H.; Cremers, C.W.R.J.; Snik, A.F.M. Comparison between a New Implantable Transcutaneous Bone Conductor and Percutaneous Bone-Conduction Hearing Implant. Otol. Neurotol. 2013, 34, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Stenfelt, S. Transcranial Attenuation of Bone-Conducted Sound When Stimulation Is at the Mastoid and at the Bone Conduction Hearing Aid Position. Otol. Neurotol. 2012, 33, 105–114. [Google Scholar] [CrossRef]
- Han, J.-H.; Lee, J.; Lee, H.-J. Ear-Specific Hemispheric Asymmetry in Unilateral Deafness Revealed by Auditory Cortical Activity. Front. Neurosci. 2021, 15, 698718. [Google Scholar] [CrossRef]
- Vogt, K.; Wasmann, J.-W.; Van Opstal, A.J.; Snik, A.F.M.; Agterberg, M.J.H. Contribution of Spectral Pinna Cues for Sound Localization in Children with Congenital Unilateral Conductive Hearing Loss after Hearing Rehabilitation. Hear. Res. 2020, 385, 107847. [Google Scholar] [CrossRef]
- Mondelli, M.F.C.G.; Jacob, R.T.d.S.; Honório, H.M. The Use of Remote Microphone Systems in Unilateral Hearing Loss: A Preliminary Study among Brazilian Children and Teenagers. J. Appl. Oral Sci. 2019, 27, e20180744. [Google Scholar] [CrossRef] [PubMed]
- Oosthuizen, I.; Picou, E.M.; Pottas, L.; Myburgh, H.C.; Swanepoel, D.W. Listening Effort in School-Aged Children With Limited Useable Hearing Unilaterally: Examining the Effects of a Personal, Digital Remote Microphone System and a Contralateral Routing of Signal System. Trends Hear. 2021, 25, 2331216520984700. [Google Scholar] [CrossRef]
- Canfarotta, M.W.; Kane, S.L.G.; Buss, E. Effects of Presentation Level on Spatial Hearing With and Without Bone-Conduction Amplification in Congenital Unilateral Aural Atresia. Otol. Neurotol. 2021, 42, e388–e392. [Google Scholar] [CrossRef]
- Danhauer, J.L.; Johnson, C.E.; Mixon, M. Does the Evidence Support Use of the Baha Implant System (Baha) in Patients with Congenital Unilateral Aural Atresia? J. Am. Acad. Audiol. 2010, 21, 274–286. [Google Scholar] [CrossRef]
- Nelissen, R.C.; Mylanus, E.A.M.; Cremers, C.W.R.J.; Hol, M.K.S.; Snik, A.F.M. Long-Term Compliance and Satisfaction With Percutaneous Bone Conduction Devices in Patients With Congenital Unilateral Conductive Hearing Loss. Otol. Neurotol. 2015, 36, 826–833. [Google Scholar] [CrossRef]
- Picou, E.M.; Davis, H.; Tharpe, A.M. Considerations for Choosing Microphone Technologies for Students With Limited Useable Hearing Unilaterally. Lang. Speech Hear. Serv. Sch. 2020, 51, 74–83. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | SSD | UAA | p | |
|---|---|---|---|---|
| Mean Age (y) | 10.2 (5 ÷ 15) | 9.6 (5 ÷ 15) | 10.8 (8 ÷ 13) | 0.575 |
| Gender (F; M) | 3; 7 | 2; 3 | 1; 4 | 0.500 |
| Hearing-impaired side (R; L) | 2; 8 | 2; 3 | 0; 5 | 0.444 |
| Hearing threshold better ear (AC) (dB HL) | 17.2 (15 ÷ 20) | 18.7 (15 ÷ 20) | 16 (15 ÷ 20) | 0.125 |
| Hearing threshold worse ear (AC) (dB HL) | 62.7 (55 ÷ 85) | 80 (65 ÷ 105) | 58 (55 ÷ 65) | 0.017 * |
| Hearing threshold better ear (BC) (dB HL) | 17.2 (15 ÷ 20) | 18.7 (15 ÷ 20) | 16 (15 ÷ 20) | 0.125 |
| Hearing threshold worse ear (BC) (dB HL) | N.T. | N.T. | 15 (15÷15) |
| Total | SSD | UAA | p | |
|---|---|---|---|---|
| Unaided | ||||
| Unaided SRT S0N0 (dB HL) | −1.9 [−4.3 ÷ 1.7] | −0.9 [−1.9 ÷ 1.7] | −2.8 [−4.3 ÷ 0] | 0.095 |
| Unaided SRT SbNw (dB HL) | −6.6 [−9.4 ÷ −2.9] | −5.9 [−8.5 ÷ −2.9] | −7.3 [−9.4 ÷ −4.8] | 0.421 |
| Unaided SRT SwNb (dB HL) | −0.9 [−3.7 ÷ 2.7] | 0.9 [−0.9 ÷ 2.7] | −2.7 [−3.7 ÷ −1.2] | 0.008 * |
| BAHD | ||||
| SRT S0N0 with BAHD (dB HL) | −3.4 [−6.1 ÷ 2.3] | −2.3 [−5.4 ÷ 2.3] | −4.7 [−6.1 ÷ −3.2] | 0.151 |
| SRT SbNw with BAHD (dB HL) | −5.1 [−8.4 ÷ 2.4] | −3.4 [−7.9 ÷ 2.4] | −6.9 [−8.4 ÷ −5.1] | 0.151 |
| SRT SbNw with BAHD (dB HL) | −3.7 [−7 ÷ 0.1] | −2.8 [−4.8 ÷ −0.1] | −4.6 [−7.0 ÷ −1.3] | 0.222 |
| RM | ||||
| SRT S0N0 with RM (dB HL) | −3.3 [−7.5 ÷ −0.2] | −2.0 [−3.8 ÷ −0.2] | −4.7 [−7.5 ÷ −2] | 0.095 |
| SRT SbNw with RM (dB HL) | −7.5 [−12.1 ÷ −1.3] | −6.3 [−9.9 ÷ −1.3] | −8.7 [−12.1 ÷ −4.7] | 0.310 |
| SRT SbNw with RM (dB HL) | −5.5 [−12.3 ÷ −1] | −4.2 [−8 ÷ −1] | −6.8 [−12.3 ÷ −3.4] | 0.421 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazzerini, F.; Bruschini, L.; Fiacchini, G.; Canzi, P.; Berrettini, S.; Forli, F. The Role of Bone-Anchored Hearing Devices and Remote Microphones in Children with Congenital Unilateral Hearing Loss. Brain Sci. 2023, 13, 1379. https://doi.org/10.3390/brainsci13101379
Lazzerini F, Bruschini L, Fiacchini G, Canzi P, Berrettini S, Forli F. The Role of Bone-Anchored Hearing Devices and Remote Microphones in Children with Congenital Unilateral Hearing Loss. Brain Sciences. 2023; 13(10):1379. https://doi.org/10.3390/brainsci13101379
Chicago/Turabian StyleLazzerini, Francesco, Luca Bruschini, Giacomo Fiacchini, Pietro Canzi, Stefano Berrettini, and Francesca Forli. 2023. "The Role of Bone-Anchored Hearing Devices and Remote Microphones in Children with Congenital Unilateral Hearing Loss" Brain Sciences 13, no. 10: 1379. https://doi.org/10.3390/brainsci13101379
APA StyleLazzerini, F., Bruschini, L., Fiacchini, G., Canzi, P., Berrettini, S., & Forli, F. (2023). The Role of Bone-Anchored Hearing Devices and Remote Microphones in Children with Congenital Unilateral Hearing Loss. Brain Sciences, 13(10), 1379. https://doi.org/10.3390/brainsci13101379